Abstract
Benzoyl peroxide (BPO) and niacinamide (Niac) are commonly used alone or in combination with other molecules in the treatment of acne. BPO and Niac in the same product could exert complementary and synergistic effects improving efficacy in acne. Furthermore, Niac could reduce some side effects of BPO, such as skin irritation and erythema. A film-forming cream product containing BPO 4% and Niac 4%, vehiculated in a mixture of polyvinyl alcohol (PVA) and perfluoropolyether (PFPE) has been recently developed (B-N cream). A 28-day, assessor-blinded pilot trial was conducted to evaluate the clinical efficacy, skin tolerability, sebum production, skin redness, and skin microbiome modulation of B-N cream in subjects with mild to moderate acne of the face. Twenty-two adult men and women with mild-to-moderate acne of the face participated in this trial, after their written informed consent. B-N cream was applied once daily in the evening. The use of B-N cream was associated with a statistically significant decrease in acne lesions after treatment in comparison with baseline (non-inflammatory lesions: −40%; inflammatory lesions: −43% and total lesions: −41%). The use of the cream was not associated with a skin barrier function alteration. The skin redness score (−11%) and the sebum production (−42%) were significantly reduced after treatment. The use of B-N cream determined a reduction in the relative abundance of the Actinobacteria phylum (Corynebacterium and Propionibacterium, from 56% to 47%) and a significant increase in the abundance of Bacteroidetes phylum (from 3% to 5.2%). In addition, the product was well tolerated. In conclusion, this film-forming, medical device cream was effective in subjects with mild-to-moderate acne, reducing acne lesions and sebum production without altering skin barrier function, offering good skin tolerability. Furthermore, this product exerts positive skin microbiome modulation effects.
1. Introduction
Acne vulgaris (AV) is a very common skin inflammatory disease affecting the pilosebaceous unit [1]. It is well known that AV pathogenesis involves an increase in sebum production, follicular hyperkeratinization with sebaceous follicules obstruction, Propionibacterium acnes (Cutibacterium acnes) proliferation and inflammation [2]. AV is characterized by an alteration in the skin barrier function even in the absence of anti-acne aggressive treatments such as oral or topical retinoids [3]. Commonly, AV is treated using topical products, alone or in combination, such as benzoyl peroxide, retinoids and antibiotics [4]. The clinical success of acne treatments is deeply influenced by adherence or compliance with the therapy. Low skin tolerability and/or low efficacy are the main reasons for the lack of compliance [5,6]. Benzoyl peroxide (BPO) and niacinamide (Niac) are commonly used alone or in combination with other molecules in the treatment of acne. BPO is a very effective topical product able to express bactericidal activity against C. acnes [7]. BPO has also keratolytic effects. However, BPO can have, especially during the initial treatment phases, a low skin tolerability with skin erythema and a negative effect on skin barrier function [8]. During treatment with BPO, the transepidermal water loss can increase up to 80%, demonstrating that BPO can alter skin barrier function. In subjects with acne, the transepidermal water loss is higher in comparison with normal subjects [9] and the application of irritative molecules, like BPO and retinoids, could further increase this parameter [10]. Niacinamide provides potent anti-inflammatory properties without the risk of bacterial resistance and systemic side effects and this molecule could represent an interesting treatment modality for acne vulgaris [11]. Several reviews support that the use of Niac is effective in acne [11,12]. Combination products of BPO (2.5%) and Niac (5%) have been developed [13]. Combining BPO and Niac in the same product could have the advantage of expressing complementary and synergistic effects improving efficacy in acne [13]. Furthermore, Niac could reduce some side effects of BPO, such as skin irritation and erythema. A film-forming cream product using BPO 4% and Niac 4% (B-N cream) has been recently developed. In this medical device, BPO 4% and Niac 4% are vehiculated in a mixture of polyvinyl alcohol (PVA) and perfluoropolyether (PFPE). These two components of the cream after application form a transparent and non-occlusive film on the skin allowing BPO and Niac to act locally. Topical film-forming systems exert emollient or protective effects and facilitate the local action or transdermal penetration of actives [14].
PVA and PFPE are color and odorless film-forming polymers [15]. Due to their inertness and stability, they are generally considered safe and biocompatible. PVA is able to absorb water and therefore when applied to the skin it could act as a moisturizer. Both polymers are also effective transdermal drug delivery systems when used in topical products. PFPE is another kind of special liquid material [16]. It is colorless, tasteless, non-poisonous, hypo-allergenic, and has excellent handling properties, chemical stability, lower viscosity, and excellent film-forming ability, so it is suitable for application in the field of cosmetics. PFPE has been demonstrated to reduce the quantity of sebum on the skin [17]. So far, no clinical and instrumental data on this medical device are available. To evaluate the clinical efficacy, skin tolerability, sebum production, and skin microbiome modulation of B-N cream in subjects with mild to moderate acne of the face, we conducted a 28-day, prospective, assessor-blinded trial.
2. Materials and Methods
2.1. Population and Study Design
Twenty-two adult men (N = 3) and women (N = 19), with a mean age 23 years (range 18–32) participated, after their written informed consent in a 28-day, assessor-blinded trial. B-N cream (a film-forming cream containing BPO 4% and Niac 4% vehiculated in a mixture of polyvinyl alcohol and perfluoropolyether) was applied once daily in the evening. The main inclusion criteria were age between 18 and 40 years old; both females and males with a clinical diagnosis of mild-to-moderate acne affecting the face. The main exclusion criteria were (1) personal history of adverse reactions to the same type of products as the investigational product, (2) under treatment, before the study, able to interfere with the interpretation of the study results, particularly: systemic retinoids (isotretinoin per os) within the 6 months, other systemic anti-acne medication within the 3 months, topical retinoids within the 2 months, other topical anti-acne medication within the month, anti-acne cosmetic products within the 2 weeks, topical or systemic medication with anti-inflammatory or antihistamine products within the 2 weeks, antibiotics within the 2 weeks, medication for malignancy (of any kind) within the 5 years, desensitization treatment within the 6 months. The trial was coordinated by Eurofins Cosmetics & Personal Care Italy S.r.l. (20055 Vimodrone (MI), Italy,). The tested product should be applied at home by the test subjects under the normal conditions of use: (1) application site: face; (2) duration and frequency of use: once a day, for 28 consecutive days; and (3) the Investigational product directions for use were to apply the product in the evening on the surfaces to be treated distributing uniformly, after thoroughly cleansing the affected areas. The cream should be distributed with clean hands. Regarding the cleansing procedures, the subject was instructed to apply it morning and evening to wet skin, massaging gently letting it act for 1–2 min, then rinse thoroughly.
2.2. Study Outcomes
Clinical efficacy was evaluated by acne lesion count (non-inflammatory lesions, NI-L, Inflammatory lesions, I-L, and total lesions, T-L) by comparing baseline values and values at the end of the treatment period. Skin tolerability was assessed by performing a transepidermal water loss measurement (TEWL expressed in g/m2/h; Tewameter® TM Hex, Courage & Khazaka, Cologne, Germany); skin redness was determined using a dedicated software imaging analysis of the face calculating a skin redness score (Antera® 3D PRO, Miravex, Irland, using a dedicate software for the analysis of the parameters “redness”); and sebum production was evaluated using Sebumeter SM 815 (Courage & Khazaka, Germany). TEWL, sebum production, and skin redness were determined at baseline and after treatment in the same check area. Finally, the determination of the skin microbiota through skin swabs by skin DNA sequencing was performed to analyze the bacterial genes present on the skin and their relative proportions (microbiome). The genomic DNA from the swab heads is extracted using Ion 16S Metagenomics Kit (ThermoFisher Scientific, Waltham, MA, USA). The Ion 16S™ Metagenomics Kit uses two primer pools to amplify seven hypervariable regions of bacterial 16S rRNA. The amplified fragments can then be sequenced on either the Ion S5™ or the Ion PGM™ Systems and analyzed using the Ion16S metagenomics workflow in Ion Reporter™ Software (ThermoFisher Scientific, Waltham, MA, USA). Considering the potential variation of skin microbiota according to the skin area, skin swabs were performed on the right cheek area of each subject. All the efficacy parameters were performed by an investigator unaware of the type of treatment. All the tests were performed by competent investigators and trained and qualified technical staff.
2.3. Statistical Analysis
Statistical analysis was performed using Graph-Pad Statistical Software (Version 10, GraphPad Software, Inc., La Jolla, CA, USA). Continuous variables were expressed as mean ± standard deviation (SD). The primary (evolution of AV lesions count) and secondary outcomes of the study were evaluated using both paired parametric and non-parametric tests (Student’s t-test and Wilcoxon test, respectively) comparing baseline with end-of-treatment values according to the type of the distribution (normal or not). In relation to the skin microbiome analysis, the bacterial community was investigated by assessing for each experimental time (D0/T0, D28) the average and standard deviation, the variations versus D0/T0 and the distribution of difference (D28-D0/T0) of each bacterial population (Shapiro–Wilk normality test, threshold 1%; Student’s t-test set at 5%—Wilcoxon test set at 5%). In view of the proof-of-concept nature of the present trial, a formal sample size calculation was not performed. We decided to enroll at least 20 evaluable subjects.
2.4. Ethical Issues
The study was performed in the spirit of (1) the general principles of medical ethics in clinical research coming from the Declaration of Helsinki (June 1964) and its successive amendments, (2) the international recommendations relating to Good Clinical Practices for conducting clinical trials for drugs ICH TOPIC E6 (R2) of November 2016; CPMP/ICH/135/95), and (3) the Directive of the European Parliament and Council 2001/20/EC concerning the harmonization of legislative, statutory and administrative provisions of the member States relating to the application of good clinical practices when conducting clinical trials for drugs for human use—OJ/EC of 01/05/2001. The study did not begin without the approval of the Internal Revision Committee. The Internal Revision Committee gave its opinion on 18 November 2022. The information about the study was given to each test subject before the start of the study. This information was accessible, understandable, and suitable for each test subject. It was orally given and then in a written specific document. This information was completed, if necessary, by the dermatologist (or the competent person designated) who answered all the questions asked by the test subject.
3. Results
All the subjects concluded the 28-day treatment period. The use of B-N cream was associated with a statistically significant decrease in acne lesions after treatment in comparison with the baseline (NI-L: −40%; I-L: −43% and TL: −41%). Table 1 reports numerical variations of NI-L, I-L and TL from baseline to day 28.

Table 1.
Acne lesions evaluated at baseline (T0) and after 28 days (T28) in all the subjects included in the study (n = 22).
The use of the cream was not associated with a skin barrier function alteration. At baseline, the TEWL value was 17.3 ± 5 and 18.4 ± 4 at day 28 (difference not significant) (Table 2). The skin redness score was significantly reduced after treatment in comparison with the baseline (54 ± 14 vs. 61 ± 15; representing an 11% reduction; p < 0.05). Sebum production was significantly reduced by 42% after treatment (Table 2).
Table 2.
Evolution of Transepidermal water loss measurements, sebum production (skin lipids), and skin redness.
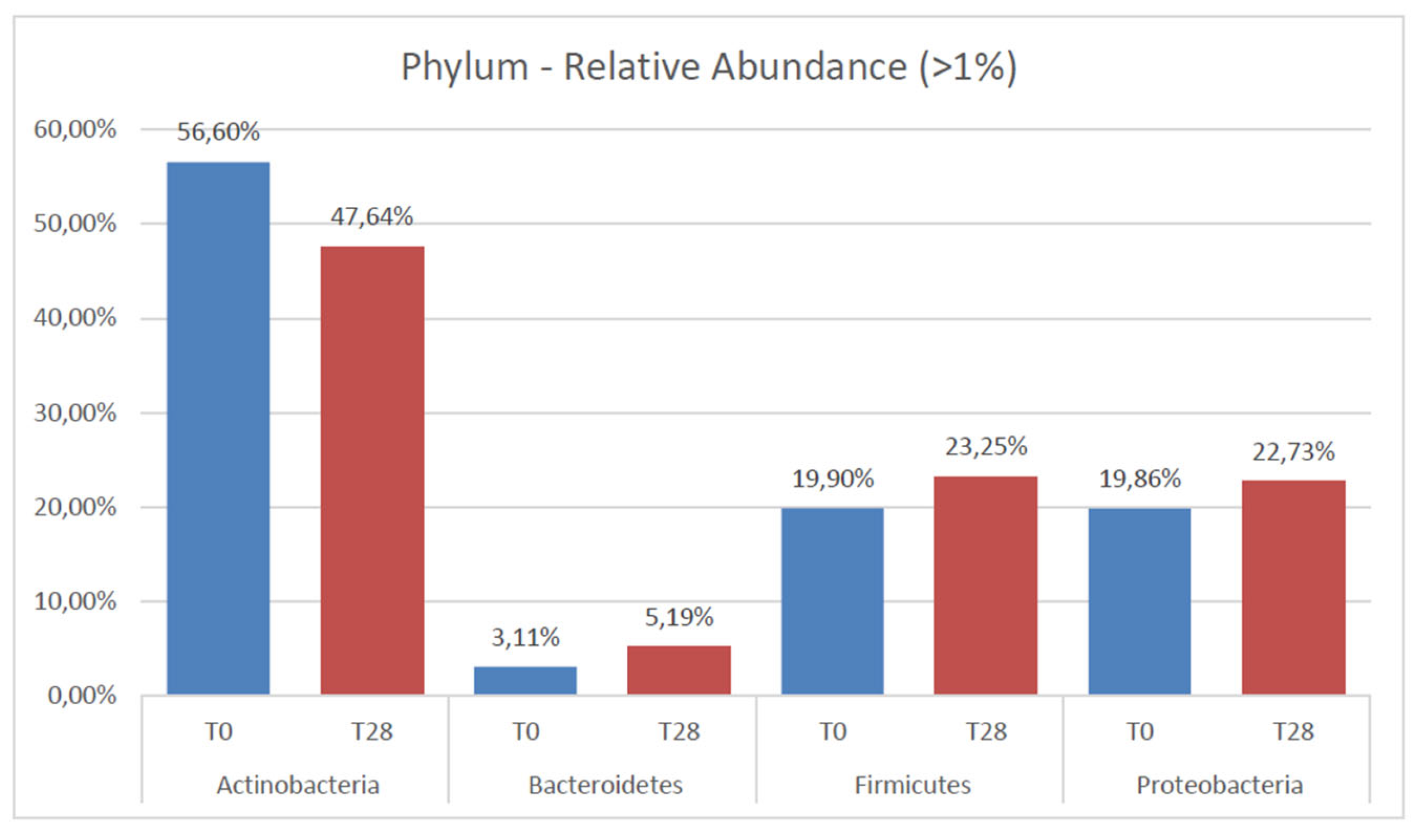
The skin microbiome evaluation demonstrated that the use of B-N cream was associated with a significant reduction in the relative abundance of the Actinobacteria phylum (Corynebacterium and Propionibacterium) which was reduced from 56.6 ± 23.5% at baseline to 47.6 ± 14.5% after treatment. The treatment was also able to increase significantly the abundance of Bacteroidetes phylum (from 3.1 ± 3.2% to 5.2 ± 3.5%). No other modification in the skin microbiome was observed (Figure 1).
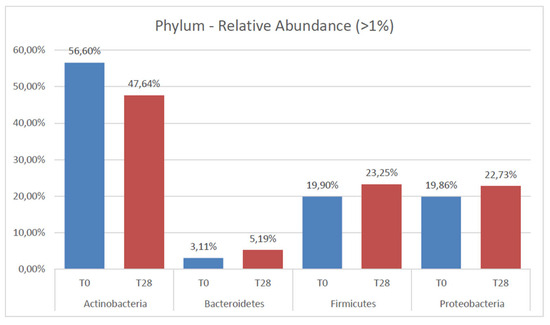
Figure 1.
Relative abundance of each phyla detected at a level > 1%, at baseline (T0) and after 28 consecutive days of treatment (T28).
The product was well tolerated. No relevant side effects were recorded.
4. Discussion
In our trial, we demonstrated that a film-forming cream containing BPP 4% and Niacinamide 4% is effective and well tolerated in the treatment of AV. This product does not alter skin barrier function and is also able to reduce skin inflammation. This combination reduces sebum production and can positively modulate the skin microbiome. Benzoyl peroxide is available in various strengths (2.5–20%) and vehicles (gels, lotions, solutions, creams, soap bars, pads, masks, and washes), as well as in combination formulation with the topical antibiotic erythromycin or clindamycin phosphate [18]. It is also combined with the topical retinoid adapalene. BPO is an effective antibacterial compound reducing the risk of selected resistant bacterial strains. However, BPO can alter skin barrier function and cause skin irritation. Part of the mechanism of action of BPO could be ascribed to the formation of reactive oxygen species (ROS) which can exert bactericidal activity but also skin irritation [4,7,19]. Niacinamide is also a common topical product used in different skin inflammatory diseases, such as AV [12]. Topical Niac induced a significant reduction in the sebum excretion rate and decreased the casual sebum levels (sebum on the skin surface) after 4 weeks of treatment [20]. Niac helps protect the natural barrier of the skin and may have a bacteriostatic effect on C. acnes. Finally, in vitro data show that Niac decreases the secretion of interleukin-8, a cytokine produced by keratinocytes in response to pathogens (including C. acnes) [21]. Niac therefore can exert an anti-inflammatory effect through the inhibition of leukocyte chemotaxis. There is a strong rational to use BPO and Niacinamide in combination due to the fact that these two molecules have different anti-acne mechanisms of action. Furthermore, niacinamide can in part reduce the negative effects of BPO on skin barrier function with the advantage of increasing skin tolerability. It is relevant to point out that in our study the TEWL measured values are in line with published data supporting the fact that TEWL in acne subjects is higher, even before the use of specific products, in comparison with healthy subjects [9]. In addition, quite recently a relevant role of the WNT-βcatenin and AKT/mTORC systems have been demonstrated in the pathogenesis of acne [22,23]. Aberrant Wnt-βcatenin signaling is involved in the formation of comedons. Akt/mTORC is activated in acne subjects and can be involved in hypersebhorrea and comedogenesis [24]. Both BPO and niacinamide have been demonstrated to attenuate Wnt-βcatenin and Akt/mTORC signaling [25]; therefore, the composition of the tested product could be interesting also for this aspect and rationale. This B-N film-forming cream is at the moment the only medical device using an equal concentration (4%) of both products in a film-forming cream formulation. Our trial supports the data that this combination vehiculated with two specific film-forming substances such as polyvinyl alcohol (PVA) and perfluoropolyether (PFPE) is very effective in reducing acne lesions with good skin tolerability. It is interesting to note that in our study we observed a reduction in acne total lesions of 41%.
The use of BPO as monotherapy in a recent network metanalysis of 221 trials assessing the efficacy of different topical anti-acne products, was associated with a 20% reduction (95% CI: 17–25%). When used in combination with adapalene, BPO reduces total acne lesions by 25%. When used in combination with retinoid and topical antibiotics, BPO can reduce total acne lesion number by 33% (95% CI: 25–41%). However, the fixed combination of BPO and retinoids is associated with a significant odd ratio of discontinuation due to adverse events compared to the placebo of 4.4 [26].
The tested product of this trial was very well tolerated with a reduction in skin irritation and a lack of skin barrier alteration function. Another interesting effect of this medical device was the relevant reduction in sebum production observed after 28 days of treatment (−42%). This effect was not observed so far for BPO. A sebum regulatory effect could be performed by the film-forming components of the tested cream (PFPE or PVA). This latter aspect can further underline the peculiarity of this medical device as an interesting therapeutic approach in subjects with mild to moderate acne. Finally, we observed that the use of this cream was associated with positive modulating effects on the face microbiome, with a significant reduction in the Acinetobacter group (to which C. acnes belongs to). Recent data have shown that even if a clinical improvement is registered, after oral retinoids treatment or topical BPO, a negative effect on the skin microbiome is observed [27]. In this view, our data can support the concept that B-N film-forming cream could be an interesting first-line treatment in mild to moderate acne but also an interesting coadjuvant treatment strategy in severe forms. Some study limitations should be taken into account by evaluating the study results. This was not a double-blind trial, and there was not a control group. However, the present study was a pilot proof-of-concept trial. The study duration was only 28 days. To assess the full efficacy of an anti-acne regimen, in general 12 weeks is considered the most appropriate treatment period. However, one of the main outcomes of our study was to evaluate the skin tolerability of this combination, and 4 weeks in this regard could be considered sufficient. Further larger prospective controlled studies are warranted to evaluate whether this therapeutic strategy could be helpful in the management of common acne.
5. Conclusions
This film-forming, medical device cream containing BPO 4% and Niacinamide 4% in subjects with mild-to-moderate acne has shown to be effective in reducing acne lesions, and sebum production without altering skin barrier function, offering good skin tolerability. Furthermore, the use of this product was also associated with positive skin microbiome modulation effects.
Author Contributions
Conceptualization, M.P. and K.E.; methodology, M.P. and K.E.; writing—original draft preparation, M.P. and K.E. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Internal Revision Committee of Eurofins Biolab S.r.l. on 18 November 2022.
Informed Consent Statement
All participants provided written informed consent before starting the study.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Kircik, L.H. Advances in the Understanding of the Pathogenesis of Inflammatory Acne. J. Drugs Dermatol. 2016, 15, s7–s10. [Google Scholar]
- Vasam, M.; Korutla, S.; Bohara, R.A. Acne vulgaris: A review of the pathophysiology, treatment, and recent nanotechnology based advances. Biochem. Biophys. Rep. 2023, 36, 101578. [Google Scholar] [CrossRef]
- Schachner, L.A.; Alexis, A.F.; Andriessen, A.; Berson, D.; Gold, M.; Goldberg, D.J.; Hu, S.; Keri, J.; Kircik, L.; Woolery-Lloyd, H. Insights into acne and the skin barrier: Optimizing treatment regimens with ceramide-containing skincare. J. Cosmet. Dermatol. 2023, 22, 2902–2909. [Google Scholar] [CrossRef]
- Rathi, S. Acne vulgaris treatment: The Current Scenario. Indian J. Dermatol. 2011, 56, 7. [Google Scholar] [CrossRef]
- Bhatia, A.C.; Jimenez, F. Rapid treatment of mild acne with a novel skin care system containing 1% salicylic acid, 10% buffered glycolic acid, and botanical ingredients. J. Drugs Dermatol. 2014, 13, 678–683. [Google Scholar]
- De Lucas, R.; Moreno-Arias, G.; Perez-López, M.; Vera-Casaño, Á.; Aladren, S.; Milani, M. Adherence to drug treatments and adjuvant barrier repair therapies are key factors for clinical improvement in mild to moderate acne: The ACTUO observational prospective multicenter cohort trial in 643 patients. BMC Dermatol. 2015, 15, 17. [Google Scholar] [CrossRef]
- Leyden, J.J.; Del Rosso, J.Q.; Webster, G.F. Clinical considerations in the treatment of acne vulgaris and other inflammatory skin disorders: Focus on antibiotic resistance. Cutis 2007, 79, 9–25. [Google Scholar]
- Araviiskaia, E.; Layton, A.M.; Estebaranz, J.L.L.; Ochsendorf, F.; Micali, G. The Synergy between Pharmacological Regimens and Dermocosmetics and Its Impact on Adherence in Acne Treatment. Dermatol. Res. Pract. 2022, 2022, 1–10. [Google Scholar] [CrossRef]
- Yamamoto, A.; Takenouchi, K.; Ito, M. Impaired water barrier function in acne vulgaris. Arch. Dermatol. Res. 1995, 287, 214–218. [Google Scholar] [CrossRef]
- Thiboutot, D.; Del Rosso, J.Q. Acne Vulgaris and the Epidermal Barrier: Is Acne Vulgaris Associated with Inherent Epidermal Abnormalities that Cause Impairment of Barrier Functions? Do Any Topical Acne Therapies Alter the Structural and/or Functional Integrity of the Epidermal Barrier? J. Clin. Aesthet. Dermatol. 2013, 6, 18–24. [Google Scholar]
- Walocko, F.M.; Eber, A.E.; Keri, J.E.; AL-Harbi, M.A.; Nouri, K. The role of nicotinamide in acne treatment. Dermatol. Ther. 2017, 30, e12481. [Google Scholar] [CrossRef]
- Forbat, E.; Al-Niaimi, F.; Ali, F.R. Use of nicotinamide in dermatology. Clin. Exp. Dermatol. 2017, 42, 137–144. [Google Scholar] [CrossRef]
- Kaewsanit, T.; Chakkavittumrong, P.; Waranuch, N. Clinical Comparison of Topical 2.5% Benzoyl Peroxide plus 5% Niacinamide to 2.5% Benzoyl Peroxide Alone in the Treatment of Mild to Moderate Facial Acne Vulgaris. J. Clin. Aesthet. Dermatol. 2021, 14, 35–41. [Google Scholar]
- Kathe, K.; Kathpalia, H. Film forming systems for topical and transdermal drug delivery. Asian J. Pharm. Sci. 2017, 12, 487–497. [Google Scholar] [CrossRef]
- Muppalaneni, S.; Omidian, H. Polyvinyl Alcohol in Medicine and Pharmacy: A Perspective. J. Dev. Drugs 2013, 2, 1–5. [Google Scholar] [CrossRef]
- Rigano, L.; Savonelli, S.; Bencini, P.L. Use and properties of perfluoropolymethyl-isopropylethers in skin and hair cleaning; system stabilization and interference with sebum redistribution on skin and hair. Int. J. Cosmet. Sci. 1989, 11, 259–282. [Google Scholar] [CrossRef]
- Zhang, D.; Zhang, Y.; Bai, Y.; Tai, X.; Wang, W.; Wang, G. Preparation and Property of Perfluoropolyether Emulsions. Polymers 2019, 11, 932. [Google Scholar] [CrossRef]
- Dutil, M. Benzoyl peroxide: Enhancing antibiotic efficacy in acne management. Skin. Therapy Lett. 2010, 15, 5–7. [Google Scholar]
- Worret, W.; Fluhr, J.W. Acne therapy with topical benzoyl peroxide, antibiotics and azelaic acid. JDDG J. Der Dtsch. Dermatol. Ges. 2006, 4, 293–300. [Google Scholar] [CrossRef]
- Draelos, Z.D.; Matsubara, A.; Smiles, K. The effect of 2% niacinamide on facial sebum production. J. Cosmet. Laser Ther. 2006, 8, 96–101. [Google Scholar] [CrossRef]
- Grange, P.A.; Raingeaud, J.; Calvez, V.; Dupin, N. Nicotinamide inhibits Propionibacterium acnes-induced IL-8 production in keratinocytes through the NF-κB and MAPK pathways. J. Dermatol. Sci. 2009, 56, 106–112. [Google Scholar] [CrossRef]
- Liu, C.; Takada, K.; Zhu, D. Targeting Wnt/β-Catenin Pathway for Drug Therapy. Med. Drug Discov. 2020, 8, 100066. [Google Scholar] [CrossRef]
- Han, J.; Lin, K.; Choo, H.; Chen, Y.; Zhang, X.; Xu, R.-H.; Wang, X.; Wu, Y. Distinct bulge stem cell populations maintain the pilosebaceous unit in a β-catenin-dependent manner. IScience 2023, 26, 105805. [Google Scholar] [CrossRef]
- Cong, T.-X.; Hao, D.; Wen, X.; Li, X.-H.; He, G.; Jiang, X. From pathogenesis of acne vulgaris to anti-acne agents. Arch. Dermatol. Res. 2019, 311, 337–349. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.-H.; Shin, J.Y.; Kim, J.; Kang, N.-G.; Lee, S. Niacinamide Down-Regulates the Expression of DKK-1 and Protects Cells from Oxidative Stress in Cultured Human Dermal Papilla Cells. Clin. Cosmet. Investig. Dermatol. 2021, 14, 1519–1528. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.-Y.; Chang, I.-J.; Bolick, N.; Hsu, W.-T.; Su, C.-H.; Hsieh, T.-S.; Huang, I.-H.; Lee, C.-C. Comparative Efficacy of Pharmacological Treatments for Acne Vulgaris: A Network Meta-Analysis of 221 Randomized Controlled Trials. Ann. Fam. Med. 2023, 21, 358–369. [Google Scholar] [CrossRef] [PubMed]
- Lam, M.; Hu, A.; Fleming, P.; Lynde, C.W. The Impact of Acne Treatment on Skin Bacterial Microbiota: A Systematic Review. J. Cutan. Med. Surg. 2022, 26, 93–97. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).