Functionalization of Ceramic Coatings for Enhancing Integration in Osteoporotic Bone: A Systematic Review

 ,
, 



Abstract

1. Introduction
2. Methods
2.1. Focused Question
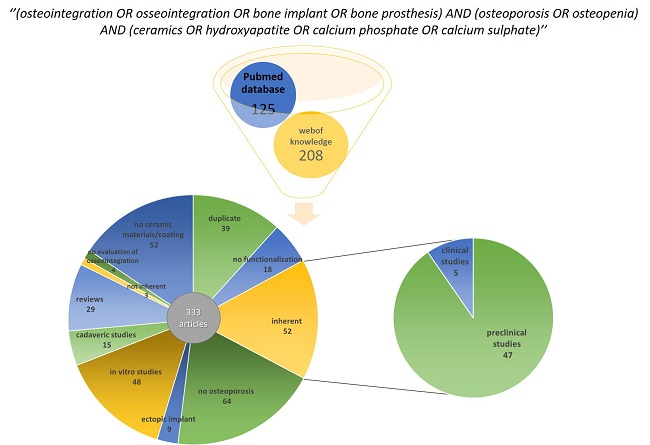
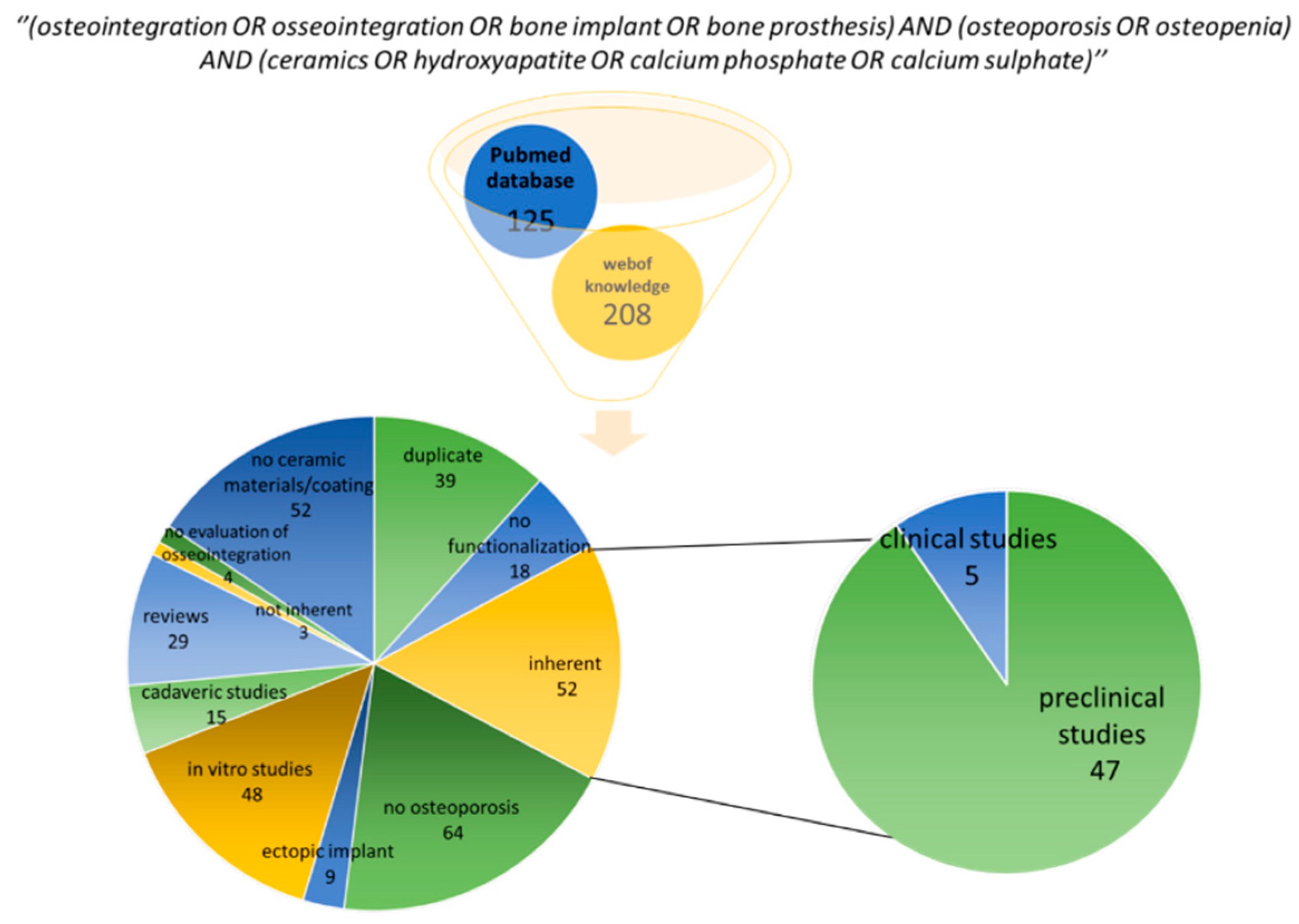
2.2. Descriptive Systematic Literature Review
2.3. Data Extraction and Management
3. Results
3.1. Summary of the Literature Results
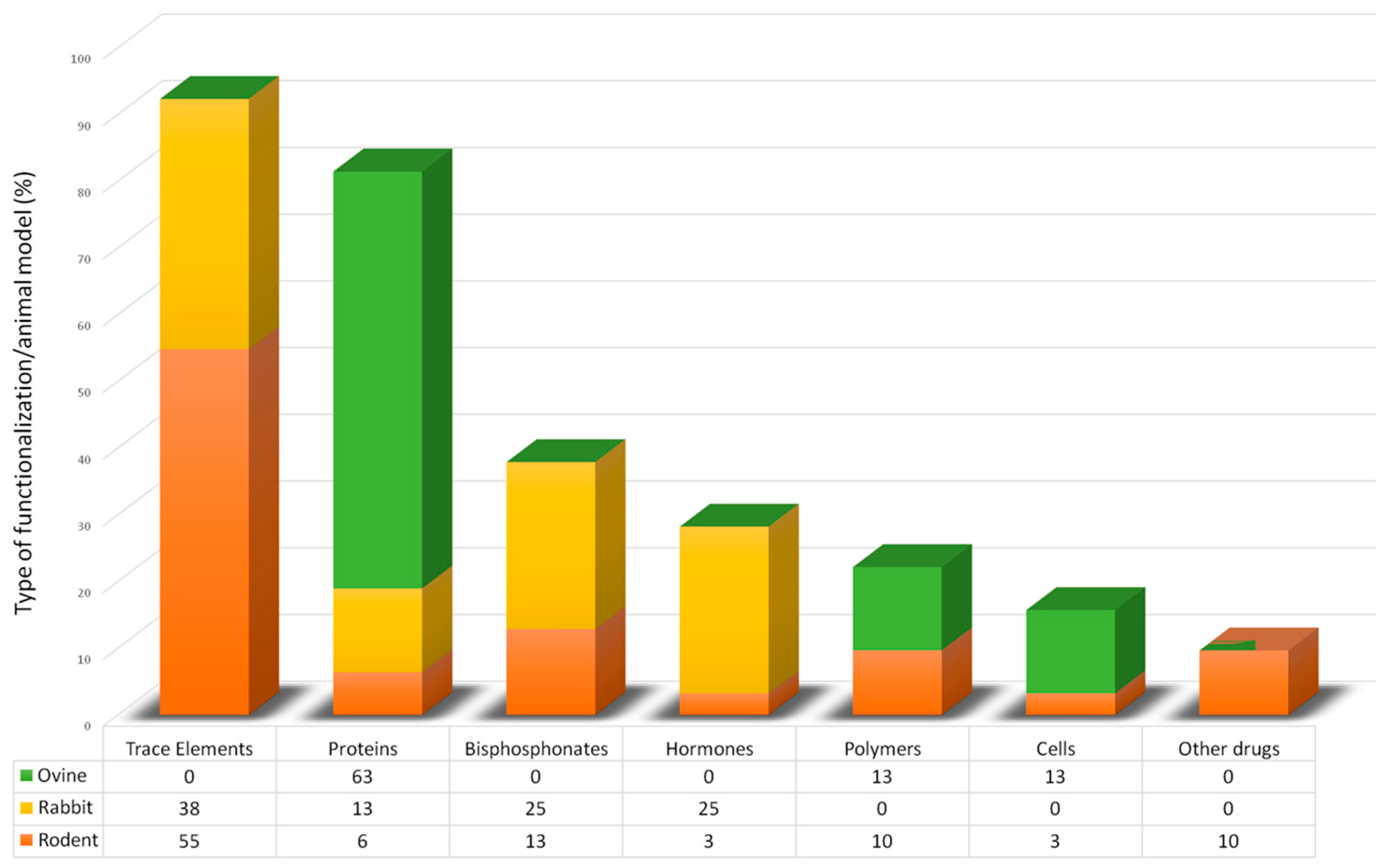
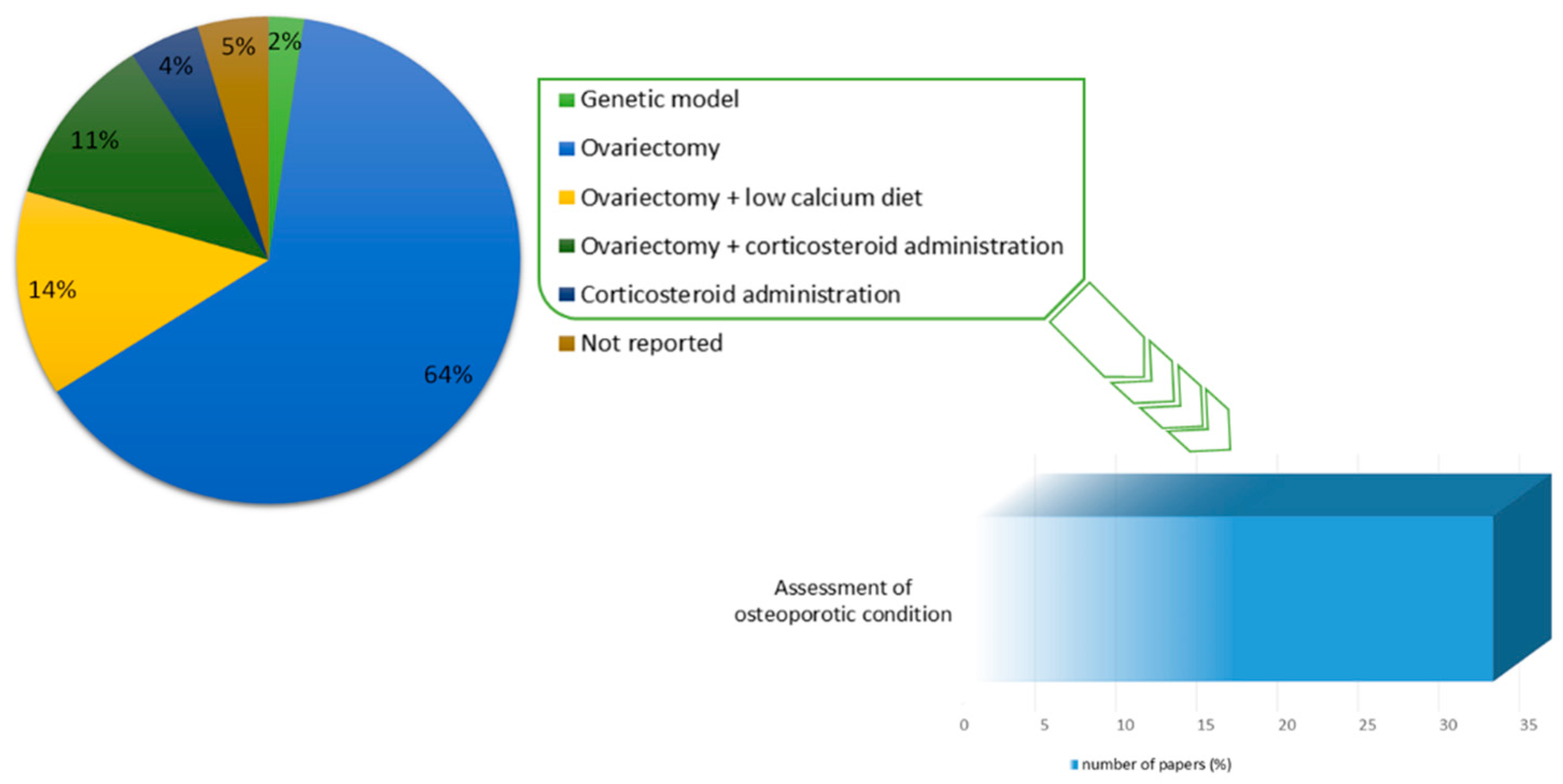
3.2. Preclinical Studies
3.2.1. Small Animal Models
Mouse Model
Rat Model
3.2.2. Medium Animal Model
3.2.3. Large Animal Model
3.2.4. Clinical Studies
4. Discussion
5. Conclusions
Funding
Conflicts of Interest
Abbreviations
| mAChR | muscarinic acetylcholine receptors |
| KO | knock out |
| MBG | morcellized bone graft |
| HR SEM | high resolution scanning electron microscopy |
| EDS | energy dispersive X-ray spectrometry |
| MAR | mineral apposition rate |
| H/E | hematoxylin/eosin |
| CRP | C reactive protein |
| ALP | alkaline phosphatase |
| ICP-AES | inductively coupled plasma atomic emission spectroscopy |
| FESEM | field emission scanning electron microscopy |
| CatK | cathepsin K |
| XPS | X-ray photoelectron spectroscopy |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Animal Model | No. of Animals and Site of Implant | Materials Characteristics and Functionalization | Experimental Set-up | Main Results | Ref. |
|---|---|---|---|---|---|
| Female homozygous M3 mA ChR KO breeder mice (16-week-old) | 87 female bicortical osteotomy of 1.2 mm in right distal femoral metaphysis | A composite of α-TCP-based HA-forming bone cement containing mesoporous bioactive CaP-SiO2 glass particles (cement/MBG composite) MBG was functionalized by loading with BDNF (84.1 ng/g). | Group I: KO mice treated with cement/MBG composite with BDNF Group II: KO mice treated with cement/MBG composite without BDNF Group III: WT mice treated with cement/MBG composite with BDNF Group IV: WT mice treated with cement/MBG composite without BDNF Experimental times: 35 days -Real-Time RT-PCR on homogenized tissue -Ex vivo microCT -Histology -Histomorphometrical Analysis: -ToF-SIMS, HR-SEM and EDS | Results show effectiveness of BDNF-functionalization but only in WT group. Real-Time RT-PCR: ↑ bone formation and ALP concentration and ↓ CRP levels in OVX mice with cement/MBG composite without BDNF. Histology/histomorphometry: ↑ newly formed bone ToF-SIMS, HR-SEM and EDS: bone formation inside pores of material | [21] |
| Skeletally-mature male Wistar rats (12-weeks old) Orchidectomy surgery OP assessment after 6 weeks: in vivo μCT | 60 rats Femoral condyles bilaterally (diameter: 1.5 mm, depth: 7 mm) | Electrostatic Spray Deposition was used to create a surface coating onto titanium implant of: nCaP crystals: suspension of Ca(CH3COO)2 (0.35 M) by slow addition of an aqueous solution of H3PO4 (0.21 M) nCaP/BP coatings: alendronate sodium trihydrate ≥ 97% powder added to a suspension containing nCaP crystals (concentration 3 mg/mL and weight ratio of 1:10). BP coatings: alendronate sodium powder was dissolved in milli- Q and adjusted with ethanol (final concentration 0.3 mg/mL) | Group I: OVX with non-coated implant Group II: OVX with nCaP implant Group III: OVX with nCaP/BP implant Group IV: OVX with BP implant Group V: SHAM with non-coated implant Group VI: SHAM with nCaP implant Group VII: SHAM with nCaP/BP implant Group VIII: SHAM with BP implant Experimental time: 4 weeks -Ex-vivo microCT -Histology in PMMA -Histomorphometry -Real-Time RT PCR | MicroCT/ histomorphometry: ↑ %BV (mCT) and BA (histomorphometry) in OVX and sham groups with BP coating. ↑ both BIC and BV in nCaP/BP implant vs. nCaP or BPs alone, in OVX and healthy groups. | [22] |
| Female Sprague-Dawley rats (10 weeks old) Ovariectomy OP assessment After 8 weeks: DEXA | 60 rats distal right femoral growth line in the lateral femoral cortex and the metaphyseal cancellous bone filled with 0.25 mL of each material | Strontium enriched calcium phosphate cement (SPC) in the solid phase in comparison to calcium phosphate cement (CPC) | Group I: OVX with CPC material Group II: OVX with SPC material Experimental time: 3 and 6 months -Histology in acrylic resin -Histomorphometry -DEXA | Histomorphometry: ↑ Circumferential contact index for SrPC vs. CPC at 3 months ↑ Ingrowth index for SrPC vs. CPC at 6 months ↑ Implant discontinuities for SrPC vs. CPC at 3 and 6 months | [35] |
| Female Sprague-Dawley rats (12 months old) Ovariectomy | 64 rats Distal femur bilaterally (7–11 granules/defect) | Strontium enriched CaP particles (SCP) realized adopting a surfactant-free mineralization method. Teflon plate with holes in diameter of 1.5 mm and height of 1.5 mm, was used to produce SCP and HA granules. | Group I: OVX with HA doped implants Group II: OVX with SCP doped implants Group III: SHAM with HA doped implants Group IV: SHAM with SCP doped implants Experimental time: 6 and 28 days -Material characterization -Gene expression -Histology | ↑ TNF-α in SHAM and OVX HA group at 6 days; ↑ IL-6 in SHAM SrCP group at 6 and 28 d Similar expression of RANKL ↑ CR and CatK in SHAM and OVX HA group | [36] |
| Female Wistar rats (3 months old) Ovariectomy OP assessment after 10 months: ex vivo microCT in 10 rats | 9 rats drill hole defect of 3 mm × 1.5 mm was made at the proximal end of each femur (two defect sites were made available in each animal) | Strontium enriched (10%) HA micro-granules obtained by with wet precipitation method. | Group I: OVX with HA granules Group II: OVX with SrHA granules Group III: SHAM with HA granules Group IV: SHAM with SrHA granules Experimental time: 8 week -Histology -Histomorphometry | Histomorphometry: ↑ regeneration efficacy in OVX SrHA group ↑ healing efficacy on par with material resorption in SrHA group | [37] |
| Female Sprague-Dawley rats (4-month-old) Ovariectomy and calcium-, phosphorous-, vitamin D3-, soy- and phytoestrogen-free diet | 65 rats After 3 months from OVX surgery, wedge-shaped defect with a lateral height of 4 mm created at the metaphyseal area of the femur | Strontium enriched CPC (total Sr content of 2.21%) in the solid phase. Composites of silica and fibrillar bovine collagen as monolithic gel (B30, 70 wt % silica, 30 wt % colla gen) or as porous scaffold (Sc-B30: B30 particles B30, size < 250 μm, embedded in a collagen matrix with xerogel/matrix weight ratio of 1.0). Composite porous scaffold of 50 wt % silica, 30 wt % fibrillar bovine colla gen and 20 wt % strontium carbonate (Sc-B30Sr20) added to the collagen suspension. | Group I: control Group II: CPC Group III: SrCPC Group IV: BC30- Monolithic xerogels (silica/collagen) Group V: Scaffold xerogels particles B30 Group VI: Scaffold xerogels particles (silica/fibrillar bovine collagen/strontium carbonate) Group VII: Iron foams Group VIII: Iron foam with strontium Group IX: Iron foam with ZOL Experimental time: 6 weeks -dPET-CT | dPET-CT: Sr release from SrCP cements increase bone formation in comparison to CP cement alone as well as the porous scaffold silica/collagen xerogel in comparison to monolithic silica/collagen xerogel | [39] |
| Female Sprague–Dawley rats (1 month old) Ovariectomy | 33 rats Critical-sized defects (6 mm × 6 mm) were created in the calvarial bone. In the scheduled groups, ~325 µL PRP was added to the superior surface containing the osteotomy | Calcium aluminate (CA) disks prepared by a room temperature cast of different sized CA aggregates. Melatonin was chemically attached to CA surface using a two-step deposition process (Ca-Mel). | Group I: CA Group II: CA + PRP Group III: CA-Mel Group IV: CA-Mel + PRP Experimental time: 3 and 6 months. -X-ray -Histology in resin | Histology: ↑ percentage fluorescence in CA-Mel groups vs. all other groups at 6 months ↑ osteoinductive and osteoconductive activity of Ca-Mel scaffold vs. Ca scaffold. | [43] |
| Female Sprague-Dawley rats: Ovariectomy | 36 rats. After 12 weeks from OVX surgery, two different implants (n = 72) were inserted into the distal tibia | Porous Ti implant (2.2 mm × 4 mm) coated with HA and HA-Simvastatin (HA-Sim) applying an electrochemical deposition process. | Group I: HA coating Group II: HA + Sim coating Group III: control Experimental time: 2, 4 and 12 weeks -Histology and Histomorphometry | Histomorphometry: ↑ BIC percentage in HA/Simvastatin group vs. other groups at 12 weeks | [45] |
| Wistar Crl: WI (Han) rats female, retired breeders (8–10 months old): Ovariectomy, OP assessment after 7 months: pQCT | 18 rats. 8 weeks after OVX surgery subcutaneously injection of vehicle/ALN; 13 weeks after OVX surgery critical size defect (5 mm) | BMP2 or L51P were loaded onto β-TCP cylinders by physical immobilization (adsorption). | Group I: unloaded Group II: 1 µg BMP2 Group III: 10 µg BMP2 Group IV: 10 µg L51P Group V: 1 µg BMP2/10 µg L51P Experimental time: 16 weeks -X-ray -ex vivo microCT -Histology -Histomorphometry | Histomorphometry: ↑ bone volume and ↓ βTCP in group V ↓ βTCP turnover after ALN administration | [50] |
| Mature female Wistar rats (3 months old) Ovariectomy + low calcium diet OP assessment after 6 weeks with in vivo microCT in 6 animals | 32 rats. Bone defect created bilaterally longitudinal to the axis of the femur | CPC/PLGA composite cylinders made of 70 wt % a-TCP powder and 30 wt % PLGA powder, containing both a lactic and glycolic weight percentage of 50% and 0.5% carboxymethylcellulose (CMC). | Group I: OVX with Bio-Oss® granules Group II: OVX with CPC/PLGA cylinders Group III: SHAM with Bio-Oss® granules Group IV: SHAM with CPC/PLGA cylinders Experimental time: 4 and 1 weeks -Fluorescence analysis -Ex vivo microCT -Histology -Histomorphometry | Histomorphometry: ↑ Bio- Oss degradation in comparison to CPC/PLGA both in SHAM and OVX ↑ bone formation from the centre of the defect with Bio- Oss in comparison to CPC/PLGA both in SHAM and OVX | [40] |
| Female Wistar rats (12 weeks old) Ovariectomy | 30 rats After 4 weeks from OVX surgery, implantation in proximal tibial growth plate | Composite of biodegradable PLGA with b-TCP screws (1.6 mm × 4 mm) | Group I: SHAM group Group II: OVX group Group III: PLGA only group Group IV: PLGA/βTCP group Experimental time: 25 weeks -Ex vivo microCT -Histology in paraffin | MicroCT: ↑ BMD, BV/TV and Tb.N ↓ Tb.Th and Tb.Sp in sham group. ↑ BMD in OVX/CSR group ↑ BV/TV and Tb.N values ↓ Tb.Sp than OVX and OVX/BSR | [42] |
| Virgin female Wistar rats (17 weeks old) Ovariectomy OP assessment 1 day before treatment: in vivo microCT | 8 rats. After 5 weeks from OVX surgery, implantation of miniature screw in femoral condyles bilaterally (same implants for each animal). | NanoHA particles added to an aqueous solution of zoledronate (nHA:zoledronate ratio of 100:1). Hydrogel composed by hyaluronan derivative and PVA crosslinker was used to deliver nHA-zoledronate, nHA or zolendronate. | Group I:nHA-Gel Group II:nHA-Zol-Gel Group III: Zol-Gel Group IV: Gel Experimental time: 58 weeks -In vivo microCT -Histology | Histology: ↑ MV/TV in nHA-Gel vs. Gel alone ↑ MV/TV in nHA-Zol-Gel vs. Gel alone ZOL-loaded nHA further inhibited a degradation of the mineralized hydrogel as well as a resorption of the peri-implant bone as effectively as unbound ZOL. | [24] |
| Female Sprague-Dawley (three-month-old) Ovariectomy After 12 weeks OP assessmentwith histology in 4 rats | 32 rats Bilateral implantation in femoral medullary cavity | Ti rods (1.1 mm × 12 mm) and disks (9 mm × 1 mm) surfaced functionalized with Zolendronate HA coating (ZnHA) realized with sol-gel dip technique. | Group I: Zn coated Ti implant Group II: ZnHA coated Ti implant Experimental time: 6 and 12 weeks -Material characterization -Histology in PMMA -Histomorphometry -MicroCT -Mechanical tests | Histology/histomorphometry: ↑ MAR, BA and BIC values in ZnHA coating group vs. HA coated group ↑ bone mass formation around the implant ↑ strength of osseointegration values in ZnHA coating group vs. HA coated group MicroCT analysis: ↑ BV/TV and OI% in ZnHA coating group vs. HA coated group Mechanical tests: ↑ maximum force and interfacial shear strenght in ZnHA coating group vs. HA coated group | [25] |
| Female Sprague Dawley rat (3 months old) Ovariectomy (12 weeks) | 18 rats Bilateral implantation in femoral medullary cavity | Ti implants (1.2 mm) surfaced functionalized with Magnesium HA (MgHA) realized with sol-gel dip-coating method (10 mol% Ca2+ replaced by Mg2+). | Group I: MgHA coated implant Group II: HA coated implant Experimental time: 12 weeks -Material characterization -Histology -Histomorphometry -Ex vivo microCT -Mechanical tests | Histology: ↑ osteointegration and bone formation in MgHA group Ex vivo microCT: ↑ BV/TV, Tb.N, Tb.Th, Conn.D. and %OI Mechanical tests: ↑ maximum force and interfacial shear strenght in MgHA group | [26] |
| Female Sprague Dawley (3-month-old) Ovariectomy | 20 rats After 12 weeks from OVX surgery, bilateral implantation in femoral medullary cavity | HA and 10% Strontium enriched HA (HA with 10 mol% calcium substituted by strontium) were obtained with chemical co-precipitation method. | Group I: HA coated implant Group II: 10% SrHA coated implant Experimental time: 8 weeks -Material characterization -Ex vivo microCT -Histology in paraffin -Histomorphometry | Ex vivo microCT: ↑ Tb.N and Tb.Th in 10% Sr HA coating group vs. HA coating alone ↓ Tb.Sp in 10% Sr HA coating group vs. HA coating alone Histomorphometry: ↑ BV, BIC in 10% Sr HA coating group vs. HA coating alone | [27] |
| Female Sprague Dawley rats (3-month-old) Ovariectomy Zol administration (1.5 lg/kg weekly) for 12 weeks | 26 rats After 12 weeks from OVX surgery, bilateral implantation in femoral medullary cavity | HA and 10% Strontium HA enriched (HA with 10 mol% calcium substituted by strontium) were obtained with chemical co-precipitation method. Previous treatment with BPs | Group I: HA coated implant Group II: 10% SrHA coated implant Experimental time: 8 weeks -Material characterization -Ex vivo microCT -Histology -Histomorphometry | Ex vivo microCT: ↑ Tb.N and Tb.Th in 10% Sr HA coating group vs. HA coating alone ↓ Tb.Sp in 10% Sr HA coating group vs. HA coating alone Histomorphometry ↑ BV, BA in 10% Sr HA coating group vs. HA coating alone | [28] |
| Female Sprague–Dawley (6-month-old) Ovariectomy After 12 weeks OP assessment with microCT | Animals number not reported. 6 months after OVX surgery, bilateral implantation at the medial aspect of the tibial shaft. | Lithium enriched calcium phosphate cement in the liquid phase (Li/CPC) and realized as cylindrical implant (2.5 × 4). | Group I: OVX with Li/CPC-100 Group II: OVX with CPC Experimental time: 4 and 8 weeks -Material characterization -Ex vivo microCT -Histology | Ex vivo microCT: ↑ BV/TV in Li/CPC-100 vs. CPC alone Histology: greater osteoconductivity and osseointegration in Li/CPC group vs. CPC alone | [44] |
| Female Sprague-Dawley rats Bilateral ovariectomy (3 months) | 36 rats Full-thickness 5 mm diameter round bone defect made on each side of the mandible | Genetically modify BMSCs for OPG overexpression seeded at 2 × 105 cm−2 concentration onto HA scaffold (5 mm × 1 mm) | Group I: HA Group II: BMSC/HA Group III: OPG-BMSC/HA Experimental times: 4, 6 and 8 weeks -Ex vivo microCT -Histology in PMMA -Immunohistochemistry | Ex vivo microCT: ↑ MV/TV in OPG-BMSC/HA group at the longest experimental times Histology: ↑ mineralized new bone in OPG-BMSC/HA group ↓ number of osteoclasts in OPG-BMSC/HA group | [49] |
| Female Sprague-Dawley rats (10 and 11 months old) Ovariectomy After 3 months OP assessment with microCT: BMD | 42 rats Bilateral implantation in the median aspect of the tibial shaft, below the tibial plateau. | β-TCP, calcium silicate (CS) and 10% Strontium enriched CS (Sr-CS) (3 mm × 3 mm) obtained by a chemical precipitation method. | Group I: Blank Group II: β-TCP Group III: CS Group IV: Sr-CS Experimental times: 3 days, 1, 4 and 9 weeks -Material characterization EDX and SEM -Detection of in vivo µe-pH -MicroCT -Histology | MicroCT: ↑ VNB/TV in CS and Sr-CS groups Histology: ↓ TRAP staining positivity in CS and Sr-CS groups Alkaline materials induce an increase in µe-pH, which is associated with higher bone formation and delay in osteoclasts activity. Residual materials is detectable up to the latest experimental time. | [48] |
| Female Sprague-Dawley rats (8 weeks old) Ovariectomy (3 months) | 20 rats 3 months after OVX surgery, bilateral implantation in the proximal metaphyseal region of the tibiae. | Titanium screw coated with a biomimetic CaP coating onto which Zolendronate was immobilized by dipping at different concentration (0, 8, 80 and 800 µg/mL). | Group I: control Group II: 8 µg/mL Group III: 80 µg/mL Group IV: 800 µg/mL Experimental times: 8 weeks -Material characterization -Histology -Histomorphometry -Ex vivo microCT | Histomorphometry: ↑ BV% in group IV, no differences in BIC% between groups | [23] |
| Female Sprague Dawley (12 weeks old) Ovariectomy | Animals number not reported 4 weeks after OVX surgery, implantation in the lateral femoral condyle | Alendronate enriched nHA (HA-AL), Fe3O4 enriched nHA (HAFe) and Alendronate/ Fe3O4 enriched nHA crystals synthesized by a wet chemical technique. Spiral-cylindrical scaffolds (2.5 mm × 3 mm) were obtained by a solvent-casting/particle-leaching using polycaprolactone as polymer matrix. | Group I: Blank Group II: PCL Group III: HA Group IV: HA-AL2 Group V: HA-Fe10 Group VI: HA-AL2-Fe10 Experimental times: 4 weeks -MicroCT -Histology -Immunohistochemistry | MicroCT: ↑ BMD, BV/TV, Conn.D, Tb.Th, Tb.N in HA-AL2, HA-Fe10 and HA-AL2-Fe10 groups vs. HA group ↓ Tb.Sp in HA-AL2, HA-Fe10 and HA-AL2-Fe10 groups vs. HA group. Histology: Func-HA induces bone regeneration and integration, increasing Coll and reducing osteoclasts activity. | [41] |
| Female Sprague-Dawley rats (3 months old) Ovariectomy OP assessment after 12 weeks: ex-vivo microCT in 5 ovx and 5 sham | 50 rats. Implantation in the femoral medullary canal after marrow ablation. all OVX rats from the first two groups received HA-coated implants and those from latter two groups got Sr-HA ones. | Titanium screws (1 mm × 2 mm) coated with 10% Strontium enriched HA titanium implant via electrochemical deposition + intermittent administration of human PTH (1–34) (60 mg/kg, 3 times a week) | Group I: Sr Group II: PTH Group III: PTH/Sr Experimental times: 12 weeks -Ex vivo microCT -Mechanical test -Histology -Histomoprhometry | microCT: ↑ BV/TV, Tb.Th, Tb.N in PTH + Sr group ↓ in PTH + Sr group Histomorphometry: ↑ BAR and BIC % in PTH + Sr group Mechanical test: ↑ push out force in PTH + Sr group | [30] |
| Female Sprague Dawley rats (3 months old) Ovariectomy OP assessment after 12 weeks: ex-vivo microCT in 5 ovx and 5 sham | 50 rats Implantation in the femoral medullary canal after marrow ablation. | Titanium implants (1.2 mm × 15 mm) coated with Strontium enriched HA (Sr-HA) coating at different contents via electrochemical deposition. | Group I: HA Group II: 5% Sr-HA Group III: 10% Sr-HA Group IV: 20% Sr-HA Experimental times: 12 weeks -Material characterization -Ex-vivo microCT -Mechanical test -Histology -Histomorphometry | MicroCT: ↑ BV/TV, Tb.Th, Tb.N, Conn.D in 10 and 20% SrHA groups ↓ Tb.Sp. in 10% and 20% SrHA groups Histomorphometry: ↑ BAR and BIC % in 10% and 20% SrHA groups Mechanical test: ↑ push out force in 10% and 20% SrHA groups | [29] |
| Female Sprague Dawley rats (3 months old) Ovariectomy OP assessment after 12 weeks: ex-vivo microCT in 5 ovx and 5 sham | 50 rats Implantation in the femoral medullary canal after marrow ablation. | Titanium implants (1 mm × 2 mm) coated with Strontium enriched HA (Sr-HA) or zinc enriched HA (Zn-HA) or Magnesium enriched HA (Mg-HA) coating via electrochemical deposition. | Group I: HA Group II: Zn-HA Group III: Mg-HA Group IV: Sr-HA Experimental times: 12 weeks -Material characterization -Ex-vivo microCT -Mechanical test -Histology -Histomorphometry | MicroCT: ↑ BV/TV, Tb.Th, Tb.N, Conn.D in SrHA group ↓ Tb.Sp. in SrHA group Histomorphometry: ↑ BAR and BIC % in SrHA group Mechanical test: ↑ push out force in SrHA group | [33] |
| Female Sprague Dawley rats (three months old) Ovariectomy OP assessment after 12 weeks: ex-vivo microCT | 70 rats Creation of femoral cylindrical defects above the distal epiphyseal growth plate | Strontium enriched Calcium Phosphate cement (SCPC) (3 mm × 5 mm) in the solid phase combined with single-dose local administration of BMP-2 (BSCPC) | Group I: Control Group II: CPC Group III: SCPC Group IV: BSCPC Experimental times: 8 weeks -Ex-vivo microCT -Biomechanical testing -Histology | MicroCT: ↑ BV/TV, Tb.Th, Tb.N, in BSCPC group ↓ Tb.Sp. in BSCPC group Histology: ↑ new bone formation % in BSCPC group ↓ remaining materials % in BSCPC group Mechanical test: ↑ Ultimate load in BSCPC group | [34] |
| Female Sprague Dawley rats (10 weeks olds) Ovariectomy + low Ca-, P- and vit D3- and soy- and phytoestrogen-free multi-deficient diet (12 weeks) | 45 rats After 12 weeks from OVX surgery, creation of 4 mm defect in the distal femur metaphysis | Strontium enriched Calcium Phosphate Cement (SrCPC) in the solid phase compared to CPC | Group I: Control empty Group II: CPC Group III: SrCPC Experimental times: 6 weeks -TOF-SIMS analysis -Histology -Histomorphometry -Immunohistochemistry | Histomorphometry: ↑ BV/TV (defect region) in SrCPC vs. other groups ↑ BV/TV (implant region) in SrCPC vs. CPC ↑ Ma/Tb.Ar (defect region) in SrCPC vs. other groups ↑ Ma/Tb.Ar (implant region) in SrCPC vs. CPC | [38] |
| Female Wistar rats (3 months old) Ovariectomy + low calcium diet (6 weeks) | 20 rats After 6 weeks from OVX surgery, bilaterally creation of defects in femoral condyles (2.5 mm × 5 mm) | Calcium Phosphate Cement (CPC)/Poly(DL-lactic-co-glycolic acid) PLGA composite in comparison with Alendronate enriched CPC/PLGA composite in the liquid phase (CPC/PLGA-ALN). | Group I: CPC/PLGA-blank Group II: CPC/PLGA-lowALN Experimental times: 4 and 12 weeks -Material characterization -Bone dynamics analysis -Ex vivo microCT -Histology -Histomorphometry | Bone dynamics analysis: ↑ calcein green within ROI for CPC/PLGA-blank vs. CPC/PLGA-lowALN ↑ calcein green in the eROI for CPC/PLGA-lowALN vs CPC/PLGA-blank Histomorphometry: ↑ bone formation within ROI from 4 to 12 weeks for both CPC/PLGA-blank and CPC/PLGA-lowALN ↓ bone formation over time in the ROI for CPC/PLGA-blank ↑ bone formation over time for CPC/PLGA-lowALN ↓ material remnants CPC/PLGA-blank ↑ bone at 12 weeks in the ROI for CPC/PLGA-low ALN vs. CPC/PLGA-blank | [40] |
| Female Sprague Dawley rats (3 months old) Ovariectomy | 36 rats Bilateral critical-sized defect in calvaria (5 mm Ø) | CPC scaffold (5 mm × 3 mm) loaded with Icariin at concentrations of 0, 20, 200 or 2000 μM (CPC-ICA) and lyophilized + seeding with autologous BMSCs. | Group I: CPC Group II: CPC/ICA-2000 Group III: CPC/ ICA-ig 5 mm Group IV: CPC/ICA-200 + ICA-ig Experimental times: 8 weeks -Serum dosage: Ca, Pi and ALP activity -DEXA -Biomechanical parameters -Histology (with fluorescent labelling) -Microfil perfusion | Fluorescent labelling: ↑ fluorescent staining in CPC/ICA-2000 + ICA-ig Microfil perfusion: ↑ new vessels formation in CPC/ICA-2000 + ICA-ig Histology: ↑ new bone % in CPC/ICA-2000 + ICA-ig | [46] |
| Female Sprague- Dawley rats (16 weeks old) Ovariectomy After 3 months, OP assessment | 20 rats Bilateral critical-sized defect in calvaria (5 mm Ø) | Akermanite powders (Ca2MgSi2O7) were synthesized by a sol-gel process, while β-TCP powders synthesized by chemical precipitation. Scaffolds were obtained (5 × 3) adopting polyethylene glycol (PEG) particulates as porogens. | Group I: β-TCP Group II: Akermanite Experimental times: 8 weeks -Material characterization -Ex vivo microCT -Histology in PMMA -Fluorescent labelling -Gene expression | Ex vivo microCT: ↑ BV/TV and Tb.Th in Akermanite group Histology: ↓ Trap positivity in akermanite group ↑ Bone formation % in akermanite group ↑ MAR% and fluorescence positivity in akermanite group Gene expression: ↑ RUNX2, OCN, OPG, TRA, CD31 expression in akermanite group | [47] |
| Female Sprague–Dawley rats (8 months old) Ovariectomy After 3 months, OP assessment | 72 rats Creation of a bilateral defect in distal end of the femur and materials injection in the femoral bone marrow space | CaP particles enriched with trace elements (te) (silicon, zinc and strontium ions) and synthesized in simulated body fluid (teCaP) | Group I: Sham-Ctrl Group II: Sham-CaP Group III: Sham-teCaP Group IV: OVX-Ctrl Group V: OVX-CaP Group VI: OVX-teCaP Experimental times: 2 and 3 months -DEXA -Ex vivo microCT -Biomechanical test -Femoral bone element analysis -Histology | Ex vivo microCT: ↑ BV/TV, BSA/BV, Tb.Tn. in OVX-teCaP gropus vs. other OVX groups ↓ Tb.Sp in OVX-teCaP gropus vs. other OVX groups | [32] |
| Female Sprague–Dawley rats (3 months old) Ovariectomy | 36 rats After 12 weeks, creation of defect in the proximal tibia. | Titanium implants (2 mm × 6 mm) coated with HA or Zn/Mg/Sr enriched HA via electrochemical deposition. | Group I: HA coating Group II: Zn-HA Group III: Mg-HA Group IV: Sr-HA Experimental times: 4, 8, 12 weeks -Material characterization -Histology -Histomorphometry | Histomorphometry ↑ BIC% in Zn-HA vs. HA at 4 weeks ↑ BIC% in Sr-HA vs. HA at 8 and 12 weeks ↑ BA% in Zn-HA and SR-HA at 8 and 12 weeks | [31] |
| Animal Model | No. of Animals and Site of Implant | Materials Characteristics and Functionalization | Experimental Set-up | Main Results | Ref. |
|---|---|---|---|---|---|
| Rabbit | |||||
| New Zealand rabbits (~6 months) ovariectomized + methylprednisolone injection for 28 d | 30 rabbits with defects created in epiphysis of the right medial tibia (d = 6 mm, ø = 3 mm) | A composite material made of Calcium silicate powder (50 wt % of Ca2SiO4 and 50 wt % of Ca3SiO5) Risedronate Calcium Phosphate Silicate Cements (RA-CPSC), 10 wt % of monocalcium phosphate (MCP, Ca(H2PO4)2 and 0.5 wt % or 1.0 wt % of risedronate added into calcium silicate powder and homogeneously mixed respectively. | Group I: CPCS Group II: RA-CPCS 0.5% Group III: sham control Experimental time: 8 weeks and 10 weeks -X-ray semi-quantitative analysis -CR array analysis | X-ray ↑ Trabecular bone formation with X-ray in Group II in comparison to Group I after 10 weeks PCR analysis ↑ up-regulation of genes in Group II in comparison with Group I | [51] |
| Osteoporosis induced with daily injected with MPS hemisuccinate for 4 consecutive weeks OP assessment: DEXA | Lateral and medial defects (4 mm diameter 3–4 mm deep) in the both distal femoral epiphysis | Mesoporous silica (SBA15) 100% SiO2 surface was chemically modified with an organic modification of silica walls with alkoxysilane, n-octyltriethoxysilane (C8) and functionalized by soaking the mesoporous in a solution of PTHrP (107–111) (osteostatin) in PBS | Group I: SBA15 Group II: PTHrP + SBA15 Group III: SBA15 + C8 Group IV: PTHrP + SBA15 + C8 Experimental time: 2 weeks -Histology and Immunohistochemistry | No inflammation. ↑ staining for PCNA, Runx2, osteopontin, and/or VEGF in OVX rabbits in both Group II and IV | [56] |
| Female ovariectomized New Zealand rabbits (4.6 ± 0.5 kg) | After 6 months from ovariectomy, in 60 rabbits, two sub-periosteal mandibular defects (4 mm × 5 mm × 10 mm) | Porous commercial HA (approximate porosity: 40%, pore size: 5–500 μm, compressive strength: 15 MPa) was physically functionalized in surface with or without 10 μg of APN or 100 μL Matrigel or combination of both. | Group I: APN + Matrigel + HA Group II: APN + HA Group III: Matrigel + HA Group IV: HA Experimental time: 4 weeks -Histomorphometric analysis -Micro-CT analysis -Biomechanical analyses | Histological analyses ↓ TRAP activity in Group I than other groups ↑ NBV in Group I than the other groups micro-CT analysis ↑ BV/TV, Conn.D, Tb.Th and Tb.N. in Group I than other groups ↓ Tb.Sp in Group I than other groups biomechanical analyses ↑ compressive strength and elastic modulus in Group I than other groups | [57] |
| New Zealand OVX white rabbits by administering corticosteroids (1.5 mg/kg/day) for 28 d | 42 rabbits with steel cancellous bones screws (ø = 4 mm, h = 10 mm) implanted bilaterally in the medial femoral condyles with or without augmentation with HA and Fibronectin loaded HA | Physical incorporation of fibronectin in HA bulk material by adding 240 mg of HA to a solution containing 3.6 mg of fibronectin in PBS. | Group I: augmentation with fibronectin loaded HA Group II: augmentation with HA Group III: no augmentation Experimental time: 24 h, 48 h and 5 dys -Micro-CT analysis -Histological analysis | micro-CT analysis: ↑ Tb.Th in Group I in the area next the screw in comparison with area far from the device Histological analysis: ↑ cellularity at 24 h in Group I than the other Groups | [58] |
| Female New Zealand white rabbits (about 2.5kg) ovariectomized OP assessment after 3 months in 3 healthy and 3 OVX rabbits: microCT ex vivo and histology | After 3 months from ovariectomy in 43 rabbits implantation into the femoral epiphysis | TNT were immersed in supersaturated Ca(OH)2 solution, Ca(NO3)2·4H2O (0.2 M) and (NH4)2HPO4 (0.2 M) solutions to create a coating of HA. TNT-HA was subsequently functionalized with Aln by immersion in Aln solution (physical absorption). | Group I: Ti Group II: TNT Group III: TNT-HA Group IV: TNT-HA-Aln Experimental time: 12 weeks -X-rays -Micro-CT -Push out analysis -Histological analyses | X-rays and micro-CT: no dislocation and inflammation occurred. ↑ BV/TV and Tb.Th in Group IV and III than Group I and II Push out: ↑ interfacial strength in Group IV than other groups ↑ interfacial strength in Group III than Group I and II Histological analyses: ↑ Osteoid tissue in Group IV and III than other Groups. | [52] |
| New Zealand White rabbits (6-month old; ca. 3 kg) ovariectomized | Bilateral screw implantation in distal femurs of 16 rabbits | A composite material was realized creating a Strontium enriched CPC in the solid phase and PCL (poly e-caprolactone). | Group I: PCL Group II: CPC/PCL Group III: Sr-CPC/PCL Experimental time: 24 weeks -Micro-CT analysis | Micro-CT analysis: ↑ BV/TV, Tb.Th, Tb.N, connectivity density in Group III than Group I ↓ Tb.Sp, SMI and total porosity in Group III than Group I ↓ Tb.Sp in Group III than Group II | [53] |
| Female New Zealand white rabbits (90–100 days old, 2–2.5 kg) ovariectomized + MPS sodium succinate (1.0 mg/kg/day) injections for 4 consecutive months | Bilateral implants in 40 rabbits: two implants (2-mm diameter, 10-mm depth) into each femur | Ti–6Al–4V implants (ø10 × 2 mm) coated by means of plasma-spray technique with HA or CaSiO3 or zinc-modified calcium silicate (Ca2ZnSi2O7) at two different Zn contents (coating thickness about 170 μm) | Group I: uncoated Ti–6Al–4V Group II: HA-coated Ti–6Al–4V, Group III: CaSiO3-coated Ti–6Al–4V, Group IV: Ca2ZnSi2O7 -coated Ti–6Al–4V (Zn–Ca 0.1) Group V: Ca2ZnSi2O7-coated Ti–6Al–4V (Zn–Ca 0.3) Experimental time: 4, 8 and 12 weeks -Micro-CT analysis -Histological analysis | Micro-CT analysis: all parameters ↑ from 4 to 8 weeks ↑ highest values of all parameters in Group V than all other Groups Histological analysis: No new bone in Group I Small bone in Group II and III stating from 4 weeks Strong new bone formation in Group IV and V and improved osteointegration | [55] |
| California rabbits (eight months old) ovariectomy + i.m. administration of methylprednisolone (1 mg/kg/day) for 6 weeks | 30 rabbits in which defect created in the right (5 mm wide and 4 mm) 20 OVX and 10 healthy as control | A composite material of HAP/TCP (23 wt % HAP and 77 wt % TCP) granules with or without 5% Sr substitution. Micro porosity and grain size of granules were in the range from 400 to 1 μm. The measured specific surface area of the prepared granules was 0.56 m2/g. Determined bulk density of the granules was 1.28 g/cm3. | Group I: healthy bone (10 animals) Group II: biphasic ceramic granules of HAP/TCP 30/70 (7 animals); Group III: HAP/TCP + 5% strontium (7 animals) Group IV: sham (6 animals) Experimental time: 12 weeks -Histomorphometry -Immunohistochemistry | Histomorphometry ↑ Greater mean trabecular area in Group I in comparison to other groups Immunohistochemistry ↑ increase of NFkB, OPG, OC, BMP 2/4, COL-1α and IL-1 in Group III in comparison to Group IV. | [54] |
| Ovine Model | |||||
| Goat ovariectomy + low-calcium diet for 3 mthsAdditional 6 mos for OP development, confirmed with BMD, prior of surgery. | 3 Chinese goats with a total of 24 defects. In each goats 8 cylindrical defects with a diameter of 8 mm were created:
| Nanocrystalline paste (Ostim®, Germany) suspension of pure HA in water prepared by a wet chemical reaction. needle shaped HA crystals with a size of 21 nm in a-direction and of 36 nm in c-direction form agglomerates. Pure HA and an average crystallite size of 18 nm. The atomic ratio of calcium: phosphorus is 1.67. | Group I: empty defects; Group II: nanoparticulate hydroxyapatite; Group III: nanoparticulatehydroxyapatite + collagen type I. Experimental time: 6 weeks -High-resolution peripheral quantitative computed tomography (HR-pQCT) -Histomorphometry | Osteoporosis confirmed by BMD (pQCT) at each calcaneus (loss of 24% ± 2% of the initial BMD). HR-pQCT: ↑ BV/TV in Group II in comparison to Group I and Group III within 1mm; ↓ Tb.Sp Group II in comparison to Group I and Group III within 1mm; ↑ Conn.D and Tb.N in Group III in comparison to Group I and Group II. Histomorphometry ↑ new bone formation (initial defect region) in Group II and Group III in comparison to Group I | [65] |
| Skeletally mature female sheeps ovariectomy + daily treatment for 6 months with MPS. 4 weeks before surgery gradual reduction in GC and 1 week before no GC treatment. | 10 sheep. Defects (10 mm × 12 mm) created laterally and medially into the bone of distal femurs bilaterally. 4 implants/sheep: 40 implants. Defects were filled with cylindrical Ti plasma sprayed pin. Around the Ti, the circumferential gap of 2 mm filled with one of the experimental materials. | -HA/βTCP (70:30%) with a Ø ~ 500–1400 μm, ~80% porosity; pore size of the composite was 300–700 μm and interconnecting pore size was 100–200 μm. -HA/βTCP-HyA granules infiltrated with biopolymer HyA (~80% porosity); -HA/βTCP added an ultra-thin layer of 10% PDLLA (50% D-PLA, 50% L-PLA) with a porosity ~70% | Group I: allograft from healthy sheep (control) Group II: uncoated HA/βTCP Group III: HA/βTCP-PDLLA Group IV: HA/βTCP–HyA Experimental time: 12 weeks -Histomorphometry -Push-out test | ↑ bone marrow was statistically significantly larger in the allograft group (ROI-1 and ROI-2) compared with the other groups Histomorphometry ↑ BV/TV in Group I in comparison with Group II ↑ Bone marrow in Group I (ROI-1 and ROI-2) compared with the other Groups | [63] |
| Skeletally mature female sheep ovariectomy + calcium deficient diet. OP assessment after 10 months: microCT in the hind limb | 10 sheep: 8 for the OVX group 2 as control CTR Cylindrical implants (12 mm × 4 mm) cortical bone defect (12 mm × 4 mm) | 10% Strontium/Hydroxyapatite (SrHA)–Ca9Sr(PO4)6(OH)2and Control scaffold–Hydroxyapatite (HA)–Ca10(PO4)6(OH)2 synthesized by wet precipitation method ADMSC isolated from subcutaneous fat pad of control sheep used to functionalize SrHA (cSrHA) e HA (cHA). | Group I: SrHA Group II: HA Group III: cSrHA Group IV: cHA Experimental time: 8 weeks -EDX -Micro-computed tomography -Histomorphometry | Micro-computed tomography ↑ Bv/Tv in Group III than Group IV and Group I. Histomorphometry: ↑ de novo bone formation in Group III, followed by Group IV. Group I exhibited a RE ratio of 0.24 ± 0.04 and Group II exhibited the least RE | [66] |
| Aged osteopenic sheep (6–10 years) | Vertebral defects (diameter: 5 mm × 14 mm):
24 sheep were treated with CPC + fibers + BB-1 100 and 500 μg BB-1 (12 sheep at 3 months and 12 sheep at 9 months). | Powder of a commercially bone cement mixed with 10% fiber content of poly(l-lactide-co-glycolide, PLGA) acid fibers (diameter of 25 μm) Lyophilized BB1 was dissolved in the liquid and added to the cement reinforced powder. | Group I: L1 untouched (control); Group II: L4 injected with CPC + fibers; Group III: L5 injected with CPC + fibers +BB-1 (5, 100 and 500 μg); Group IV: L3 injected with pure CPC (only for comparison with selected parameters) Experimental time: 12 and 36 weeks -Measurement of BMD -Micro-CT -Static and dynamic histomorphometry -Biomechanical compressive strength | ↑ BMD in Group II and III vs Group I in all groups; ↓ BMD for Group II and III from 12 to 36 weeks, with a significant difference for Group III at 500 μg. Micro-computed tomography ↑ BV/TV in Group II and III vs. Group I; ↑ BV/TV in Group III (500 μg) vs. Group II ↑ BV/TV TV in Group II and III vs. Group I in all groups; ↑ BV/TV also in Group IV vs. Group I; ↑ BV/TV values for Group III vs. Group II and Group IV for all doses of BB-1; Significant differences between Group III and Group II for 5 and 100 μg BB-1 at 3 months and for 500 μg BB-1 at 9 months; Significant differences between Group III and Group IV for 500 μg at 3 months, as well as for 100 and 500 μg BB-1 at 9 months | [59] |
| Aged osteopenic (6–9 years old) | Forty four sheep in which vertebral defects (diameter 5 mm × 14 mm) were created:
| CPC powder was mixed with 10% poly (l-lactide-co-glycolide) acid (PLGA) fibers. BMP-2 was dissolved and added to the cement powder. | Group I: L1 untouched (control); Group II: L4 injected with CPC + fibers; Group III: L5 injected with CPC + fibers+BMP-2 (1, 5 and 100 μg); Experimental time: 12 and 36 weeks -Measurement of BMD -Analysis of bone structure with -Micro-CT -Static and dynamic histomorphometry -Biomechanical compressive strength | ↑ BMD in Group II and III vs. Group I at 12 and 36 weeks; Micro-computed tomography ↑ BV/TV in Group II and Group III vs. Group I at all distances from the edge of the drill channel ↑ BV/TV between Group III and Group II at 36 weeks for 100 μg of BMP-2 Static and dynamic histomorphometry: ↑ BV/TV in Group II and Group III vs. Group I; ↑ BV/TV in Group III vs. Group II for all doses of BMP-2. ↓ effects from 1 and 5 to 100 and 500 μg BMP-2 at 3 months ↑ BV/TV, all 3-month and 9-month Tb.Th values for Group III vs those for Group II for all doses of BMP-2 ↓ Tb.N in Group II and III vs Group I in all groups | [60] |
| Sheep (4 years old) ovariectomy + low-calcium diet + corticosteroids administration (500 mg MPS via i.m. injection every 3 weeks) | 6 sheep with 6 cylindrical defects each (10 mm × 13 mm) created in the cancellous bone after 6 months of:
| Ti6Al4V ELI cylinders (1 cm × 1 cm) with a macroporous structures obtained with EBM technique (pores of 2 mm Ø and wall thickness ~700–800 μm). Si enriched HA coating were realized (Si-HA) followed by a dip-coating process and adsorption and immobilization of VEGF by means a non-covalent binding with 5 μg/mL of VEGF-A. | Group I: Ti6Al4V-ELI (Ti) Group II: Ti6Al4V -ELI + adsorbed VEGF (Ti-VEGF) Group III: Ti6Al4V-ELI + coated with Si-HA (Ti@SiHA) Group IV: Ti6Al4V-ELI + coated with Si-HA and adsorbed VEGF (Ti@SiHA-VEGF) Experimental time: 12 weeks -Physico-chemical characterization -Histomorphometry | Histomorphometry ↑ Bone formation in Group IV in comparison with other Groups ↑ Vessel formation in Group IV in comparison with Group III | [64] |
| Sheep (4 years old) ovariectomy + low calcium and low vitamin D diet + corticosteroids administration (500 mg MPS via i.m. injection every 3 weeks starting 2 weeks post-OVX) OP assessment after 4 months: DEXA | Six sheep in which 2.0 cm diameter defect was created in lumbar vertebrae L2 and L4. Knitted OptiMesh sac was inserted into the vertebral defect. rhNELL-1 was implanted at 0.09 mg in L2 and at 2.25 mg in L4 (n = 3 sheep). Control materials were implanted in the 3 remaining sheep. | Control materials: hyaluronic acid (HA) and hydroxyapatite-coated β-tricalcium phosphate (β-TCP with granule size: 50 μm, pore size: 10 μm, mixed with 500 μm hydroxyapatite). Treatment materials: rhNELL-1 protein lyophilized onto b-TCP mixed into the HA, for protein release at two doses (0.9 and 2.25 mg) | Group I: control (HA and β-TCP) Group II: HA/β-TCP + rhNELL-1 0.09 mg Group III: HA/β-TCP + rhNELL-1 2.25 mg Experimental time: 12 weeks -Measurement of BMD -MicroCT -Histomorphometry | Measurement of BMD ↑ BMD in Group II and Group III vs. Group I Micro-computed tomography ↑ BV/TV, Tb.N and Tb.Sp in Group II and Group III vs. Group I Histomorphometry: ↑ endocortical bone formation (Ct. Wi), Tb. Area and Tb. N in Group II and Group III vs. Group I ↓ Tb.Sp. in Group II and Group III dose dependent vs. Group I ↑ Ob. N significantly increased in Group III; ↓ Oc. N significant decrease in a dose manner in Group II and Group III. | [61] |
| Sheep ovariectomized OP assessment: sampling of Iliac crest biopsy the time of ovariectomy and 6 months later during the lumbar procedure | Twelve adult sheep (6 ovariectomized and 6 healthy as control) with lumbar vertebral bodies defects (8 mm high × 10 mm deep 20 mm long), created into the L3 and L4 vertebral bodies | Alendronate enriched Calcium Deficient Apatite (CDA) in the solid phase. | Group I: CDA in L3 Group II: Al-CDA in L4 Group III: no surger Experimental time: 12 weeks -MicroCT | Micro-computed tomography ↑ BV/TV in Group II vs. Group III ↑ BV/TV (+6.8%) and TbTh (+10.5%) until 1.2 mm and TbSp until 0.8 mm from the implant in Group II vs. Group I. ↑ TbN and TbPf in Group II. ↑ cortical thickness (+43%) in vertebrae after implantation in Group II vs. Group I. | [62] |
| Enrolled Patients and Pathology | Type of Trial | Anatomical Site and Type of Prosthesis | Aim | Patient Groups (Analyzed Patient Number) | Quantitative Measurements | Main Results | Ref. |
|---|---|---|---|---|---|---|---|
| 39 with OA | Prospective study | Hip hydroxyapatite stem implant with RSA-markers. Ceramic heads and liners were made of Al2O3 | To determine if low BMD (OP and osteopenic patients) affects primary hip implant stability assessed by RSA | 1) normal BMD (12 pt) 2) low BMD (27:22 osteopenic and 5 osteoporotic) | RSA at 7 days (baseline) and 3, 6, 12 and 24 months, Harris hip and WOMAC scores | In pts with low BMD higher significant translation at 3 months than those with normal BMD. Patients with low BMD had a 4% probability of osseointegration at 3 months, as compared to a 50% probability in patients with normal BMD. | [67] |
| 85 with instable intertrochanteric fractures and OP | Retrospective cohort study | Bipolar hemiarthroplasty (57 hips) with fully HA-coated long-stem titanium alloy prosthesis | To determine clinical and radiologic results of cementless hemiarthroplasty using a fully HA-coated long stem in unstable inter- trochanteric fractures of patients with OP | 87 cementless bipolar hemiarthroplasties (85 pt) | Koval’s, Merle d’Aubigne and Postel scores (at 6 weeks, at 3, 6, 9 and 12 months and every year thereafter) X-rays morphometry; | Koval’s score: 28.3% patients were independent, 11.7% walked with canes, 16.7% with crutches or walkers, 18.3% used household ambulators and 21.7% pts became non functional ambulatory at the final follow-up. Merled’Aubigne and Postel: mean score was 14.7 points. Cortical porosis in 37.5%; acetabular erosion in 4.2%; heterotopic ossification in 6.3%; no subsidence, no failure of leg length equalization, no osteolysis. | [68] |
| 22 requiring bilateral pedicle screw fixation for lumbar fusion surgery | Prospective within-patient, left-right comparative study | Posterior pedicle screw fixation with HA sticks (100% pure HA granules with 3 d. Interconnected porous (70% porosity) structure of 100–300 μm) and interbody fusion | To evaluate the efficacy of HA stick augmentation on enhancing initial pedicle screw fixation strength, in OP and nonosteoporotic pts | 1) nonosteoporotic group with HA sticks and conventional screws 2) osteoporotic group with HA sticks and conventional screws | Torque measurement at surgery VAS, ODI and Short Form-36 Health Survey (preop and at 1 year) CT scan (at 1 year) X-rays (post op and at 6, 12 and 24 months) | Torque: pedicle screws with HA stick insertion significantly higher values than that without HA insertion in both OP and non OP pts with significant higher values in the non OP group then in the OP one. Differences in bone sclerosis between HA and control groups, regardless of the presence of osteoporosis | [71] |
| 34 with spondylolisthesis grade I or II and osteoporosis | Retrospective cohort study | Spinal transforaminal lumbar interbody fusion (L4–L5) with PEEK cages with or without screw augmentation with HA cement | To determine the efficacy of HA cement for screw augmentation in osteoporotic patients | 1) a screw augmentation group with HA cement (not reported) 2) a non augmented group (not reported) | X-rays morphometry (at day 1, at 3 months, at 1 and 2 years), VAS (post-op, 3 months and 2 years) | 1) 1 patient had revision surgery for the removal of a drainage tube that was tightly anchored to the fascia 2) 1 patient had revision surgery because of subcutaneous fluid collection; significant increases in SL, SA and DH; | [70] |
| 11 with painful OP vertebral fractures | Retrospective cohort study | Kyphoplasty using CaP cement | To investigate long-term radio-morphologic features of intraosseous and extraosseous linkages of CaP implants | twenty-four kyphoplasty procedures (11 pt) | X-rays morphometry CT scan VAS and EVOS scores (1 week and 1, 2 and 3 years) | Moderate reduction of 6.6% per year of the intraosseous CaP volume. ↑ postoperative vertebral height and sagittal index VAS improved significantly 2 years after implantation and EVOS from 1 year | [69] |
References
- Mavrogenis, A.F.; Dimitriou, R.; Parvizi, J.; Babis, G.C. Biology of implant osseointegration. J. Musculoskelet. Neuronal Interact. 2009, 9, 61–71. [Google Scholar]
- Fini, M.; Carpi, A.; Borsari, V.; Tschon, M.; Nicolini, A.; Sartori, M.; Mechanick, J.; Giardino, R. Bone remodeling, humoral networks and smart biomaterial technology for osteoporosis. Fron. Biosci. (Sch. Ed.) 2010, 2, 68–82. [Google Scholar] [CrossRef][Green Version]
- Smeets, R.; Stadlinger, B.; Schwarz, F.; Beck-Broichsitter, B.; Jung, O.; Precht, C.; Kloss, F.; Gröbe, A.; Heiland, M.; Ebker, T. Impact of dental implant surface modifications on osseointegration. BioMed Res. Int. 2016, 2016, 6285620. [Google Scholar] [CrossRef] [PubMed]
- Treccani, L.; Yvonne Klein, T.; Meder, F.; Pardun, K.; Rezwan, K. Functionalized ceramics for biomedical, biotechnological and environmental applications. Acta Biomater. 2013, 9, 7115–7150. [Google Scholar] [CrossRef]
- Li, L.; Lu, H.; Zhao, Y.; Luo, J.; Yang, L.; Liu, W.; He, Q. Functionalized cell-free scaffolds for bone defect repair inspired by self-healing of bone fractures: A review and new perspectives. Mater. Sci. Eng. C Mater. Biol. Appl. 2019, 98, 1241–1251. [Google Scholar] [CrossRef]
- Fini, M.; Salamanna, F.; Veronesi, F.; Torricelli, P.; Nicolini, A.; Benedicenti, S.; Carpi, A.; Giavaresi, G. Role of obesity, alcohol and smoking on bone health. Fron. Biosci. (Elite Ed.) 2012, 4, 2586–2606. [Google Scholar]
- Fini, M.; Giavaresi, G.; Torricelli, P.; Borsari, V.; Giardino, R.; Nicolini, A.; Carpi, A. Osteoporosis and biomaterial osteointegration. Biomed. Pharmacother. 2004, 58, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Fini, M.; Giavaresi, G.; Salamanna, F.; Veronesi, F.; Martini, L.; De Mattei, M.; Tschon, M. Harmful lifestyles on orthopedic implantation surgery: A descriptive review on alcohol and tobacco use. J. Bone Min. Metab. 2011, 29, 633–644. [Google Scholar] [CrossRef] [PubMed]
- Akkawi, I.; Zmerly, H. Osteoporosis: Current concepts. Joints 2018, 6, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Reginster, J.Y.; Burlet, N. Osteoporosis: A still increasing prevalence. Bone 2006, 38, S4–S9. [Google Scholar] [CrossRef]
- Cawthon, P.M. Gender differences in osteoporosis and fractures. Clin. Orthop. Relat. Res. 2011, 469, 1900–1905. [Google Scholar] [CrossRef]
- Tomé-Bermejo, F.; Piñera, A.R.; Alvarez, L. Osteoporosis and the management of spinal degenerative disease (II). Arch. Bone Jt. Surg. 2017, 5, 363–374. [Google Scholar] [PubMed]
- Dereka, X.; Calciolari, E.; Donos, N.; Mardas, N. Osseointegration in osteoporotic-like condition: A systematic review of preclinical studies. J. Periodontal Res. 2018, 53, 933–940. [Google Scholar] [CrossRef] [PubMed]
- Alghamdi, H.S.; Cuijpers, V.M.; Wolke, J.G.; van den Beucken, J.J.; Jansen, J.A. Calcium-phosphate-coated oral implants promote osseointegration in osteoporosis. J. Dent. Res. 2013, 92, 982–988. [Google Scholar] [CrossRef]
- Libicher, M.; Hillmeier, J.; Liegibel, U.; Sommer, U.; Pyerin, W.; Vetter, M.; Meinzer, H.P.; Grafe, I.; Meeder, P.; Nöldge, G.; Nawroth, P.; et al. Osseous integration of calcium phosphate in osteoporotic vertebral fractures after kyphoplasty: Initial results from a clinical and experimental pilot study. Osteoporos. Int. 2006, 17, 1208–1215. [Google Scholar] [CrossRef]
- Alghamdi, H.S.; Junker, R.; Bronkhorst, E.M.; Jansen, J.A. Bone regeneration related to calcium phosphate-coated implants in osteoporotic animal models: A meta-analysis. Tissue Eng. Part B Rev. 2012, 18, 383–395. [Google Scholar] [CrossRef] [PubMed]
- Daculsi, G.; Laboux, O.; Malard, O.; Weiss, P. Current state of the art of biphasic calcium phosphate bioceramics. J. Mater. Sci. Mater. Med. 2003, 14, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Davies, J. Understanding peri-implant endosseous healing. J. Dent. Educ. 2003, 67, 932–949. [Google Scholar]
- McEntire, B.J.; Bal, B.S.; Rahaman, M.N.; Chevalier, J.; Pezzotti, G. Ceramics and ceramic coatings in orthopaedics. J. Eur. Ceram. Soc. 2015, 35, 4327–4369. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1–9. [Google Scholar] [CrossRef]
- Kauschke, V.; Schneider, M.; Jauch, A.; Schumacher, M.; Kampschulte, M.; Rohnke, M.; Henss, A.; Bamberg, C.; Trinkaus, K.; Gelinsky, M.; et al. Effects of a pasty bone cement containing brain-derived neurotrophic factor-functionalized mesoporous bioactive glass particles on metaphyseal healing in a new murine osteoporotic fracture model. Int. J. Mol. Sci. 2018, 19, 3531. [Google Scholar] [CrossRef]
- Alghamdi, H.S.; Bosco, R.; Both, S.K.; Iafisco, M.; Leeuwenburgh, S.C.; Jansen, J.A.; van den Beucken, J.J. Synergistic effects of bisphosphonate and calcium phosphate nanoparticles on peri-implant bone responses in osteoporotic rats. Biomaterials 2014, 35, 5482–5490. [Google Scholar] [CrossRef]
- Pyo, S.W.; Kim, Y.M.; Kim, C.S.; Lee, I.S.; Park, J.U. Bone formation on biomimetic calcium phosphate- coated and zolendronate- immobilized titanium implants in osteoporotic rat tibiae. Int. J. Oral Maxillofac. Implants 2014, 29, 478–484. [Google Scholar] [CrossRef]
- Kettenberger, U.; Luginbuehl, V.; Procter, P.; Pioletti, D.P. In vitro and in vivo investigation of bisphosphonate-loaded hydroxyapatite particles for peri-implant bone augmentation. J. Tissue Eng. Regen. Med. 2017, 11, 1974–1985. [Google Scholar] [CrossRef]
- Li, X.; Li, Y.; Peng, S.; Ye, B.; Lin, W.; Hu, J. Effect of zinc ions on improving implant fixation in osteoporotic bone. Connect. Tissue Res. 2013, 54, 290–296. [Google Scholar] [CrossRef]
- Li, X.; Li, Y.; Liao, Y.; Li, J.; Zhang, L.; Hu, J. The effect of magnesium-incorporated hydroxyapatite coating on titanium implant fixation in ovariectomized rats. Int. J. Oral Maxillofac. Implants 2014, 29, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Luo, E.; Zhu, S.; Li, J.; Zhang, L.; Hu, J. Cancellous bone response to strontium-doped hydroxyapatite in osteoporotic rats. J. Appl. Biomater. Funct. Mater. 2015, 13, 28–34. [Google Scholar] [CrossRef]
- Li, Y.; Shui, X.; Zhang, L.; Hu, J. Cancellous bone healing around strontium-doped hydroxyapatite in osteoporotic rats previously treated with zoledronic acid. J. Biomed. Mater. Res. B Appl. Biomater. 2016, 104, 476–481. [Google Scholar] [CrossRef]
- Tao, Z.S.; Bai, B.L.; He, X.W.; Liu, W.; Li, H.; Zhou, Q.; Sun, T.; Huang, Z.L.; Tu, K.K.; Lv, Y.X.; et al. A comparative study of strontium-substituted hydroxyapatite coating on implant’s osseointegration for osteopenic rats. Med. Biol. Eng. Comput. 2016, 54, 1959–1968. [Google Scholar] [CrossRef] [PubMed]
- Tao, Z.S.; Zhou, W.S.; Qiang, Z.; Tu, K.K.; Huang, Z.L.; Xu, H.M.; Sun, T.; Lv, Y.X.; Cui, W.; Yang, L. Intermittent administration of human parathyroid hormone (1-34) increases fixation of strontium-doped hydroxyapatite coating titanium implants via electrochemical deposition in ovariectomized rat femur. J. Biomater. Appl. 2016, 30, 952–960. [Google Scholar] [CrossRef]
- Zhang, J.; Liu, L.; Zhao, S.; Wang, H.; Yang, G. Characterization and in vivo evaluation of trace element-loaded implant surfaces in ovariectomized rats. Int. J. Oral Maxillofac. Implants 2015, 30, 1105–1112. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Xu, S.; Chen, X.; He, D.; Ke, X.; Zhang, L.; Yang, G.; Liu, A.; Mou, X.; Xia, W.; et al. Intra-bone marrow injection of trace elements co-doped calcium phosphate microparticles for the treatment of osteoporotic rat. J. Biomed. Mater. Res. A 2017, 105, 1422–1432. [Google Scholar] [CrossRef] [PubMed]
- Tao, Z.S.; Zhou, W.S.; He, X.W.; Liu, W.; Bai, B.L.; Zhou, Q.; Huang, Z.L.; Tu, K.K.; Li, H.; Sun, T.; et al. A comparative study of zinc, magnesium, strontium-incorporated hydroxyapatite-coated titanium implants for osseointegration of osteopenic rats. Mater. Sci. Eng. C Mater. Biol. Appl. 2016, 62, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Tao, Z.; Zhou, W.; Jiang, Y.; Wu, X.; Xu, Z.; Yang, M.; Xie, J. Effects of strontium-modified calcium phosphate cement combined with bone morphogenetic protein-2 on osteoporotic bone defects healing in rats. J. Biomater. Appl. 2018, 33, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Baier, M.; Staudt, P.; Klein, R.; Sommer, U.; Wenz, R.; Grafe, I.; Meeder, P.J.; Nawroth, P.P.; Kasperk, C. Strontium enhances osseointegration of calcium phosphate cement: A histomorphometric pilot study in ovariectomized rats. J. Orthop. Surg. Res. 2013, 8, 16. [Google Scholar] [CrossRef] [PubMed]
- Cardemil, C.; Elgali, I.; Xia, W.; Emanuelsson, L.; Norlindh, B.; Omar, O.; Thomsen, P. Strontium-doped calcium phosphate and hydroxyapatite granules promote different inflammatory and bone remodelling responses in normal and ovariectomised rats. PLoS ONE. 2013, 8, e84932. [Google Scholar] [CrossRef] [PubMed]
- Chandran, S.; Babu, S.S.; Vs, H.K.; Varma, H.K.; John, A. Osteogenic efficacy of strontium hydroxyapatite micro-granules in osteoporotic rat model. J. Biomater. Appl. 2016, 31, 499–509. [Google Scholar] [CrossRef] [PubMed]
- Thormann, U.; Ray, S.; Sommer, U.; Elkhassawna, T.; Rehling, T.; Hundgeburth, M.; Henß, A.; Rohnke, M.; Janek, J.; Lips, K.S.; et al. Bone formation induced by strontium modified calcium phosphate cement in critical-size metaphyseal fracture defects in ovariectomized rats. Biomaterials 2013, 34, 8589–8598. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.; Alt, V.; Pan, L.; Thormann, U.; Schnettler, R.; Strauss, L.G.; Heinemann, S.; Schumacher, M.; Gelinsky, M.; Nies, B.; et al. Application of F-18-sodium fluoride (NaF) dynamic PET-CT (dPET-CT) for defect healing: A comparison of biomaterials in an experimental osteoporotic rat model. Med. Sci. Monit. 2014, 20, 1942–1949. [Google Scholar] [PubMed]
- van Houdt, C.I.A.; Ulrich, D.J.O.; Jansen, J.A.; van den Beucken, J.J.J.P. The performance of CPC/PLGA and Bio-Oss® for bone regeneration in healthy and osteoporotic rats. J. Biomed. Mater. Res. B Appl. Biomater. 2018, 106, 131–142. [Google Scholar] [CrossRef]
- Quan, H.; He, Y.; Sun, J.; Yang, W.; Luo, W.; Dou, C.; Kang, F.; Zhao, C.; He, J.; Yang, X.; et al. Chemical self-assembly of multifunctional hydroxyapatite with a coral-like nanostructure for osteoporotic bone reconstruction. ACS Appl. Mater. Interfaces 2018, 10, 25547–25560. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J.H.; Jin, E.S.; Kim, J.Y.; Lee, B.; Min, J.; Jeon, S.R.; Lee, M.; Choi, K.H. The effect of biocomposite screws on bone regeneration in a rat osteoporosis model. World Neurosurg. 2017, 106, 964–972. [Google Scholar] [CrossRef]
- Clafshenkel, W.P.; Rutkowski, J.L.; Palchesko, R.N.; Romeo, J.D.; McGowan, K.A.; Gawalt, E.S.; Witt-Enderby, P.A. A novel calcium aluminate-melatonin scaffold enhances bone regeneration within a calvarial defect. J. Pineal Res. 2012, 53, 206–218. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Peng, X.; Qin, Y.; Wang, R.; Tang, J.; Cui, X.; Wang, T.; Liu, W.; Pan, H.; Li, B. Acceleration of bone regeneration by activating Wnt/β-catenin signalling pathway via lithium released from lithium chloride/calcium phosphate cement in osteoporosis. Sci. Rep. 2017, 7, 45204. [Google Scholar] [CrossRef] [PubMed]
- Fang, W.; Zhao, S.; He, F.; Liu, L.; Yang, G. Influence of simvastatin-loaded implants on osseointegration in an ovariectomized animal model. BioMed Res. Int. 2015, 2015, 831504. [Google Scholar] [CrossRef]
- Wu, Y.; Cao, L.; Xia, L.; Wu, Q.; Wang, J.; Wang, X.; Xu, L.; Zhou, Y.; Xu, Y.; Jiang, X. Evaluation of osteogenesis and angiogenesis of icariin in local controlled release and systemic delivery for calvarial defect in ovariectomized rats. Sci. Rep. 2017, 7, 5077. [Google Scholar] [CrossRef]
- Xia, L.; Yin, Z.; Mao, L.; Wang, X.; Liu, J.; Jiang, X.; Zhang, Z.; Lin, K.; Chang, J.; Fang, B. Akermanite bioceramics promote osteogenesis, angiogenesis and suppress osteoclastogenesis for osteoporotic bone regeneration. Sci. Rep. 2016, 6, 22005. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Wang, T.; Yang, C.; Darvell, B.W.; Wu, J.; Lin, K.; Chang, J.; Pan, H.; Lu, W.W. Alkaline biodegradable implants for osteoporotic bone defects--importance of microenvironment pH. Osteoporos. Int. 2016, 27, 93–104. [Google Scholar] [CrossRef]
- Liu, X.; Bao, C.; Xu, H.H.K.; Pan, J.; Hu, J.; Wang, P.; Luo, E. Osteoprotegerin gene-modified BMSCs with hydroxyapatite scaffold for treating critical-sized mandibular defects in ovariectomized osteoporotic rats. Acta Biomater. 2016, 42, 378–388. [Google Scholar] [CrossRef]
- Hauser, M.; Siegrist, M.; Denzer, A.; Saulacic, N.; Grosjean, J.; Bohner, M.; Hofstetter, W. Bisphosphonates reduce biomaterial turnover in healing of critical-size rat femoral defects. J. Orthop. Surg. (Hong Kong) 2018, 26, 2309499018802487. [Google Scholar] [CrossRef]
- Gong, T.; Chen, Y.; Zhang, Y.; Zhang, Y.; Liu, X.; Troczynski, T.; Häfeli, U.O. Osteogenic and anti-osteoporotic effects of risedronate-added calcium phosphate silicate cement. Biomed. Mater. 2016, 11, 045002. [Google Scholar] [CrossRef]
- Shen, X.; Ma, P.; Hu, Y.; Xu, G.; Xu, K.; Chen, W.; Ran, Q.; Dai, L.; Yu, Y.; Mu, C.; et al. Alendronate-loaded hydroxyapatite-TiO2 nanotubes for improved bone formation in osteoporotic rabbits. J. Mater. Chem. B 2016, 4, 1423–1436. [Google Scholar] [CrossRef]
- Wu, C.C.; Kuo, C.L.; Fan, F.Y.; Yang, K.C. Strontium-impregnated bioabsorbable composite for osteoporotic fracture fixation. J. Biomed. Mater. Res. A 2015, 103, 3355–3363. [Google Scholar] [CrossRef]
- Zarins, J.; Pilmane, M.; Sidhoma, E.; Salma, I.; Locs, J. Immunohistochemical evaluation after Sr-enriched biphasic ceramic implantation in rabbits femoral neck: Comparison of seven different bone conditions. J. Mater. Sci. Mater. Med. 2018, 29, 119. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Xu, L.; Li, K.; Xie, N.; Xi, Y.; Wang, Y.; Zheng, X.; Chen, X.; Wang, M.; Ye, X. Zinc-modified calcium silicate coatings promote osteogenic differentiation through TGF-β/Smad pathway and osseointegration in osteopenic rabbits. Sci. Rep. 2017, 7, 3440. [Google Scholar] [CrossRef]
- Lozano, D.; Trejo, C.G.; Gómez-Barrena, E.; Manzano, M.; Doadrio, J.C.; Salinas, A.J.; Vallet-Regí, M.; García-Honduvilla, N.; Esbrit, P.; Buján, J. Osteostatin-loaded onto mesoporous ceramics improves the early phase of bone regeneration in a rabbit osteopenia model. Acta Biomater. 2012, 8, 2317–2323. [Google Scholar] [CrossRef] [PubMed]
- Luo, E.; Hu, J.; Bao, C.; Li, Y.; Tu, Q.; Murray, D.; Chen, J. Sustained release of adiponectin improves osteogenesis around hydroxyapatite implants by suppressing osteoclast activity in ovariectomized rabbits. Acta Biomater. 2012, 8, 734–743. [Google Scholar] [CrossRef] [PubMed]
- Plaza, J.Q.; Garzón, L.B.; Gimenez, B.B.; Moraleda, B.F.; Collía, F.; Rodríguez-Lorenzo, L.M. Application of calcium phosphates and fibronectin as complementary treatment for osteoporotic bone fractures. Injury 2016, 47, S15–S21. [Google Scholar] [CrossRef]
- Gunnella, F.; Kunisch, E.; Maenz, S.; Horbert, V.; Xin, L.; Mika, J.; Borowski, J.; Bischoff, S.; Schubert, H.; Sachse, A.; et al. The GDF5 mutant BB-1 enhances the bone formation induced by an injectable, poly(l-lactide-co-glycolide) acid (PLGA) fiber-reinforced, brushite-forming cement in a sheep defect model of lumbar osteopenia. Spine J. 2018, 18, 357–369. [Google Scholar] [CrossRef]
- Gunnella, F.; Kunisch, E.; Bungartz, M.; Maenz, S.; Horbert, V.; Xin, L.; Mika, J.; Borowski, J.; Bischoff, S.; Schubert, H.; et al. Low-dose BMP-2 is sufficient to enhance the bone formation induced by an injectable, PLGA fiber-reinforced, brushite-forming cement in a sheep defect model of lumbar osteopenia. Spine J. 2017, 17, 1699–1711. [Google Scholar] [CrossRef]
- James, A.W.; Chiang, M.; Asatrian, G.; Shen, J.; Goyal, R.; Chung, C.G.; Chang, L.; Shrestha, S.; Turner, A.S.; Seim, H.B.; et al. Vertebral Implantation of NELL-1 Enhances Bone Formation in an Osteoporotic Sheep Model. Tissue Eng. Part A 2016, 22, 840–849. [Google Scholar] [CrossRef]
- Verron, E.; Pissonnier, M.L.; Lesoeur, J.; Schnitzler, V.; Fellah, B.H.; Pascal-Moussellard, H.; Pilet, P.; Gauthier, O.; Bouler, J.M. Vertebroplasty using bisphosphonate-loaded calcium phosphate cement in a standardized vertebral body bone defect in an osteoporotic sheep model. Acta Biomater. 2014, 10, 4887–4895. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, C.M.; Ding, M.; Andersen, T.L.; Overgaard, S. Effects of substitute coated with hyaluronic acid or poly-lactic acid on implant fixation: Experimental study in ovariectomized and glucocorticoid-treated sheep. J. Tissue Eng. Regen. Med. 2018, 12, e1122–e1130. [Google Scholar] [CrossRef]
- Izquierdo-Barba, I.; Santos-Ruiz, L.; Becerra, J.; Feito, M.J.; Fernández-Villa, D.; Serrano, M.C.; Díaz-Güemes, I.; Fernández-Tomé, B.; Enciso, S.; Sánchez-Margallo, F.M.; et al. Synergistic effect of Si-hydroxyapatite coating and VEGF adsorption on Ti6Al4V-ELI scaffolds for bone regeneration in an osteoporotic bone environment. Acta Biomater. 2019, 83, 456–466. [Google Scholar] [CrossRef]
- Alt, V.; Cheung, W.H.; Chow, S.K.; Thormann, U.; Cheung, E.N.; Lips, K.S.; Schnettler, R.; Leung, K.S. Bone formation and degradation behavior of nanocrystalline hydroxyapatite with or without collagen-type 1 in osteoporotic bone defects—an experimental study in osteoporotic goats. Injury 2016, 47, S58–65. [Google Scholar] [CrossRef]
- Chandran, S.; Shenoy, S.J.; Babu, S.S.; P Nair, R.; Varma, H.K.; John, A. Strontium hydroxyapatite scaffolds engineered with stem cells aid osteointegration and osteogenesis in osteoporotic sheep model. Colloids Surf B Biointerfaces 2018, 163, 346–354. [Google Scholar] [CrossRef]
- Aro, H.T.; Alm, J.J.; Moritz, N.; Mäkinen, T.J.; Lankinen, P. Low BMD affects initial stability and delays stem osseointegration in cementless total hip arthroplasty in women: A 2-year RSA study of 39 patients. Acta Orthop. 2012, 83, 107–114. [Google Scholar] [CrossRef]
- Lee, Y.K.; Ha, Y.C.; Chang, B.K.; Kim, K.C.; Kim, T.Y.; Koo, K.H. Cementless bipolar hemiarthroplasty using a hydroxyapatite-coated long stem for osteoporotic unstable intertrochanteric fractures. J. Arthroplast. 2011, 26, 626–632. [Google Scholar] [CrossRef]
- Klein, R.; Tetzlaff, R.; Weiss, C.; Schäfer, M.K.; Tanner, M.; Wiedenhöfer, B.; Grafe, I.; Meeder, P.J.; Noeldge, G.; Nawroth, P.P.; et al. Osteointegration and resorption of intravertebral and extravertebral calcium phosphate cement. Clin. Spine Surg. 2017, 30, E291–E296. [Google Scholar] [CrossRef]
- Jang, S.H.; Lee, J.H.; Cho, J.Y.; Lee, H.Y.; Lee, S.H. The efficacy of hydroxyapatite for screw augmentation in osteoporotic patients. Neurol. Med. Chir. (Tokyo) 2013, 53, 875–881. [Google Scholar] [CrossRef]
- Shin, S.J.; Lee, J.H.; Lee, J.H. Influence of hydroxyapatite stick on pedicle screw fixation in degenerative lumbar spine: Biomechanical and radiologic study. Clin. Spine Surg. 2017, 30, E819–E826. [Google Scholar] [CrossRef]
- Epidemiology. Available online: https://www.iofbonehealth.org/epidemiology (accessed on 11 March 2019).
- Curtis, E.M.; Moon, R.J.; Harvey, N.C.; Cooper, C. The impact of fragility fracture and approaches to osteoporosis risk assessment worldwide. Bone 2017, 104, 29–38. [Google Scholar] [CrossRef]
- Pesce, V.; Speciale, D.; Sammarco, G.; Patella, S.; Spinarelli, A.; Patella, V. Surgical approach to bone healing in osteoporosis. Clin. Cases Miner. Bone Metab. 2009, 6, 131–135. [Google Scholar]
- Barfeie, A.; Wilson, J.; Rees, J. Implant surface characteristics and their effect on osseointegration. Br. Dent. J. 2015, 218, E9. [Google Scholar] [CrossRef]
- Ogle, O.E. Implant surface material, design and osseointegration. Dent. Clin. N. Am. 2015, 59, 505–520. [Google Scholar] [CrossRef] [PubMed]
- Malard, O.; Bouler, J.M.; Guicheux, J.; Heymann, D.; Pilet, P.; Coquard, C.; Daculsi, G. Influence of biphasic calcium phosphate granulometry on bone ingrowth, ceramic resorption and inflammatory reactions: Preliminary in vitro and in vivo study. J. Biomed. Mater. Res. 1999, 46, 103–111. [Google Scholar] [CrossRef]
- Lange, T.; Schilling, A.F.; Peters, F.; Mujas, J.; Wicklein, D.; Amling, M. Size dependent induction of proinflammatory cytokines and cytotoxicity of particulate beta-tricalciumphosphate in vitro. Biomaterials 2011, 32, 4067–4075. [Google Scholar] [CrossRef] [PubMed]
- Laquerriere, P.; Grandjean-Laquerriere, A.; Guenounou, M.; Laurent-Maquin, D.; Frayssinet, P.; Nardin, M. Correlation between sintering temperature of hydroxyapatite particles and the production of inflammatory cytokines by human monocytes. Colloid Surf. B 2003, 30, 207–213. [Google Scholar] [CrossRef]
- Boanini, E.; Torricelli, P.; Sima, F.; Axente, E.; Fini, M.; Mihailescu, I.N.; Bigi, A. Strontium and zoledronate hydroxyapatites graded composite coatings for bone prostheses. J. Colloid Interface Sci. 2015, 448. [Google Scholar] [CrossRef]
- Panzavolta, S.; Torricelli, P.; Casolari, S.; Parrilli, A.; Fini, M.; Bigi, A. Strontium-substituted hydroxyapatite-gelatin biomimetic scaffolds modulate bone cell response. Macromol. Biosci. 2018, 18, e1800096. [Google Scholar] [CrossRef] [PubMed]
- Boanini, E.; Torricelli, P.; Sima, F.; Axente, E.; Fini, M.; Mihailescu, I.N.; Bigi, A. Gradient coatings of strontium hydroxyapatite/zinc β-tricalcium phosphate as a tool to modulate osteoblast/osteoclast response. J. Inorg. Biochem. 2018, 183. [Google Scholar] [CrossRef]
- Bracci, B.; Torricelli, P.; Panzavolta, S.; Boanini, E.; Giardino, R.; Bigi, A. Effect of Mg(2+), Sr(2+) and Mn(2+) on the chemico-physical and in vitro biological properties of calcium phosphate biomimetic coatings. J. Inorg. Biochem. 2009, 103, 1666–1674. [Google Scholar] [CrossRef] [PubMed]
- Bigi, A.; Boanini, E. Functionalized biomimetic calcium phosphates for bone tissue repair. J. Appl. Biomater. Funct. Mater. 2017, 15, e313–e325. [Google Scholar] [CrossRef]
- Pan, J.; He, S.; Yin, X.; Li, Y.; Zhou, C.; Zou, S. Lithium enhances alveolar bone formation during orthodontic retention in rats. Orthod. Craniofac. Res. 2017, 20, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Salamanna, F.; Giavaresi, G.; Contartese, D.; Bigi, A.; Boanini, E.; Parrilli, A.; Lolli, R.; Gasbarrini, A.; Barbanti Brodano, G.; Fini, M. Effect of strontium substituted β-TCP associated to mesenchymal stem cells from bone marrow and adipose tissue on spinal fusion in healty and ovariectomized rat. J. Cell Physiol. 2019. [Google Scholar] [CrossRef]
- Dolci, L.S.; Panzavolta, S.; Torricelli, P.; Albertini, B.; Sicuro, L.; Fini, M.; Bigi, A.; Passerini, N. Modulation of Alendronate release from a calcium phosphate bone cement: An in vitro osteoblast-osteoclast co-culture study. Int. J. Pharm. 2019, 554, 245–255. [Google Scholar] [CrossRef]
- Forte, L.; Sarda, S.; Combes, C.; Brouillet, F.; Gazzano, M.; Marsan, O.; Boanini, E.; Bigi, A. Hydroxyapatite functionalization to trigger adsorption and release of risedronate. Colloids Surf. B Biointerfaces 2017, 160, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Panzavolta, S.; Torricelli, P.; Bracci, B.; Fini, M.; Bigi, A. Functionalization of biomimetic calcium phosphate bone cements with alendronate. J. Inorg. Biochem. 2010, 104, 1099–1106. [Google Scholar] [CrossRef]
- Asaumi, K.; Nakanishi, T.; Asahara, H.; Inoue, H.; Takigawa, M. Expression of neurotrophins and their receptors (TRK) during fracture healing. Bone 2000, 26, 625–633. [Google Scholar] [CrossRef]
- Shah, S.R.; Werlang, C.A.; Kasper, F.K.; Mikos, A.G. Novel applications of statins for bone regeneration. Natl. Sci. Rev. 2015, 2, 85–99. [Google Scholar] [CrossRef]
- Liu, J.; Huang, F.; He, H.W. Melatonin effects on hard tissues: Bone and tooth. Int. J. Mol. Sci. 2013, 14, 10063–10074. [Google Scholar] [CrossRef]
- Zhang, X.; Liu, T.; Huang, Y.; Wismeijer, D.; Liu, Y. Icariin: Does it have an osteoinductive potential for bone tissue engineering? Phytother. Res. 2014, 28, 498–509. [Google Scholar] [CrossRef]
- Amengual-Peñafiel, L.; Brañes-Aroca, M.; Marchesani-Carrasco, F.; Jara-Sepúlveda, M.C.; Parada-Pozas, L.; Cartes-Velásquez, R. Coupling between osseointegration and mechanotransduction to maintain foreign body equilibrium in the long-term: A comprehensive overview. J. Clin. Med. 2019, 8, 139. [Google Scholar] [CrossRef] [PubMed]
- Velard, F.; Braux, J.; Amedee, J.; Laquerriere, P. Inflammatory cell response to calcium phosphate biomaterial particles: An overview. Acta Biomater. 2013, 9, 4956–4963. [Google Scholar] [CrossRef]
- Macari, S.; Duffles, L.F.; Queiroz-Junior, C.M.; Madeira, M.F.M.; Dias, G.J.; Teixeira, M.M.; Szawka, R.E.; Silva, T.A. Oestrogen regulates bone resorption and cytokine production in the maxillae of female mice. Arch. Oral Biol. 2015, 60, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Rehman, D.; Qureshi, S.; Haq, A.A. Early detection of osteoporosis from incisure depth of human mandible in an orthopantomogram. J. Pak. Med. Assoc. 2014, 64, 766–769. [Google Scholar] [PubMed]
- Scalize, P.H.; de Sousa, L.G.; Regalo, S.C.; Semprini, M.; Pitol, D.L.; da Silva, G.A.; de Almeida Coelho, J.; Coppi, A.A.; Laad, A.A.; Prado, K.F.; et al. Low-level laser therapy improves bone formation: Stereology findings for osteoporosis in rat model. Lasers Med. Sci. 2015, 30, 1599–1607. [Google Scholar] [CrossRef] [PubMed]
- Hirata, H.H.; Munhoz, M.A.; Plepis, A.M.; Martins, V.C.; Santos, G.R.; Galdeano, E.A.; Cunha, M.R. Feasibility study of collagen membranes derived from bovine pericardium and intestinal serosa for the repair of cranial defects in ovariectomised rats. Injury 2015, 46, 1215–1222. [Google Scholar] [CrossRef] [PubMed]




© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sartori, M.; Maglio, M.; Tschon, M.; Nicoli Aldini, N.; Visani, A.; Fini, M. Functionalization of Ceramic Coatings for Enhancing Integration in Osteoporotic Bone: A Systematic Review. Coatings 2019, 9, 312. https://doi.org/10.3390/coatings9050312
Sartori M, Maglio M, Tschon M, Nicoli Aldini N, Visani A, Fini M. Functionalization of Ceramic Coatings for Enhancing Integration in Osteoporotic Bone: A Systematic Review. Coatings. 2019; 9(5):312. https://doi.org/10.3390/coatings9050312
Chicago/Turabian StyleSartori, Maria, Melania Maglio, Matilde Tschon, Nicolò Nicoli Aldini, Andrea Visani, and Milena Fini. 2019. "Functionalization of Ceramic Coatings for Enhancing Integration in Osteoporotic Bone: A Systematic Review" Coatings 9, no. 5: 312. https://doi.org/10.3390/coatings9050312
APA StyleSartori, M., Maglio, M., Tschon, M., Nicoli Aldini, N., Visani, A., & Fini, M. (2019). Functionalization of Ceramic Coatings for Enhancing Integration in Osteoporotic Bone: A Systematic Review. Coatings, 9(5), 312. https://doi.org/10.3390/coatings9050312