Differentiation of Patients with Balance Insufficiency (Vestibular Hypofunction) versus Normal Subjects Using a Low-Cost Small Wireless Wearable Gait Sensor



Abstract
1. Introduction
2. Materials and Methods
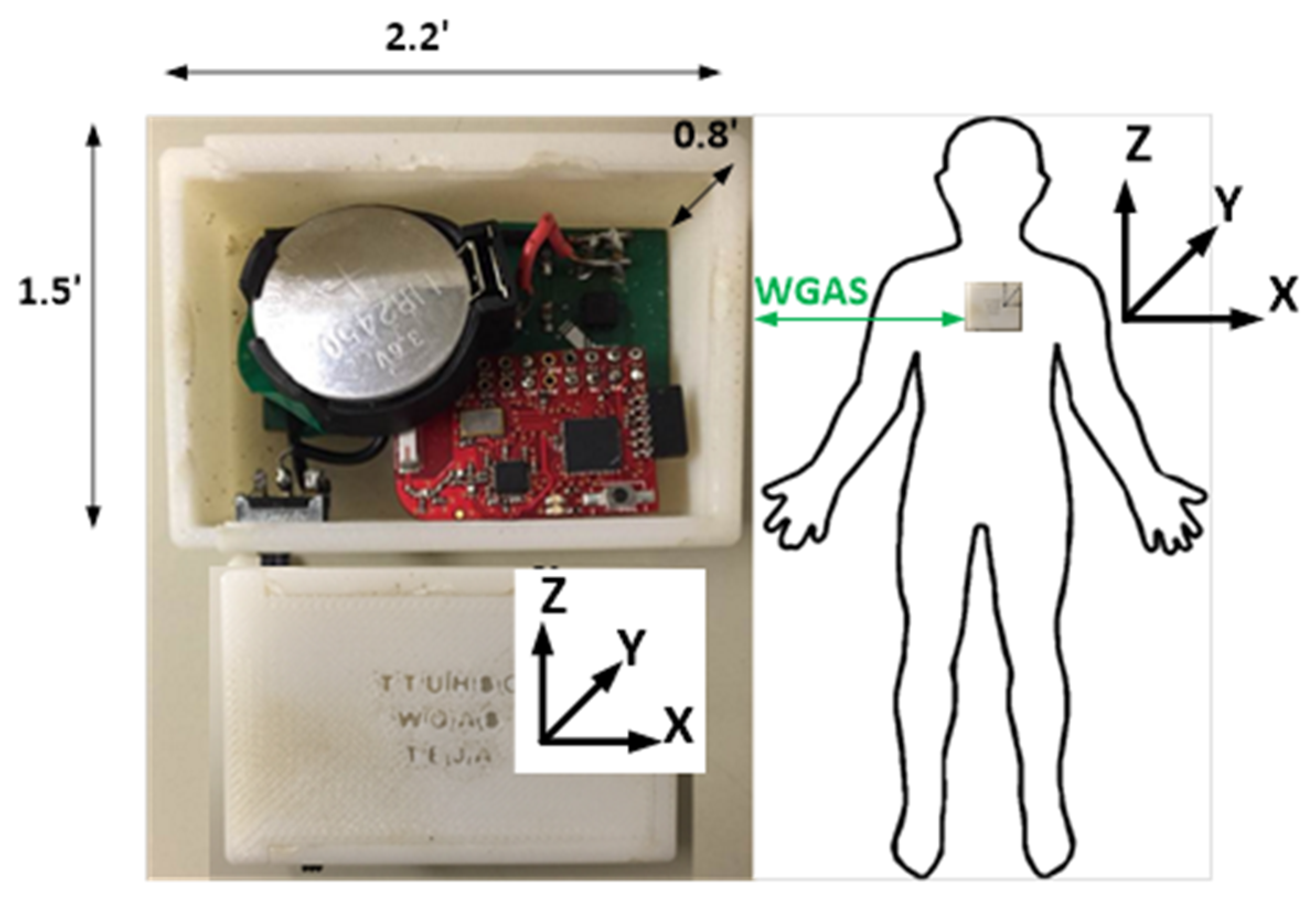
2.1. Gait Data Collection
2.2. Gait Data Analysis
2.3. Data Availability
3. Results
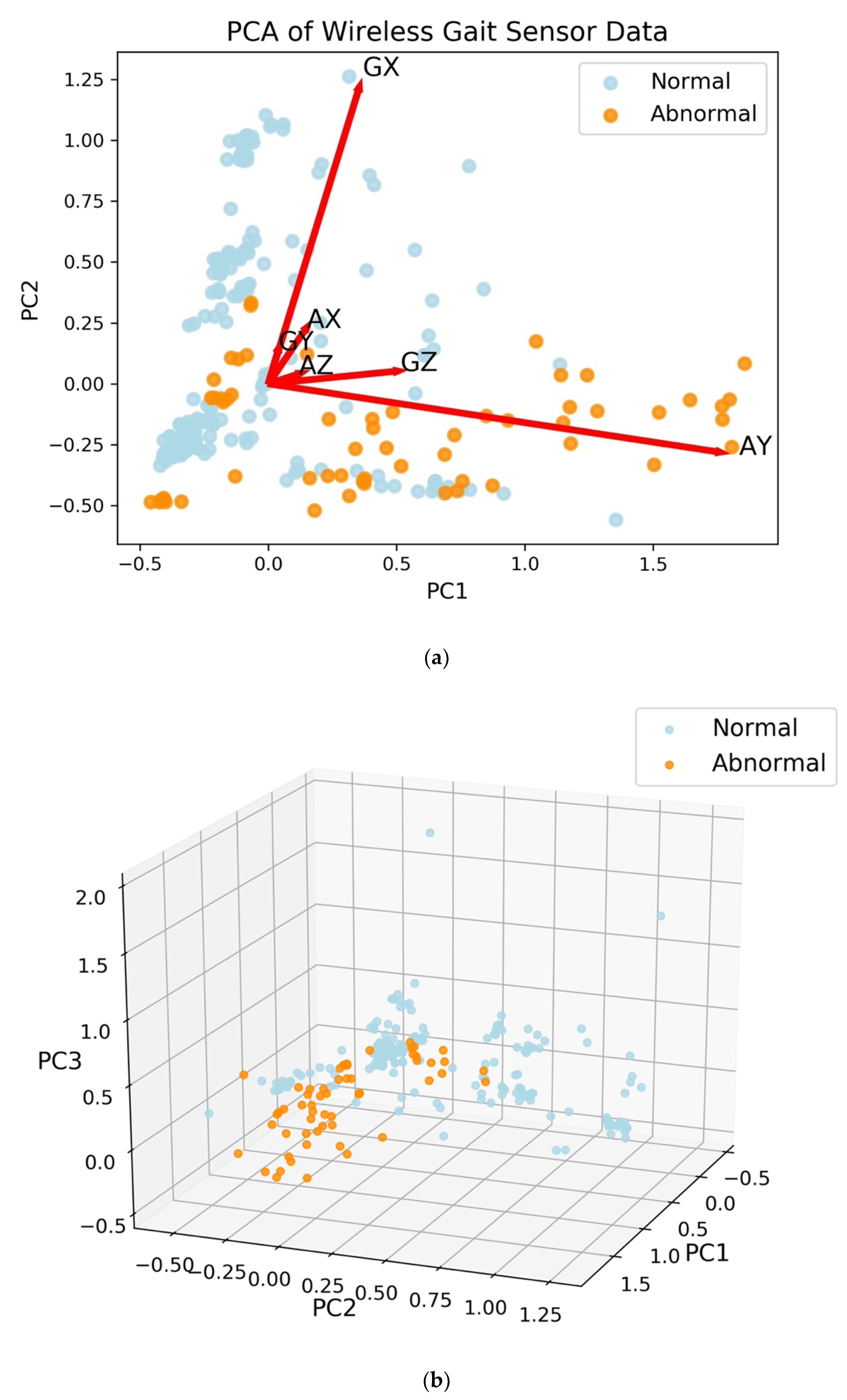
3.1. Feature Extraction Separates Normal from Abnormal Gaits
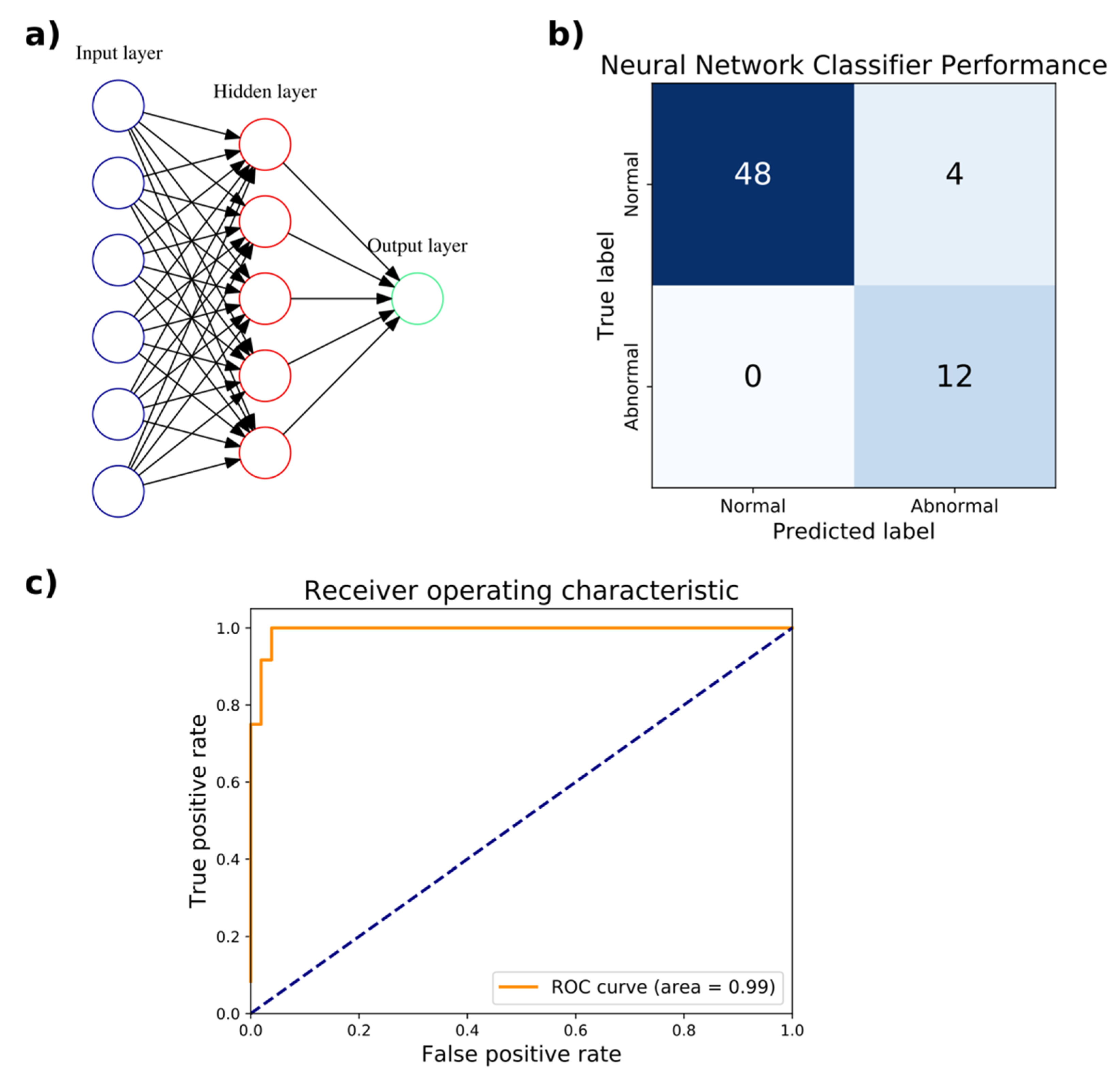
3.2. An Artificial Neural Network Classifies Abnormal and Normal Gaits with High Accuracy
3.3. A Support Vector Machine Yields Excellent Performance in Gait Classification
3.4. Feature Extraction Allows for High-Performance Classification
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Burns, E.R.; Stevens, J.A.; Lee, R. The direct costs of fatal and non-fatal falls among older adults—United States. J. Saf. Res. 2016, 58, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Thomas, S.M.; Veroniki, A.A.; Hamid, J.S.; Cogo, E.; Strifler, L.; Khan, P.A.; Robson, R.; Sibley, K.M.; MacDonald, H.; et al. Comparisons of Interventions for Preventing Falls in Older Adults: A Systematic Review and Meta-analysis. JAMA 2017, 318, 1687–1699. [Google Scholar] [CrossRef] [PubMed]
- Goebel, J. Practical Management of the Dizzy Patient, 2nd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008; ISBN 978-0-7817-6562-6. [Google Scholar]
- Hogg, D. Model-based vision: A program to see a walking person. Image Vis. Comput. 1983, 1, 5–20. [Google Scholar] [CrossRef]
- Harris, G.F.; Wertsch, J.J. Procedures for gait analysis. Arch. Phys. Med. Rehabil. 1994, 75, 216–225. [Google Scholar] [PubMed]
- Aminian, K.; Rezakhanlou, K.; Andres, E.D.; Fritsch, C.; Leyvraz, P.-F.; Robert, P. Temporal feature estimation during walking using miniature accelerometers: An analysis of gait improvement after hip arthroplasty. Med. Biol. Eng. Comput. 1999, 37, 686–691. [Google Scholar] [CrossRef] [PubMed]
- Selles, R.W.; Formanoy, M.A.G.; Bussmann, J.B.J.; Janssens, P.J.; Stam, H.J. Automated estimation of initial and terminal contact timing using accelerometers; development and validation in transtibial amputees and controls. IEEE Trans. Neural Syst. Rehabil. Eng. 2005, 13, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Boutaayamou, M.; Schwartz, C.; Stamatakis, J.; Denoël, V.; Maquet, D.; Forthomme, B.; Croisier, J.-L.; Macq, B.; Verly, J.G.; Garraux, G.; et al. Development and validation of an accelerometer-based method for quantifying gait events. Med. Eng. Phys. 2015, 37, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, T.; Mizuno, F.; Hayasaka, T.; Tsubota, K.; Wada, S.; Yamaguchi, T. Gait Analysis for Detecting a Leg Accident with an Accelerometer. In Proceedings of the 1st Transdisciplinary Conference on Distributed Diagnosis and Home Healthcare, Arlington, VA, USA, 2–4 April 2006; pp. 43–46. [Google Scholar]
- Nukala, B.T.; Shibuya, N.; Rodriguez, A.; Tsay, J.; Lopez, J.; Nguyen, T.; Zupancic, S.; Lie, D.Y.-C. An Efficient and Robust Fall Detection System Using Wireless Gait Analysis Sensor with Artificial Neural Network (ANN) and Support Vector Machine (SVM) Algorithms. Open J. Appl. Biosens. 2015, 3, 29–39. [Google Scholar] [CrossRef]
- Nukala, B.T.; Shibuya, N.; Rodriguez, A.I.; Tsay, J.; Nguyen, T.Q.; Zupancic, S.; Lie, D.Y.C. A real-time robust fall detection system using a wireless gait analysis sensor and an Artificial Neural Network. In Proceedings of the 2014 IEEE Healthcare Innovation Conference (HIC), Seattle, WA, USA, 8–10 October 2014; pp. 219–222. [Google Scholar]
- Lie, D.Y.C.; Nukala, B.T.; Jacob, J.; Tsay, J.; Shibuya, N.; Lie, P.E.; Rodriguez, A.; Nguyen, T.Q.; Zupancic, S. The Design of Robust Real-Time Wearable Fall Detection Systems Aiming for Fall Prevention. In Activities of Daily Living (ADL): Cultural Differences, Impacts of Disease and Long-Term Health Effects; Nova Science Publishers, Inc.: Hauppauge, NY, USA, 2015; pp. 51–76. ISBN 978-1-63463-913-2. [Google Scholar]
- Nukala, B.T.; Nakano, T.; Rodriguez, A.; Tsay, J.; Lopez, J.; Nguyen, T.Q.; Zupancic, S.; Lie, D.Y.C. Real-Time Classification of Patients with Balance Disorders vs. Normal Subjects Using a Low-Cost Small Wireless Wearable Gait Sensor. Biosensors 2016, 6, 58. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, G.P.; Newman, C.W. The Development of the Dizziness Handicap Inventory. Arch. Otolaryngol. Head Neck Surg. 1990, 116, 424–427. [Google Scholar] [CrossRef] [PubMed]
- Pearson, K.F.R.S. On lines and planes of closest fit to systems of points in space. Lond. Edinb. Dublin Philos. Mag. J. Sci. 1901, 2, 559–572. [Google Scholar] [CrossRef]
- Cortes, C.; Vapnik, V. Support-vector networks. Mach. Learn. 1995, 20, 273–297. [Google Scholar] [CrossRef]
- Kingma, D.P.; Ba, J. Adam: A Method for Stochastic Optimization. arXiv, 2014; arXiv:1412.6980. [Google Scholar]
- Hunter, J.D. Matplotlib: A 2D Graphics Environment. Comput. Sci. Eng. 2007, 9, 90–95. [Google Scholar] [CrossRef]
- Lemaître, G.; Nogueira, F.; Aridas, C.K. Imbalanced-learn: A Python Toolbox to Tackle the Curse of Imbalanced Datasets in Machine Learning. J. Mach. Learn. Res. 2017, 18, 1–5. [Google Scholar]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Ihlen, E.A.F.; Weiss, A.; Helbostad, J.L.; Hausdorff, J.M. The Discriminant Value of Phase-Dependent Local Dynamic Stability of Daily Life Walking in Older Adult Community-Dwelling Fallers and Nonfallers. Available online: https://www.hindawi.com/journals/bmri/2015/402596/ (accessed on 31 January 2019).
- Bizovska, L.; Svoboda, Z.; Janura, M.; Bisi, M.C.; Vuillerme, N. Local dynamic stability during gait for predicting falls in elderly people: A one-year prospective study. PLoS ONE 2018, 13, e0197091. [Google Scholar] [CrossRef] [PubMed]
- Hemmatpour, M.; Ferrero, R.; Gandino, F.; Montrucchio, B.; Rebaudengo, M. Nonlinear Predictive Threshold Model for Real-Time Abnormal Gait Detection. Available online: https://www.hindawi.com/journals/jhe/2018/4750104/ (accessed on 31 January 2019).
- Howcroft, J.; Kofman, J.; Lemaire, E.D. Feature selection for elderly faller classification based on wearable sensors. J. Neuroeng. Rehabil. 2017, 14, 47. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.C.; Kim, J.Y.; Lee, H.N.; Lee, H.H.; Kwon, J.H.; Kim, N.B.; Kim, M.J.; Hwang, J.H.; Han, G.C. A quantitative analysis of gait patterns in vestibular neuritis patients using gyroscope sensor and a continuous walking protocol. J. Neuroeng. Rehabil. 2014, 11, 58. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, G.; Shepard, N. Balance Function Assessment and Management, 2nd ed.; Plural Publishing, Inc.: San Diego, CA, USA, 2014; ISBN 978-1-59756-547-9. [Google Scholar]
- Keogh, E.; Ratanamahatana, C.A. Exact indexing of dynamic time warping. Knowl. Inf. Syst. 2005, 7, 358–386. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Approximate Range of Operation | 12 m (40 ft) |
|---|---|
| Approximate battery life | 40 h (estimated for always-on time) |
| Weight | 42 g |
| Dimensions | 2.2” × 1.5” × 0.8” |
| Condition | Description |
|---|---|
| 1 | Walk on a level surface at normal speed for 20′ |
| 2 | Walk at normal speed for 5′, walk fast for next 5′, walk slowly for next 5′, walk at normal speed for final 5′ |
| 3 | Walk for 20′ while turning the head horizontally |
| 4 | Walk for 20′ while turning the head vertically |
| 5 | Walk normally up to the 20′ mark; at the end pivot to turn around |
| 6 | Walk normally for 20′ with an obstacle in the path; step over (not around) the obstacle |
| Male | Female | Normal Gait | Abnormal Gait | |
|---|---|---|---|---|
| Number of subjects | 22 | 38 | 50 | 10 |
| Range | 21–80 years old | |||
| Average age | 51.8 years old | |||
| Number of Hidden Layers | Number of Neurons Per Hidden Layer | Accuracy | F1 Score | AUC |
|---|---|---|---|---|
| 1 | 3 | 0.895 | 0.800 | 0.986 |
| 1 | 4 | 0.895 | 0.800 | 0.986 |
| 1 | 5 | 0.947 | 0.909 | 1.000 |
| 1 | 6 | 0.895 | 0.800 | 0.986 |
| 1 | 7 | 0.947 | 0.909 | 0.986 |
| 1 | 8 | 0.947 | 0.909 | 0.986 |
| 2 | 3/2 | 0.263 | 0.417 | 0.757 |
| 2 | 4/2 | 0.263 | 0.417 | 0.857 |
| 2 | 4/3 | 0.895 | 0.800 | 0.986 |
| 2 | 5/2 | 0.947 | 0.909 | 0.943 |
| 2 | 5/3 | 0.263 | 0.417 | 0.786 |
| 2 | 5/4 | 0.263 | 0.417 | 0.757 |
| Kernel | Hyperparameters | Accuracy | AUC |
|---|---|---|---|
| Linear | C = 10 | 0.910 | 0.936 |
| Linear | C = 102 | 0.933 | 0.944 |
| Linear | C = 103 | 0.937 | 0.941 |
| Linear | C = 104 | 0.941 | 0.941 |
| Linear | C = 105 | 0.937 | 0.938 |
| Radial basis function | C = 103, γ = 10−1 | 0.961 | 0.968 |
| Radial basis function | C = 103, γ = 10−2 | 0.918 | 0.944 |
| Radial basis function | C = 103, γ = 10−3 | 0.878 | 0.922 |
| Radial basis function | C = 104, γ = 10−1 | 0.961 | 0.964 |
| Radial basis function | C = 104, γ = 10−2 | 0.914 | 0.942 |
| Radial basis function | C = 104, γ = 10−3 | 0.922 | 0.945 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, T.Q.; Young, J.H.; Rodriguez, A.; Zupancic, S.; Lie, D.Y.C. Differentiation of Patients with Balance Insufficiency (Vestibular Hypofunction) versus Normal Subjects Using a Low-Cost Small Wireless Wearable Gait Sensor. Biosensors 2019, 9, 29. https://doi.org/10.3390/bios9010029
Nguyen TQ, Young JH, Rodriguez A, Zupancic S, Lie DYC. Differentiation of Patients with Balance Insufficiency (Vestibular Hypofunction) versus Normal Subjects Using a Low-Cost Small Wireless Wearable Gait Sensor. Biosensors. 2019; 9(1):29. https://doi.org/10.3390/bios9010029
Chicago/Turabian StyleNguyen, Tam Q., Jonathan H. Young, Amanda Rodriguez, Steven Zupancic, and Donald Y.C. Lie. 2019. "Differentiation of Patients with Balance Insufficiency (Vestibular Hypofunction) versus Normal Subjects Using a Low-Cost Small Wireless Wearable Gait Sensor" Biosensors 9, no. 1: 29. https://doi.org/10.3390/bios9010029
APA StyleNguyen, T. Q., Young, J. H., Rodriguez, A., Zupancic, S., & Lie, D. Y. C. (2019). Differentiation of Patients with Balance Insufficiency (Vestibular Hypofunction) versus Normal Subjects Using a Low-Cost Small Wireless Wearable Gait Sensor. Biosensors, 9(1), 29. https://doi.org/10.3390/bios9010029