Development of an Optical Method for the Evaluation of Whole Blood Coagulation


Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Preparation
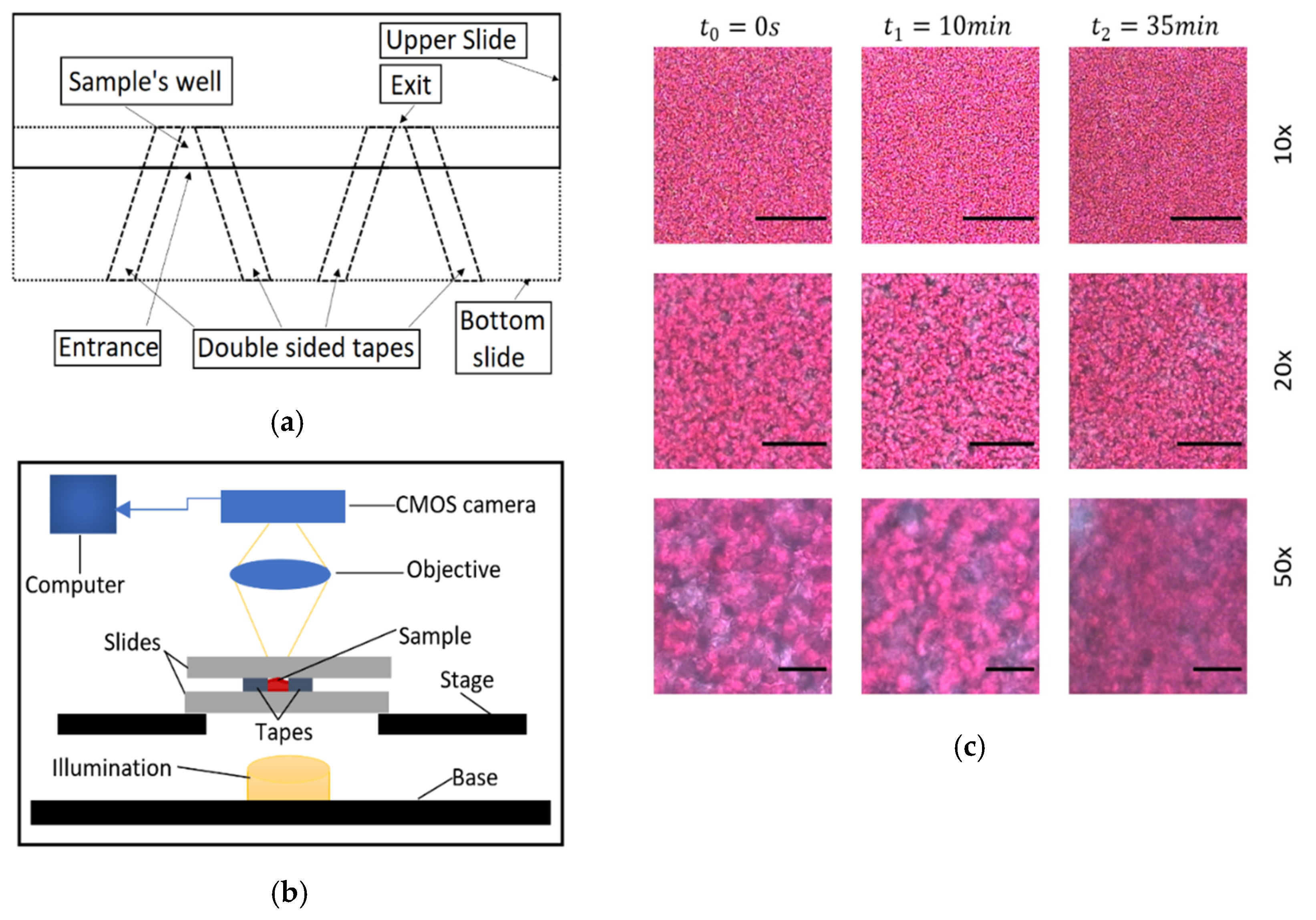
2.2. Experimental Setup
2.3. Whole Blood Sample Coagulation Evaluation
3. Results and Discussion
4. Limitations and Sources of Uncertainty
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dahlbäck, B. Blood coagulation. Lancet 2000, 355, 1627–1632. [Google Scholar] [CrossRef]
- Ruggeri, Z.M. The role of von Willebrand factor in thrombus formation. Thromb. Res. 2007, 120. [Google Scholar] [CrossRef]
- Gale, A.J. Continuing Education Course #2: Current Understanding of Hemostasis. Toxicol. Pathol. 2011, 39, 273–280. [Google Scholar]
- Weisel, J.W. The mechanical properties of fibrin for basic scientists and clinicians. Biophys. Chem. 2004, 112, 267–276. [Google Scholar] [CrossRef]
- Lippi, G.; Favaloro, E.J.; Franchini, M.; Guidi, G.C. Milestones and perspectives in coagulation and hemostasis. Semin. Thromb. Hemost. 2009, 35, 9–22. [Google Scholar] [CrossRef] [PubMed]
- Alzahrani, S.H.; Ajjan, R.A. Review article: Coagulation and fibrinolysis in diabetes. Diabetes Vasc. Dis. Res. 2010, 7, 260–273. [Google Scholar] [CrossRef]
- Franchini, M.; Mannucci, P.M. Venous and arterial thrombosis: Different sides of the same coin? Eur. J. Intern. Med. 2008, 19, 476–481. [Google Scholar] [CrossRef]
- Federici, A.B. Prophylaxis of bleeding episodes in patients with von Willebrand’s disease. Blood Transfus. 2008, 6 (Suppl. 2), s26. [Google Scholar]
- Baskurt, O.K.; Meiselman, H.J. Erythrocyte aggregation: Basic aspects and clinical importance. Clin. Hemorheol. Microcirc. 2013, 53, 23–37. [Google Scholar] [CrossRef]
- Smith, S.A.; Travers, R.J.; Morrissey, J.H. How it all starts: Initiation of the clotting cascade. Crit. Rev. Biochem. Mol. Biol. 2015, 50, 326–336. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi Aria, M.; Erten, A.; Yalcin, O. Technology Advancements in Blood Coagulation Measurements for Point-of-Care Diagnostic Testing. Front. Bioeng. Biotechnol. 2019, 7, 395. [Google Scholar] [CrossRef]
- Paniccia, R.; Priora, R.; Liotta, A.A.; Abbate, R. Platelet Function tests: A Comparative Review. Vasc. Health Risk Manag. 2015, 11, 133–148. [Google Scholar] [CrossRef]
- Monroe, D.M.; Hoffman, M. What does it take to make the perfect clot? Arterioscler. Thromb. Vasc. Biol. 2006, 26, 41–48. [Google Scholar] [CrossRef]
- Harris, L.F.; Castro-López, V.; Killard, A.J. Coagulation monitoring devices: Past, present, and future at the point of care. TrAC-Trends Anal. Chem. 2013, 50, 85–95. [Google Scholar] [CrossRef]
- Poller, L.; Ibrahim, S.; Keown, M.; Pattison, A.; Jespersen, J. The prothrombin time/international normalized ratio (PT/INR) Line: Derivation of local INR with commercial thromboplastins and coagulometers—Two independent studies. J. Thromb. Haemost. 2011, 9, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Lei, K.F.; Chen, K.H.; Tsui, P.H.; Tsang, N.M. Real-Time Electrical Impedimetric Monitoring of Blood Coagulation Process under Temperature and Hematocrit Variations Conducted in a Microfluidic Chip. PLoS ONE 2013, 8. [Google Scholar] [CrossRef]
- Andrew, M.; Ansell, J.L.; Becker, D.M.; Becker, R.C.; Triplett, D.A. Point-of-care prothrombin time measurement for professional and patient self-testing use: A multicenter clinical experience. Am. J. Clin. Pathol. 2001, 115, 288–296. [Google Scholar] [CrossRef]
- Nam, M.H.; Kyoung, H.R.; Pak, H.N.; Chang, K.L.; Kim, Y.H.; Kap, N.L.; Cho, Y. Evaluation of the Roche CoaguChek XS handheld coagulation analyzer in a cardiac outpatient clinic. Ann. Clin. Lab. Sci. 2008, 38, 37–40. [Google Scholar]
- Hartert, H. Blutgerinnungsstudien mit der Thrombelastographie, einem neuen Untersuchungsverfahren. Klin. Wochenschr. 1948, 26, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Whiting, D.; Dinardo, J.A. TEG and ROTEM: Technology and clinical applications. Am. J. Hematol. 2014, 89, 228–232. [Google Scholar] [CrossRef]
- Nardi, G.; Agostini, V.; Rondinelli, B.; Russo, E.; Bastianini, B.; Bini, G.; Bulgarelli, S.; Cingolani, E.; Donato, A.; Gambale, G.; et al. Trauma-induced coagulopathy: Impact of the early coagulation support protocol on blood product consumption, mortality and costs. Crit. Care 2015, 19. [Google Scholar] [CrossRef] [PubMed]
- Schöchl, H.; Nienaber, U.; Hofer, G.; Voelckel, W.; Jambor, C.; Scharbert, G.; Kozek-Langenecker, S.; Solomon, C. Goal-directed coagulation management of major trauma patients using thromboelastometry (ROTEM®)-guided administration of fibrinogen concentrate and prothrombin complex concentrate. Crit. Care 2010, 14, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Davies, E.R. Computer and Machine Vision; Academic Press: Cambridge, MA, USA, 2012; ISBN 9780123869081. [Google Scholar]
- Sotiropoulou, C.L.; Voudouris, L.; Gentsos, C.; Demiris, A.M.; Vassiliadis, N.; Nikolaidis, S. Real-time machine vision FPGA implementation for microfluidic monitoring on lab-on-chips. IEEE Trans. Biomed. Circuits Syst. 2014. [Google Scholar] [CrossRef]
- Chang, H.; Yang, Q.; Parvin, B. Segmentation of heterogeneous blob objects through voting and level set formulation. Pattern Recognit. Lett. 2007. [Google Scholar] [CrossRef] [PubMed]
- Kaliviotis, E.; Sherwood, J.M.; Balabani, S. Partitioning of red blood cell aggregates in bifurcating microscale flows. Sci. Rep. 2017, 7. [Google Scholar] [CrossRef]
- Martínez-López, J.I.; Betancourt, H.A.; García-López, E.; Rodriguez, C.A.; Siller, H.R. Rapid fabrication of disposable micromixing arrays using xurography and laser ablation. Micromachines 2017, 8, 144. [Google Scholar] [CrossRef]
- Roggo, C.; van der Meer, J.R. Miniaturized and integrated whole cell living bacterial sensors in field applicable autonomous devices. Curr. Opin. Biotechnol. 2017, 45, 24–33. [Google Scholar] [CrossRef]
- Rosado-Galindo, H.; Domenech, M. Polystyrene Topography Sticker Array for Cell-Based Assays. Recent Prog. Mater. 2020, 2, 1–18. [Google Scholar] [CrossRef]
- Pasias, D.; Passos, A.; Constantinides, G.; Balabani, S.; Kaliviotis, E. Surface tension driven flow of blood in a rectangular microfluidic channel: Effect of erythrocyte aggregation. Phys. Fluids 2020. [Google Scholar] [CrossRef]
- Zhukov, E.L.; Gubarev, F.A.; Tyutrin, I.I. A Portable Device for Rapid Assessment of the Functional State of the Hemostasis System. Biomed. Eng. 2021, 54, 345–349. [Google Scholar] [CrossRef]
- Weissleder, R. A clearer vision for in vivo imaging: Progress continues in the development of smaller, more penetrable probes for biological imaging. Nat. Biotechnol. 2001, 19, 316–317. [Google Scholar] [CrossRef] [PubMed]
- Panteleev, M.A.; Ovanesov, M.V.; Kireev, D.A.; Shibeko, A.M.; Sinauridze, E.I.; Ananyeva, N.M.; Butylin, A.A.; Saenko, E.L.; Ataullakhanov, F.I. Spatial propagation and localization of blood coagulation are regulated by intrinsic and protein C pathways, respectively. Biophys. J. 2006, 90, 1489–1500. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.; Nam, J.; Xue, S.; Shin, S. Measurement of blood coagulation with considering RBC aggregation through a microchip-based light transmission aggregometer. Clin. Hemorheol. Microcirc. 2011, 47, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Zhu, J.; Chen, Z. Dynamic and quantitative assessment of blood coagulation using optical coherence elastography. Sci. Rep. 2016, 6. [Google Scholar] [CrossRef] [PubMed]
- Faivre, M.; Peltié, P.; Planat-Chrétien, A.; Cosnier, M.-L.; Cubizolles, M.; Nougier, C.; Negrier, C.; Pouteau, P.; Négrier, C. Society of Photo-optical Instrumentation Engineers. J. Biomed. Opt. 2011, 16, 57001. [Google Scholar] [CrossRef]
- Patiño-Velasco, M.M.; Andrade-Eraso, C.; Vásquez-López, J.; Trivi, M.; Rabal, H.J. Blood coagulation measurements using dynamic speckle technique. In Proceedings of the VI Latin American Congress on Biomedical Engineering CLAIB 2014, Paraná, Argentina, 29–31 October 2014; Volume 49, pp. 91–94. [Google Scholar]
- Tripathi, M.M.; Hajjarian, Z.; Van Cott, E.M.; Nadkarni, S.K. Assessing blood coagulation status with laser speckle rheology. Biomed. Opt. Express 2014, 5, 817. [Google Scholar] [CrossRef]
- Araújo, A.C.O.; Domingues, R.B.; van Bellen, B. Determinação do INR: Comparação entre método convencional e dispositivo portátil. J. Vasc. Bras. 2014, 13, 88–93. [Google Scholar] [CrossRef]
- Savva, G.; Manousakis, K.; Ellinas, G. Eavesdropping-Aware Routing and Spectrum/Code Allocation in OFDM-Based EONs Using Spread Spectrum Techniques. J. Opt. Commun. Netw. 2019, 11, 409–421. [Google Scholar] [CrossRef]
- Boas, D.A.; Dunn, A.K. Laser speckle contrast imaging in biomedical optics. J. Biomed. Opt. 2010, 15, 011109. [Google Scholar] [CrossRef]
- Durila, M.; Kalincik, T.; Cvachovec, K.; Filho, R. Heparinase-modified thromboelastography can result in a fibrinolytic pattern. Anaesthesia 2010, 65, 864–865. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inputs | Outputs | ||||
|---|---|---|---|---|---|
| 0 | 0 | 1 | 0 | 0 | 0 |
| 0 | 1 | 0 | 1 | 0 | 0 |
| 1 | 0 | 0 | 0 | 1 | 0 |
| 1 | 1 | 0 | 0 | 0 | 1 |
| 10× | MI * | PR | CF | |||
|---|---|---|---|---|---|---|
| CS(m:s) | CT(m:s) | CT(m:s) | SI(m:s) | CT(m:s) | SI(m:s) | |
| Red | 9:33 | 5:20 | 5:03 | −40.54% | 3:28 | 46.78% |
| Green | 9:16 | 3:45 | 4:28 | −28.20% | 1:24 | 37.54% |
| Blue | 9:05 | 4:00 | 4:20 | −50.59% | 2:12 | 46.15% |
| Gray | 9:16 | 4:29 | 4:52 | −34.41% | 1:56 | 42.87% |
| Mean | 9:18 | 4:24 | 4:41 | −38.44% | 2:15 | 43.34% |
| SD | ±0:11 | ±0:42 | ±0:28 | ±9.54% | ±0:52 | ±4.22% |
| 20× | MI * | PR | CF | |||
|---|---|---|---|---|---|---|
| CS(m:s) | CT(m:s) | CT(m:s) | SI(m:s) | CT(m:s) | SI(m:s) | |
| Red | 11:05 | 5:00 | 4:23 | −30.71% | 1:43 | 39.79% |
| Green | 10:41 | 3:53 | 3:43 | −32.43% | 0:51 | 35.17% |
| Blue | 10:57 | 3:53 | 3:47 | −52.33% | 1:35 | 42.67% |
| Gray | 10:53 | 4:20 | 4:19 | −36.26% | 1:19 | 40.93% |
| Mean | 10:54 | 4:16 | 4:03 | −37.93% | 1:22 | 39.64% |
| SD | ±0:10 | ±0:32 | ±0:20 | ±9.87% | ±0:22 | ±3.20% |
| 50× | MI * | PR | CF | |||
|---|---|---|---|---|---|---|
| CS(m:s) | CT(m:s) | CT(m:s) | SI (m:s) | CT(m:s) | SI(m:s) | |
| Red | 10:25 | 5:25 | 4:15 | −92.45% | 2:48 | 57.60% |
| Green | 10:57 | 2:40 | 1:19 | −90.36% | 1:03 | 42.53% |
| Blue | 10:53 | 3:24 | 1:35 | −95.03% | 1:11 | 50.20% |
| Gray | 10:53 | 3:45 | 2:12 | −93.57% | 1:39 | 53.94% |
| Mean | 10:46 | 3:48 | 2:20 | −92.85% | 1:40 | 51.07% |
| SD | ±0:14 | ±1:09 | ±1:19 | ±1.96% | ±0:47 | ±6.44% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Louka, M.; Kaliviotis, E. Development of an Optical Method for the Evaluation of Whole Blood Coagulation. Biosensors 2021, 11, 113. https://doi.org/10.3390/bios11040113
Louka M, Kaliviotis E. Development of an Optical Method for the Evaluation of Whole Blood Coagulation. Biosensors. 2021; 11(4):113. https://doi.org/10.3390/bios11040113
Chicago/Turabian StyleLouka, Marinos, and Efstathios Kaliviotis. 2021. "Development of an Optical Method for the Evaluation of Whole Blood Coagulation" Biosensors 11, no. 4: 113. https://doi.org/10.3390/bios11040113
APA StyleLouka, M., & Kaliviotis, E. (2021). Development of an Optical Method for the Evaluation of Whole Blood Coagulation. Biosensors, 11(4), 113. https://doi.org/10.3390/bios11040113