
Nanomaterials Application in Orthodontics

 ,
,  ,
, 
 and
and 
Abstract
1. Introduction
2. Nano-Coatings in Orthodontic Archwires
2.1. Nano Coatings Reducing Friction on Orthodontic Archwires
2.2. Delivering Nanoparticles from an Elastomeric Ligature
2.3. Shape Memory Polymers (SMP) in Orthodontics
2.4. Control of Oral Biofilms during Orthodontic Treatment
3. Bracket Materials
4. Nanomaterials in Orthodontics
4.1. Silver Nanoparticles (AgNPs) Coating
4.2. Chitosan
4.3. Copper Oxide
4.4. Nitrogen-Doped Titanium Dioxide (N-Doped TiO2) Brackets
4.5. Zinc Oxide (ZnO)
5. Relationship between the Orthodontic Arch and Bracket Materials
6. Microbial Colonization Associated with Different Kinds of FOAs.
7. Introduction of Nanofillers or NP (Silver, TiO2) to Orthodontic Adhesives
8. Nanomaterials in Orthodontics and Their Use in the Nearest Future
9. Materials in Orthodontics and Their Use in the Nearest Future
10. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Song, W.; Ge, S. Application of Antimicrobial Nanoparticles in Dentistry. Molecules 2019, 24, 1033. [Google Scholar] [CrossRef] [PubMed]
- Sharan, J.; Singh, S.; Lale, S.V.; Mishra, M.; Koul, V.; Kharbanda, O.P. Applications of nanomaterials in dental science: A review. J. Nanosci. Nanotechnol. 2017, 17, 2235–2255. [Google Scholar] [CrossRef] [PubMed]
- Gkantidis, N.; Christou, P.; Topouzelis, N. The orthodontic-periodontic interrelationship in integrated treatment challenges: A systematic review. J. Oral Rehabil. 2010, 37, 377–390. [Google Scholar] [CrossRef] [PubMed]
- Behnaz, M.; Dalaie, K.; Mirmohammadsadeghi, H.; Salehi, H.; Rakhshan, V.; Aslani, F. Shear bond strength and adhesive remnant index of orthodontic brackets bonded to enamel using adhesive systems mixed with tio 2 nanoparticles. Dental Press J. Orthod. 2018, 23, 43.e1–43.e7. [Google Scholar] [CrossRef] [PubMed]
- Sevinç, B.A.; Hanley, L. Antibacterial activity of dental composites containing zinc oxide nanoparticles. J. Biomed. Mater. Res. Part B Appl. Biomater. 2010, 94, 22–31. [Google Scholar] [CrossRef]
- Boverhof, D.R.; Bramante, C.M.; Butala, J.H.; Clancy, S.F.; Lafranconi, W.M.; West, J.; Gordon, S.C. Comparative assessment of nanomaterial definitions and safety evaluation considerations. Regul. Toxicol. Pharmacol. 2015, 73, 137–150. [Google Scholar] [CrossRef] [PubMed]
- Chieruzzi, M.; Pagano, S.; Moretti, S.; Pinna, R.; Milia, E.; Torre, L.; Eramo, S. Nanomaterials for tissue engineering in dentistry. Nanomaterials 2016, 6, 134. [Google Scholar] [CrossRef]
- Feng, X.; Chen, A.; Zhang, Y.; Wang, J.; Shao, L.; Wei, L. Application of dental nanomaterials: Potential toxicity to the central nervous system. Int. J. Nanomed. 2015, 10, 3547–3565. [Google Scholar] [CrossRef]
- Redlich, M.; Katz, A.; Rapoport, L.; Wagner, H.D.; Feldman, Y.; Tenne, R. Improved orthodontic stainless steel wires coated with inorganic fullerene-like nanoparticles of WS2 impregnated in electroless nickel-phosphorous film. Dent. Mater. 2008, 24, 1640–1646. [Google Scholar] [CrossRef]
- Bourauel, C.; Fries, T.; Drescher, D.; Plietsch, R. Surface roughness of orthodontic wires via atomic force microscopy, laser specular reflectance, and profilometry. Eur. J. Orthod. 1998, 20, 79–92. [Google Scholar] [CrossRef]
- Alcock, J.P.; Barbour, M.E.; Sandy, J.R.; Ireland, A.J. Nanoindentation of orthodontic archwires: The effect of decontamination and clinical use on hardness, elastic modulus and surface roughness. Dent. Mater. 2009, 25, 1039–1043. [Google Scholar] [CrossRef] [PubMed]
- Doherty, U.B.; Benson, P.E.; Higham, S.M. Fluoride-releasing elastomeric ligatures assessed with the in situ caries model. Eur. J. Orthod. 2002, 24, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Miura, K.K.; Ito, I.Y.; Enoki, C.; Elias, A.M.; Matsumoto, M.A.N. Anticariogenic effect of fluoride-releasing elastomers in orthodontic patients. Braz. Oral Res. 2007, 21, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Nalbantgil, D.; Oztoprak, M.O.; Cakan, D.G.; Bozkurt, K.; Arun, T. Prevention of demineralization around orthodontic brackets using two different fluoride varnishes. Eur. J. Dent. 2013, 7, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.C.; Cho, J.W. Application of shape memory polyurethane in orthodontic. J. Mater. Sci. Mater. Med. 2010, 21, 2881–2886. [Google Scholar] [CrossRef]
- Meng, Q.; Hu, J. A review of shape memory polymer composites and blends. Compos. Part A Appl. Sci. Manuf. 2009, 40, 1661–1672. [Google Scholar] [CrossRef]
- Leng, J.; Lan, X.; Liu, Y.; Du, S. Shape-memory polymers and their composites: Stimulus methods and applications. Prog. Mater. Sci. 2011, 56, 1077–1135. [Google Scholar] [CrossRef]
- Allaker, R.P. Critical review in oral biology & medicine: The use of nanoparticles to control oral biofilm formation. J. Dent. Res. 2010, 89, 1175–1186. [Google Scholar] [CrossRef]
- Hill, W. Argyria; the Pharmacology of Silver; The Williams & Wilkins Company: Baltimore, MD, USA, 1939. [Google Scholar]
- Moolya, N.; Sharma, R.; Shetty, A.; Gupta, N.; Gupta, A.; Jalan, V. Orthodontic bracket designs and their impact on microbial profile and periodontal disease: A clinical trial. J. Orthod. Sci. 2014, 3, 125. [Google Scholar] [CrossRef]
- Monteiro, D.R.; Gorup, L.F.; Takamiya, A.S.; Ruvollo-Filho, A.C.; de Camargo, E.R.; Barbosa, D.B. The growing importance of materials that prevent microbial adhesion: Antimicrobial effect of medical devices containing silver. Int. J. Antimicrob. Agents 2009, 34, 103–110. [Google Scholar] [CrossRef]
- Yamamoto, K.; Ohashi, S.; Aono, M.; Kokubo, T.; Yamada, I.; Yamauchi, J. Antibacterial activity of silver ions implanted in SiO2 filler on oral streptococci. Dent. Mater. 1996, 12, 227–229. [Google Scholar] [CrossRef]
- Oh, K.T.; Choo, S.U.; Kim, K.M.; Kim, K.N. A stainless steel bracket for orthodontic application. Eur. J. Orthod. 2005, 27, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Eliades, T.; Zinelis, S.; Bourauel, C.; Eliades, G. Manufacturing of Orthodontic Brackets: A Review of Metallurgical Perspectives and Applications. Recent Patents Mater. Sci. 2010, 1, 135–139. [Google Scholar] [CrossRef]
- Ogiński, T.; Kawala, B.; Mikulewicz, M.; Antoszewska-Smith, J. A Clinical Comparison of Failure Rates of Metallic and Ceramic Brackets: A Twelve-Month Study. BioMed Res. Int. 2020, 2020. [Google Scholar] [CrossRef] [PubMed]
- Iijima, M.; Zinelis, S.; Papageorgiou, S.N.; Brantley, W.; Eliades, T. Orthodontic brackets. In Orthodontic Applications of Biomaterials; Elsevier: New York, NY, USA, 2017; pp. 75–96. [Google Scholar]
- Zinelis, S.; Sifakakis, I.; Katsaros, C.; Eliades, T. Microstructural and mechanical characterization of contemporary lingual orthodontic brackets. Eur. J. Orthod. 2014, 36, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Jithesh, C.; Venkataramana, V.; Penumatsa, N.; Reddy, S.N.; Poornima, K.Y.; Rajasigamani, K. Comparative evaluation of nickel discharge from brackets in artificial saliva at different time intervals. J. Pharm. Bioallied Sci. 2015, 7, S587–S593. [Google Scholar] [CrossRef]
- Platt, J.A.; Guzman, A.; Zuccari, A.; Thornburg, D.W.; Rhodes, B.F.; Oshida, Y.; Moore, B.K. Corrosion behavior of 2205 duplex stainless steel. Am. J. Orthod. Dentofac. Orthop. 1997, 112, 69–79. [Google Scholar] [CrossRef]
- Orthodontic Brackets Selection, Placement and Debonding. Available online: https://www.researchgate.net/publication/275582644_ORTHODONTIC_BRACKETS_SelectionPlacement_and_Debonding (accessed on 21 September 2020).
- Schiff, N.; Dalard, F.; Lissac, M.; Morgon, L.; Grosgogeat, B. Corrosion resistance of three orthodontic brackets: A comparative study of three fluoride mouthwashes. Eur. J. Orthod. 2005, 27, 541–549. [Google Scholar] [CrossRef]
- Nair, S.; Janardhanam, P.; Padmanabhan, R. Evaluation of the effect of bracket and archwire composition on frictional forces in the buccal segments. Indian J. Dent. Res. 2012, 23, 203. [Google Scholar] [CrossRef]
- Ali, O.; Makou, M.; Papadopoulos, T.; Eliades, G. Laboratory evaluation of modern plastic brackets. Eur. J. Orthod. 2012, 34, 595–602. [Google Scholar] [CrossRef]
- Matsui, S.; Umezaki, E.; Komazawa, D.; Otsuka, Y.; Suda, N. Evaluation of mechanical properties of esthetic brackets. J. Dent. Biomech. 2015, 6. [Google Scholar] [CrossRef] [PubMed]
- Sadat-Khonsari, R.; Moshtaghy, A.; Schlegel, V.; Kahl-Nieke, B.; Möller, M.; Bauss, O. Die Verformung von Kunststoffbrackets unter Torque-belastung: Eine Vergleichsstudie. J. Orofac. Orthop. 2004, 65, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Retamoso, L.B.; Luz, T.B.; Marinowic, D.R.; Machado, D.C.; De Menezes, L.M.; Freitas, M.P.M.; Oshima, H.M.S. Cytotoxicity of esthetic, metallic, and nickel-free orthodontic brackets: Cellular behavior and viability. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 70–74. [Google Scholar] [CrossRef]
- Russell, J.S. Current products and practice: Aesthetic orthodontic brackets. J. Orthod. 2005, 32, 146–163. [Google Scholar] [CrossRef] [PubMed]
- Kloukos, D.; Pandis, N.; Eliades, T. Bisphenol-A and residual monomer leaching from orthodontic adhesive resins and polycarbonate brackets: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2013, 143. [Google Scholar] [CrossRef]
- Elekdag-Türk, S.; Yilmaz (née Huda Ebulkbash), H. Ceramic Brackets Revisited. In Current Approaches in Orthodontics; IntechOpen: London, UK, 2019. [Google Scholar]
- Venugopal, A.; Muthuchamy, N.; Tejani, H.; Anantha-Iyenga-Gopalan; Lee, K.P.; Lee, H.J.; Kyung, H.M. Incorporation of silver nanoparticles on the surface of orthodontic microimplants to achieve antimicrobial properties. Korean J. Orthod. 2017, 47, 3–10. [Google Scholar] [CrossRef]
- Padovani, G.C.; Feitosa, V.P.; Sauro, S.; Tay, F.R.; Durán, G.; Paula, A.J.; Durán, N. Advances in Dental Materials through Nanotechnology: Facts, Perspectives and Toxicological Aspects. Trends Biotechnol. 2015, 33, 621–636. [Google Scholar] [CrossRef]
- Kasraei, S.; Sami, L.; Hendi, S.; AliKhani, M.-Y.; Rezaei-Soufi, L.; Khamverdi, Z. Antibacterial properties of composite resins incorporating silver and zinc oxide nanoparticles on Streptococcus mutans and Lactobacillus. Restor. Dent. Endod. 2014, 39, 109. [Google Scholar] [CrossRef]
- Arun, D.; Adikari Mudiyanselage, D.; Gulam Mohamed, R.; Liddell, M.; Monsur Hassan, N.M.; Sharma, D. Does the Addition of Zinc Oxide Nanoparticles Improve the Antibacterial Properties of Direct Dental Composite Resins? A Systematic Review. Materials (Basel) 2020, 14, 40. [Google Scholar] [CrossRef]
- Targino, A.G.R.; Flores, M.A.P.; Dos Santos, V.E.; De Godoy Bené Bezerra, F.; De Luna Freire, H.; Galembeck, A.; Rosenblatt, A. An innovative approach to treating dental decay in children. A new anti-caries agent. J. Mater. Sci. Mater. Med. 2014, 25, 2041–2047. [Google Scholar] [CrossRef]
- Kalaivani, R.; Maruthupandy, M.; Muneeswaran, T.; Hameedha Beevi, A.; Anand, M.; Ramakritinan, C.M.; Kumaraguru, A.K. Synthesis of chitosan mediated silver nanoparticles (Ag NPs) for potential antimicrobial applications. Front. Lab. Med. 2018, 2, 30–35. [Google Scholar] [CrossRef]
- Vargas-Reus, M.A.; Memarzadeh, K.; Huang, J.; Ren, G.G.; Allaker, R.P. Antimicrobial activity of nanoparticulate metal oxides against peri-implantitis pathogens. Int. J. Antimicrob. Agents 2012, 40, 135–139. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Su, P.; Chen, S.; Wang, N.; Ma, Y.; Liu, Y.; Wang, J.; Zhang, Z.; Li, H.; Webster, T.J. Synthesis of TiO2 nanotubes with ZnO nanoparticles to achieve antibacterial properties and stem cell compatibility. Nanoscale 2014, 6, 9050–9062. [Google Scholar] [CrossRef] [PubMed]
- Sodagar, A.; Akhoundi, M.S.A.; Bahador, A.; Jalali, Y.F.; Behzadi, Z.; Elhaminejad, F.; Mirhashemi, A.H. Effect of TiO2 nanoparticles incorporation on antibacterial properties and shear bond strength of dental composite used in orthodontics. Dental Press J. Orthod. 2017, 22, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Liu, X.; Xie, Y.; Zhang, Q.; Zhang, W.; Jiang, X.; Lin, J. Biological Safe Gold Nanoparticle-Modified Dental Aligner Prevents the Porphyromonas gingivalis Biofilm Formation. ACS Omega 2020, 5, 18685–18692. [Google Scholar] [CrossRef]
- Roveri, N.; Battistella, E.; Foltran, I.; Foresti, E.; Iafisco, M.; Lelli, M.; Palazzo, B.; Rimondini, L. Synthetic biomimetic carbonate-hydroxyapatite nanocrystals for enamel remineralization. In Proceedings of the Advanced Materials Research; Trans Tech Publications: Cham, Switzerland, 2008; Volume 47–50, Part 2. pp. 821–824. [Google Scholar]
- Chen, C.; Weir, M.D.; Cheng, L.; Lin, N.J.; Lin-Gibson, S.; Chow, L.C.; Zhou, X.; Xu, H.H.K. Antibacterial activity and ion release of bonding agent containing amorphous calcium phosphate nanoparticles. Dent. Mater. 2014, 30, 891–901. [Google Scholar] [CrossRef]
- Ladd, M.R.; Lee, S.J.; Stitzel, J.D.; Atala, A.; Yoo, J.J. Co-electrospun dual scaffolding system with potential for muscle-tendon junction tissue engineering. Biomaterials 2011, 32, 1549–1559. [Google Scholar] [CrossRef]
- Huang, Z.; Sargeant, T.D.; Hulvat, J.F.; Mata, A.; Bringas, P.; Koh, C.Y.; Stupp, S.I.; Snead, M.L. Bioactive nanofibers instruct cells to proliferate and differentiate during enamel regeneration. J. Bone Miner. Res. 2008, 23, 1995–2006. [Google Scholar] [CrossRef]
- Batra, P. Nanoparticles and their Applications in Orthodontics. Adv. Dent. Oral Health 2016, 2. [Google Scholar] [CrossRef]
- Borzabadi-Farahani, A.; Borzabadi, E.; Lynch, E. Nanoparticles in orthodontics, a review of antimicrobial and anti-caries applications. Acta Odontol. Scand. 2014, 72, 413–417. [Google Scholar] [CrossRef]
- Bapat, R.A.; Chaubal, T.V.; Joshi, C.P.; Bapat, P.R.; Choudhury, H.; Pandey, M.; Gorain, B.; Kesharwani, P. An overview of application of silver nanoparticles for biomaterials in dentistry. Mater. Sci. Eng. C 2018, 91, 881–898. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Gómora, A.E.; Lara-Carrillo, E.; Robles-Navarro, J.B.; Scougall-Vilchis, R.J.; Hernández-López, S.; Medina-Solís, C.E.; Morales-Luckie, R.A. Biosynthesis of silver nanoparticles on orthodontic elastomeric modules: Evaluation of mechanical and antibacterial properties. Molecules 2017, 22, 1407. [Google Scholar] [CrossRef] [PubMed]
- Mhaske, A.R.; Shetty, P.C.; Bhat, N.S.; Ramachandra, C.S.; Laxmikanth, S.M.; Nagarahalli, K.; Tekale, P.D. Antiadherent and antibacterial properties of stainless steel and NiTi orthodontic wires coated with silver against Lactobacillus acidophilus—an in vitro study. Prog. Orthod. 2015, 16. [Google Scholar] [CrossRef]
- Espinosa-Cristóbal, L.F.; López-Ruiz, N.; Cabada-Tarín, D.; Reyes-López, S.Y.; Zaragoza-Contreras, A.; Constandse-Cortéz, D.; Donohué-Cornejo, A.; Tovar-Carrillo, K.; Cuevas-González, J.C.; Kobayashi, T. Antiadherence and antimicrobial properties of silver nanoparticles against streptococcus mutans on brackets and wires used for orthodontic treatments. J. Nanomater. 2018, 2018. [Google Scholar] [CrossRef]
- Besinis, A.; Hadi, S.D.; Le, H.R.; Tredwin, C.; Handy, R.D. Antibacterial activity and biofilm inhibition by surface modified titanium alloy medical implants following application of silver, titanium dioxide and hydroxyapatite nanocoatings. Nanotoxicology 2017, 11, 327–338. [Google Scholar] [CrossRef] [PubMed]
- Besinis, A.; De Peralta, T.; Handy, R.D. Inhibition of biofilm formation and antibacterial properties of a silver nano-coating on human dentine. Nanotoxicology 2014, 8, 745–754. [Google Scholar] [CrossRef] [PubMed]
- Tuan, T.Q.; Van Son, N.; Dung, H.T.K.; Luong, N.H.; Thuy, B.T.; Van Anh, N.T.; Hoa, N.D.; Hai, N.H. Preparation and properties of silver nanoparticles loaded in activated carbon for biological and environmental applications. J. Hazard. Mater. 2011, 192, 1321–1329. [Google Scholar] [CrossRef] [PubMed]
- Vanitha, G.; Rajavel, K.; Boopathy, G.; Veeravazhuthi, V.; Neelamegam, P. Physiochemical charge stabilization of silver nanoparticles and its antibacterial applications. Chem. Phys. Lett. 2017, 669, 71–79. [Google Scholar] [CrossRef]
- Bürgers, R.; Eidt, A.; Frankenberger, R.; Rosentritt, M.; Schweikl, H.; Handel, G.; Hahnel, S. The anti-adherence activity and bactericidal effect of microparticulate silver additives in composite resin materials. Arch. Oral Biol. 2009, 54, 595–601. [Google Scholar] [CrossRef]
- Espinosa-Cristóbal, L.F.; Martinez-Castanon, G.A.; Téllez-Déctor, E.J.; Niño-Martínez, N.; Zavala-Alonso, N.V.; Loyola-Rodríguez, J.P. Adherence inhibition of Streptococcus mutans on dental enamel surface using silver nanoparticles. Mater. Sci. Eng. C 2013, 33, 2197–2202. [Google Scholar] [CrossRef]
- PRIME PubMed | Nanosilver Coated Orthodontic Brackets: In Vivo Antibacterial Properties and Ion Release. Available online: https://wwww.unboundmedicine.com/medline/citation/26787659/Nanosilver_coated_orthodontic_brackets:_in_vivo_antibacterial_properties_and_ion_release_ (accessed on 13 July 2020).
- Kim, J.-S.; Shin, D.-H. Inhibitory effect on Streptococcus mutans and mechanical properties of the chitosan containing composite resin. Restor. Dent. Endod. 2013, 38, 36. [Google Scholar] [CrossRef] [PubMed]
- Inhibitory Effect of Water-Soluble Chitosan on Growth of Streptococcus Mutans—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/14964411/ (accessed on 14 July 2020).
- Ikinci, G.; Şenel, S.; Akincibay, H.; Kaş, S.; Erciş, S.; Wilson, C.G.; Hincal, A.A. Effect of chitosan on a periodontal pathogen Porphyromonas gingivalis. Int. J. Pharm. 2002, 235, 121–127. [Google Scholar] [CrossRef]
- Yassaei, S.; Nasr, A.; Zandi, H.; Motallaei, M.N. Comparison of antibacterial effects of orthodontic composites containing different nanoparticles on Streptococcus mutans at different times. Dental Press J. Orthod. 2020, 25, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Eshed, M.; Lellouche, J.; Matalon, S.; Gedanken, A.; Banin, E. Sonochemical coatings of ZnO and CuO nanoparticles inhibit streptococcus mutans biofilm formation on teeth model. Langmuir 2012, 28, 12288–12295. [Google Scholar] [CrossRef]
- The Effect of CuO Nanoparticles on Antimicrobial Effects and Shear Bond Strength of Orthodontic Adhesives—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/29492409/ (accessed on 16 July 2020).
- Poosti, M.; Ramazanzadeh, B.; Zebarjad, M.; Javadzadeh, P.; Naderinasab, M.; Shakeri, M.T. Shear bond strength and antibacterial effects of orthodontic composite containing TiO2 nanoparticles. Eur. J. Orthod. 2013, 35, 676–679. [Google Scholar] [CrossRef]
- Salehi, P.; Babanouri, N.; Roein-Peikar, M.; Zare, F. Long-term antimicrobial assessment of orthodontic brackets coated with nitrogen-doped titanium dioxide against Streptococcus mutans. Prog. Orthod. 2018, 19, 35. [Google Scholar] [CrossRef]
- Ahn, S.J.; Lee, S.J.; Kook, J.K.; Lim, B.S. Experimental antimicrobial orthodontic adhesives using nanofillers and silver nanoparticles. Dent. Mater. 2009, 25, 206–213. [Google Scholar] [CrossRef]
- Cao, B.; Wang, Y.; Li, N.; Liu, B.; Zhang, Y. Preparation of an orthodontic bracket coated with an nitrogen-doped TiO2-xNy thin film and examination of its antimicrobial performance. Dent. Mater. J. 2013, 32, 311–316. [Google Scholar] [CrossRef]
- Kachoei, M.; Eskandarinejad, F.; Divband, B.; Khatamian, M. The effect of zinc oxide nanoparticles deposition for friction reduction on orthodontic wires. Dent. Res. J. (Isfahan) 2013, 10, 499–505. [Google Scholar] [CrossRef]
- Behroozian, A.; Kachoei, M.; Khatamian, M.; Divband, B. The effect of ZnO nanoparticle coating on the frictionalresistance between orthodontic wires and ceramic brackets. J. Dent. Res. Dent. Clin. Dent. Prospects 2016, 10, 106–111. [Google Scholar] [CrossRef]
- Goto, M.; Kasahara, A.; Tosa, M. Low-friction coatings of zinc oxide synthesized by optimization of crystal preferred orientation. Tribol. Lett. 2011, 43, 155–162. [Google Scholar] [CrossRef]
- Rossouw, P.E. Friction: An overview. Semin. Orthod. 2003, 9, 218–222. [Google Scholar] [CrossRef]
- Influence of Fluid Media on the Frictional Coefficients in Orthodontic Sliding | Request PDF. Available online: https://www.researchgate.net/publication/248866046_Influence_of_fluid_media_on_the_frictional_coefficients_in_orthodontic_sliding (accessed on 13 September 2020).
- Kusy, R.P.; Whitley, J.Q. Influence of archwire and bracket dimensions on sliding mechanics: Derivations and determinations of the critical contact angles for binding. Eur. J. Orthod. 1999, 21, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Drescher, D.; Bourauel, C.; Schumacher, H.A. Frictional forces between bracket and arch wire. Am. J. Orthod. Dentofac. Orthop. 1989, 96, 397–404. [Google Scholar] [CrossRef]
- Frank, C.A.; Nikolai, R.J. A comparative study of frictional resistances between orthodontic bracket and arch wire. Am. J. Orthod. 1980, 78, 593–609. [Google Scholar] [CrossRef]
- Kusy, R.P.; Whitley, J.Q.; Ambrose, W.W.; Newman, J.G. Evaluation of titanium brackets for orthodontic treatment: Part I. The passive configuration. Am. J. Orthod. Dentofac. Orthop. 1998, 114, 558–572. [Google Scholar] [CrossRef]
- Pratten, D.H.; Popli, K.; Germane, N.; Gunsolley, J.C. Frictional resistance of ceramic and stainless steel orthodontic brackets. Am. J. Orthod. Dentofac. Orthop. 1990, 98, 398–403. [Google Scholar] [CrossRef]
- Baker, K.L.; Nieberg, L.G.; Weimer, A.D.; Hanna, M. Frictional changes in force values caused by saliva substitution. Am. J. Orthod. Dentofac. Orthop. 1987, 91, 316–320. [Google Scholar] [CrossRef]
- Sapata, D.M.; Ramos, A.L.; Sábio, S.; Normando, D.; Pascotto, R.C. Evaluation of biofilm accumulation on and deactivation force of orthodontic Ni-Ti archwires before and after exposure to an oral medium: A prospective clinical study. J. Dent. Res. Dent. Clin. Dent. Prospects 2020, 14, 41–47. [Google Scholar] [CrossRef]
- Lin, J.; Han, S.; Zhu, J.; Wang, X.; Chen, Y.; Vollrath, O.; Wang, H.; Mehl, C. Influence of fluoride-containing acidic artificial saliva on the mechanical properties of Nickel-Titanium orthodontics wires. Indian J. Dent. Res. 2012, 23, 591–595. [Google Scholar] [CrossRef]
- Wichelhaus, A.; Geserick, M.; Hibst, R.; Sander, F.G. The effect of surface treatment and clinical use on friction in NiTi orthodontic wires. Dent. Mater. 2005, 21, 938–945. [Google Scholar] [CrossRef] [PubMed]
- Sukontapatipark, W.; El-Agroudi, M.A.; Selliseth, N.J.; Thunold, K.; Selvig, K.A. Bacterial colonization associated with fixed orthodontic appliances. A scanning electron microscopy study. Eur. J. Orthod. 2001, 23, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Hägg, U.; Kaveewatcharanont, P.; Samaranayake, Y.H.; Samaranayake, L.P. The effect of fixed orthodontic appliances on the oral carriage of Candida species and Enterobacteriaceae. Eur. J. Orthod. 2004, 26, 623–629. [Google Scholar] [CrossRef] [PubMed]
- Anhoury, P.; Nathanson, D.; Hughes, C.V.; Socransky, S.; Feres, M.; Chou, L.L. Microbial profile on metallic and ceramic bracket materials. Angle Orthod. 2002, 72. [Google Scholar] [CrossRef]
- Boyd, R.L.; Baumrind, S. Periodontal considerations in the use of bonds or bands on molars in adolescents and adults. Angle Orthod. 1992, 62. [Google Scholar] [CrossRef]
- Stobie, N.; Duffy, B.; McCormack, D.E.; Colreavy, J.; Hidalgo, M.; McHale, P.; Hinder, S.J. Prevention of Staphylococcus epidermidis biofilm formation using a low-temperature processed silver-doped phenyltriethoxysilane sol-gel coating. Biomaterials 2008, 29, 963–969. [Google Scholar] [CrossRef]
- Abstract—Europe PMC. Available online: https://europepmc.org/article/med/19339161 (accessed on 9 December 2020).
- Hernández-Sierra, J.F.; Ruiz, F.; Cruz Pena, D.C.; Martínez-Gutiérrez, F.; Martínez, A.E.; de Jesús Pozos Guillén, A.; Tapia-Pérez, H.; Martínez Castañón, G. The antimicrobial sensitivity of Streptococcus mutans to nanoparticles of silver, zinc oxide, and gold. Nanomed. Nanotechnol. Biol. Med. 2008, 4, 237–240. [Google Scholar] [CrossRef]
- Radford, D.R.; Challacombe, S.J.; Walter, J.D. Denture plaque and adherence of Candida albicans to denture-base materials in vivo and in vitro. Crit. Rev. Oral Biol. Med. 1999, 10, 99–116. [Google Scholar] [CrossRef]
- Monteiro, D.R.; Gorup, L.F.; Takamiya, A.S.; de Camargo, E.R.; Filho, A.C.R.; Barbosa, D.B. Silver Distribution and Release from an Antimicrobial Denture Base Resin Containing Silver Colloidal Nanoparticles. J. Prosthodont. 2012, 21, 7–15. [Google Scholar] [CrossRef]
- Spampinato, C.; Leonardi, D. Candida infections, causes, targets, and resistance mechanisms: Traditional and alternative antifungal agents. BioMed Res. Int. 2013, 2013. [Google Scholar] [CrossRef]
- Hibino, K.; Wong, R.W.K.; HÄgg, U.; Samaranayake, L.P. The effects of orthodontic appliances on Candida in the human mouth. Int. J. Paediatr. Dent. 2009, 19, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Arendorf, T.; Addy, M. Candidal carriage and plaque distribution before, during and after removable orthodontic appliance therapy. J. Clin. Periodontol. 1985, 12, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Sodagar, A.; Bahador, A.; Khalil, S.; Saffar Shahroudi, A.; Zaman Kassaee, M. The effect of TiO2 and SiO2 nanoparticles on flexural strength of poly (methyl methacrylate) acrylic resins. J. Prosthodont. Res. 2013, 57, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Juvvadi, S.; Rammohan, S.; Gandikota, C.; Challa, P.; Manne, R.; Mathur, A. Adherence of Streptococcus mutans and Candida albicans to different bracket materials. J. Pharm. Bioallied Sci. 2012, 4, 212. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, J.M.; Jenkinson, H.F.; Cannon, R.D. Adhesion of Candida albicans to oral streptococci is promoted by selective adsorption of salivary proteins to the streptococcal cell surface. Microbiology 2000, 146, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Forsberg, C.M.; Brattström, V.; Malmberg, E.; Nord, C.E. Ligature wires and elastomeric rings: Two methods of ligation, and their association with microbial colonization of streptococcus mutans and iactobacilli. Eur. J. Orthod. 1991, 13, 416–420. [Google Scholar] [CrossRef]
- Brusca, M.I.; Chara, O.; Sterin-Borda, L.; Rosa, A.C. Influence of different orthodontic brackets on adherence of microorganisms in vitro. Angle Orthod. 2007, 77, 331–336. [Google Scholar] [CrossRef]
- Lim, B.S.; Lee, S.J.; Lee, J.W.; Ahn, S.J. Quantitative analysis of adhesion of cariogenic streptococci to orthodontic raw materials. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 882–888. [Google Scholar] [CrossRef]
- Colony forming Unit Levels of Salivary Lactobacilli and Streptococcus Mutans in Orthodontic Patients—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/16302600/ (accessed on 20 September 2020).
- Desoet, J.J.; Van Loveren, C.; Lammens, A.J.; Pavićič, M.; Hamburg, C.; Ten Cate, J.M.; De Graaff, J. Differences in cariogenicity between fresh isolates of streptococcus sobrinus and streptococcus mutans. Caries Res. 1991, 25, 116–122. [Google Scholar] [CrossRef]
- Neel, A.; Bozec, L.; Perez, R.A.; Kim, H.-W.; Knowles, J.C. Nanotechnology in dentistry: Prevention, diagnosis, and therapy. Int. J. Nanomed. 2015, 10, 6371. [Google Scholar] [CrossRef]
- Shrestha, A.; Kishen, A. Antibacterial Nanoparticles in Endodontics: A Review. J. Endod. 2016, 42, 1417–1426. [Google Scholar] [CrossRef] [PubMed]
- Raura, N.; Garg, A.; Arora, A.; Roma, M. Nanoparticle technology and its implications in endodontics: A review. Biomater. Res. 2020, 24, 21. [Google Scholar] [CrossRef] [PubMed]
- Roberts-Harry, D.; Sandy, J. Orthodontics. Part 9: Anchorage control and distal movement. Br. Dent. J. 2004, 196, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Stress in Dentistry—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/9828615/ (accessed on 14 January 2021).
- Biocompatibility and Toxicity of Nanoparticles and Nanotubes. Available online: https://www.hindawi.com/journals/jnm/2012/548389/ (accessed on 14 January 2021).
- Subramani, K.; Huja, S.; Kluemper, G.T.; Morford, L.; Hartsfield, J.K. Nanotechnology in Orthodontics-1: The Past, Present, and a Perspective of the Future. In Nanobiomaterials in Clinical Dentistry; Elsevier Inc.: New York, NY, USA, 2012; pp. 231–247. ISBN 9781455731275. [Google Scholar]
- Eliades, T. Orthodontic material applications over the past century: Evolution of research methods to address clinical queries. Am. J. Orthod. Dentofac. Orthop. 2015, 147, S224–S231. [Google Scholar] [CrossRef][Green Version]
- Lendlein, A.; Jiang, H.; Jünger, O.; Langer, R. Light-induced shape-memory polymers. Nature 2005, 434, 879–882. [Google Scholar] [CrossRef]
- Cordier, P.; Tournilhac, F.; Soulié-Ziakovic, C.; Leibler, L. Self-healing and thermoreversible rubber from supramolecular assembly. Nature 2008, 451, 977–980. [Google Scholar] [CrossRef]
- Berengueres, J.; Saito, S.; Tadakuma, K. Structural properties of a scaled gecko foot-hair. Bioinspir. Biomim. 2007, 2, 1–8. [Google Scholar] [CrossRef]
- Lee, H.; Lee, B.P.; Messersmith, P.B. A reversible wet/dry adhesive inspired by mussels and geckos. Nature 2007, 448, 338–341. [Google Scholar] [CrossRef]
- Özyildiz, F.; Uzel, A.; Hazar, A.S.; Güden, M.; Ölmez, S.; Aras, I.; Karaboz, İ. Photocatalytic antimicrobial effect of TiO2 anatase thin-film–coated orthodontic arch wires on 3 oral pathogens. Turkish J. Biol. 2014, 38, 289–295. [Google Scholar] [CrossRef]
- Brantley, W.A.; Eliades, T. The Role of Biomedical Engineers in the Design and Manufacture of Customized Orthodontic Appliances. In Integrated Clinical Orthodontics; John Wiley and Sons: New York, NY, USA, 2013; pp. 366–379. ISBN 9781444335972. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nanomaterial | Method of Use | Application | References |
|---|---|---|---|
| Silver NPs (AgNPs) | Applied as a coating agent on titanium | Implants | [40,41] |
| Zinc oxide NPs (ZnONPs) | Incorporated into dental resins | Resin composite adhesives | [42,43] |
| Chitosan NPs | Conjugated with silver nanoparticles | Resin composites adhesives | [44,45] |
| Copper (I) oxide NPs (Cu2ONPs) | Antimicrobial effect in resin adhesives | Resin composites adhesives | [46] |
| Titanium (IV) oxide NPs (TiO2NPs) | Nanotubes on titanium surfaces and incorporated with ZnONPs | Implants | [47,48] |
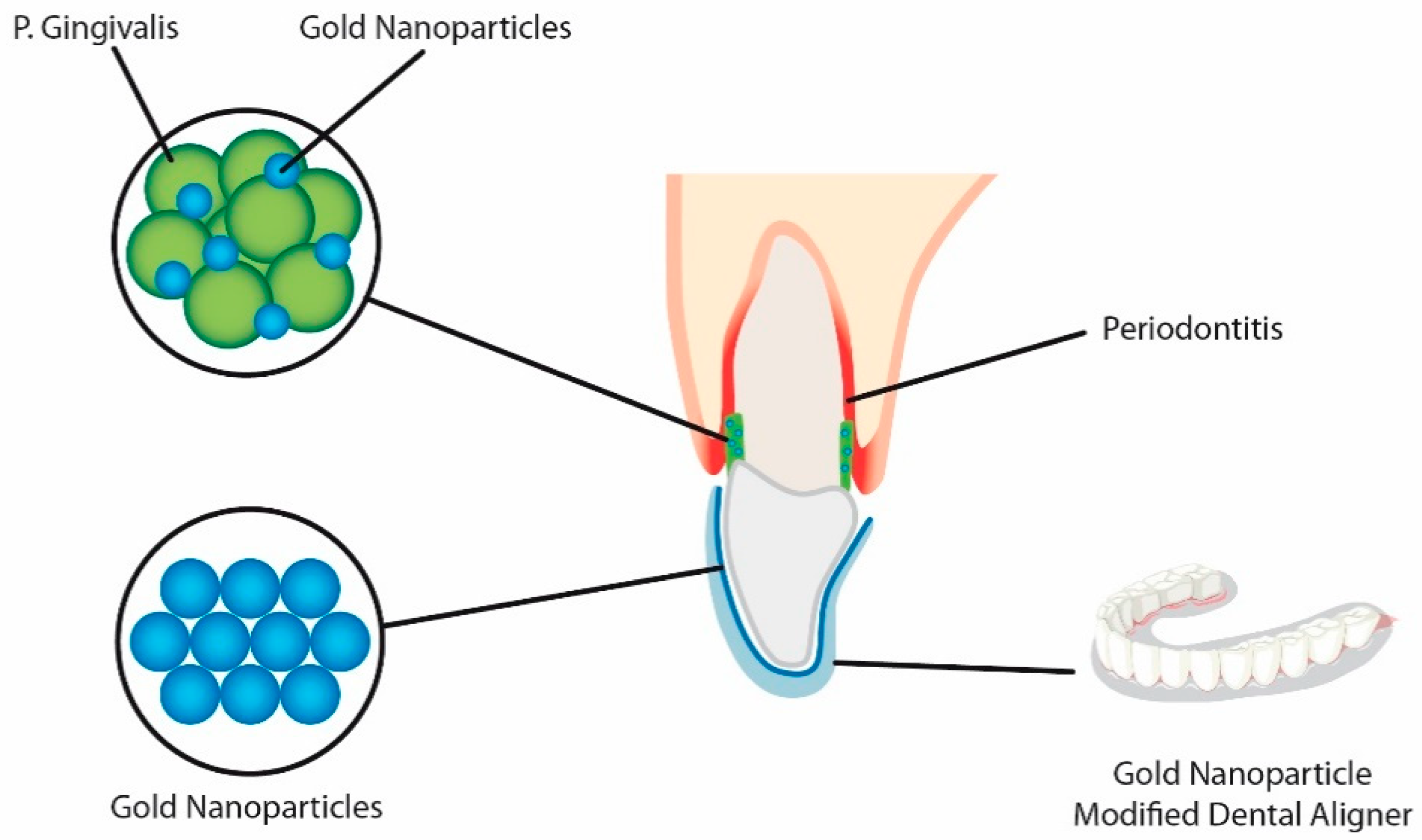
| Gold NPs (AuNPs) | Modified gold nanoparticles (AuDAPT) coated onto orthodontic aligners | Antimicrobial coated aligner | [49] |
| Carbonate hydroxyapatite nanocrystal | Antibacterial and antidemineralizing properties | Toothpastes, mouthwashes and composite resins | [50] |
| Amorphous Calcium Phosphate (ACP) | Antibacterial and antidemineralizing properties | Antibacterial and antidemineralizing properties | [51] |
| Novel Poly(l-lactic acid) (PLLA)/Multi-walled carbon nanotubes (MWNTs)/hydroxyapatite (HA) nanofibrous scaffolds | Polymer solution FOR entire-tooth regeneration | Dental Surface applications | [52] |
| Bioactive peptide—Amphiphile nanofibers | Branched peptide Amphiphile molecules containing the peptide motif Arg-Gly-Asp, or “RGD” | Dental surface applications | [53] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zakrzewski, W.; Dobrzynski, M.; Dobrzynski, W.; Zawadzka-Knefel, A.; Janecki, M.; Kurek, K.; Lubojanski, A.; Szymonowicz, M.; Rybak, Z.; Wiglusz, R.J. Nanomaterials Application in Orthodontics. Nanomaterials 2021, 11, 337. https://doi.org/10.3390/nano11020337
Zakrzewski W, Dobrzynski M, Dobrzynski W, Zawadzka-Knefel A, Janecki M, Kurek K, Lubojanski A, Szymonowicz M, Rybak Z, Wiglusz RJ. Nanomaterials Application in Orthodontics. Nanomaterials. 2021; 11(2):337. https://doi.org/10.3390/nano11020337
Chicago/Turabian StyleZakrzewski, Wojciech, Maciej Dobrzynski, Wojciech Dobrzynski, Anna Zawadzka-Knefel, Mateusz Janecki, Karolina Kurek, Adam Lubojanski, Maria Szymonowicz, Zbigniew Rybak, and Rafal J. Wiglusz. 2021. "Nanomaterials Application in Orthodontics" Nanomaterials 11, no. 2: 337. https://doi.org/10.3390/nano11020337
APA StyleZakrzewski, W., Dobrzynski, M., Dobrzynski, W., Zawadzka-Knefel, A., Janecki, M., Kurek, K., Lubojanski, A., Szymonowicz, M., Rybak, Z., & Wiglusz, R. J. (2021). Nanomaterials Application in Orthodontics. Nanomaterials, 11(2), 337. https://doi.org/10.3390/nano11020337