Comparative Assessment and External Validation of Hepatic Steatosis Formulae in a Community-Based Setting


Abstract
:1. Introduction
2. Materials and Methods
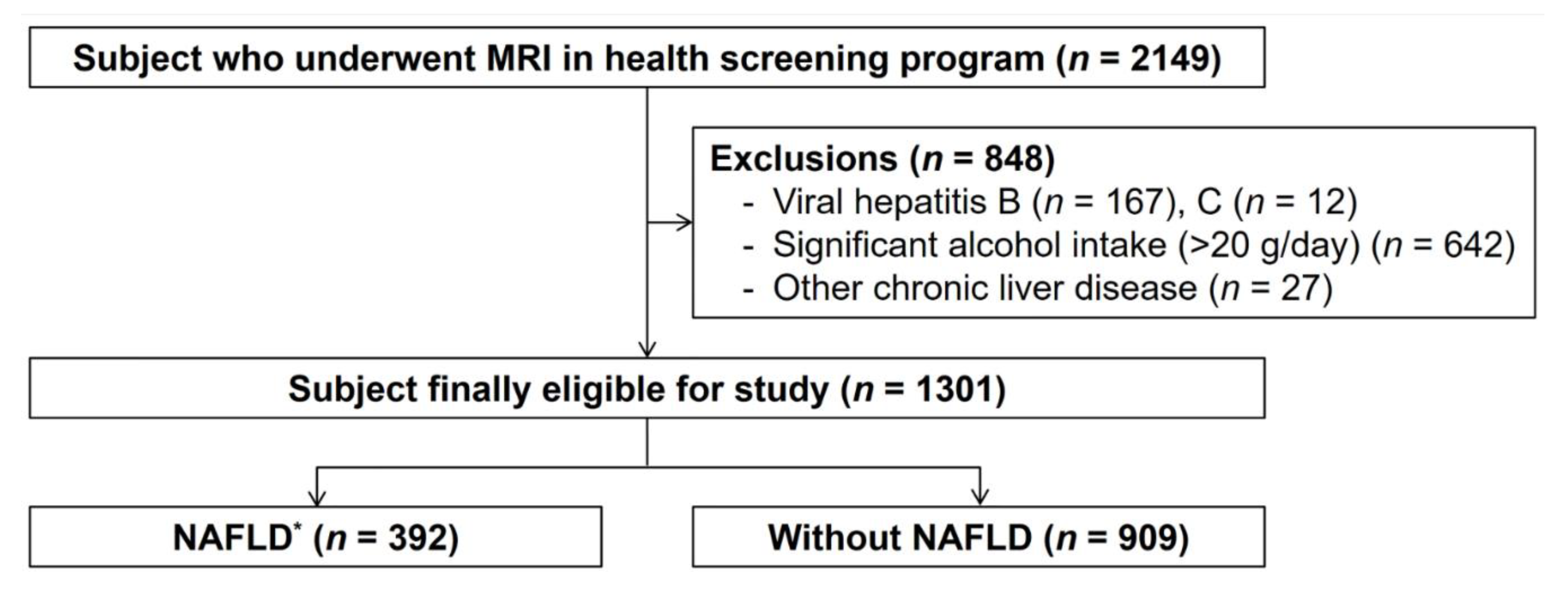
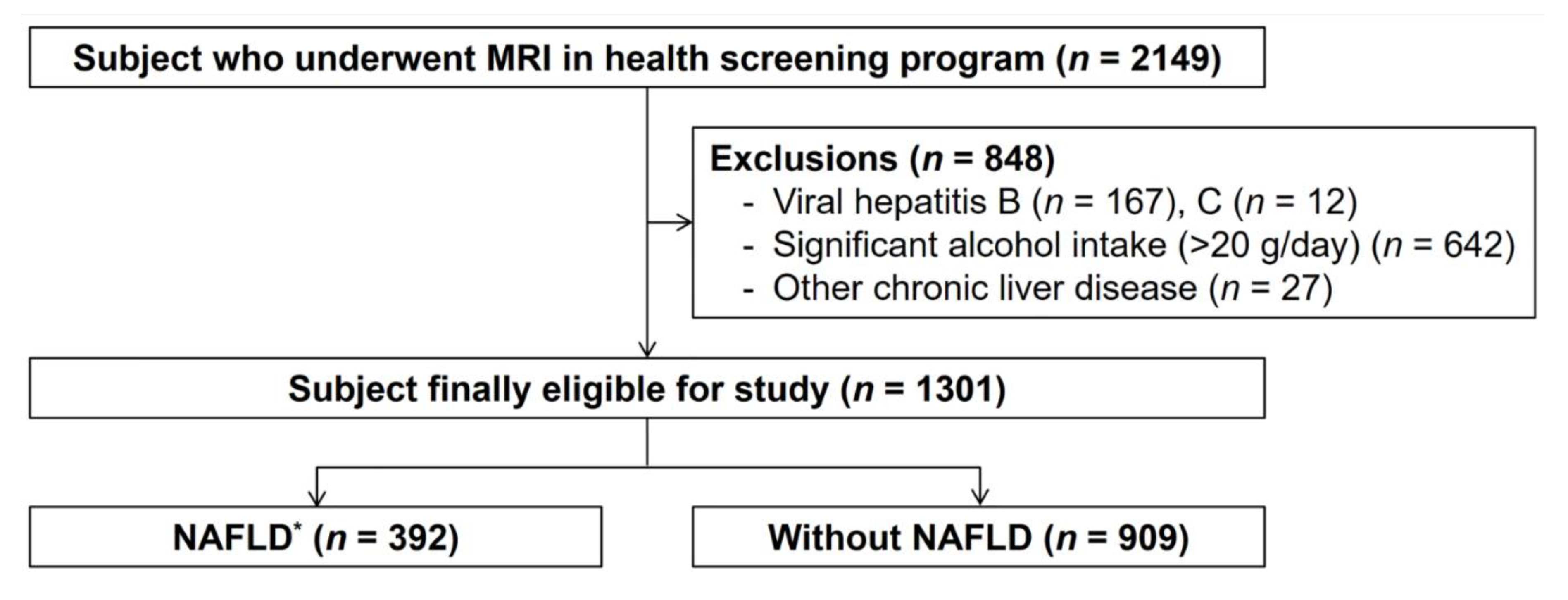
2.1. Study Population
2.2. Inclusion and Exclusion Criteria
2.3. Imaging Assessment
2.4. Fat Fraction Quantification
2.5. Anthropometric Measurements
2.6. Definitions
2.7. Biochemical Tests
2.8. Estimation Formulae for Hepatic Steatosis
- Fatty liver index (FLI) [20] = ex/(1 + ex), where X = 0.953 × Loge(TG, mg/dL) + 0.139 × (body mass index (BMI), kg/m2) + 0.718 × Loge(GGT, U/L) + 0.053 × (waist circumference, cm) − 15.745;
- Hepatic steatosis index (HSI) [18] = 8 × ALT/AST ratio + BMI (+2 if type 2 diabetic; +2 if female);
- ZJU index [21] = BMI (kg/m2) + fasting plasma glucose (mmol/L) + TG (mmol/L) + 3 × ALT/AST ratio (+2 if female);
- NAFLD liver fat score (NAFLD-LFS) [17] = −2.89 + 1.18 × (metabolic syndrome—yes = 1, no = 0) + 0.45 × (type 2 diabetes—yes = 2, no = 0) + 0.15 × (fasting serum insulin, mU/L) + 0.04 × (AST, IU/L) − 0.94 × (AST/ALT);
- Framingham steatosis index (FSI) [22] = ex/(1 + ex), where X = −7.981 + 0.011 × age (years) − 0.146 × sex (female = 1, male = 0) + 0.173 × BMI (kg/m2) + 0.007 × TG (mg/dL) + 0.593 × hypertension (yes = 1, no = 0) + 0.789 × diabetes (yes = 1, no = 0) + 1.1 × ALT:AST ratio ≥ 1.33 (yes = 1, no = 0).
2.9. Statistical Analysis
3. Results
3.1. Baseline Characteristics
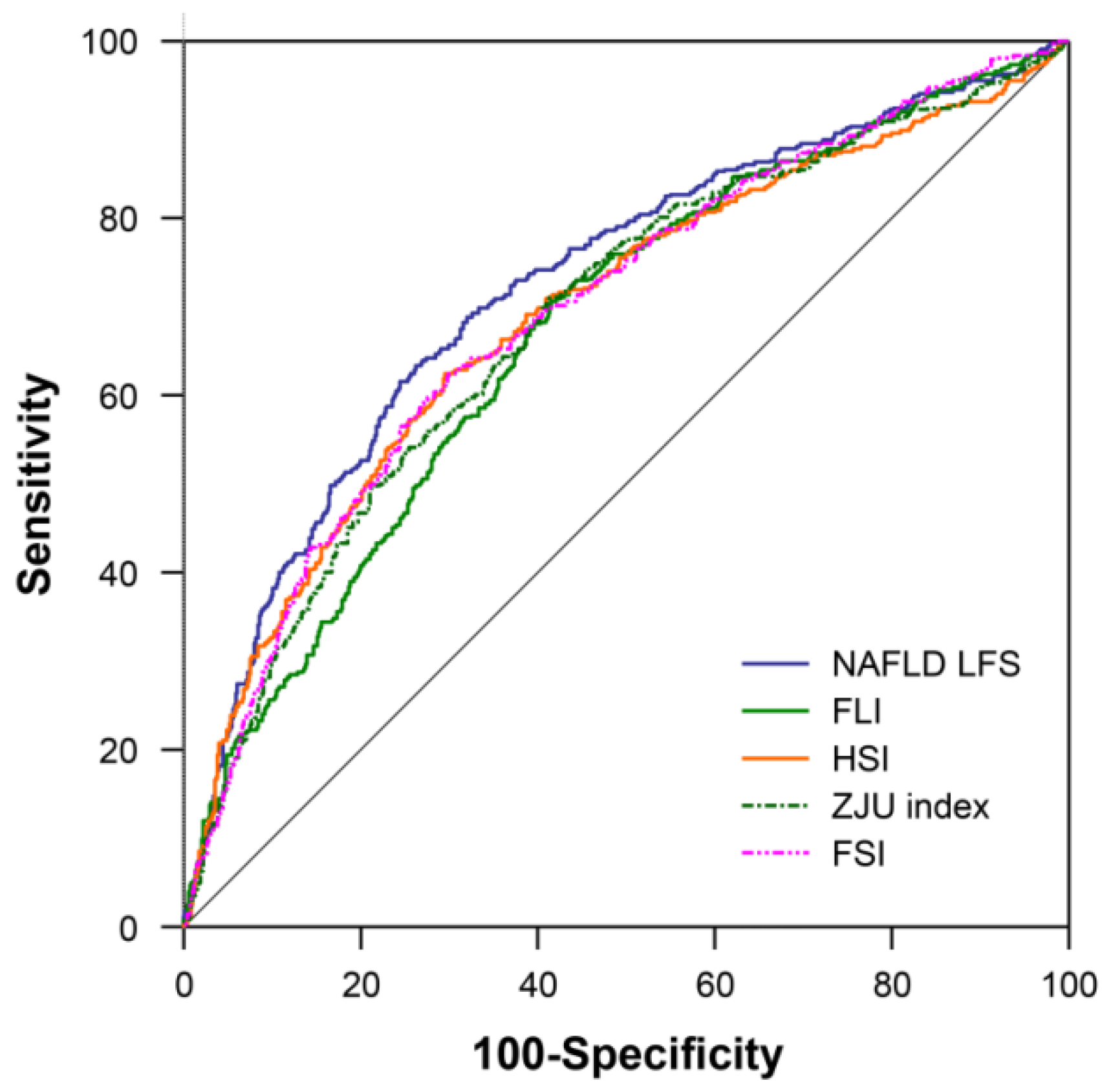
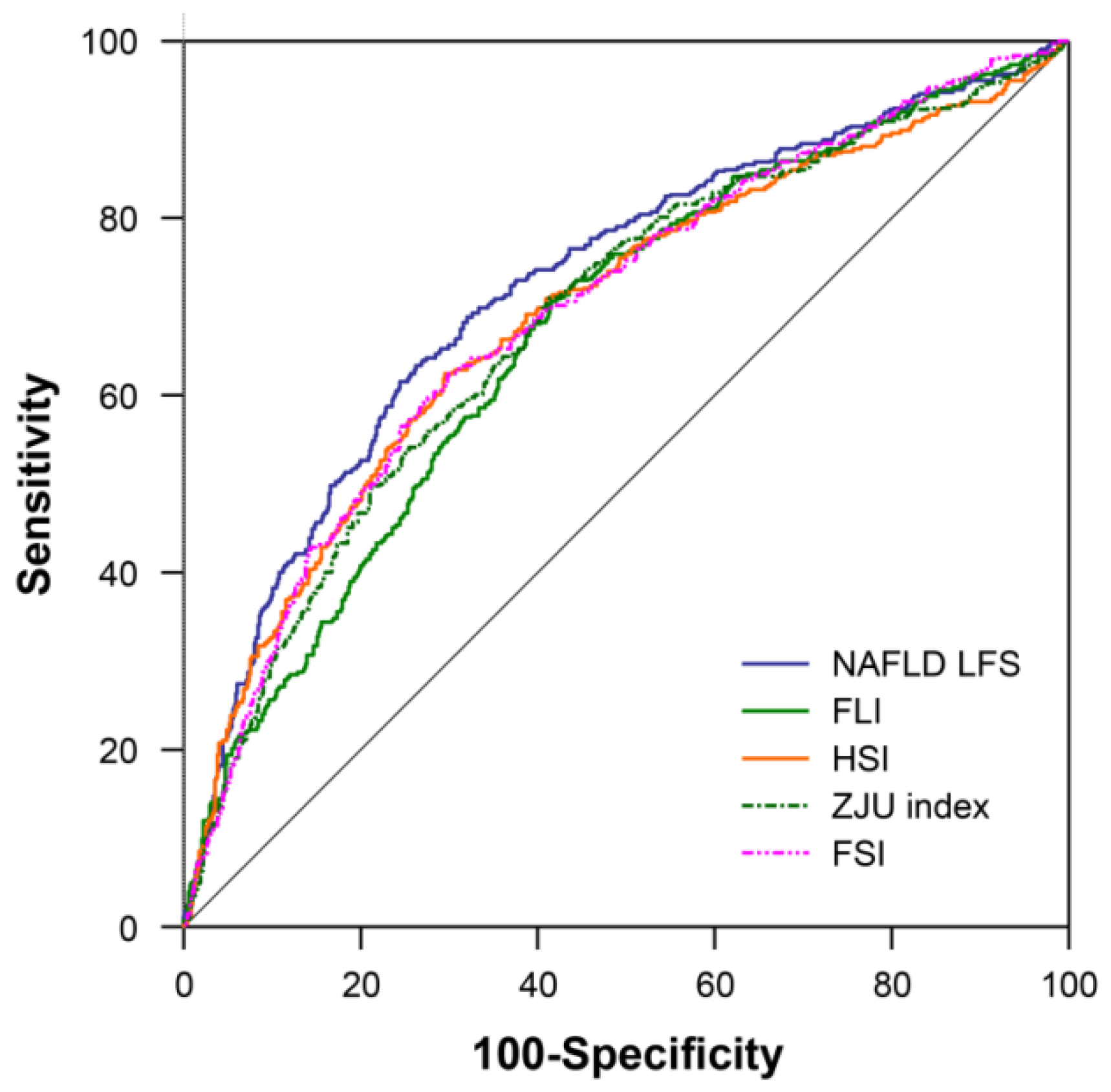
3.2. Diagnostic Performance of Estimated Hepatic Steatosis Formulae
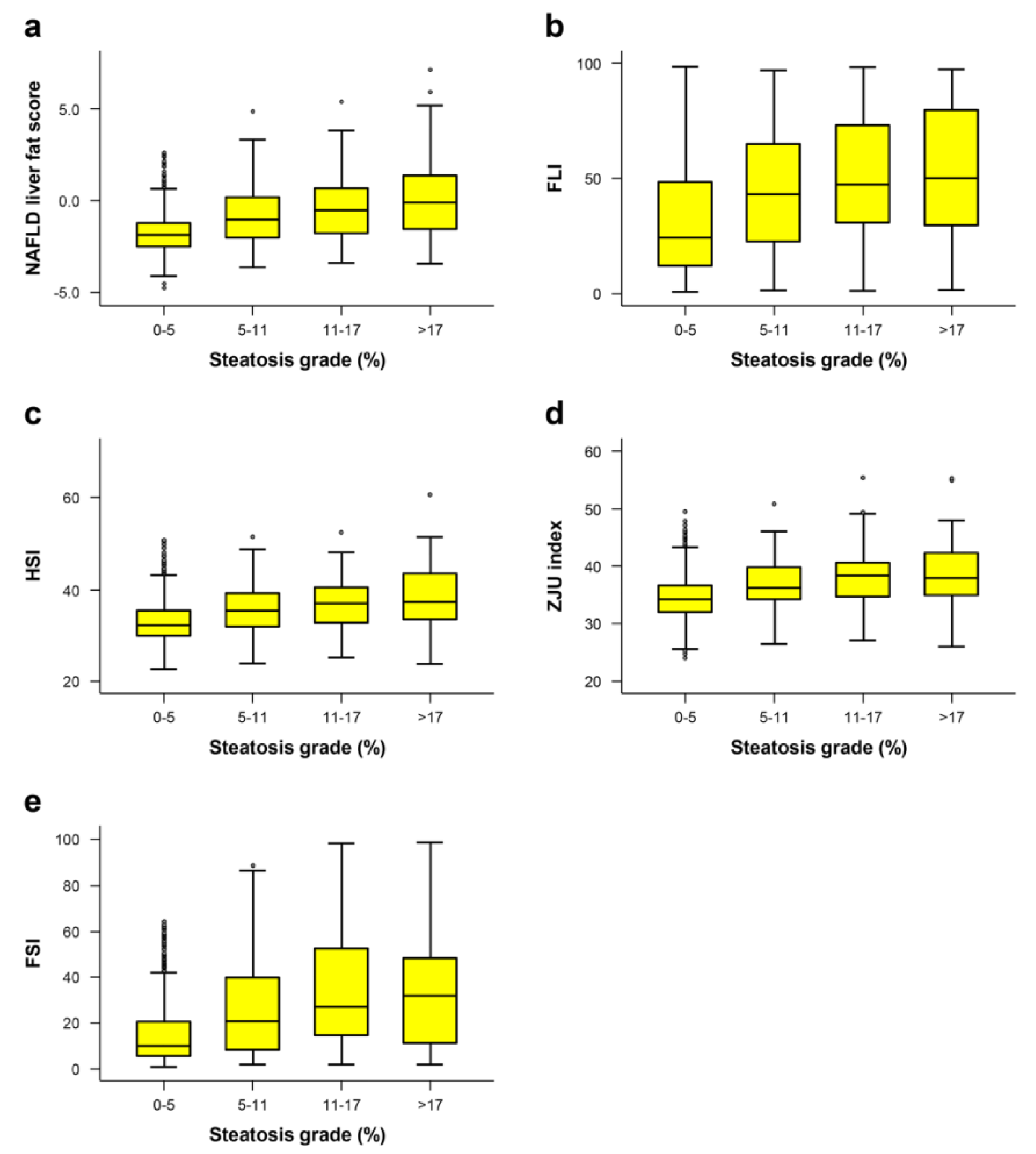
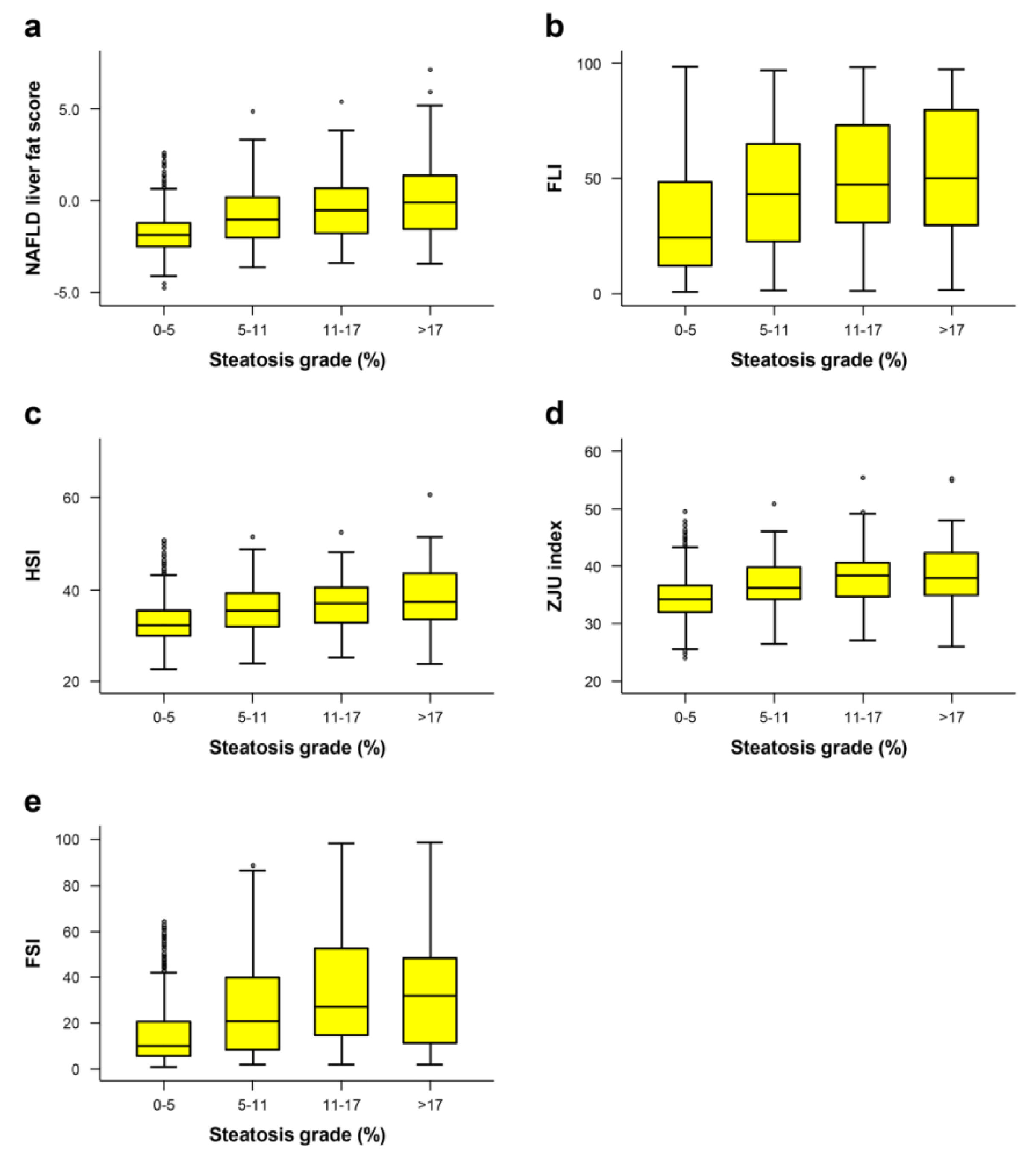
3.3. Correlation between Hepatic Steatosis Estimation Formulae and Fatty Liver Grade
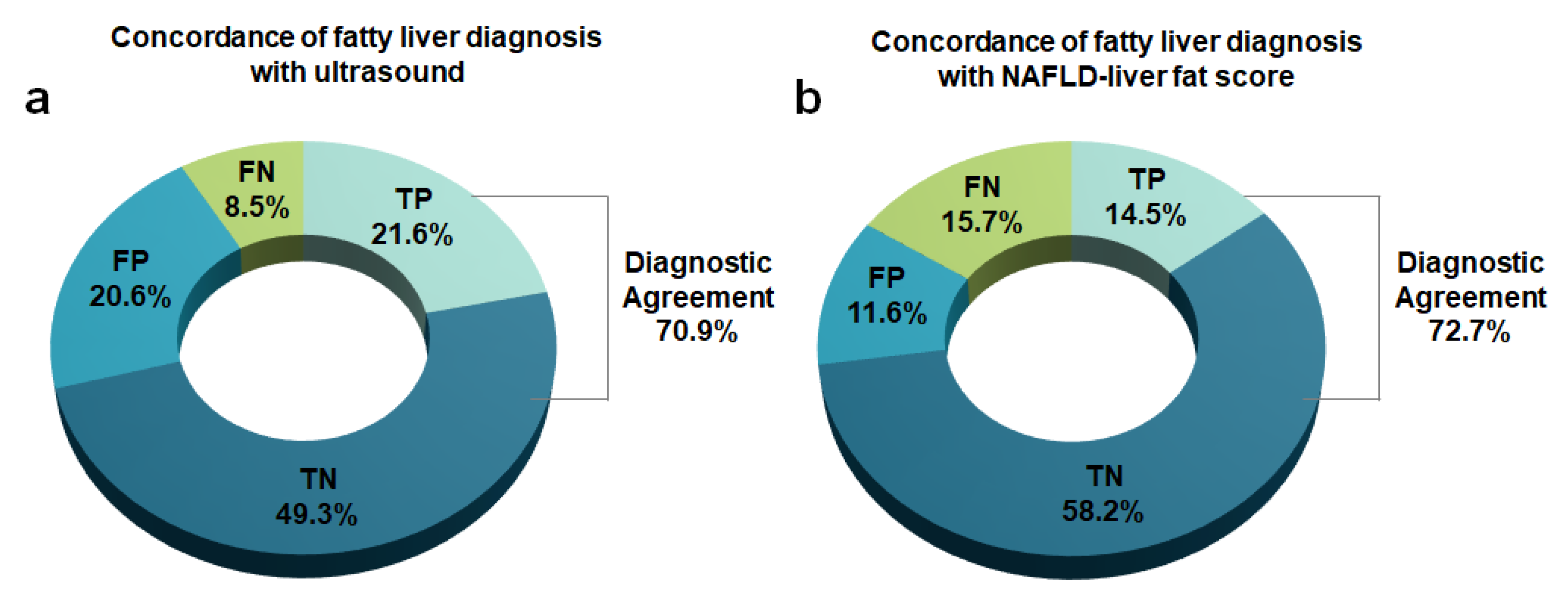
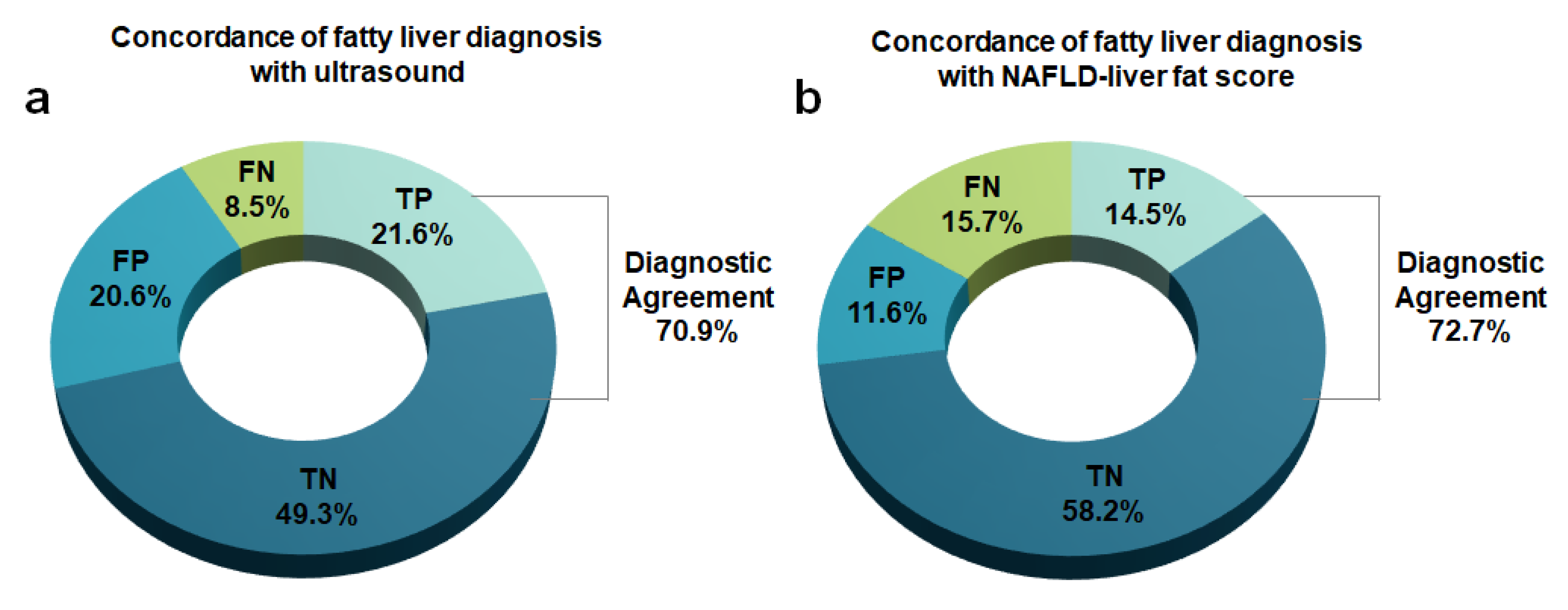
3.4. Comparison of Diagnostic Performance between NAFLD-LFS and USG
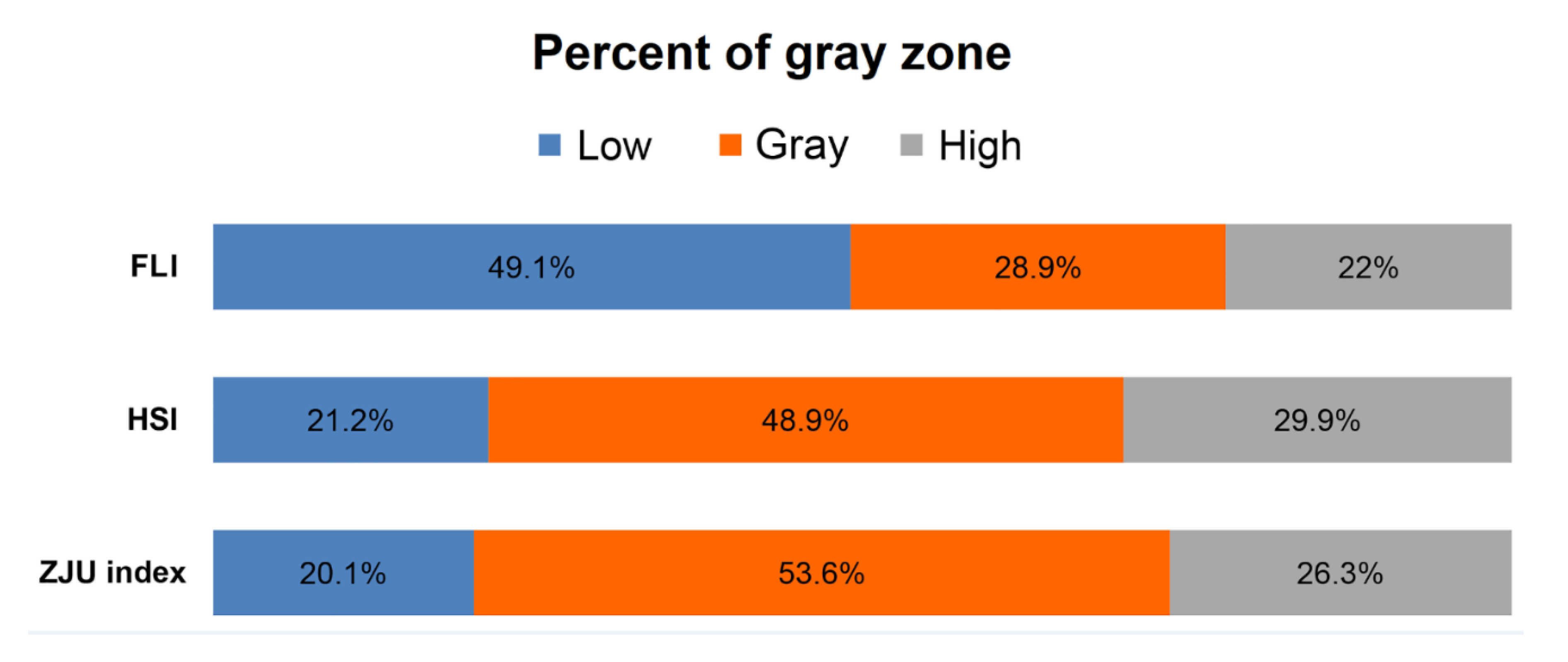
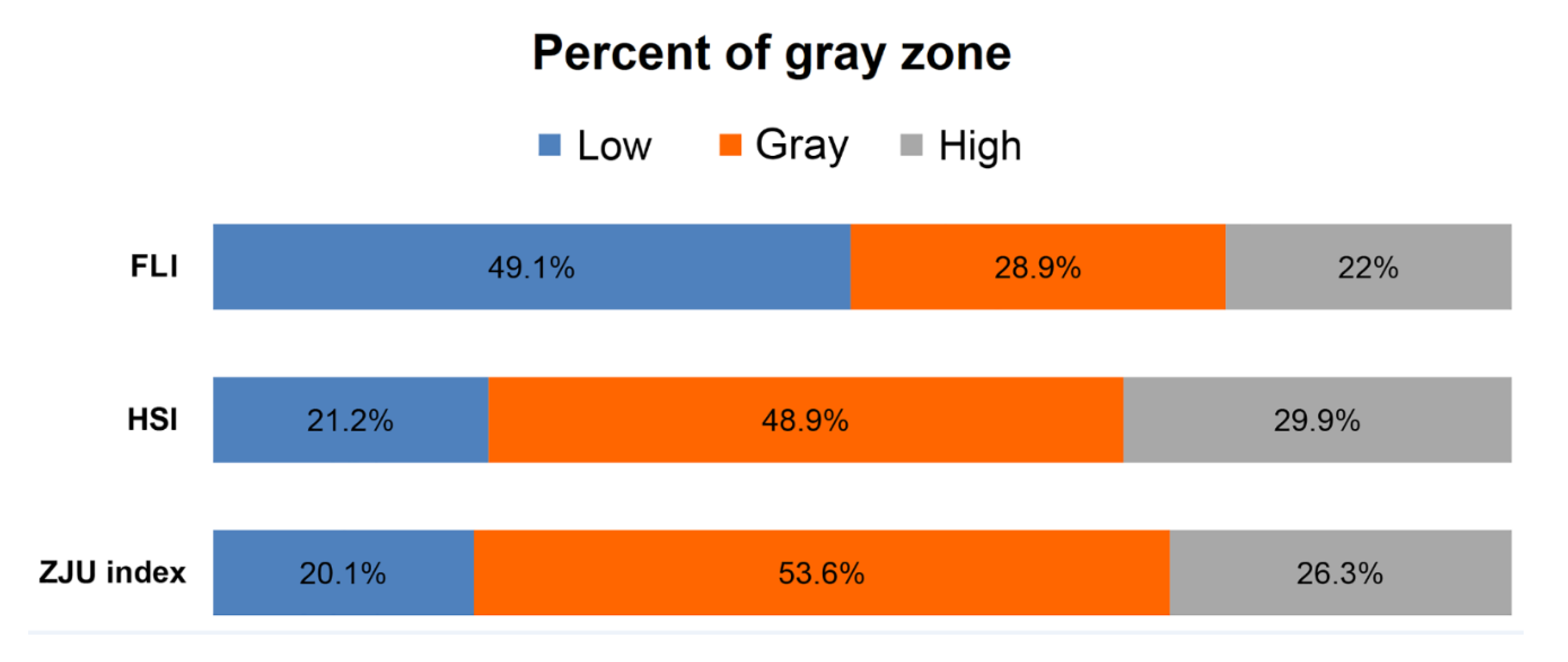
3.5. Proportion of Gray Zone of Dual Cutoff Prediction Models
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Estes, C.; Chan, H.L.Y.; Chien, R.N.; Chuang, W.L.; Fung, J.; Goh, G.B.; Hu, T.H.; Huang, J.F.; Jang, B.K.; Jun, D.W.; et al. Modelling NAFLD disease burden in four Asian regions-2019–2030. Aliment Pharm. Ther. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, X.; Xu, M.; Chen, Y.; Peng, K.; Huang, Y.; Wang, P.; Ding, L.; Lin, L.; Xu, Y.; Chen, Y.; et al. Validation of the Fatty Liver Index for Nonalcoholic Fatty Liver Disease in Middle-Aged and Elderly Chinese. Medicine 2015, 94, e1682. [Google Scholar] [CrossRef] [PubMed]
- Koehler, E.M.; Schouten, J.N.; Hansen, B.E.; Hofman, A.; Stricker, B.H.; Janssen, H.L. External validation of the fatty liver index for identifying nonalcoholic fatty liver disease in a population-based study. Clin. Gastroenterol. Hepatol. 2013, 11, 1201–1204. [Google Scholar] [CrossRef] [PubMed]
- Meffert, P.J.; Baumeister, S.E.; Lerch, M.M.; Mayerle, J.; Kratzer, W.; Volzke, H. Development, external validation, and comparative assessment of a new diagnostic score for hepatic steatosis. Am. J. Gastroenterol. 2014, 109, 1404–1414. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.N.; Yu, M.X.; Gao, Q.; Li, Y.Y.; Huang, J.J.; Sun, C.M.; Qiao, N.; Zhang, H.X.; Wang, H.; Lu, Q.; et al. External validation of non-invasive prediction models for identifying ultrasonography-diagnosed fatty liver disease in a Chinese population. Medicine 2017, 96, e7610. [Google Scholar] [CrossRef] [PubMed]
- Wong, V.W.; Adams, L.A.; de Ledinghen, V.; Wong, G.L.; Sookoian, S. Noninvasive biomarkers in NAFLD and NASH—Current progress and future promise. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 461–478. [Google Scholar] [CrossRef]
- Lee, Y.-H.; Bang, H.; Park, Y.M.; Bae, J.C.; Lee, B.-W.; Kang, E.S.; Cha, B.S.; Lee, H.C.; Balkau, B.; Lee, W.-Y. Non–Laboratory-Based Self-Assessment Screening Score for Non-Alcoholic Fatty Liver Disease: Development, Validation and Comparison with Other Scores. PLoS ONE 2014, 9, e107584. [Google Scholar] [CrossRef]
- Yang, B.-L.; Wu, W.-C.; Fang, K.-C.; Wang, Y.-C.; Huo, T.-I.; Huang, Y.-H.; Yang, H.-I.; Su, C.-W.; Lin, H.-C.; Lee, F.-Y. External validation of fatty liver index for identifying ultrasonographic fatty liver in a large-scale cross-sectional study in Taiwan. PLoS ONE 2015, 10, e0120443. [Google Scholar] [CrossRef] [Green Version]
- Ma, X.; Holalkere, N.-S.; Mino-Kenudson, M.; Hahn, P.F.; Sahani, D.V. Imaging-based quantification of hepatic fat: Methods and clinical applications. Radiographics 2009, 29, 1253–1277. [Google Scholar] [CrossRef] [Green Version]
- Reeder, S.B.; Cruite, I.; Hamilton, G.; Sirlin, C.B. Quantitative Assessment of Liver Fat with Magnetic Resonance Imaging and Spectroscopy. J. Magn. Reson. Imaging 2011, 34, 729–749. [Google Scholar] [CrossRef]
- Fedchuk, L.; Nascimbeni, F.; Pais, R.; Charlotte, F.; Housset, C.; Ratziu, V.; Group, L.S. Performance and limitations of steatosis biomarkers in patients with nonalcoholic fatty liver disease. Aliment Pharm. Ther. 2014, 40, 1209–1222. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, L.; Göbl, C.S.; Tura, A.; Chmelik, M.; Prikoszovich, T.; Kosi, L.; Wagner, O.; Roden, M.; Pacini, G.; Gastaldelli, A. Fatty liver index predicts further metabolic deteriorations in women with previous gestational diabetes. PLoS ONE 2012, 7, e32710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuthbertson, D.J.; Weickert, M.O.; Lythgoe, D.; Sprung, V.S.; Dobson, R.; Umpleby, A.; Pfeiffer, A.; Thomas, E.; Bell, J.; Jones, H. External validation of the fatty liver index and lipid accumulation product indices, using 1H-magnetic resonance spectroscopy, to identify hepatic steatosis in healthy controls and obese, insulin-resistant individuals. Eur. J. Endocrinol. 2014, 171, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Guiu, B.; Crevisy-Girod, E.; Binquet, C.; Duvillard, L.; Masson, D.; Lepage, C.; Hamza, S.; Krausé, D.; Verges, B.; Minello, A. Prediction for steatosis in type-2 diabetes: Clinico-biological markers versus 1 H-MR spectroscopy. Eur. Radiol. 2012, 22, 855–863. [Google Scholar] [CrossRef] [PubMed]
- Kahl, S.; Straßburger, K.; Nowotny, B.; Livingstone, R.; Klüppelholz, B.; Kessel, K.; Hwang, J.-H.; Giani, G.; Hoffmann, B.; Pacini, G. Comparison of liver fat indices for the diagnosis of hepatic steatosis and insulin resistance. PLoS ONE 2014, 9, e94059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ranganathan, P.; Aggarwal, R. Common pitfalls in statistical analysis: Understanding the properties of diagnostic tests—Part 1. Perspect. Clin. Res. 2018, 9, 40. [Google Scholar] [CrossRef] [PubMed]
- Kotronen, A.; Peltonen, M.; Hakkarainen, A.; Sevastianova, K.; Bergholm, R.; Johansson, L.M.; Lundbom, N.; Rissanen, A.; Ridderstrale, M.; Groop, L.; et al. Prediction of non-alcoholic fatty liver disease and liver fat using metabolic and genetic factors. Gastroenterology 2009, 137, 865–872. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kim, D.; Kim, H.J.; Lee, C.H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.H.; Cho, S.H.; Sung, M.W.; et al. Hepatic steatosis index: A simple screening tool reflecting nonalcoholic fatty liver disease. Dig. Liver Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef]
- Imajo, K.; Kessoku, T.; Honda, Y.; Tomeno, W.; Ogawa, Y.; Mawatari, H.; Fujita, K.; Yoneda, M.; Taguri, M.; Hyogo, H.; et al. Magnetic Resonance Imaging More Accurately Classifies Steatosis and Fibrosis in Patients With Nonalcoholic Fatty Liver Disease Than Transient Elastography. Gastroenterology 2016, 150, 626–637. [Google Scholar] [CrossRef] [Green Version]
- Bedogni, G.; Bellentani, S.; Miglioli, L.; Masutti, F.; Passalacqua, M.; Castiglione, A.; Tiribelli, C. The Fatty Liver Index: A simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 2006, 6, 33. [Google Scholar] [CrossRef] [Green Version]
- Palmeri, M.; Nightingale, K.; Fielding, S.; Rouze, N.; Yufeng, D.; Lynch, T.; Chen, S.; Song, P.; Urban, M.; Xie, H.; et al. RSNA QIBA ultrasound shear wave speed Phase II phantom study in viscoelastic media. In IEEE International Ultrasonics Symposium (IUS); IEEE: Piscataway, NJ, USA, 2015. [Google Scholar] [CrossRef]
- Long, M.T.; Pedley, A.; Colantonio, L.D.; Massaro, J.M.; Hoffmann, U.; Muntner, P.; Fox, C.S. Development and Validation of the Framingham Steatosis Index to Identify Persons with Hepatic Steatosis. Clin. Gastroenterol. Hepatol. 2016, 14, 1172–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Kwon, S.Y.; Lee, S.W.; Lee, C.H. Validation of fatty liver index and lipid accumulation product for predicting fatty liver in Korean population. Liver Int. 2011, 31, 1600–1601. [Google Scholar] [CrossRef] [PubMed]
- Saadeh, S.; Younossi, Z.M.; Remer, E.M.; Gramlich, T.; Ong, J.P.; Hurley, M.; Mullen, K.D.; Cooper, J.N.; Sheridan, M.J. The utility of radiological imaging in nonalcoholic fatty liver disease. Gastroenterology 2002, 123, 745–750. [Google Scholar] [CrossRef] [PubMed]
- Lijmer, J.G.; Mol, B.W.; Heisterkamp, S.; Bonsel, G.J.; Prins, M.H.; van der Meulen, J.H.; Bossuyt, P.M. Empirical evidence of design-related bias in studies of diagnostic tests. JAMA 1999, 282, 1061–1066. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Zou, B.; Yeo, Y.H.; Feng, Y.; Xie, X.; Lee, D.H.; Fujii, H.; Wu, Y.; Kam, L.Y.; Ji, F. Prevalence, incidence, and outcome of non-alcoholic fatty liver disease in Asia, 1999–2019: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2019, 4, 389–398. [Google Scholar] [CrossRef]
- Szczepaniak, L.S.; Nurenberg, P.; Leonard, D.; Browning, J.D.; Reingold, J.S.; Grundy, S.; Hobbs, H.H.; Dobbins, R.L. Magnetic resonance spectroscopy to measure hepatic triglyceride content: Prevalence of hepatic steatosis in the general population. Am. J. Physiol. Endocrinol. Metab. 2005, 288, E462–E468. [Google Scholar] [CrossRef] [Green Version]
- Brunt, E.M. Pathology of fatty liver disease. Mod. Pathol. 2007, 20, S40–S48. [Google Scholar] [CrossRef]
- Hubscher, S.G. Histological assessment of non-alcoholic fatty liver disease. Histopathology 2006, 49, 450–465. [Google Scholar] [CrossRef]
- Park, C.C.; Nguyen, P.; Hernandez, C.; Bettencourt, R.; Ramirez, K.; Fortney, L.; Hooker, J.; Sy, E.; Savides, M.T.; Alquiraish, M.H.; et al. Magnetic Resonance Elastography vs Transient Elastography in Detection of Fibrosis and Noninvasive Measurement of Steatosis in Patients With Biopsy-Proven Nonalcoholic Fatty Liver Disease. Gastroenterology 2017, 152, 598–607. [Google Scholar] [CrossRef] [Green Version]
- Tang, A.; Tan, J.; Sun, M.; Hamilton, G.; Bydder, M.; Wolfson, T.; Gamst, A.C.; Middleton, M.; Brunt, E.M.; Loomba, R.; et al. Nonalcoholic fatty liver disease: MR imaging of liver proton density fat fraction to assess hepatic steatosis. Radiology 2013, 267, 422–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total n = 1301 (100%) | No NAFLD n = 909 (69.9%) | NAFLD n = 392 (30.1%) | p-Value |
|---|---|---|---|---|
| Age (years) | 51 (46–56) | 51 (46–56) | 50 (44–56) | 0.013 |
| Males, n (%) | 1001 (76.9%) | 676 (74.4%) | 325 (82.9%) | 0.001 |
| Body mass index (kg/m2) | 24.4 (22.6–26.2) | 24 (22.3–25.6) | 25.6 (23.6–27.5) | <0.001 |
| Waist circumference (cm) | 85.3 (80.0–90.8) | 84 (79.0–89.5) | 88.6 (83.0–93.5) | <0.001 |
| Diabetes, n (%) | 170 (13.1%) | 92 (10.1%) | 78 (19.9%) | <0.001 |
| Hypertension, n (%) | 423 (32.5%) | 272 (29.9%) | 151 (38.5%) | 0.002 |
| Metabolic syndrome (%) | 321 (24.7%) | 164 (18.0%) | 157 (40.1%) | <0.001 |
| Platelet (109/L) | 237.0 (206.0–272.0) | 234.0 (204.0–268.0) | 248 (213.5–279.0) | 0.001 |
| AST (U/L) | 22.0 (19.0–28.0) | 21.0 (18.0–26.0) | 25.0 (21.0–34.0) | <0.001 |
| ALT (U/L) | 23.0 (17.0–34.0) | 21.0 (16.0–28.0) | 32.0 (22.0–47.5) | <0.001 |
| ALT/AST ratio | 1.0 (0.8–1.3) | 1.0 (0.8–1.2) | 1.2 (0.9–1.5) | <0.001 |
| GGT (U/L) | 29.0 (19.0–52.0) | 26.0 (17.0–44.0) | 39.0 (24.0–67.5) | <0.001 |
| TG (mg/dL) | 111.0 (79.0–162.0) | 102.0 (74.0–149.0) | 132.5 (92.5–199.0) | <0.001 |
| HDL-C (mg/dL) | 54.0 (45.0–65.0) | 56.0 (47.0–66.0) | 50.0 (42.0–60.0) | <0.001 |
| LDL-C (mg/dL) | 132.0 (108.0–154.0) | 130.0 (106.0–151.0) | 138.0 (111.5–160.0) | 0.001 |
| Fasting glucose (mg/dL) | 98.0 (92.0–105.0) | 97.0 (91.0–104.0) | 99.5 (93.5–110.0) | <0.001 |
| HbA1c (mmol/L) | 5.6 (5.4–5.8) | 5.6 (5.4–5.8) | 5.7 (5.5–5.9) | <0.001 |
| FLI | 30.9 (14.1–55.8) | 24.3 (12.2–48.6) | 46.2 (25.6–71.2) | <0.001 |
| HSI | 33.4 (30.5–37.1) | 32.5 (30–35.3) | 36.1 (32.6–40.4) | <0.001 |
| ZJU index | 34.9 (32.5–38.1) | 34.2 (32.2–36.7) | 37.2 (34.6–40.2) | <0.001 |
| NAFLD-LFS | −1.8 (−2.4–−0.6) | −2.0 (−2.5 – −1.2) | –0.7 (−1.9–0.5) | <0.001 |
| FSI | 12.4 (6.5–29.3) | 9.9 (5.7–20.4) | 24.6 (10–46.1) | <0.001 |
| Fatty liver on USG (%) | 549 (42.2%) | 268 (29.5%) | 281 (71.7%) | <0.001 |
| Prediction Models | FLI | HSI | ZJU Index | NAFLD-LFS | FSI | ||||
|---|---|---|---|---|---|---|---|---|---|
| AUROC (95% CI) | 0.68 (0.64–0.71) | 0.69 (0.66–0.73) | 0.69 (0.66–0.72) | 0.72 (0.69–0.75) | 0.70 (0.66–0.73) | ||||
| Cutoff value | Low | High | Low | High | Low | High | Traditional | New | |
| (30) | (60) | (30) | (36) | (32) | (38) | (−0.64) | (−1.33) | (23) | |
| Sensitivity (%) | 71.2 | 34.4 | 87.8 | 50.5 | 89.0 | 44.4 | 48.1 | 63.5 | 52.0 |
| Specificity (%) | 57.8 | 83.4 | 25.0 | 79.0 | 24.1 | 81.5 | 83.4 | 73.6 | 77.1 |
| PPV (%) | 42.1 | 47.2 | 33.5 | 50.9 | 33.6 | 50.9 | 55.7 | 51.0 | 49.5 |
| NPV (%) | 82.3 | 74.7 | 82.5 | 78.7 | 83.6 | 77.3 | 78.8 | 82.3 | 78.9 |
| Univariable | Multivariable | |||||
|---|---|---|---|---|---|---|
| Variables | OR | 95% CI | p-Value | OR | 95% CI | p-Value |
| Male (%) | 1.67 | (1.24–2.26) | 0.001 | |||
| Age (years) | 0.98 | (0.97–1.00) | 0.007 | |||
| BMI (kg/m2) | 1.18 | (1.14–1.23) | <0.001 | |||
| Waist Circumference (cm) | 1.06 | (1.04–1.07) | <0.001 | |||
| Platelet (109/L) | 1.00 | (1.00–1.01) | 0.002 | 1.00 | (1.00–1.01) | 0.009 |
| ALT/AST | 4.73 | (3.42–6.53) | <0.001 | 2.49 | (1.70–3.65) | <0.001 |
| GGT (U/L) | 1.01 | (1.00–1.01) | <0.001 | |||
| TG (mg/dL) | 1.00 | (1.00–1.00) | <0.001 | |||
| HDL-C (mg/dL) | 0.98 | (0.97–0.99) | <0.001 | |||
| HOMA-IR | 1.48 | (1.35–1.63) | <0.001 | 1.17 | (1.05–1.30) | 0.006 |
| Diabetes | 2.21 | (1.59–3.06) | <0.001 | 1.55 | (1.06–2.26) | 0.023 |
| Hypertension | 1.47 | (1.15–1.88) | 0.002 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, T.Y.; Kim, M.S.; Hong, H.P.; Kang, K.A.; Jun, D.W. Comparative Assessment and External Validation of Hepatic Steatosis Formulae in a Community-Based Setting. J. Clin. Med. 2020, 9, 2851. https://doi.org/10.3390/jcm9092851
Jung TY, Kim MS, Hong HP, Kang KA, Jun DW. Comparative Assessment and External Validation of Hepatic Steatosis Formulae in a Community-Based Setting. Journal of Clinical Medicine. 2020; 9(9):2851. https://doi.org/10.3390/jcm9092851
Chicago/Turabian StyleJung, Tae Yang, Myung Sub Kim, Hyun Pyo Hong, Kyung A Kang, and Dae Won Jun. 2020. "Comparative Assessment and External Validation of Hepatic Steatosis Formulae in a Community-Based Setting" Journal of Clinical Medicine 9, no. 9: 2851. https://doi.org/10.3390/jcm9092851
APA StyleJung, T. Y., Kim, M. S., Hong, H. P., Kang, K. A., & Jun, D. W. (2020). Comparative Assessment and External Validation of Hepatic Steatosis Formulae in a Community-Based Setting. Journal of Clinical Medicine, 9(9), 2851. https://doi.org/10.3390/jcm9092851