Infertility: Practical Clinical Issues for Routine Investigation of the Male Partner


Abstract
1. Introduction
2. When the Male Partner Should be Investigated and Goals of Evaluation
3. Initial Clinical Approach: History and Physical Examination
4. Semen Analysis: The Mainstream for Further Decision-Making Investigations
5. When and Why Second-Line Investigation is Indicated: The Role of Semen Microbiological, Endocrine, and Imaging Assessment
6. When and Why Third-Line Investigation is Indicated: The Role of Genetic Testing and Testicular Histology/Cytology
7. Indication for Additional Tests and Sperm Analyses
8. Conclusions
Author Contributions
Conflicts of Interest
References
- Tournaye, H.; Krausz, C.; Oates, R.D. Concepts in diagnosis and therapy for male reproductive impairment. Lancet Diabetes Endocrinol. 2017, 5, 554–564. [Google Scholar] [CrossRef]
- American Urological Association. Optimal Evaluation of the Infertile Male. Available online: https://www.auanet.org/education/guidelines/male-infertility-d.cfm (accessed on 1 March 2020).
- European Association of Urology. Sexual and Reproductive Health. Available online: https://uroweb.org/guideline/sexual-and-reproductive-health/ (accessed on 18 May 2020).
- National Institute for Health and Care Excellence. Fertility Problems: Assessment and Treatment. Available online: http://www.nice.org.uk/guidance/CG156 (accessed on 1 March 2020).
- Practice Committee of American Society for Reproductive Medicine. Diagnostic evaluation of the infertile male: A committee opinion. Fertil. Steril. 2015, 103, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Esteves, S.C.; Chan, P. A systematic review of recent clinical practice guidelines and best practice statements for the evaluation of the infertile male. Int. Urol. Nephrol. 2015, 47, 1441–1456. [Google Scholar] [CrossRef] [PubMed]
- Colpi, G.M.; Francavilla, S.; Haidl, G.; Link, K.; Behre, H.M.; Goulis, D.G.; Krausz, C.; Giwercman, A. European Academy of Andrology guideline Management of oligo-astheno-teratozoospermia. Andrology 2018, 6, 513–524. [Google Scholar] [CrossRef]
- Esteves, S.C. Novel concepts in male factor infertility: Clinical and laboratory perspectives. J. Assist. Reprod Genet. 2016, 33, 1319–1335. [Google Scholar] [CrossRef]
- Krausz, C. Male infertility: Pathogenesis and clinical diagnosis. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 271–285. [Google Scholar] [CrossRef]
- McLachlan, R.I.; Krausz, C. Clinical evaluation of the infertile male: New options, new challenges. Asian J. Androl. 2012, 14, 3–5. [Google Scholar] [CrossRef]
- Oates, R. Evaluation of the azoospermic male. Asian J. Androl. 2012, 14, 82–87. [Google Scholar] [CrossRef]
- Ferlin, A.; Garolla, A.; Ghezzi, M.; Selice, R.; Palego, P.; Caretta, N.; Di Mambro, A.; Valente, U.; De Rocco Ponce, M.; Dipresa, S.; et al. Sperm Count and Hypogonadism as Markers of General Male Health. Eur. Urol. Focus 2019. [Google Scholar] [CrossRef]
- Tournaye, H.; Krausz, C.; Oates, R.D. Novel concepts in the aetiology of male reproductive impairment. Lancet Diabetes Endocrinol. 2017, 5, 544–553. [Google Scholar] [CrossRef]
- Barbonetti, A.; Calogero, A.E.; Balercia, G.; Garolla, A.; Krausz, C.; La Vignera, S.; Lombardo, F.; Jannini, E.A.; Maggi, M.; Lenzi, A.; et al. The use of follicle stimulating hormone (FSH) for the treatment of the infertile man: Position statement from the Italian Society of Andrology and Sexual Medicine (SIAMS). J. Endocrinol. Invest. 2018, 41, 1107–1122. [Google Scholar] [CrossRef] [PubMed]
- Calogero, A.E.; Aversa, A.; La Vignera, S.; Corona, G.; Ferlin, A. The use of nutraceuticals in male sexual and reproductive disturbances: Position statement from the Italian Society of Andrology and Sexual Medicine (SIAMS). J. Endocrinol. Invest. 2017, 40, 1389–1397. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Laboratory Manual for the Examination and Processing of Human Semen, 5th ed.; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Calogero, A.E.; Duca, Y.; Condorelli, R.A.; La Vignera, S. Male accessory gland inflammation, infertility, and sexual dysfunctions: A practical approach to diagnosis and therapy. Andrology 2017, 5, 1064–1072. [Google Scholar] [CrossRef] [PubMed]
- Foresta, C.; Noventa, M.; De Toni, L.; Gizzo, S.; Garolla, A. HPV-DNA sperm infection and infertility: From a systematic literature review to a possible clinical management proposal. Andrology 2015, 3, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Lotti, F.; Maggi, M. Ultrasound of the male genital tract in relation to male reproductive health. Hum. Reprod. Update 2015, 21, 56–83. [Google Scholar] [CrossRef] [PubMed]
- Richenberg, J.; Belfield, J.; Ramchandani, P.; Rocher, L.; Freeman, S.; Tsili, A.C.; Cuthbert, F.; Studniarek, M.; Bertolotto, M.; Turgut, A.T.; et al. Testicular microlithiasis imaging and follow-up: Guidelines of the ESUR scrotal imaging subcommittee. Eur. Radiol. 2015, 25, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Ferlin, A.; Dipresa, S.; Delbarba, A.; Maffezzoni, F.; Porcelli, T.; Cappelli, C.; Foresta, C. Contemporary genetics-based diagnostics of male infertility. Expert Rev. Mol. Diagn. 2019, 19, 623–633. [Google Scholar] [CrossRef]
- Pizzol, D.; Ferlin, A.; Garolla, A.; Lenzi, A.; Bertoldo, A.; Foresta, C. Genetic and molecular diagnostics of male infertility in the clinical practice. Front. Biosci (Landmark Ed.) 2014, 19, 291–303. [Google Scholar] [CrossRef]
- Hotaling, J.; Carrell, D.T. Clinical genetic testing for male factor infertility: Current applications and future directions. Andrology 2014, 2, 339–350. [Google Scholar] [CrossRef]
- Foresta, C.; Ferlin, A.; Gianaroli, L.; Dallapiccola, B. Guidelines for the appropriate use of genetic tests in infertile couples. Eur. J. Hum. Genet. 2002, 10, 303–312. [Google Scholar] [CrossRef]
- Krausz, C.; Hoefsloot, L.; Simoni, M.; Tüttelmann, F.; European Academy of Andrology; European Molecular Genetics Quality Network. EAA/EMQN best practice guidelines for molecular diagnosis of Y-chromosomal microdeletions: State-Of-The-Art 2013. Andrology 2014, 2, 5–19. [Google Scholar] [CrossRef] [PubMed]
- Ferlin, A. Re: Taylor P. Kohn, Jaden R. Kohn, Ryan C. Owen, R. Matthew Coward. The Prevalence of Y-chromosome Microdeletions in Oligozoospermic Men: A Systematic Review and Meta-analysis of European and North American Studies. Eur Urol 2019;76:626–36: Indication for Y Chromosome Microdeletion Analysis in Infertile Men Should Not Be Based Merely on Sperm Concentration. Eur. Urol. 2020, 77, e96–e97. [Google Scholar] [CrossRef]
- Ferlin, A.; Stuppia, L. Diagnostics of CFTR-negative patients with congenital bilateral absence of vas deferens: Which mutations are of most interest? Expert Rev. Mol. Diagn. 2020, 20, 265–267. [Google Scholar] [CrossRef] [PubMed]
- Ferlin, A.; Foresta, C. New genetic markers for male infertility. Curr. Opin. Obstet. Gynecol. 2014, 26, 193–198. [Google Scholar] [CrossRef]
- Zuccarello, D.; Ferlin, A.; Cazzadore, C.; Pepe, A.; Garolla, A.; Moretti, A.; Cordeschi, G.; Francavilla, S.; Foresta, C. Mutations in dynein genes in patients affected by isolated non-syndromic asthenozoospermia. Hum. Reprod. 2008, 23, 1957–1962. [Google Scholar] [CrossRef]
- Foresta, C.; Zuccarello, D.; Garolla, A.; Ferlin, A. Role of hormones, genes, and environment in human cryptorchidism. Endocr. Rev. 2008, 29, 560–580. [Google Scholar] [CrossRef]
- Ferlin, A.; Zuccarello, D.; Zuccarello, B.; Chirico, M.R.; Zanon, G.F.; Foresta, C. Genetic alterations associated with cryptorchidism. JAMA 2008, 300, 2271–2276. [Google Scholar] [CrossRef]
- Ferlin, A.; Rocca, M.S.; Vinanzi, C.; Ghezzi, M.; Di Nisio, A.; Foresta, C. Mutational screening of NR5A1 gene encoding steroidogenic factor 1 in cryptorchidism and male factor infertility and functional analysis of seven undescribed mutations. Fertil. Steril. 2015, 104, 163–169. [Google Scholar] [CrossRef]
- Rocca, M.S.; Msaki, A.; Ghezzi, M.; Cosci, I.; Pilichou, K.; Celeghin, R.; Foresta, C.; Ferlin, A. Development of a novel next-generation sequencing panel for diagnosis of quantitative spermatogenic impairment. J. Assist. Reprod. Genet. 2020, 37, 753–762. [Google Scholar] [CrossRef]
- Pengo, M.; Ferlin, A.; Arredi, B.; Ganz, F.; Selice, R.; Garolla, A.; Foresta, C. FSH receptor gene polymorphisms in fertile and infertile Italian men. Reprod. Biomed. Online 2006, 13, 795–800. [Google Scholar] [CrossRef]
- Selice, R.; Garolla, A.; Pengo, M.; Caretta, N.; Ferlin, A.; Foresta, C. The response to FSH treatment in oligozoospermic men depends on FSH receptor gene polymorphisms. Int. J. Androl. 2011, 34, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Simoni, M.; Santi, D.; Negri, L.; Hoffmann, I.; Muratori, M.; Baldi, E.; Cambi, M.; Marcou, M.; Greither, T.; Baraldi, E.; et al. Treatment with human, recombinant FSH improves sperm DNA fragmentation in idiopathic infertile men depending on the FSH receptor polymorphism p.N680S: A pharmacogenetic study. Hum. Reprod. 2016, 31, 1960–1969. [Google Scholar] [CrossRef] [PubMed]
- Santi, D.; Crépieux, P.; Reiter, E.; Spaggiari, G.; Brigante, G.; Casarini, L.; Rochira, V.; Simoni, M. Follicle-stimulating Hormone (FSH) Action on Spermatogenesis: A Focus on Physiological and Therapeutic Roles. J. Clin. Med. 2020, 9, 1014. [Google Scholar] [CrossRef] [PubMed]
- Foresta, C.; Selice, R.; Ferlin, A.; Garolla, A. Recombinant FSH in the treatment of oligozoospermia. Expert Opin. Biol. Ther. 2009, 9, 659–666. [Google Scholar] [CrossRef]
- Foresta, C.; Bettella, A.; Merico, M.; Garolla, A.; Plebani, M.; Ferlin, A.; Rossato, M. FSH in the treatment of oligozoospermia. Mol. Cell Endocrinol. 2000, 161, 89–97. [Google Scholar] [CrossRef]
- Bettella, A.; Ferlin, A.; Menegazzo, M.; Ferigo, M.; Tavolini, I.M.; Bassi, P.F.; Foresta, C. Testicular fine needle aspiration as a diagnostic tool in non-obstructive azoospermia. Asian J. Androl. 2005, 7, 289–294. [Google Scholar] [CrossRef]
- Condorelli, R.A.; Calogero, A.E.; Russo, G.I.; La Vignera, S. From Spermiogram to Bio-Functional Sperm Parameters: When and Why Request Them? J. Clin. Med. 2020, 9, 406. [Google Scholar] [CrossRef]
- Ferlin, A.; Rampazzo, E.; Rocca, M.S.; Keppel, S.; Frigo, A.C.; De Rossi, A.; Foresta, C. In young men sperm telomere length is related to sperm number and parental age. Hum. Reprod. 2013, 28, 3370–3376. [Google Scholar] [CrossRef]
- Rocca, M.S.; Foresta, C.; Ferlin, A. Telomere length: Lights and shadows on their role in human reproduction. Biol. Reprod. 2019, 100, 305–317. [Google Scholar] [CrossRef]
- Ferlin, A. Sperm DNA fragmentation testing as a diagnostic and prognostic parameter of couple infertility. Transl. Androl. Urol. 2017, 6, 618–620. [Google Scholar] [CrossRef][Green Version]
- Agarwal, A.; Majzoub, A.; Esteves, S.C.; Ko, E.; Ramasamy, R.; Zini, A. Clinical utility of sperm DNA fragmentation testing: Practice recommendations based on clinical scenarios. Transl. Androl. Urol. 2016, 5, 935–950. [Google Scholar] [CrossRef] [PubMed]
- The Practice Committee of the American Society for Reproductive Medicine. The clinical utility of sperm DNA integrity testing: A guideline. Fertil. Steril. 2013, 99, 673–677. [Google Scholar] [CrossRef] [PubMed]
- Delbarba, A.; Arrighi, N.; Facondo, P.; Cappelli, C.; Ferlin, A. Positive effect of nutraceuticals on sperm DNA damage in selected infertile patients with idiopathic high sperm DNA fragmentation. Minerva Endocrinol. 2020. [Google Scholar] [CrossRef]
- Balen, A.H.; Rutherford, A.J. Management of infertility. BMJ 2007, 335, 608–611. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Major Risk Factors | Minor Risk Factors |
|---|---|
| Cryptorchidism Testicular hypotrophy Testicular cancer Known genetic factors (e.g., karyotype anomalies, cystic fibrosis, thalassemia) Varicocele Testicular trauma Reproductive tract infections Testicular torsion Iatrogenic causes (pelvic and inguinal surgery, chemotherapy, radiotherapy, medications) Systemic diseases and/or endocrine diseases (e.g., diabetes mellitus, renal diseases, hepatic disease) Anabolic steroid use Pubertal disorders Infertility with previous partners | Environmental and/or occupational exposition Aging Cigarette smoking Alcohol and substances of abuse Obesity Genital heat stress Repeated abortion Testicular microlithiasis Family history for infertility and repeated abortion |
| General data | Age |
| Religion | |
| Primary or secondary infertility | |
| Duration of infertility | |
| Fertility history with previous partners | |
| Family history | Infertility |
| Repeated abortion | |
| Fetal malformation | |
| Genetic disorders | |
| Past medical history | Known genetic factors |
| Cancers and related treatments | |
| Medications | |
| Systemic diseases | |
| Endocrine diseases | |
| Anabolic steroid use | |
| Pubertal disorders | |
| Reproductive and urinary tract diseases | Cryptorchidism |
| Testicular cancer | |
| Varicocele | |
| Testicular trauma | |
| Reproduction tract infections (orchitis, epididymitis, prostato-vesiculitis) | |
| Testicular torsion | |
| Surgery | Pelvic and abdominal surgery (prostate, bladder) |
| Inguinal surgery (orchidopexy, orchiectomy, inguinal hernia) | |
| Varicocelectomy | |
| Hydrocele | |
| Vasectomy | |
| Vasovasostomy, vasoepididymostomy | |
| Occupational and lifestyle history | Exposure to possible endocrine disruptors, heavy metals, |
| electromagnetic fields | |
| Cigarette smoking | |
| Alcohol and substances of abuse | |
| Diet (high-energy diet, fat, and fried food consumption) | |
| Genital heat stress (tight fitting underwear, sauna use) | |
| Sexual history | Timing and frequency of sexual intercourses |
| Libido | |
| Erections | |
| Ejaculation |
| General physical examination | Height, weight, body mass index, waist circumference |
| Muscle and fat distribution | |
| Genital examination | Penis (overall anatomy, curvature, plaque, urethral meatus, condylomas, glans inflammation) |
| Testes (location, volume by Prader orchidometer, consistency, nodules, hydrocele) | |
| Epididymes and vas deferens (presence, calibre, cysts, pain at palpation) | |
| Palpable varicocele, Valsalva manoeuver | |
| Secondary sex characteristics | Gynecomastia |
| Distribution of pubic hair | |
| General hair growth and distribution | |
| Body proportion | |
| Digital rectal examination | Prostate (volume, nodules, pain) |
| Parameter | Lower Reference Limit |
|---|---|
| Semen volume (mL) | 1.5 (1.4–1.7) |
| Total sperm number (million per ejaculate) | 39 (33–46) |
| Sperm concentration (million per mL) | 15 (12–16) |
| Total motility (progressive + non-progressive, %) | 40 (38–42) |
| Progressive motility (%) | 32 (31–34) |
| Vitality | 58 (55–63) |
| Sperm morphology (normal forms, %) | 4 (3.0–4.0) |
| Other reference values | |
| pH | ≥7.2 |
| Peroxidase-positive leukocytes (million per mL) | <1.0 |
| Normozoospermia | Total number (or concentration, depending on outcome reported) * of spermatozoa, and percentages of progressively motile (PR) and morphologically normal spermatozoa, equal to or above the lower reference limits |
| Quantitative alterations | |
| Azoospermia | No spermatozoa in the ejaculate (after pellet analysis after centrifugation) |
| Cryptozoospermia | Spermatozoa absent from fresh preparations but observed in a centrifuged pellet |
| Oligozoospermia | Total number (or concentration, depending on outcome reported) * of spermatozoa below the lower reference limit |
| Qualitative sperm alterations | |
| Asthenozoospermia | Percentage of progressively motile (PR) spermatozoa below the lower reference limit |
| Necrozoospermia | Low percentage of live (and high percentage of immotile) spermatozoa in the ejaculate |
| Teratozoospermia | Percentage of morphologically normal spermatozoa below the lower reference limit |
| Mixed alterations | |
| Asthenoteratozoospermia | Progressively motile (PR) and morphologically normal spermatozoa below the lower reference limits |
| Oligoasthenozoospermia | Total number (or concentration) of spermatozoa and progressively motile (PR) spermatozoa below the lower reference limits |
| Oligoasthenoteratozoospermia | Total number (or concentration) of spermatozoa, progressively motile (PR) and morphologically normal spermatozoa below the lower reference limits |
| Oligoteratozoospermia | Total number (or concentration) of spermatozoa and morphologically normal spermatozoa below the lower reference limits |
| Other | |
| Haemospermia (haematospermia) | Presence of erythrocytes in the ejaculate |
| Leukospermia (leukocytospermia, pyospermia) | Presence of leukocytes in the ejaculate above the threshold value |
| FSH | LH | Testosterone | Interpretation | Example of Aetiology |
|---|---|---|---|---|
| Normal | Normal | Normal | Post-testicular forms | Absence/obstruction of vas deferens; retrograde ejaculation |
| Mild primary testicular forms: unilateral pathologies mild bilateral pathologies | Varicocele, orchiectomy Systemic diseases, lifestyle | |||
| Qualitative sperm alterations | MAGI, antisperm antibodies | |||
| High | High | Low-normal | Primary testicular forms (spermatogenesis and Leydig cell damage) | Klinefelter syndrome, chemoradiotherapy |
| High | Normal | Normal | Primary testicular forms (only spermatogenesis is damaged) | Y chromosome microdeletions, cryptorchidism |
| Low | Low | Low | Pre-testicular (central, hypothalamic-pituitary) forms | Congenital and acquired hypogonadotropic hypogonadism |
| Low | Low | High | Pre-testicular (central, hypothalamic-pituitary) forms | Anabolic steroid use |
| High | High | High | Mixed forms | Androgen resistance (androgen receptor mutations) |
| Low | Normal | Normal | Low FSH | FSHβ gene mutations |
| Step and Goal | Methods | Interpretation |
|---|---|---|
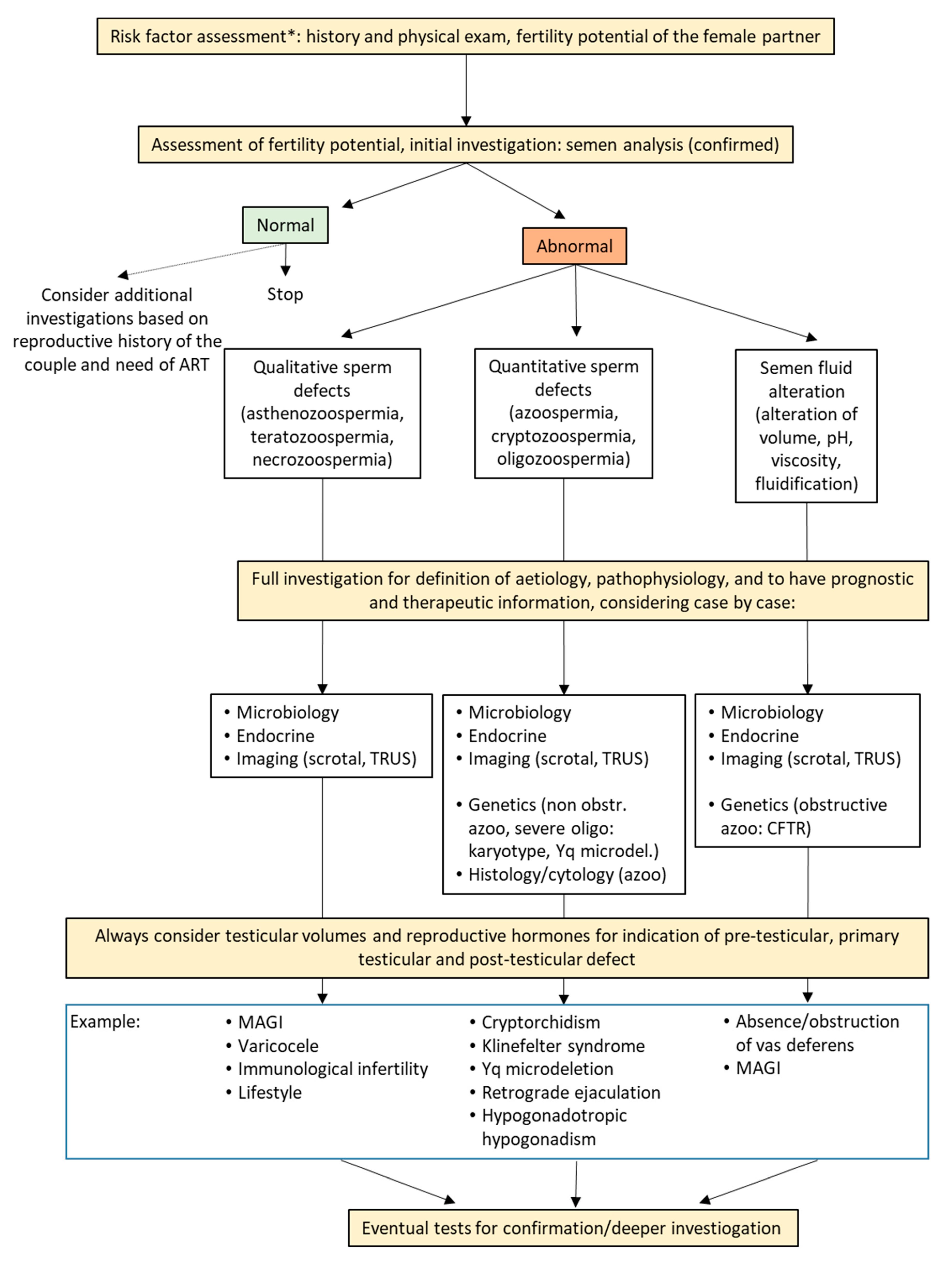
| Risk factor assessment (Table 1, Table 2 and Table 3) | History and physical examination | If risk factors are present, second and/or third-line investigation should be added to initial evaluation. |
| Fertility potential assessment, initial investigation (Table 4 and Table 5) | Fertility status of the partner | Evaluation of the couple fertility potential is essential to direct the diagnostic process of the male. |
| Semen analysis | Other than information on fertility potential, it gives evidence on the status of the entire seminal tract, therefore giving indications for further analyses other than fertility assessment. | |
| Normozoospermia is not synonymous of normal fertility, as well as alterations in semen analysis are not synonymous of infertility. | ||
| If abnormalities in semen analysis are found (quantitative or qualitative sperm defects or semen fluid alterations) indications for diagnosis, pathophysiology, and treatment could be derived only considering them together with further analyses. | ||
| No therapies should be initiated based on semen analysis alone. | ||
| Full investigation for definition of aetiology, pathophysiology and to have prognostic and therapeutic information (Table 6 and Table 7) | Semen microbiological examination Endocrine assessment Imaging | Analyses should be performed in a personalized way, based on risk factor assessment, semen analysis, and evaluation of the fertility potential of the partner. |
| Semen microbiological examination, endocrine assessment and imaging are useful in most cases of infertile men. | ||
| At minimum, semen analysis, testicular volumes, and endocrine assessment should guide on the origin of the problem (pre-testicular, testicular, post-testicular). | ||
| Testicular histology/cytology | Testicular histology/cytology should be done especially in cases of azoospermia and severe oligozoospermia. | |
| Exclusively diagnostic testicular histology is not recommended: testicular sperm cryopreservation should be done at the same time. | ||
| Genetic testing | Routine genetic testing includes karyotype and Y chromosome microdeletions in cases of non-obstructive azoospermia and severe oligozoospermia, and CFTR mutation analysis in cases of bilateral and unilateral absence of vas deferens. | |
| Other specific genetic tests should be done based on specific clinical indications, and include AR, NR5A1, TEX11, dynein genes DNAI1, DNAH5, DNAH11, DPY19L2, AURKC, INSL3, RXFP2, and genes for hypogonadotropic hypogonadism. | ||
| Polymorphism in FSHB and FSHR might have pharmacogenetic value for FSH treatment, but are not approves for routine use. | ||
| Additional tests (not yet approved for routine use) to have information in cases of unexplained infertility | Sperm DNA fragmentation | These tests, although not approved for routine investigation, could give additional information in specific conditions, such as recurrent abortion or repeated ART failure, especially when gross abnormalities on standard semen analysis are not present. |
| Sperm aneuploidies and molecular karyotype | ||
| Sperm functional tests (protamination, mitochondrial function, apoptosis) | ||
| Strict criteriafor morphological evaluation of sperm |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferlin, A.; Foresta, C. Infertility: Practical Clinical Issues for Routine Investigation of the Male Partner. J. Clin. Med. 2020, 9, 1644. https://doi.org/10.3390/jcm9061644
Ferlin A, Foresta C. Infertility: Practical Clinical Issues for Routine Investigation of the Male Partner. Journal of Clinical Medicine. 2020; 9(6):1644. https://doi.org/10.3390/jcm9061644
Chicago/Turabian StyleFerlin, Alberto, and Carlo Foresta. 2020. "Infertility: Practical Clinical Issues for Routine Investigation of the Male Partner" Journal of Clinical Medicine 9, no. 6: 1644. https://doi.org/10.3390/jcm9061644
APA StyleFerlin, A., & Foresta, C. (2020). Infertility: Practical Clinical Issues for Routine Investigation of the Male Partner. Journal of Clinical Medicine, 9(6), 1644. https://doi.org/10.3390/jcm9061644