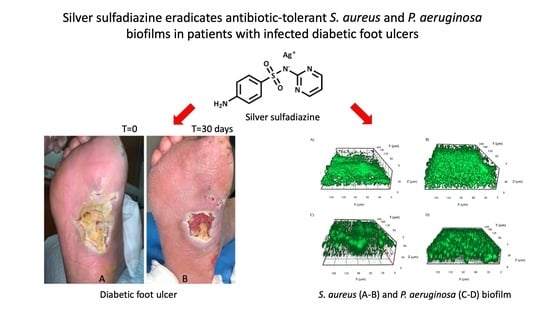
Silver Sulfadiazine Eradicates Antibiotic-Tolerant Staphylococcus aureus and Pseudomonas aeruginosa Biofilms in Patients with Infected Diabetic Foot Ulcers

 ,
,  , ,
, ,  , , , ,
, , , ,
Abstract
1. Introduction
2. Experimental Section
2.1. Ethics, Patients, and Samples
2.2. Histological Evaluation
2.3. Microbiological Assessment
2.4. Biofilm Production
2.5. Antimicrobial Susceptibility of Planktonic- and Biofilm-Grown Strains
2.6. Biofilm Imaging
2.7. Statistical Analysis
3. Results
3.1. Microscopic Evaluation
3.2. Biofilm Production
3.3. Antimicrobial Susceptibility Testing of Planktonic and Biofilm Cells
3.4. Silver Sulfadiazine Susceptibility Testing of Planktonic and Biofilm Cells
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hamdy, O.; Ashrafzadeh, S.; Mottalib, A. Weight Management in Patients with Type 2 Diabetes: A Multidisciplinary Real-world Approach. Curr. Diab. Rep. 2018, 18, 66. [Google Scholar] [CrossRef] [PubMed]
- Lipsky, B.A.; Berendt, A.R.; Cornia, P.B.; Pile, J.C.; Peters, E.J.; Armstrong, D.G.; Deery, H.G.; Embil, J.M.; Joseph, W.S.; Karchmer, A.W.; et al. 2012 Infectious Diseases Society of America clinical practice guideline for the diagnosis and treatment of diabetic foot infections. Clin. Infect Dis. 2012, 54, e132–e173. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.M.; Kim, W.H.; Lee, J.H.; Choi, M.S.S. Risk factors of treatment failure in diabetic foot ulcer patients. Arch. Plast. Surg. 2013, 40, 123–128. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Brechow, A.; Slesaczeck, T.; Münch, D.; Nanning, T.; Paetzold, H.; Schwanebeck, U.; Bornstein, S.; Weck, M. Improving major amputation rates in the multicomplex diabetic foot patient: Focus on the severity of peripheral arterial disease. Ther. Adv. Endocrinol. Metab. 2013, 4, 83–94. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.; Collier, A.; Townsend, E.M.; O’Donnell, L.E.; Abhijit, B.M.; Butcher, J.; Mackay, W.G.; Ramage, G.; Williams, C. One step closer to understanding the role of bacteria in diabetic foot ulcers: Characterizing the microbiome of ulcers. BMC Microbiol. 2016, 16, 54. [Google Scholar] [CrossRef] [PubMed]
- Sargen, M.R.; Hoffstad, O.; Margolis, D.J. Geographic variation in Medicare spending and mortality for diabetic patients with foot ulcers and amputations. J. Diabetes Complicat. 2013, 27, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Gemechu, F.W.; Seemant, F.; Curley, C.A. Diabetic foot infections. Am. Fam. Physician 2013, 88, 177–184. [Google Scholar]
- Lavery, L.A.; Armstrong, D.G.; Wunderlich, R.P.; Boulton, A.J.M.; Tredwell, J.L. Diabetic foot syndrome: Evaluating the prevalence and incidence of foot pathology in Mexican Americans and non-Hispanic whites from a diabetes disease management cohort. Diabetes Care 2003, 26, 1435–1438. [Google Scholar] [CrossRef]
- Glaudemans, A.W.; Uçkay, I.; Lipsky, B.A. Challenges in diagnosing infection in the diabetic foot. Diabet. Med. 2015, 32, 748–759. [Google Scholar] [CrossRef]
- Dowd, S.E.; Wolcott, R.D.; Sun, Y.; McKeehan, T.; Smith, E.; Rhoads, D. Polymicrobial nature of chronic diabetic foot ulcer biofilm infections determined using bacterial tag encoded FLX amplicon pyrosequencing (bTEFAP). PLoS ONE 2008, 3, e3326. [Google Scholar] [CrossRef]
- Adler, A.I.; Boyko, E.J.; Ahroni, J.H.; Smith, D.G. Lower-extremity amputation in diabetes. The independent effects of peripheral vascular disease, sensory neuropathy, and foot ulcers. Diabetes Care 1999, 22, 1029–1035. [Google Scholar] [CrossRef] [PubMed]
- Uccioli, L.; Izzo, V.; Meloni, M.; Vainieri, E.; Ruotolo, V.; Giurato, L. Non-healing foot ulcers in diabetic patients: General and local interfering conditions and management options with advanced wound dressings. J. Wound Care 2015, 24, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Barwell, N.D.; Devers, M.C.; Kennon, B.; Hopkinson, H.E.; McDougall, C.; Young, M.J.; Robertson, H.M.A.; Stang, D.; Dancer, S.J.; Seaton, A.; et al. Diabetic foot infection: Antibiotic therapy and good practice recommendations. Int. J. Clin. Pract. 2017, 71, e13006. [Google Scholar] [CrossRef] [PubMed]
- Di Domenico, E.G.; Farulla, I.; Prignano, G.; Gallo, M.T.; Vespaziani, M.; Cavallo, I.; Sperduti, I.; Pontone, M.; Bordignon, V.; Cilli, L.; et al. Biofilm is a Major Virulence Determinant in Bacterial Colonization of Chronic Skin Ulcers Independently from the Multidrug Resistant Phenotype. Int. J. Mol. Sci. 2017, 18, 1077. [Google Scholar] [CrossRef]
- Suryaletha, K.; John, J.; Radhakrishnan, M.P.; George, S.; Thomas, S. Metataxonomic approach to decipher the polymicrobial burden in diabetic foot ulcer and its biofilm mode of infection. Int. Wound J. 2018, 15, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Percival, S.L.; Hill, K.E.; Williams, D.W.; Hooper, S.J.; Thomas, D.W.; Costerton, J.W. A review of the scientific evidence for biofilms in wounds. Wound Repair Regen. 2012, 20, 647–657. [Google Scholar] [CrossRef]
- Wilson, M.; Devine, D.A. Medical Implications of Biofilms; Cambridge University Press: Cambridge, UK, 2003. [Google Scholar]
- Malone, M.; Bjarnsholt, T.; McBain, A.J.; James, G.A.; Stoodley, P.; Leaper, D.; Tachi, M.; Schultz, G.; Swanson, T.; Wolcott, R.D. The prevalence of biofilms in chronic wounds: A systematic review and meta-analysis of published data. J. Wound Care 2017, 26, 20–25. [Google Scholar] [CrossRef]
- Kwon, A.S.; Park, G.C.; Ryu, S.Y.; Lim, D.H.; Lim, D.Y.; Choi, C.H.; Park, Y.; Lim, Y. Higher biofilm formation in multidrug-resistant clinical isolates of Staphylococcus aureus. Int. J. Antimicrob. Agents 2008, 32, 68–72. [Google Scholar] [CrossRef]
- Reiter, K.C.; Da Silva Paim, T.G.; De Oliveira, C.F.; D’Azevedo, P.A. High biofilm production by invasive multiresistant staphylococci. APMIS 2011, 119, 776–781. [Google Scholar] [CrossRef]
- Sanchez, C.J., Jr.; Mende, K.; Beckius, M.L.; Akers, K.S.; Romano, D.R.; Wenke, J.C.; Murray, C.K. Biofilm formation by clinical isolates and the implications in chronic infections. BMC Infect. Dis. 2013, 13, 47. [Google Scholar] [CrossRef]
- Qi, L.; Li, H.; Zhang, C.; Liang, B.; Li, J.; Wang, L.; Du, X.; Liu, X.; Qiu, S.; Song, H. Relationship between Antibiotic Resistance, Biofilm Formation, and Biofilm-Specific Resistance in Acinetobacter baumannii. Front. Microbiol. 2016, 7, 483. [Google Scholar] [CrossRef] [PubMed]
- Katongole, P.; Nalubega, F.; Florence, N.C.; Asiimwe, B.; Andia, I. Biofilm formation, antimicrobial susceptibility and virulence genes of Uropathogenic Escherichia coli isolated from clinical isolates in Uganda. BMC Infect. Dis. 2020, 20, 453. [Google Scholar] [CrossRef] [PubMed]
- Penesyan, A.; Gillings, M.; Paulsen, I.T. Antibiotic discovery: Combatting bacterial resistance in cells and in biofilm communities. Molecules 2015, 20, 5286–5298. [Google Scholar] [CrossRef] [PubMed]
- Di Domenico, E.G.; Rimoldi, S.G.; Cavallo, I.; D’Agosto, G.; Trento, E.; Cagnoni, G.; Palazzin, A.; Pagani, C.; Romeri, F.; De Vecchi, E.; et al. Microbial biofilm correlates with an increased antibiotic tolerance and poor therapeutic outcome in infective endocarditis. BMC Microbiol. 2019, 19, 228. [Google Scholar] [CrossRef]
- Keren, I.; Kaldalu, N.; Spoering, A.; Wang, Y.; Lewis, K. Persister cells and tolerance to antimicrobials. FEMS Microbiol. Lett. 2004, 230, 13–18. [Google Scholar] [CrossRef]
- Clinton, A.; Carter, T. Chronic Wound Biofilms: Pathogenesis and Potential Therapies. Lab. Med. 2015, 46, 277–284. [Google Scholar] [CrossRef]
- Kaeberlein, T.; Lewis, K.; Epstein, S.S. Isolating “uncultivable” microorganisms in pure culture in a simulated natural environment. Science 2002, 296, 1127–1129. [Google Scholar] [CrossRef]
- Bjarnsholt, T.; Kirketerp-Møller, K.; Jensen, P.Ø.; Madsen, K.G.; Phipps, R.; Krogfelt, K.; Høiby, N.; Givskov, M. Why chronic wounds will not heal: A novel hypothesis. Wound Repair Regen. 2008, 16, 2–10. [Google Scholar] [CrossRef]
- Macià, M.D.; Rojo-Molinero, E.; Oliver, A. Antimicrobial susceptibility testing in biofilm—Growing bacteria. Clin. Microbiol. Infect. 2014, 20, 981–990. [Google Scholar] [CrossRef]
- Di Domenico, E.G.; Toma, L.; Provot, C.; Ascenzioni, F.; Sperduti, I.; Prignano, G.; Gallo, M.T.; Pimpinelli, F.; Bordignon, V.; Bernardi, T.; et al. Development of an in vitro assay, based on the Biofilm Ring Test®, for rapid profiling of biofilm—Growing bacteria. Front. Microbiol. 2016, 7, 1429. [Google Scholar] [CrossRef]
- Kennedy, P.; Brammah, S.; Wills, E. Burns, biofilm and a new appraisal of burn wound sepsis. Burns 2010, 36, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Cooper, R.A.; Bjarnsholt, T.; Alhede, M. Biofilms in wounds: A review of present knowledge. J. Wound Care 2014, 23, 570–582. [Google Scholar] [CrossRef] [PubMed]
- Rai, M.K.; Deshmukh, S.D.; Ingle, A.P.; Gade, A.K. Silver nanoparticles: The powerful nanoweapon against multidrug-resistant bacteria. J. Appl. Microbiol. 2012, 112, 841–852. [Google Scholar] [CrossRef] [PubMed]
- Paddock, H.N.; Schultz, G.S.; Perrin, K.J.U.; Moldawer, L.L.; Wright, B.; Burrell, R.E.; Mozingo, D.W. Clinical assessment of silver-coated antimicrobial dressing on MMPs and cytokine levels in non-healing wounds. Wound Rep. Reg. 2002, 10, A45. [Google Scholar]
- Ulkur, E.; Oncul, O.; Karagoz, H.; Celikoz, B.; Cavuslu, S. Comparison of silver-coated dressing (Acticoat), chlorhexidine acetate 0.5% (Bactigrass), and silver sulfadiazine 1% (Silverdin) for topical antibacterial effect in Pseudomonas aeruginosa-contaminated, full-skin thickness burn wounds in rats. J. Burn Care Rehabil. 2005, 5, 430–433. [Google Scholar]
- Chu, C.S.; McManus, A.T.; Mason, A.D.; Pruitt, B.A., Jr. Topical silver treatment after escharectomy of infected full thickness burn wounds in rats. J. Trauma 2005, 58, 1040–1046. [Google Scholar] [CrossRef]
- Atiyeh, B.S.; Costagliola, M.; Hayek, S.N.; Dibo, S.A. Effect of silver on burn wound infection control and healing: Review of the literature. Burns 2007, 33, 139–148. [Google Scholar] [CrossRef]
- Chaloupka, K.; Malam, Y.; Seifalian, A.M. Nanosilver as a new generation of nanoproduct in biomedical applications. Trends Biotechnol. 2010, 28, 580–588. [Google Scholar] [CrossRef]
- Wright, J.B.; Lam, K.; Burrell, R.E. Wound management in an era of increasing bacterial antibiotic resistance: A role for topical silver treatment. Am. J. Inf. Control 1998, 26, 572–577. [Google Scholar] [CrossRef]
- Cervantes, C.; Silver, S. Metal resistance in pseudomonas: Genes and mechanisms. In Molecular Biology of Pseudomonads; Nakazawa, T., Furukawa, K., Haas, D., Silver, S., Eds.; American Society for Microbiology: Washington, DC, USA, 1996. [Google Scholar]
- Russell, A.D.; Hugo, W.B. Antimicrobial activity and action of silver. Prog. Med. Chem. 1994, 31, 351–370. [Google Scholar]
- Marx, D.E.; Barillo, D.J. Silver in medicine: The basic science. Burns 2014, 40, S9–S18. [Google Scholar] [CrossRef] [PubMed]
- Percival, S.L.; Mayer, D.; Salisbury, A.M. Efficacy of a surfactant-based wound dressing on biofilm control. Wound Repair Regen. 2017, 25, 767–773. [Google Scholar] [CrossRef] [PubMed]
- Davis, S.C.; Li, J.; Gil, J.; Valdes, J.; Solis, M.; Higa, A.; Bowler, P. The wound-healing effects of a next-generation anti-biofilm silver Hydrofiber wound dressing on deep partial-thickness wounds using a porcine model. Int. Wound J. 2018, 15, 834–839. [Google Scholar] [CrossRef] [PubMed]
- Moyano, A.J.; Mas, C.R.; Colque, C.A.; Smania, A.M. Dealing with biofilms of Pseudomonas aeruginosa and Staphylococcus aureus: In vitro evaluation of a novel aerosol formulation of silver sulfadiazine. Burns 2020, 46, 128–135. [Google Scholar] [CrossRef]
- Lipsky, B.A.; Aragón-Sánchez, J.; Diggle, M.; Embil, J.; Kono, S.; Lavery, L.; International Working Group on the Diabetic Foot. IWGDF guidance on the diagnosis and management of foot infections in persons with diabetes. Diabetes Metab. Res. Rev. 2016, 32, 45–74. [Google Scholar] [CrossRef]
- Schultz, G.; Mozingo, D.; Romanelli, M.; Claxton, K. Wound healing and TIME; new concepts and scientific applications. Wound Repair Regen. 2005, 13, S1–S11. [Google Scholar] [CrossRef]
- European Wound Management Association (EWMA). Position Document: Wound Bed Preparation in Practice. Available online: http://woundsinternational.com (accessed on 1 March 2013).
- Wang, A.; Lv, G.; Cheng, X.; Ma, X.; Wang, W.; Gui, J.; Hu, J.; Lu, M.; Chu, G.; Chen, J.; et al. Guidelines on multidisciplinary approaches for the prevention and management of diabetic foot disease (2020 edition). Burn. Trauma 2020, 8, tkaa017. [Google Scholar] [CrossRef]
- Lucarelli, C.; Di Domenico, E.G.; Toma, L.; Bracco, D.; Prignano, G.; Fortunati, M.; Pelagalli, L.; Ensoli, F.; Pezzotti, P.; García-Fernández, A.; et al. Ralstonia mannitolilytica infections in an oncologic day ward: Description of a cluster among high-risk patients. Antimicrob. Resist. Infect. Control 2017, 6, 20. [Google Scholar] [CrossRef]
- Ceri, H.; Olson, M.E.; Stremick, C.; Read, R.R.; Morck, D.; Buret, A. The Calgary Biofilm Device: New technology for rapid determination of antibiotic susceptibilities of bacterial biofilms. J. Clin. Microbiol. 1999, 37, 1771–1776. [Google Scholar] [CrossRef]
- Peeters, E.; Nelis, H.J.; Coenye, T. Comparison of multiple methods for quantification of microbial biofilms grown in microtiter plates. J. Microbiol. Methods 2007, 72, 157–165. [Google Scholar] [CrossRef]
- Van den Driessche, F.; Rigole, P.; Brackman, G.; Coenye, T. Optimization of resazurin-based viability staining for quantification of microbial biofilms. J. Microbiol. Methods 2013, 98, 31–34. [Google Scholar] [CrossRef] [PubMed]
- Vogeleer, P.; Tremblay, Y.D.N.; Jubelin, G.; Jacques, M.; Harel, J. Biofilm-Forming Abilities of Shiga Toxin-Producing Escherichia coli Isolates Associated with Human Infections. Appl. Environ. Microbiol. 2015, 82, 1448–1458. [Google Scholar] [CrossRef] [PubMed]
- Stewart, P.S. Antimicrobial Tolerance in Biofilms. Microbiol. Spectr. 2015, 3, 269–285. [Google Scholar] [CrossRef] [PubMed]
- Di Domenico, E.G.; Petroni, G.; Mancini, D.; Geri, A.; Di Palma, L.; Ascenzioni, F. Development of Electroactive and Anaerobic Ammonium-Oxidizing (Anammox) Biofilms from Digestate in Microbial Fuel Cells. Biomed. Res. Int. 2015, 2015, 351014. [Google Scholar] [CrossRef]
- Bjarnsholt, T.; Kirketerp-Møller, K.; Kristiansen, S.; Phipps, R.; Nielsen, A.K.; Jensen, P.Ø.; Høiby, N.; Givskov, M. Silver against Pseudomonas aeruginosa biofilms. APMIS 2007, 115, 921–928. [Google Scholar] [CrossRef]
- Ramsey, S.D.; Newton, K.; Blough, D.; McCulloch, D.K.; Sandhu, N.; Reiber, G.E.; Wagner, E.H. Incidence, outcomes, and cost of foot ulcers in patients with diabetes. Diabetes Care 1999, 22, 382–387. [Google Scholar] [CrossRef]
- Maple-Brown, L.J.; Cunningham, J.; Dunne, K.; Whitbread, C.; Howard, D.; Weeramanthri, T.S.; Tatipata, S.; Dunbar, T.; Harper, C.A.; Taylor, H.R.; et al. Complications of diabetes in urban Indigenous Australians: The DRUID study. Diabetes Res. Clin. Pract. 2008, 80, 455–462. [Google Scholar] [CrossRef]
- Minges, K.E.; Zimmet, P.; Magliano, D.J.; Dunstan, D.W.; Brown, A.; Shaw, J.E. Diabetes prevalence and determinants in Indigenous Australian populations: A systematic review. Diabetes Res. Clin. Pract. 2011, 93, 139–149. [Google Scholar] [CrossRef]
- O’Dea, K.; Cunningham, J.; Maple-Brown, L.; Weeramanthri, T.; Shaw, J.; Dunbar, T.; Zimmet, P. Diabetes and cardiovascular risk factors in urban Indigenous adults: Results from the DRUID study. Diabetes Res. Clin. Pract. 2008, 80, 483–489. [Google Scholar] [CrossRef]
- Lazzarini, P.A.; Gurr, J.M.; Rogers, J.R.; Schox, A.; Bergin, S.M. Diabetes foot disease: The Cinderella of Australian diabetes management? J. Foot Ankle Res. 2012, 5, 24. [Google Scholar] [CrossRef]
- Høiby, N.; Ciofu, O.; Johansen, H.K.; Song, Z.; Moser, C.; Jensen, P.Ø.; Molin, S.; Givskov, M.; Tolker-Nielsen, T.; Bjarnsholt, T. The clinical impact of bacterial biofilms. Int. J. Oral Sci. 2011, 2, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Jensen, P.Ø.; Givskov, M.; Bjarnsholt, T.; Moser, C. The immune system vs. Pseudomonas aeruginosa biofilms. FEMS Immunol. Med. Microbiol. 2010, 59, 292–305. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, E.J.; Citron, D.M.; Warren, Y.A.; Tyrrell, K.L.; Merriam, C.V.; Fernandez, H.T. In vitro activities of dalbavancin and 12 other agents against 329 aerobic and anaerobic gram-positive isolates recovered from diabetic foot infections. Antimicrob. Agents Chemother. 2006, 50, 2875–2879. [Google Scholar] [CrossRef] [PubMed]
- Raja, N.S. Microbiology of diabetic foot infections in a teaching hospital in Malaysia: A retrospective study of 194 cases. J. Microbiol. Immunol. Infect 2007, 40, 39–44. [Google Scholar] [PubMed]
- Tascini, C.; Piaggesi, A.; Tagliaferri, E.; Iacopi, E.; Fondelli, S.; Tedeschi, A.; Rizzo, L.; Leonildi, A.; Menichetti, F. Microbiology at first visit of moderate-to-severe diabetic foot infection with antimicrobial activity and a survey of quinolone monotherapy. Diabetes Res. Clin. Pract. 2011, 94, 133–139. [Google Scholar] [CrossRef]
- Wu, M.; Pan, H.; Leng, W.; Lei, X.; Chen, L.; Liang, Z. Distribution of Microbes and Drug Susceptibility in Patients with Diabetic Foot Infections in Southwest China. J. Diabetes Res. 2018, 2018, 9817308. [Google Scholar] [CrossRef]
- Petrakis, V.; Panagopoulos, P.; Papanas, N. Dalbavancin for the Treatment of Complicated Gram-Positive Skin and Soft Tissue Infections. Int. J. Low Extrem. Wounds 2020, 19, 236–241. [Google Scholar] [CrossRef]
- Sabir, R.; Alvi, S.F.; Fawwad, A.; Basit, A. Antibiogram of Pseudomonas aeruginosa and Methicillin-resistant Staphylococcus aureus in patients with diabetes. Pak. J. Med. Sci. 2014, 30, 814–818. [Google Scholar] [CrossRef]
- Murali, T.S.; Kavitha, S.; Spoorthi, J.; Bhat, D.V.; Prasad, A.S.B.; Upton, Z.; Ramachandra, L.; Acharya, R.V.; Satyamoorthy, K. Characteristics of microbial drug resistance and its correlates in chronic diabetic foot ulcer infections. J. Med. Microbiol. 2014, 63, 1377–1385. [Google Scholar] [CrossRef]
- Jones, R.N. Resistance patterns among nosocomial pathogens: Trends over the past few years. Chest 2001, 119, 397S–404S. [Google Scholar] [CrossRef]
- Paterson, D.L.; Rossi, F.; Baquero, F.; Hsueh, P.-R.; Woods, G.L.; Satishchandran, V.; Snyder, T.A.; Harvey, C.M.; Teppler, H.; DiNubile, M.J.; et al. In vitro susceptibilities of aerobic and facultative Gram-negative bacilli isolated from patients with intraabdominal infections worldwide: The 2003 Study for Monitoring Antimicrobial Resistance Trends (SMART). J. Antimicrob. Chemother. 2005, 55, 965–973. [Google Scholar] [CrossRef] [PubMed]
- Najjad, M.K.; Idrees, Z.; Zamir, M.; Zeeshan, S.; Shah, S.A. Pseudomonas as trespassers in diabetic foot infections: More questions and fewer answers. JPMA 2014, 64, S112–S115. [Google Scholar]
- James, G.A.; Swogger, E.; Wolcott, R. Biofilms in chronic wounds. Wound Repair Regen. 2008, 16, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Wolcott, R.D.; Gontcharova, V.; Sun, Y.; Zischkau, A.M.; Dowd, S.E. Bacterial diversity in surgical site infections: Not just aerobic cocci anymore. J. Wound Care 2009, 18, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Mah, T.F. Biofilm-specific antibiotic resistance. Future Microbiol. 2012, 7, 1061–1072. [Google Scholar] [CrossRef]
- Bianchi, T.; Wolcott, R.D.; Peghetti, A.; Leaper, D.; Cutting, K.; Polignano, R.; Rosa Rita, Z.; Moscatelli, A.; Greco, A.; Romanelli, M.; et al. Recommendations for the management of biofilm: A consensus document. J. Wound Care 2016, 25, 305–317. [Google Scholar] [CrossRef]
- Schultz, G.; Bjarnsholt, T.; James, G.A.; Leaper, D.J.; McBain, A.J.; Malone, M.; Stoodley, P.; Swanson, T.; Tachi, M.; Wolcott, R.D. Global Wound Biofilm Expert Panel. Consensus guidelines for the identification and treatment of biofilms in chronic nonhealing wounds. Wound Repair Regen. 2017, 25, 744–757. [Google Scholar] [CrossRef]
- Vatan, A.; Saltoglu, N.; Yemisen, M.; Balkan, I.I.; Surme, S.; Demiray, T.; Mete, B.; Tabak, F.; Cerrahpasa Diabetic Foot Study Group. Association between biofilm and multi/extensive drug resistance in diabetic foot infection. Int. J. Clin. Pract. 2018, 72, e13060. [Google Scholar] [CrossRef]
- Girard, L.P.; Ceri, H.; Gibb, A.P.; Olson, M.; Sepandj, F. MIC versus MBEC to determine the antibiotic sensitivity of Staphylococcus aureus in peritoneal dialysis peritonitis. Perit. Dial. Int. 2010, 30, 652–656. [Google Scholar] [CrossRef]
- Castaneda, P.; McLaren, A.; Tavaziva, G.; Overstreet, D. Biofilm antimicrobial susceptibility increases with antimicrobial exposure time. Clin. Orthop. Relat. Res. 2016, 474, 1659–1664. [Google Scholar] [CrossRef]
- Di Domenico, E.G.; Cavallo, I.; Bordignon, V.; Prignano, G.; Sperduti, I.; Gurtner, A.; Trento, E.; Toma, L.; Pimpinelli, F.; Capitanio, B.; et al. Inflammatory cytokines and biofilm production sustain Staphylococcus aureus outgrowth and persistence: A pivotal interplay in the pathogenesis of Atopic Dermatitis. Sci. Rep. 2018, 8, 9573. [Google Scholar] [CrossRef] [PubMed]
- Algburi, A.; Comito, N.; Kashtanov, D.; Dicks, L.M.T.; Chikindas, M.L. Control of biofilm formation: Antibiotics and beyond. Appl. Environ. Microbiol. 2017, 83, e02508-16. [Google Scholar] [CrossRef] [PubMed]
- Price, B.L.; Morley, R.; Bowling, F.L.; Lovering, A.M.; Dobson, C.B. Susceptibility of monomicrobial or polymicrobial biofilms derived from infected diabetic foot ulcers to topical or systemic antibiotics in vitro. PLoS ONE 2020, 15, e0228704. [Google Scholar] [CrossRef] [PubMed]
- Naresh-Babu, J.; Arun-Kumar, V. Do Prophylactic Antibiotics Reach the Operative Site Adequately?: A Quantitative Analysis of Serum and Wound Concentrations of Systemic and Local Prophylactic Antibiotics in Spine Surgery. Spine 2020, 45, E196–E202. [Google Scholar] [CrossRef]
- Skhirtladze, K.; Hutschala, D.; Fleck, T.; Thalhammer, F.; Ehrlich, M.; Vukovich, T.; Müller, M.; Tschernko, E.M. Impaired target site penetration of vancomycin in diabetic patients following cardiac surgery. Antimicrob. Agents Chemother. 2006, 50, 1372–1375. [Google Scholar] [CrossRef]
- Legat, F.J.; Krause, R.; Zenahlik, P.; Hoffmann, C.; Scholz, S.; Salmhofer, W.; Tscherpel, J.; Kerl, H.; Dittrich, P.; Tscherpel, T. Penetration of piperacillin and tazobactam into inflamed soft tissue of patients with diabetic foot infection. Antimicrob. Agents Chemother. 2005, 49, 4368–4371. [Google Scholar] [CrossRef]
- Kim, S.H.; Opdahl, A.; Marmo, C.; Somorjai, G.A. AFM and SFG studies of pHEMA-based hydrogel contact lens surfaces in saline solution: Adhesion, friction, and the presence of non-crosslinked polymer chains at the surface. Biomaterials 2002, 23, 1657–1666. [Google Scholar] [CrossRef]
- Traunmüller, F.; Schintler, M.V.; Metzler, J.; Spendel, S.; Mauric, O.; Popovic, M.; Konz, K.H.; Scharnagl, E.; Joukhadar, C. Soft tissue and bone penetration abilities of daptomycin in diabetic patients with bacterial foot infections. J. Antimicrob. Chemother. 2010, 65, 1252–1257. [Google Scholar] [CrossRef]
- Hobizal, K.B.; Wukich, D.K. Diabetic foot infections: Current concept review. Diabet Foot Ankle 2012, 3, S1. [Google Scholar] [CrossRef]
- Brownrigg, J.R.W.; Apelqvist, J.; Bakker, K.; Schaper, N.C.; Hinchliffe, R.J. Evidence-based management of PAD & the diabetic foot. Eur. J. Vasc. Endovasc. Surg. 2013, 45, 673–681. [Google Scholar]
- Gullberg, E.; Cao, S.; Berg, O.G.; Ilbäck, C.; Sandegren, L.; Hughes, D.; Andersson, D.I. Selection of Resistant Bacteria at Very Low Antibiotic Concentrations. PLoS Pathog. 2011, 7, e1002158. [Google Scholar] [CrossRef] [PubMed]
- Blondeau, J.M.; Hansen, G.; Metzler, K.; Hedlin, P. The Role of PK/PD Parameters to Avoid Selection and Increase of Resistance: Mutant Prevention Concentration. J. Chemother. 2016, 16, 1–19. [Google Scholar] [CrossRef]
- Dumville, J.C.; Lipsky, B.A.; Hoey, C.; Cruciani, M.; Fiscon, M.; Xia, J. Topical antimicrobial agents for treating foot ulcers in people with diabetes. Cochrane Database Syst. Rev. 2017, 6, CD011038. [Google Scholar] [CrossRef]
- Koo, D.S.; Zhen, S.; Zhen, Z.D.; Shi, X.W.; Xiang, S.J. Assessment of topical therapy of the burn wound with silver sulphadiazine after its use for 15 years in a burn unit. Burns 1989, 15, 193–196. [Google Scholar] [PubMed]
- Marone, P.; Monzillo, V.; Perversi, L.; Carretto, E. Comparative in vitro activity of silver sulfadiazine, alone and in combination with cerium nitrate, against staphylococci and gram-negative bacteria. J. Chemother. 1998, 10, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Akiyama, H.; Yamasaki, O.; Kanzaki, H.; Tada, J.; Arata, J. Effects of sucrose and silver on Staphylococcus aureus biofilms. J. Antimicrob. Chemother. 1998, 42, 629–634. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Schuenck, R.P.; Dadalti, P.; Silva, M.G.; Fonseca, L.S.; Santos, K.R. Oxacillin- and mupirocin-resistant Staphylococcus aureus: In vitro activity of silver sulphadiazine and cerium nitrate in hospital strains. J. Chemother. 2004, 16, 453–458. [Google Scholar] [CrossRef] [PubMed]
- Lansdown, A.B.; Williams, A. How safe is silver in wound care? J Wound Care 2004, 13, 131–136. [Google Scholar] [CrossRef]
- Sun, Y.; Dowd, S.E.; Smith, E.; Rhoads, D.D.; Wolcott, R.D. In vitro multispecies Lubbock chronic wound biofilm model. Wound Repair Regen. 2008, 16, 805–813. [Google Scholar] [CrossRef]
- Loesche, M.; Gardner, S.E.; Kalan, L.; Horwinski, J.; Zheng, Q.; Hodkinson, B.P.; Tyldsley, A.S.; Franciscus, C.L.; Hillis, S.L.; Mehta, S.; et al. Temporal Stability in Chronic Wound Microbiota Is Associated With Poor Healing. J. Investig. Dermatol. 2017, 137, 237–244. [Google Scholar] [CrossRef]
- Gardiner, M.; Vicaretti, M.; Sparks, J.; Bansal, S.; Bush, S.; Liu, M.; Darling, A.; Harry, E.; Burke, C.M. A longitudinal study of the diabetic skin and wound microbiome. PeerJ 2017, 5, e3543. [Google Scholar] [CrossRef] [PubMed]
- Dalton, T.; Dowd, S.E.; Wolcott, R.D.; Sun, Y.; Watters, C.; Griswold, J.A.; Rumbaugh, K.P. An in vivo polymicrobial biofilm wound infection model to study interspecies interactions. PLoS ONE 2011, 6, e27317. [Google Scholar] [CrossRef] [PubMed]
- Howlin, R.P.; Brayford, M.J.; Webb, J.S.; Cooper, J.J.; Aiken, S.S.; Stoodley, P. Antibiotic-loaded synthetic calcium sulfate beads for prevention of bacterial colonization and biofilm formation in periprosthetic infections. Antimicrob. Agents Chemother. 2015, 59, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Mottola, C.; Mendes, J.J.; Cristino, J.M.; Cavaco-Silva, P.; Tavares, L.; Oliveira, M. Polymicrobial biofilms by diabetic foot clinical isolates. Folia Microbiol. 2016, 61, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Omar, A.; Wright, J.; Schultz, G.; Burrell, R.; Nadworny, P. Microbial Biofilms and Chronic Wounds. Microorganisms 2017, 5, 9. [Google Scholar] [CrossRef]
- Armstrong, D.G.; Liswood, P.J.; Todd, W.F. Prevalence of mixed infections in the diabetic pedal wound. A retrospective review of 112 infections. J. Am. Podiatr. Med. Assoc. 1995, 85, 533–537. [Google Scholar] [CrossRef]
- Clokie, M.; Greenway, A.L.; Harding, K.; Jones, N.J.; Vedhara, K.; Game, F.; Dhatariya, K.K. New horizons in the understanding of the causes and management of diabetic foot disease: Report from the 2017 Diabetes UK Annual Professional Conference Symposium. Diabet. Med. 2017, 34, 305–315. [Google Scholar] [CrossRef]
- Noor, S.; Zubair, M.; Ahmad, J. Diabetic foot ulcer-A review on pathophysiology, classification and microbial etiology. Diabetes Metab. Syndr. 2015, 9, 192–199. [Google Scholar] [CrossRef]
- Lipsky, B.A.; Dryden, M.; Gottrup, F.; Nathwani, D.; Seaton, R.A.; Stryja, J. Antimicrobial stewardship in wound care: A position paper from the British Society for antimicrobial chemotherapy and European wound management association. J. Antimicrob. Chemother. 2016, 71, 3026–3035. [Google Scholar] [CrossRef]
- Wolcott, R.D.; Hanson, J.D.; Rees, E.J.; Koenig, L.D.; Phillips, C.D.; Wolcott, R.A.; Cox, S.B.; White, J.S. Analysis of the chronic wound microbiota of 2,963 patients by 16S rDNA pyrosequencing. Wound Repair Regen. 2016, 24, 163174. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Description | T0 | 30 Days | p-Value |
|---|---|---|---|---|
| Tissue | Areas of necrosis | 4 (25%) | 0 (0%) | <0.001 |
| Fibrin | 12 (75%) | 2 (12.5%) | ||
| Granulation | 0 (0%) | 9 (56.3%) | ||
| Epithelialization | 0 (0%) | 5 (31.2%) | ||
| Infection | Present | 16 (100%) | 0 (0%) | <0.001 |
| Exudate | Absent | 2 (12.5%) | 8 (50%) | <0.001 |
| Low | 3 (18.7%) | 7 (43.8%) | ||
| Medium | 7 (43.8%) | 1 (6.2%) | ||
| High | 4 (25%) | 0 (0%) | ||
| Edge of wound | Hyperkeratotic | 2 (12.5%) | 0 (0%) | 0.002 |
| Excoriated | 3 (18.7%) | 0 (0%) | ||
| Maceration | 7 (43.8%) | 3 (18.7%) | ||
| Undermining | 4 (37.5%) | 0 (0%) | ||
| Integrated | 0 (0%) | 13 (81.3%) |
| Drug | AST | ABT | ||
|---|---|---|---|---|
| S. aureus | P. aeruginosa | S. aureus | P. aeruginosa | |
| Amikacin | - | 75 | - | 25 |
| Benzylpenicillin | 12.5 | - | 0 | - |
| Cefepime | - | 75 | - | 0 |
| Ceftazidime | - | 75 | - | 0 |
| Ciprofloxacin | - | 75 | - | 0 |
| Clindamycin | 75 | - | 12.5 | - |
| Colistin | - | 100 | - | 12.5 |
| Daptomycin | 100 | - | 12.5 | - |
| Erythromycin | 62.5 | - | 12.5 | - |
| Fusidic Acid | 100 | - | 25 | - |
| Gentamicin | 100 | 75 | 12.5 | 25 |
| Imipenem | - | 87.5 | - | 12.5 |
| Linezolid | 100 | - | 12.5 | - |
| Oxacillin | 87.5 | - | 25 | - |
| PIT | - | 100 | - | 0 |
| Teicoplanin | 100 | - | 25 | - |
| Tigecycline | 100 | - | 12.5 | - |
| TMP/SMX | 100 | - | 0 | - |
| Vancomycin | 100 | - | 0 | - |
| [SSD] (mg/mL) | TF (Sa/Pa) |
|---|---|
| 0.16 | 1.1 |
| 0.31 | 13.0 |
| 0.63 | 26.7 |
| 1.25 | 20.0 |
| 2.5 | 1.6 |
| 5 | 0.8 |
| 10 | 1.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Domenico, E.G.; De Angelis, B.; Cavallo, I.; Sivori, F.; Orlandi, F.; Fernandes Lopes Morais D’Autilio, M.; Di Segni, C.; Gentile, P.; Scioli, M.G.; Orlandi, A.; et al. Silver Sulfadiazine Eradicates Antibiotic-Tolerant Staphylococcus aureus and Pseudomonas aeruginosa Biofilms in Patients with Infected Diabetic Foot Ulcers. J. Clin. Med. 2020, 9, 3807. https://doi.org/10.3390/jcm9123807
Di Domenico EG, De Angelis B, Cavallo I, Sivori F, Orlandi F, Fernandes Lopes Morais D’Autilio M, Di Segni C, Gentile P, Scioli MG, Orlandi A, et al. Silver Sulfadiazine Eradicates Antibiotic-Tolerant Staphylococcus aureus and Pseudomonas aeruginosa Biofilms in Patients with Infected Diabetic Foot Ulcers. Journal of Clinical Medicine. 2020; 9(12):3807. https://doi.org/10.3390/jcm9123807
Chicago/Turabian StyleDi Domenico, Enea Gino, Barbara De Angelis, Ilaria Cavallo, Francesca Sivori, Fabrizio Orlandi, Margarida Fernandes Lopes Morais D’Autilio, Chiara Di Segni, Pietro Gentile, Maria Giovanna Scioli, Augusto Orlandi, and et al. 2020. "Silver Sulfadiazine Eradicates Antibiotic-Tolerant Staphylococcus aureus and Pseudomonas aeruginosa Biofilms in Patients with Infected Diabetic Foot Ulcers" Journal of Clinical Medicine 9, no. 12: 3807. https://doi.org/10.3390/jcm9123807
APA StyleDi Domenico, E. G., De Angelis, B., Cavallo, I., Sivori, F., Orlandi, F., Fernandes Lopes Morais D’Autilio, M., Di Segni, C., Gentile, P., Scioli, M. G., Orlandi, A., D’Agosto, G., Trento, E., Kovacs, D., Cardinali, G., Stefanile, A., Koudriavtseva, T., Prignano, G., Pimpinelli, F., Lesnoni La Parola, I., ... Ensoli, F. (2020). Silver Sulfadiazine Eradicates Antibiotic-Tolerant Staphylococcus aureus and Pseudomonas aeruginosa Biofilms in Patients with Infected Diabetic Foot Ulcers. Journal of Clinical Medicine, 9(12), 3807. https://doi.org/10.3390/jcm9123807