Health in Preconception, Pregnancy and Postpartum Global Alliance: International Network Preconception Research Priorities for the Prevention of Maternal Obesity and Related Pregnancy and Long-Term Complications

 ,
,  , , , ,
, , , ,  ,
,  and
and
Abstract
:1. Introduction
2. Method
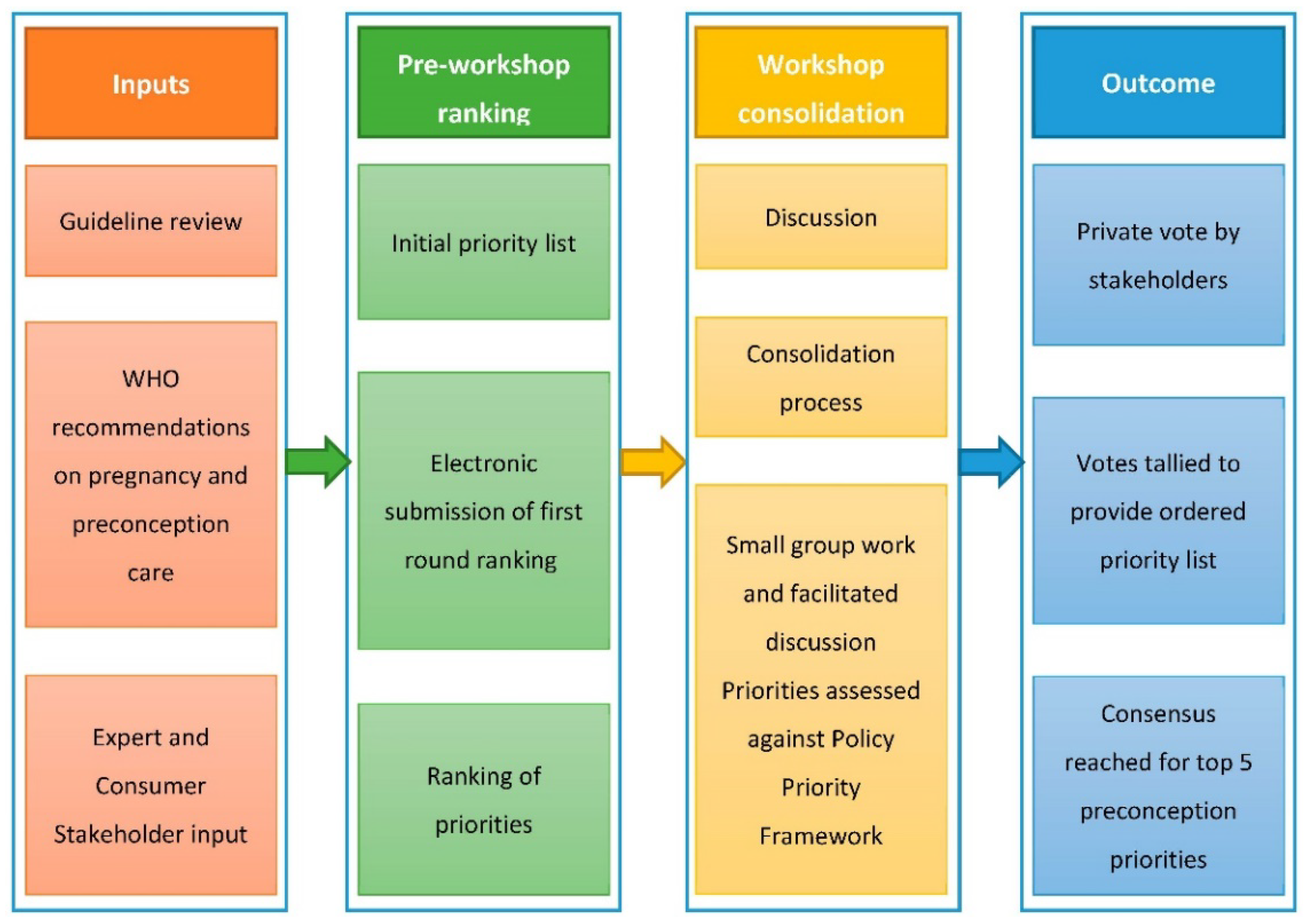
2.1. Process
2.2. Phase I. Inputs
2.2.1. Identification of Forum Participants: Experts and Consumer Representatives
2.2.2. Research Priority Areas
2.2.3. Priority Setting Framework
2.3. Phase II. Ranking
2.3.1. Round 1: Pre-Workshop Ranking
2.3.2. Rounds 2 and 3: Workshop Group Discussion and Independent Voting
2.4. Phase III. Output
2.4.1. Consensus Development of Priorities
2.4.2. Post Workshop Consultation and Collaboration
3. Results
3.1. Phase I. Inputs
3.1.1. Participants
3.1.2. Research Priority Areas
3.2. Phase II. Ranking
3.2.1. Round 1: Pre-Workshop Ranking
3.2.2. Round 2: Workshop Sense-Making, Group Discussion and Independent Voting
- Healthy diet and nutrition, including
- Folic acid supplementation
- Food security
- Weight management
- Physical activity
- Planned pregnancy including awareness and optimising fertility
- Physical, mental and psychosocial health, including
- Chronic disease including diabetes, hypertension
- Pre-existing pregnancy conditions
- Context of broader preconception/antenatal care priorities
- Social determinants of health
- Health of families
- Cultural considerations
3.2.3. Round 3: Workshop Group Discussion and Independent Voting
3.3. Phase III. Ouput
3.3.1. Consensus Development of Priorities
3.3.2. Post-Workshop Consultation and Collaboration
4. Discussion
- Establishment of Katie’s Team, a women’s health research patient and public advisory group for East London.
- Publication of a 2018 Lancet series that described the different contexts in which we can address nutrition and lifestyle preconception [4].
- Validation of the London Measure of Unplanned Pregnancy in the Australian context and cultural adaptation and validation in Brazilian Portuguese (http://www.lmup.com/).
- Development and evaluation of eHealth platforms for preconception health and care:
- ○
- The virtual conversational agent, Gabby, which screens for 100 risk factors in preconception care, and has been designed to meet the gap between the number and availability of clinicians and what is needed in preconception care in the US [37].
- ○
- A Canadian preconception health risk assessment tool intended to be used in the primary care setting to improve preconception care, adapted from Gabby (wdgpublichealth.ca/preconception-health). Both the US and Canadian programs are context specific and are undergoing evaluation.
- ○
- Development of the Dutch Preparing for Pregnancy website, which offers an internet questionnaire for risk assessment in preconception care [38].
- ○
- The mHealth ‘Smarter Pregnancy’ platform, a personal online coaching program for couples contemplating pregnancy [39].
- Publication of our first paper as an Alliance for the HiPPP Global Alliance, highlighting that we now have a clear and imperative call to action to consolidate and advance current evidence into practice and policy for the prevention of maternal obesity [34].
- Further defining the preconception population (beyond the definitions presented in Stephenson et al. [4]) and deepening our understanding of the lifestyle behaviours and mental health of women before pregnancy.
- Understanding the social determinants and disparities in perinatal health, which, for example, contribute to worse outcomes for pre-term delivery, small-for-gestational age and stillbirth [28].
- Conducting an intervention trial aiming to better understand the effect of preconception multiple micronutrient supplementation and life-skills-based education compared to the standard of care, among adolescent and young women in rural Pakistan. Outcomes will capture the health of both those who do and do not become pregnant within the context of the trial [40,41].
- Conducting an intervention to evaluate whether training health professionals on preconception health will improve delivery of preconception services in primary health care facilities in Sao Paulo, Brazil.
- In pregnancy, collaborative work of individual patient data meta-analysis and comprehensive systematic reviews of lifestyle intervention to reduce gestational weight gain have highlighted that generation of evidence needs to move from randomised controlled trials to pragmatic implementation trials sooner [42]; lessons learned in this space will be applied preconception.
- Applying our recent work developing our understanding of intervention strategies, behaviour change techniques, and implementation characteristics in lifestyle interventions for postpartum [43] women to preconception applications.
- Conducting an updated review of preconception and pregnancy guidelines for lifestyle modification in pregnancy.
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sabounchi, N.S.; Hovmand, P.S.; Osgood, N.D.; Dyck, R.F.; Jungheim, E.S. A novel system dynamics model of female obesity and fertility. Am. J. Public Health 2014, 104, 1240–1246. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, R.F.; Abell, S.K.; Ranasinha, S.; Misso, M.; Boyle, J.A.; Black, M.H.; Li, N.; Hu, G.; Corrado, F.; Rode, L.; et al. Association of gestational weight gain with maternal and infant outcomes: A systematic review and meta-analysis. J. Am. Med. Assoc. 2017, 317, 2207–2225. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, N.M.; Nicholson, W.K.; Schmitt, J. The association of pregnancy and the development of obesity—Results of a systematic review and meta-analysis on the natural history of postpartum weight retention. Int. J. Obes. 2007, 31, 1642. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, J.; Heslehurst, N.; Hall, J.; Schoenaker, D.A.J.M.; Hutchinson, J.; Cade, J.E.; Poston, L.; Barrett, G.; Crozier, S.R.; Barker, M.; et al. Before the beginning: Nutrition and lifestyle in the preconception period and its importance for future health. Lancet 2018, 391, 1830–1841. [Google Scholar] [CrossRef]
- Lindsay, A.C.; Greaney, M.L.; Wallington, S.F.; Mesa, T.; Salas, C.F. A review of early influences on physical activity and sedentary behaviors of preschool-age children in high-income countries. J. Spec. Pediatr. Nurs. 2017, 22, e12182. [Google Scholar] [CrossRef]
- Reichetzeder, C.; Dwi Putra, S.E.; Li, J.; Hocher, B. Developmental Origins of Disease—Crisis Precipitates Change. Cell. Phsiol. Biochem. 2016, 39, 919–938. [Google Scholar] [CrossRef]
- Godfrey, K.M.; Reynolds, R.M.; Prescott, S.L.; Nyirenda, M.; Jaddoe, V.W.; Eriksson, J.G.; Broekman, B.F. Influence of maternal obesity on the long-term health of offspring. Lancet Diabetes Endocrinol. 2017, 5, 53–64. [Google Scholar] [CrossRef]
- Bearak, J.; Popinchalk, A.; Alkema, L.; Sedgh, G. Global, regional, and subregional trends in unintended pregnancy and its outcomes from 1990 to 2014: Estimates from a Bayesian hierarchical model. Lancet Glob. Health 2018, 6, e380–e389. [Google Scholar] [CrossRef]
- Johnson, K.; Posner, S.F.; Biermann, J.; Cordero, J.F.; Atrash, H.K.; Parker, C.S.; Boulet, S.; Curtis, M.G. Recommendations to Improve Preconception Health and Health Care—United States; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2006.
- World Health Organization. Meeting to Develop a Global Consensus on Preconception Care to Reduce Maternal and Childhood Mortality and Morbidity; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- National Institute for Health and Care Excellence. Weight Management Before, During, and After Pregnancy (PH27); National Institute for Health and Care Excellence: London, UK, 2010. [Google Scholar]
- Public Health Agency of Canada. Family-Centred Maternity and Newborn Care: National Guidelines. Chapter 2: Preconception Care; Public Health Agency of Canada: Ottawa, ON, Canada, 2017.
- Institute of Medicine. Weight Gain during Pregnancy: Reexamining the Guidelines—Report Brief; Institute of Medicine: Washington, DC, USA, 2009. [Google Scholar]
- Hill, B.; McPhie, S.; Moran, L.J.; Harrison, P.; Huang, T.T.; Teede, H.; Skouteris, H. Lifestyle intervention to prevent obesity during pregnancy: Implications and recommendations for research and implementation. Midwifery 2017, 49, 13–18. [Google Scholar] [CrossRef]
- Skouteris, H.; Huang, T.; Millar, L.; Kuhlberg, J.; Dodd, J.; Callaway, L.; Forster, D.; Collins, C.; Hills, A.; Harrison, P.; et al. A systems approach to reducing maternal obesity: The Health in Preconception, Pregnancy and Post-Birth (HIPPP) Collaborative. Aust. N. Z. J. Obstet. Gynaecol. 2015, 55, 397–400. [Google Scholar] [CrossRef]
- Teede, H.J.; Misso, M.L.; Costello, M.F.; Dokras, A.; Laven, J.; Moran, L.; Piltonen, T.; Norman, R.J. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Fertil. Steril. 2018, 110, 364–379. [Google Scholar] [CrossRef] [PubMed]
- Hill, B.; Skouteris, H.; Boyle, J.A.; Bailey, C.; Walker, R.; Thangaratinam, S.; Sundseth, H.; Stephenson, J.; Steegers, E.; Redman, L.; et al. Health in Preconception, Pregnancy and Postpartum Global Alliance: International network pregnancy research priorities for the prevention of maternal obesity and related pregnancy and long-term complications. J. Clin. Med. submitted.
- Delbecq, A.L.; Van de Ven, A.H.; Gustafson, D.H. Group Techniques for Program Planning: A Guide to Nominal Group and Delphi Procesess; Scott-Foresman: Dallas, TX, USA, 1975. [Google Scholar]
- Rankin, N.M.; McGregor, D.; Butow, P.N.; White, K.; Phillips, J.L.; Young, J.M.; Pearson, S.A.; York, S.; Shaw, T. Adapting the nominal group technique for priority setting of evidence-practice gaps in implementation science. BMC Med. Res. Methodol. 2016, 16, 110. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Policy Brief Preconception Care: Maximizing the Gains for Maternal and Child Health; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- World Health Organization. WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience; World Health Organization: Luxembourg, 2016. [Google Scholar]
- Teede, H.; Hill, B.; Boyle, J.; Arnott, L.; Baber, R.; Byles, J.; Butera, R.; DeFazio, A.; Fourer, M.; Frayne, J.; et al. Women’s Health: Research and translation activities needed. In InSight+; Medical Journal of Australia: Australia, 2019; Available online: https://insightplus.mja.com.au/2019/21/womens-health-research-and-translation-activities-needed/ (accessed on 3 June 2019).
- Teede, H.; Johnson, A.; Buttery, J.; Jones, C.; Boyle, D.; Jennings, G.L.; Shaw, T. Australian Health Research Alliance: National priorities in data driven healthcare improvement. Med. J. Aust. 2019. [Google Scholar] [CrossRef] [PubMed]
- Wojtyła, A.; Kapka-Skrzypczak, L.; Biliński, P.; Paprzycki, P. Physical activity among women at reproductive age and during pregnancy (Youth Behavioural Polish Survey—YBPS and Pregnancy-related Assessment Monitoring Survay—PrAMS)—Epidemiological population studies in Poland during the period 2010-2011. Ann. Agric. Environ. Med. 2011, 18, 365–374. [Google Scholar]
- Legro, R.S.; Dodson, W.C.; Kunselman, A.R.; Stetter, C.M.; Kris-Etherton, P.M.; Williams, N.I.; Gnatuk, C.L.; Estes, S.J.; Allison, K.C.; Sarwer, D.B.; et al. Benefit of delayed fertility therapy with preconception weight loss over immediate therapy in obese women with PCOS. J. Clin. Endocrinol. Metab. 2016, 101, 2658–2666. [Google Scholar] [CrossRef]
- Fleming, T.P.; Watkins, A.J.; Velazquez, M.A.; Mathers, J.C.; Prentice, A.M.; Stephenson, J.; Barker, M.; Saffery, R.; Yajnik, C.S.; Eckert, J.J.; et al. Origins of lifetime health around the time of conception: Causes and consequences. Lancet 2018, 391, 1842–1852. [Google Scholar] [CrossRef]
- Holt-Lunstad, J. Why social relationships are important for physical health: A systems approach to understanding and modifying risk and protection. Annu. Rev. Psychol. 2018, 69, 437–458. [Google Scholar] [CrossRef]
- Vos, A.A.; Posthumus, A.G.; Bonsel, G.J.; Steegers, E.A.P.; Denktaş, S. Deprived neighborhoods and adverse perinatal outcome: A systematic review and meta-analysis. Acta Obstet. Gynecol. Scand. 2014, 93, 727–740. [Google Scholar] [CrossRef]
- Davies, L.; Ford-Gilboe, M.; Willson, A.; Varcoe, C.; Wuest, J.; Campbell, J.; Scott-Storey, K. Patterns of cumulative abuse among female survivors of intimate partner violence: Links to women’s health and socioeconomic status. Violence Against Women 2015, 21, 30–48. [Google Scholar] [CrossRef]
- Hanson, M.; Barker, M.; Dodd, J.M.; Kumanyika, S.; Norris, S.; Steegers, E. Interventions to prevent maternal obesity before conception, during pregnancy, and post partum. Lancet Diabetes Endocrinol. 2017, 5, 65–76. [Google Scholar] [CrossRef]
- Donetto, S.; Pierri, P.; Tsianakas, V.; Robert, G. Experience-based co-design and healthcare improvement: Realizing participatory design in the public sector. Des. J. 2015, 18, 227–248. [Google Scholar] [CrossRef]
- National Institute for Health Research (NIHR). Involve Strategy 2012–2015. Putting People First in Research; NIHR, 2012; Available online: http://www.invo.org.uk/wp-content/uploads/2012/04/INVOLVEStrategy2012-15.pdf (accessed on 26 November 2019).
- Amirav, I.; Vandall-Walker, V.; Rasiah, J.; Saunders, L. Patient and researcher engagement in health research: A parent’s perspective. Pediatrics 2017, 140, e20164127. [Google Scholar] [CrossRef] [PubMed]
- Skouteris, H.; Teede, H.; Thangaratinam, S.; Bailey, C.; Baxter, J.-A.; Bergmeier, H.; Harrison, C.; Hill, B.; Jack, B.; Jorgensen, L.; et al. Commentary: Addressing healthy lifestyle during preconception and pregnancy: Time for urgent action. Front. Endocrinol. 2019, 10, 163. [Google Scholar] [CrossRef]
- Feagin, J.; Bennefield, Z. Systemic racism and U.S. Health care. Soc. Sci. Med. 2014, 103, 7–14. [Google Scholar] [CrossRef]
- Paradies, Y.; Ben, J.; Denson, N.; Elias, A.; Priest, N.; Pieterse, A.; Gupta, A.; Kelaher, M.; Gee, G. Racism as a determinant of health: A systematic review and meta-analysis. PLoS ONE 2015, 10, e0138511. [Google Scholar] [CrossRef]
- Jack, B.; Bickmore, T.; Hempstead, M.; Yinusa-Nyahkoon, L.; Sadikova, E.; Mitchell, S.; Gardiner, P.; Adigun, F.; Penti, B.; Schulman, D.; et al. Reducing preconception risks among African American women with conversational agent technology. J. Am. Board Fam. Med. 2015, 28, 441–451. [Google Scholar] [CrossRef]
- Landkroon, A.P.; de Weerd, S.; van Vliet-Lachotzki, E.; Steegers, E.A.P. Validation of an Internet questionnaire for risk assessment in preconception care. Public Health Genom. 2010, 13, 89–94. [Google Scholar] [CrossRef]
- Van Dijk, M.R.; Huijgen, N.A.; Willemsen, S.P.; Laven, J.S.; Steegers, E.A.; Steegers-Theunissen, R.P. Impact of an mHealth platform for pregnancy on nutrition and lifestyle of the reproductive population: A Survey. JMIR mHealth uHealth 2016, 4, e53. [Google Scholar] [CrossRef]
- Baxter, J.-A.B.; Wasan, Y.; Soofi, S.B.; Suhag, Z.; Bhutta, Z.A. Effect of life skills building education and micronutrient supplements provided from preconception versus the standard of care on low birth weight births among adolescent and young Pakistani women (15–24 years): A prospective, population-based cluster-ran. Reprod. Health 2018, 15. [Google Scholar] [CrossRef]
- Baxter, J.-A.B.; Wasan, Y.; Soofi, S.B.; Suhag, Z.; Bhutta, Z.A. Feasibility and effect of life skills building education and multiple micronutrient supplements versus the standard of care on anemia among non-pregnant adolescent and young Pakistani women (15–24 years): A prospective, population-based cluster-randomized. Reprod. Health 2018, 15. [Google Scholar] [CrossRef] [PubMed]
- The International Weight Management in Pregnancy (i-WIP) Collaborative Group. Effect of diet and physical activity based interventions in pregnancy on gestational weight gain and pregnancy outcomes: Meta-analysis of individual participant data from randomised trials. Br. Med. J. 2017, 358. [Google Scholar] [CrossRef]
- Lim, S.; Liang, X.; Hill, B.; Teede, H.; Moran, L.J.; O’Reilly, S. A systematic review and meta-analysis of intervention characteristics in postpartum weight management using the TIDieR framework: A summary of evidence to implementation. Obes. Rev. 2019, 20, 1045–1056. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Criteria | Definition |
|---|---|
| Criteria 1. Prevalence or burden attributable to the proposed problem | Consider the prevalence or attributable burden of the problem and its implications/complications. Is the problem a significant issue for the community, health system and key stakeholders? |
| Criteria 2: Prevention | Is there potential to prevent the problem, including complications or secondary impacts, in the general population or in a specific vulnerable target cohort? |
| Criteria 3: Position | Consider the geographical issues around the problem and the location of services/expertise. Are there inequities that can be improved through this initiative? Is there potential to improve health outcomes for the general population and/or regional populations and/or specific vulnerable target cohorts? |
| Criteria 4: Provision | Does the current approach or system align with evidence-based best practice? Is the current approach designed to deliver the best possible community health outcomes and health care system? Is there a clear gap to address in the area proposed? |
| Criteria 5: Potential | Is there a strong rationale/evidence base for the potential for improvement in patient outcomes and health system advancement through this initiative? |
| Criteria 6: Participation | Is a collaborative approach critical to success? Are there clear drivers for stakeholders to engage and collaborate? Are there existing relationships between stakeholders that can be leveraged to drive improvement and change? |
| Criteria 7: Policy | Does the problem or the potential solution align with current policy directions at a local, state, national or international level? |
| Criteria 8: Proposed Strategy | Does the proposal align with the purpose of the Health in Preconception, Pregnancy and Postpartum strategic alliance? |
| Criteria 9: Proposed Transformation | Will addressing this problem or taking this approach collaboratively support the development of an improved health system and health outcomes? |
| Round 1 | Round 2 | Round 3 | |||
|---|---|---|---|---|---|
| Preconception Priority | Ranking | Ranking | Ranking | Mean (SD) | Median (IQR) |
Healthy diet and nutrition
| 1, 8 † | 1 | 1 | 1.6 (0.9) | 1.0 (1.0) |
| Physical activity | 3 | 2 | 2 | 2.9 (1.3) | 3.0 (1.0) |
| Weight management | 2 | 3 | 3 | 3.4 (0.9) | 4.0 (1.0) |
| Planned Pregnancy—awareness and optimising and fertility | 5, 10 † | 4 | 4 | 4.4 (2.3) | 4.5 (2.8) |
Pre-existing medical conditions *
| 4, 12 † | 5 | 5 | 4.5 (2.1) | 4.5 (3.2) |
| Substance use (including alcohol and tobacco) | 6 | 7 | 6 | 6.4 (1.4) | 6.0 (1.8) |
| Mental health * | 7 | 6 | 7 | 5.6 (1.8) | 6.5 (2.0) |
Infections
| 9, 11 † | 9 ^ | 8 | 8.6 (0.5) | 9.0 (1.0) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hill, B.; Skouteris, H.; Teede, H.J.; Bailey, C.; Baxter, J.-A.B.; Bergmeier, H.J.; Borges, A.L.V.; Harrison, C.L.; Jack, B.; Jorgensen, L.; et al. Health in Preconception, Pregnancy and Postpartum Global Alliance: International Network Preconception Research Priorities for the Prevention of Maternal Obesity and Related Pregnancy and Long-Term Complications. J. Clin. Med. 2019, 8, 2119. https://doi.org/10.3390/jcm8122119
Hill B, Skouteris H, Teede HJ, Bailey C, Baxter J-AB, Bergmeier HJ, Borges ALV, Harrison CL, Jack B, Jorgensen L, et al. Health in Preconception, Pregnancy and Postpartum Global Alliance: International Network Preconception Research Priorities for the Prevention of Maternal Obesity and Related Pregnancy and Long-Term Complications. Journal of Clinical Medicine. 2019; 8(12):2119. https://doi.org/10.3390/jcm8122119
Chicago/Turabian StyleHill, Briony, Helen Skouteris, Helena J Teede, Cate Bailey, Jo-Anna B Baxter, Heidi J Bergmeier, Ana Luiza Vilela Borges, Cheryce L Harrison, Brian Jack, Laura Jorgensen, and et al. 2019. "Health in Preconception, Pregnancy and Postpartum Global Alliance: International Network Preconception Research Priorities for the Prevention of Maternal Obesity and Related Pregnancy and Long-Term Complications" Journal of Clinical Medicine 8, no. 12: 2119. https://doi.org/10.3390/jcm8122119
APA StyleHill, B., Skouteris, H., Teede, H. J., Bailey, C., Baxter, J.-A. B., Bergmeier, H. J., Borges, A. L. V., Harrison, C. L., Jack, B., Jorgensen, L., Lim, S., Montanaro, C., Redman, L., Steegers, E., Stephenson, J., Sundseth, H., Thangaratinam, S., Walker, R., & Boyle, J. A. (2019). Health in Preconception, Pregnancy and Postpartum Global Alliance: International Network Preconception Research Priorities for the Prevention of Maternal Obesity and Related Pregnancy and Long-Term Complications. Journal of Clinical Medicine, 8(12), 2119. https://doi.org/10.3390/jcm8122119