
Proton Pump Inhibitor Use in Older Adult Patients with Multiple Chronic Conditions: Clinical Risks and Best Practices


 ,
,  , ,
, , 
Abstract
1. Introduction
2. Aging of the Gastrointestinal System
3. Material and Methods
4. Proton Pump Inhibitors (PPIs)
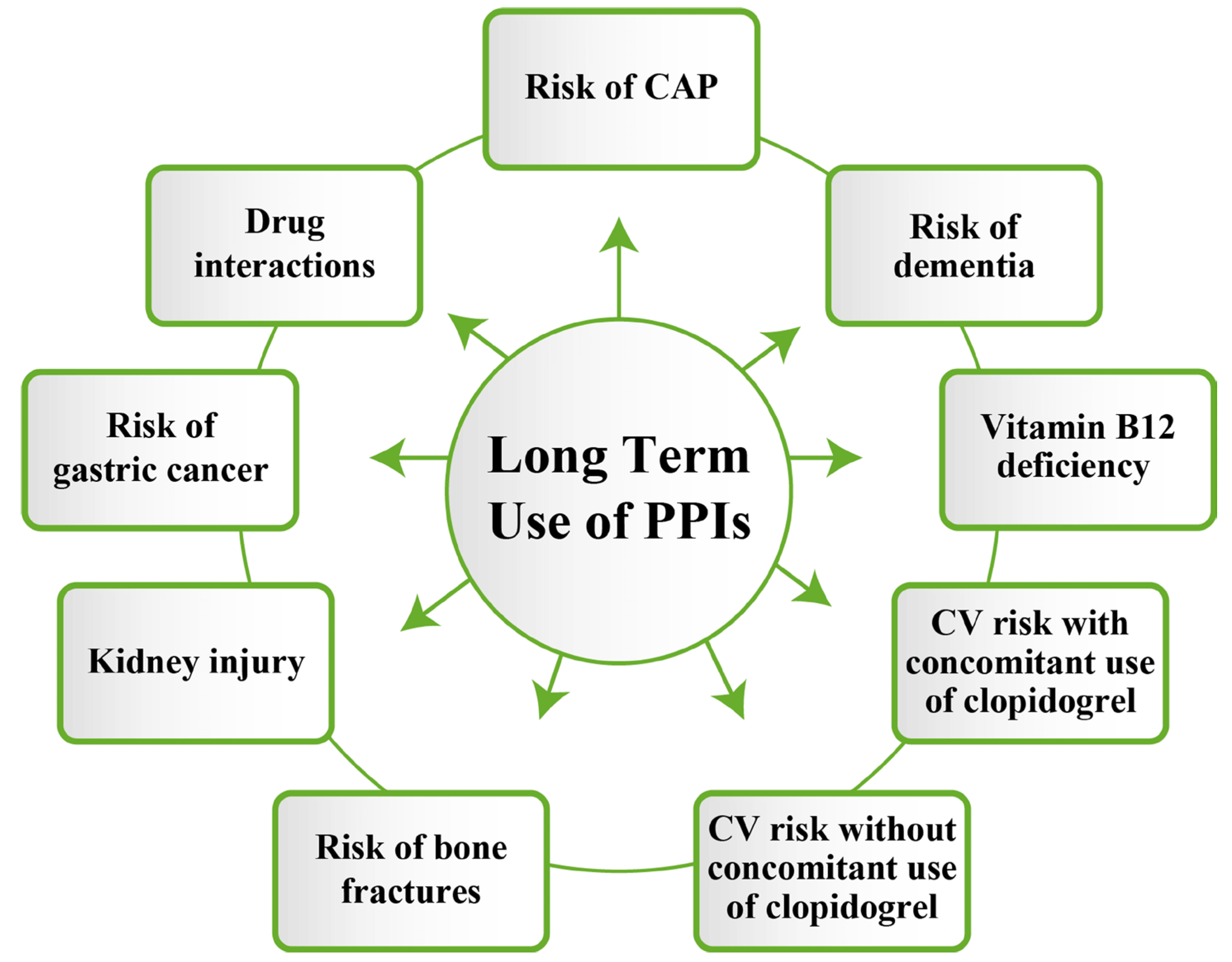
5. Adverse Effects of Proton Pump Inhibitors
5.1. Hypomagnesemia
5.2. Deficiency in Vitamin B12, Vitamin D, Vitamin C, Iron, or Calcium
5.3. Osteoporosis and Risk of Fracture
5.4. Increased Risk of Cardiovascular Complications and Death
5.5. Impairment of Renal Function
5.6. The Infectious Risk of Overuse of PPIs
5.7. PPI and the Risk of SARS-COV-2 Infection [46]
5.8. The Role of PPIs on the Intestinal Microbiota
5.9. The Risk of Cancer
5.10. The Risk of Dementia and Neurocognitive Disorders
6. Proton Pump Inhibitors and Drug Interactions
7. Proton Pump Inhibitors Treatment Approach for Older Adults Patients with Comorbidities
8. Strengths and Limitations
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Alexa, I.D.; Ilie, A.C.; Pislaru, A.I.; Stefaniu, R.; Sandu, I.A. Note de Curs Geriatrie Gerontologie; Popa, G.T., Ed.; UMF Iasi: Iasi, Romania, 2021. [Google Scholar]
- Donca, V.; Avram, L. Esential in Geriatrie; Casa Cartii de Stiinta: Cluj-Napoca, Romania, 2024. [Google Scholar]
- Wang, X.; Liu, K.; Shirai, K.; Tang, C.; Hu, Y.; Wang, Y.; Hao, Y.; Dong, J.Y. Prevalence and trends of polypharmacy in U.S. adults, 1999–2018. Glob. Health Res. Policy 2023, 8, 25. [Google Scholar] [CrossRef]
- Bonanno, E.G.; Figueiredo, T.; Mimoso, I.F.; Morgado, M.I.; Carrilho, J.; Midão, L.; Costa, E. Polypharmacy Prevalence Among Older Adults Based on the Survey of Health, Ageing and Retirement in Europe: An Update. J. Clin. Med. 2025, 14, 1330. [Google Scholar] [CrossRef]
- Donca, V. Abordarea Terapeutica a Pacientului Geriatric; Casa Cartii de Stiinta: Cluj-Napoca, Romania, 2022. [Google Scholar]
- Haruma, K.; Kamada, T.; Kawaguchi, H.; Okamoto, S.; Yoshihara, M.; Sumii, K.; Inoue, M.; Kishimoto, S.; Kajiyama, G.; Miyoshi, A. Effect of age and Helicobacter pylori infection on gastric acid secretion. J. Gastroenterol. Hepatol. 2000, 15, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Salles, N. Basic Mechanisms of the Aging Gastrointestinal Tract. Dig. Dis. 2007, 25, 112–117. [Google Scholar] [CrossRef]
- Spiru, L.; Romosan, I. Aeternus-Tratat de Geriatrie si Medicina Longevitatii; Academiei Romane: Bucharest, Romania, 2020. [Google Scholar]
- Jungo, K.T.; Mantelli, S.; Rozsnyai, Z.; Missiou, A.; Kitanovska, B.G.; Weltermann, B.; Mallen, C.; Collins, C.; Bonfim, D.; Kurpas, D.; et al. General practitioners’ deprescribing decisions in older adults with polypharmacy: A case vignette study in 31 countries. BMC Geriatr. 2021, 21, 19. [Google Scholar] [CrossRef] [PubMed]
- Maideen, N.M.P. Adverse Effects Associated with Long-Term Use of Proton Pump Inhibitors. Chonnam Med. J. 2023, 59, 115–127. [Google Scholar] [CrossRef] [PubMed]
- Savarino, V.; Dulbecco, P.; de Bortoli, N.; Ottonello, A.; Savarino, E. The appropriate use of proton pump inhibitors (PPIs): Need for a reappraisal. Eur. J. Intern. Med. 2017, 37, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.-Y. Initiatives for a Healthy Stomach. Curr. Treat. Options Gastroenterol. 2019, 17, 628–635. [Google Scholar] [CrossRef]
- Whitaker, M. Proton pump inhibitors in the elderly population. Eur. J. Gastroenterol. Hepatol. 2002, 14 (Suppl. 1), S5–S9. [Google Scholar] [PubMed]
- Shin, J.S.; Lee, J.Y.; Cho, K.H.; Park, H.L.; Kukulka, M.; Wu, J.T.; Kim, D.Y.; Park, S.H. The pharmacokinetics, pharmacodynamics and safety of oral doses of ilaprazole 10, 20 and 40 mg and esomeprazole 40 mg in healthy subjects: A randomised, open-label crossover study. Aliment. Pharmacol. Ther. 2014, 40, 548–561. [Google Scholar] [CrossRef]
- Shanika, L.G.T.; Reynolds, A.; Pattison, S.; Braund, R. Proton pump inhibitor use: Systematic review of global trends and practices. Eur. J. Clin. Pharmacol. 2023, 79, 1159–1172. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Clarke, J.O. Proton Pump Inhibitors (PPI); StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Shin, J.M.; Munson, K.; Vagin, O.; Sachs, G. The gastric HK-ATPase: Structure, function, and inhibition. Pflug. Arch. 2009, 457, 609–622. [Google Scholar] [CrossRef] [PubMed]
- Lahner, E.; Marzinotto, I.; Lampasona, V.; Dottori, L.; Bazzigaluppi, E.; Brigatti, C.; Secchi, M.; Piemonti, L.; Conti, L.; Pilozzi, E.; et al. Autoantibodies Toward ATP4A and ATP4B Subunits of Gastric Proton Pump H+,K+-ATPase Are Reliable Serological Pre-endoscopic Markers of Corpus Atrophic Gastritis. Clin. Transl. Gastroenterol. 2020, 11, e00240. [Google Scholar] [CrossRef] [PubMed]
- Chaudhry, A.S.; Kochhar, R.; Kohli, K.K. Genetic polymorphism of CYP2C19 & therapeutic response to proton pump inhibitors. Indian. J. Med. Res. 2008, 127, 521–530. [Google Scholar]
- Gronich, N.; Lavi, I.; Lejbkowicz, F.; Pinchev, M.; Rennert, G. Association of CYP2C19 Polymorphism With Proton Pump Inhibitors Effectiveness and With Fractures in Real-Life: Retrospective Cohort Study. Clin. Pharmacol. Ther. 2022, 111, 1084–1092. [Google Scholar] [CrossRef]
- Maes, M.L.; Fixen, D.R.; Linnebur, S.A. Adverse effects of proton-pump inhibitor use in older adults: A review of the evidence. Ther. Adv. Drug Saf. 2017, 8, 273–297. [Google Scholar] [CrossRef]
- Kanno, T.; Moayyedi, P. Proton Pump Inhibitors in the Elderly, Balancing Risk and Benefit: An Age-Old Problem. Curr. Gastroenterol. Rep. 2019, 21, 65. [Google Scholar] [CrossRef]
- Freedberg, D.E.; Kim, L.S.; Yang, Y.X. The Risks and Benefits of Long-term Use of Proton Pump Inhibitors: Expert Review and Best Practice Advice From the American Gastroenterological Association. Gastroenterology 2017, 152, 706–715. [Google Scholar] [CrossRef]
- Xia, B.; He, Q.; Smith, F.G.; Gkoutos, V.G.; Nirantharakumar, K.; Kuo, Z.C.; Wang, D.; Feng, Q.; Cheung, E.C.; Dai, L.; et al. Individualized prevention of proton pump inhibitor related adverse events by risk stratification. Nat. Commun. 2024, 15, 3591. [Google Scholar] [CrossRef]
- Rodrigues, D.A.; Herdeiro, M.T.; Mateos-Campos, R.; Figueiras, A.; Roque, F. Magnitude and Determinants of Long-term Use of Proton Pump Inhibitors Among Portuguese Older Adults in Primary Health Care. Clin. Ther. 2024, 46, e54–e58. [Google Scholar] [CrossRef] [PubMed]
- George, C.J.; Korc, B.; Ross, J.S. Appropriate proton pump inhibitor use among older adults: A retrospective chart review. Am. J. Geriatr. Pharmacother. 2008, 6, 249–254. [Google Scholar] [CrossRef]
- Dixon, R.; Bolt, J. Appropriateness of proton pump inhibitor therapy in an ambulatory geriatrics clinic: A retrospective cross-sectional analysis. Can. Pharm. J. 2023, 156, 331–336. [Google Scholar] [CrossRef]
- Voukelatou, P.; Vrettos, I.; Emmanouilidou, G.; Dodos, K.; Skotsimara, G.; Kontogeorgou, D.; Kalliakmanis, A. Predictors of Inappropriate Proton Pump Inhibitors Use in Elderly Patients. Curr. Gerontol. Geriatr. Res. 2019, 2019, 7591045. [Google Scholar] [CrossRef] [PubMed]
- Gommers, L.M.M.; Hoenderop, J.G.J.; de Baaij, J.H.F. Mechanisms of proton pump inhibitor-induced hypomagnesemia. Acta Physiol. 2022, 235, e13846. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, M.; Fernando, H.; Mohammed, H.H.; Vithanage, N. Proton Pump Inhibitor Induced Hypomagnesemia Causing Seizures: A Rare Adverse Effect of a Commonly Used Medication. Cureus 2024, 16, e64044. [Google Scholar] [CrossRef]
- Srinutta, T.; Chewcharat, A.; Takkavatakarn, K.; Praditpornsilpa, K.; Eiam-Ong, S.; Jaber, B.L.; Susantitaphong, P. Proton pump inhibitors and hypomagnesemia: A meta-analysis of observational studies. Medicine 2019, 98, e17788. [Google Scholar] [CrossRef] [PubMed]
- Mumtaz, H.; Ghafoor, B.; Saghir, H.; Tariq, M.; Dahar, K.; Ali, S.H.; Waheed, S.T.; Syed, A.A. Association of Vitamin B12 deficiency with long-term PPIs use: A cohort study. Ann. Med. Surg. 2022, 82, 104762. [Google Scholar] [CrossRef]
- Brisebois, S.; Merati, A.; Giliberto, J.P. Proton pump inhibitors: Review of reported risks and controversies. Laryngoscope Investig. Otolaryngol. 2018, 3, 457–462. [Google Scholar] [CrossRef] [PubMed]
- Zirk-Sadowski, J.; Masoli, J.A.; Strain, W.D.; Delgado, J.; Henley, W.; Hamilton, W.; Melzer, D.; Ble, A. Proton-Pump Inhibitors and Fragility Fractures in Vulnerable Older Patients. Am. J. Gastroenterol. 2017, 112, 520–523. [Google Scholar] [CrossRef]
- Geng, T.; Chen, J.X.; Zhou, Y.F.; Lu, Q.; Wan, Z.; Liu, L.; Pan, A.; Liu, G. Proton Pump Inhibitor Use and Risks of Cardiovascular Disease and Mortality in Patients With Type 2 Diabetes. J. Clin. Endocrinol. Metab. 2023, 108, e216–e222. [Google Scholar] [CrossRef]
- Foresta, A.; Fernandez, L.O.; Torrigiani, G.; Schena, S.; Roncaglioni, M.C.; Nobili, A.; Tettamanti, M.; Franchi, C.; Fortino, I.; Succurro, E.; et al. Proton Pump Inhibitor Use and the Risk of Cardiovascular Complications and Death in Older Adults with Diabetes: A Population-Based Cohort Study. Drugs Aging 2024, 41, 239–249. [Google Scholar] [CrossRef]
- Bell, E.J.; Bielinski, S.J.; St Sauver, J.L.; Chen, L.Y.; Rooney, M.R.; Larson, N.B.; Takahashi, P.Y.; Folsom, A.R. Association of Proton Pump Inhibitors With Higher Risk of Cardiovascular Disease and Heart Failure. Mayo Clin. Proc. 2021, 96, 2540–2549. [Google Scholar] [CrossRef] [PubMed]
- Song, H.J.; Seo, H.-J.; Jiang, X.; Jeon, N.; Lee, Y.J.; Ha, I.-H. Proton pump inhibitors associated with an increased risk of mortality in elderly: A systematic review and meta-analysis. Eur. J. Clin. Pharmacol. 2024, 80, 367–382. [Google Scholar] [CrossRef] [PubMed]
- Fan, W.; Liu, H.; Shen, Y.; Hong, K. The Association of Proton Pump Inhibitors and QT Interval Prolongation in Critically Ill Patients. Cardiovasc. Drugs Ther. 2024, 38, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Xie, Y.; Al-Aly, Z. The association of proton pump inhibitors and chronic kidney disease: Cause or confounding? Curr. Opin. Nephrol. Hypertens. 2018, 27, 182–187. [Google Scholar] [CrossRef]
- Parmar, M.P.; Kaleem, S.; Samuganathan, P.; Ishfaq, L.; Anne, T.; Patel, Y.; Bollu, S.; Vempati, R. Impact of Proton Pump Inhibitors on Kidney Function and Chronic Kidney Disease Progression: A Systematic Review. Cureus 2023, 15, e49883. [Google Scholar] [CrossRef]
- Wu, C.C.; Liao, M.H.; Kung, W.M.; Wang, Y.C. Proton Pump Inhibitors and Risk of Chronic Kidney Disease: Evidence from Observational Studies. J. Clin. Med. 2023, 12, 2262. [Google Scholar] [CrossRef]
- Ben-Eltriki, M.; Chhabra, M.; Cassels, A.; Wright, J.M. Inappropriate Use of Proton Pump Inhibitor Among Elderly Patients in British Columbia: What are the Long-term Adverse Events? Curr. Drug Saf. 2024, 19, 244–247. [Google Scholar] [CrossRef]
- Maret-Ouda, J.; Panula, J.; Santoni, G.; Xie, S.; Lagergren, J. Proton pump inhibitor use and risk of pneumonia: A self-controlled case series study. J. Gastroenterol. 2023, 58, 734–740. [Google Scholar] [CrossRef]
- Trifan, A.; Stanciu, C.; Girleanu, I.; Stoica, O.C.; Singeap, A.M.; Maxim, R.; Chiriac, S.A.; Ciobica, A.; Boiculese, L. Proton pump inhibitors therapy and risk of Clostridium difficile infection: Systematic review and meta-analysis. World J. Gastroenterol. 2017, 23, 6500–6515. [Google Scholar] [CrossRef]
- Lee, S.W.; Ha, E.K.; Yeniova, A.; Moon, S.Y.; Kim, S.Y.; Koh, H.Y.; Yang, J.M.; Jeong, S.J.; Moon, S.J.; Cho, J.Y.; et al. Severe clinical outcomes of COVID-19 associated with proton pump inhibitors: A nationwide cohort study with propensity score matching. Gut 2021, 70, 76–84. [Google Scholar] [CrossRef]
- Fatima, K.; Almas, T.; Lakhani, S.; Jahangir, A.; Ahmed, A.; Siddiqui, A.; Rahim, A.; Qureshi, S.; Arshad, Z.; Golani, S.; et al. The Use of Proton Pump Inhibitors and COVID-19: A Systematic Review and Meta-Analysis. Trop. Med. Infect. Dis. 2022, 7, 37. [Google Scholar] [CrossRef] [PubMed]
- Charpiat, B.; Bleyzac, N.; Tod, M. Proton Pump Inhibitors are Risk Factors for Viral Infections: Even for COVID-19? Clin. Drug Investig. 2020, 40, 897–899. [Google Scholar] [CrossRef]
- Tsuda, A.; Suda, W.; Morita, H.; Takanashi, K.; Takagi, A.; Koga, Y.; Hattori, M. Influence of Proton-Pump Inhibitors on the Luminal Microbiota in the Gastrointestinal Tract. Clin. Transl. Gastroenterol. 2015, 6, e89. [Google Scholar] [CrossRef]
- Takagi, T.; Naito, Y.; Inoue, R.; Kashiwagi, S.; Uchiyama, K.; Mizushima, K.; Tsuchiya, S.; Okayama, T.; Dohi, O.; Yoshida, N.; et al. The influence of long-term use of proton pump inhibitors on the gut microbiota: An age-sex-matched case-control study. J. Clin. Biochem. Nutr. 2018, 62, 100–105. [Google Scholar] [CrossRef]
- Yang, Y.S.H.; Chang, H.W.; Lin, I.H.; Chien, L.N.; Wu, M.J.; Liu, Y.R.; Chu, P.G.; Xie, G.; Dong, F.; Jia, W.; et al. Long-term Proton Pump Inhibitor Administration Caused Physiological and Microbiota Changes in Rats. Sci. Rep. 2020, 10, 866. [Google Scholar] [CrossRef] [PubMed]
- He, Q.; Xia, B.; Yang, M.; Lu, K.; Fan, D.; Li, W.; Liu, Y.; Pan, Y.; Yuan, J. Alterations in gut microbiota and bile acids by proton-pump inhibitor use and possible mediating effects on elevated glucose levels and insulin resistance. FASEB J 2024, 38, e23541. [Google Scholar] [CrossRef]
- Fossmark, R.; Olaisen, M. Changes in the Gastrointestinal Microbiota Induced by Proton Pump Inhibitors—A Review of Findings from Experimental Trials. Microorganisms 2024, 12, 1110. [Google Scholar] [CrossRef]
- Weitsman, S.; Celly, S.; Leite, G.; Mathur, R.; Sedighi, R.; Barlow, G.M.; Morales, W.; Sanchez, M.; Parodi, G.; Villanueva-Millan, M.J.; et al. Effects of Proton Pump Inhibitors on the Small Bowel and Stool Microbiomes. Dig. Dis. Sci. 2022, 67, 224–232. [Google Scholar] [CrossRef]
- Zhang, X.; Li, Q.; Xia, S.; He, Y.; Liu, Y.; Yang, J.; Xiao, X. Proton Pump Inhibitors and Oral–Gut Microbiota: From Mechanism to Clinical Significance. Biomedicines 2024, 12, 2271. [Google Scholar] [CrossRef]
- Jackson, M.A.; Goodrich, J.K.; Maxan, M.E.; Freedberg, D.E.; Abrams, J.A.; Poole, A.C.; Sutter, J.L.; Welter, D.; Ley, R.E.; Bell, J.T.; et al. Proton pump inhibitors alter the composition of the gut microbiota. Gut 2016, 65, 749–756. [Google Scholar] [CrossRef]
- Wroblewski, L.E.; Peek, R.M., Jr.; Coburn, L.A. The Role of the Microbiome in Gastrointestinal Cancer. Gastroenterol. Clin. North. Am. 2016, 45, 543–556. [Google Scholar] [CrossRef]
- Zhang, M.L.; Fan, Y.X.; Meng, R.; Cai, W.K.; Yin, S.J.; Zhou, T.; Huang, Y.H.; Wang, P.; Jiang, F.F.; Yang, M.; et al. Proton Pump Inhibitors and Cancer Risk: An Umbrella Review and Meta-analysis of Observational Studies. Am. J. Clin. Oncol. 2022, 45, 475–485. [Google Scholar] [CrossRef] [PubMed]
- Sawaid, I.O.; Samson, A.O. Proton Pump Inhibitors and Cancer Risk: A Comprehensive Review of Epidemiological and Mechanistic Evidence. J. Clin. Med. 2024, 13, 1970. [Google Scholar] [CrossRef]
- Brusselaers, N.; Wahlin, K.; Engstrand, L.; Lagergren, J. Maintenance therapy with proton pump inhibitors and risk of gastric cancer: A nationwide population-based cohort study in Sweden. BMJ Open 2017, 7, e017739. [Google Scholar] [CrossRef]
- Tran, T.H.; Myung, S.K.; Trinh, T.T.K. Proton pump inhibitors and risk of gastrointestinal cancer: A meta-analysis of cohort studies. Oncol. Lett. 2024, 27, 28. [Google Scholar] [CrossRef]
- Cavalcoli, F.; Zilli, A.; Conte, D.; Ciafardini, C.; Massironi, S. Gastric neuroendocrine neoplasms and proton pump inhibitors: Fact or coincidence? Scand. J. Gastroenterol. 2015, 50, 1397–1403. [Google Scholar] [CrossRef]
- Poly, T.N.; Lin, M.C.; Syed-Abdul, S.; Huang, C.W.; Yang, H.C.; Li, Y.J. Proton Pump Inhibitor Use and Risk of Gastric Cancer: Current Evidence from Epidemiological Studies and Critical Appraisal. Cancers 2022, 14, 3052. [Google Scholar] [CrossRef]
- Pourhadi, N.; Janbek, J.; Jensen-Dahm, C.; Gasse, C.; Laursen, T.M.; Waldemar, G. Proton pump inhibitors and dementia: A nationwide population-based study. Alzheimer’s Dement. 2024, 20, 837–845. [Google Scholar] [CrossRef]
- Caplin, M.; Khan, K.; Savage, K.; Rode, J.; Varro, A.; Michaeli, D.; Grimes, S.; Brett, B.; Pounder, R.; Dhillon, A. Expression and processing of gastrin in hepatocellular carcinoma, fibrolamellar carcinoma and cholangiocarcinoma. J. Hepatol. 1999, 30, 519–526. [Google Scholar] [CrossRef]
- Ahn, N.; Nolde, M.; Krause, E.; Güntner, F.; Günter, A.; Tauscher, M.; Gerlach, R.; Meisinger, C.; Linseisen, J.; Baumeister, S.E.; et al. Do proton pump inhibitors increase the risk of dementia? A systematic review, meta-analysis and bias analysis. Br. J. Clin. Pharmacol. 2023, 89, 602–616. [Google Scholar] [CrossRef] [PubMed]
- Khan, Z.; Mehan, S.; Saifi, M.A.; Gupta, G.D.; Narula, A.S.; Kalfin, R. Proton Pump Inhibitors and Cognitive Health: Review on Unraveling the Dementia Connection and Co-morbid Risks. Curr. Alzheimer Res. 2024, 20, 739–757. [Google Scholar] [CrossRef] [PubMed]
- Surugiu, R.; Iancu, M.A.; Vintilescu, Ș.B.; Stepan, M.D.; Burdusel, D.; Genunche-Dumitrescu, A.V.; Dogaru, C.-A.; Dumitra, G.G. Molecular Mechanisms of Healthy Aging: The Role of Caloric Restriction, Intermittent Fasting, Mediterranean Diet, and Ketogenic Diet—A Scoping Review. Nutrients 2024, 16, 2878. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.M.; Juurlink, D.N. Navigating Drug Interactions with Proton Pump Inhibitors. JAMA Netw. Open 2024, 7, e2419818. [Google Scholar] [CrossRef]
- Bhatnagar, M.S.; Choudhari, S.; Pawar, D.; Sharma, A. Long-Term Use of Proton-Pump Inhibitors: Unravelling the Safety Puzzle. Cureus 2024, 16, e52773. [Google Scholar] [CrossRef]
- Cena, C.; Traina, S.; Parola, B.; Bo, M.; Fagiano, R.; Siviero, C. Prescription of proton pump inhibitors in older adults with complex polytherapy. Eur. J. Hosp. Pharm. 2020, 27, 341–345. [Google Scholar] [CrossRef]
- Drepper, M.D.; Spahr, L.; Frossard, J.L. Clopidogrel and proton pump inhibitors—where do we stand in 2012? World J. Gastroenterol. 2012, 18, 2161–2171. [Google Scholar] [CrossRef]
- Jourdi, G.; Jean-Sébastien, H.; Gaussem, P. An update on oral antiplatelet drug interactions with proton pump inhibitors: What are the risks? Expert Opin. Drug Metab. Toxicol. 2024, 20, 749–764. [Google Scholar] [CrossRef]
- Rababa, M.; Al-Ghassani, A.A.; Kovach, C.R.; Dyer, E.M. Proton Pump Inhibitors and the Prescribing Cascade. J. Gerontol. Nurs. 2016, 42, 23–31. [Google Scholar] [CrossRef]
- Padwale, V.; Kirnake, V.; Daswani, R.; Kodmalwar, A.; Gupta, A. A Comprehensive Review on the Efficacy and Safety of Vonoprazan in the Management of Gastric Acid-Related Diseases. Cureus 2024, 16, e64777. [Google Scholar] [CrossRef]
- American Geriatrics Society 2023 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. J. Am. Geriatr. Soc. 2023, 71, 2052–2081. [CrossRef]
- O’Mahony, D.; Cherubini, A.; Guiteras, A.R.; Denkinger, M.; Beuscart, J.-B.; Onder, G.; Gudmundsson, A.; Cruz-Jentoft, A.J.; Knol, W.; Bahat, G.; et al. STOPP/START criteria for potentially inappropriate prescribing in older people: Version 3. Eur. Geriatr. Med. 2023, 14, 625–632. [Google Scholar] [CrossRef]
- Wehling, M.; Weindrich, J.; Weiss, C.; Heser, K.; Pabst, A.; Luppa, M.; Bickel, H.; Weyerer, S.; Pentzek, M.; König, H.H.; et al. Validation of MyFORTA: An Automated Tool to Improve Medications in Older People Based on the FORTA List. Drugs Aging 2024, 41, 555–564. [Google Scholar] [CrossRef]
- Del-Pino, M.; Sanz, E.J. Analysis of deprescription strategies of proton pump inhibitors in primary care: A narrative review. Prim. Health Care Res. Dev. 2023, 24, e14. [Google Scholar] [CrossRef]
- Leszcynski, L.; Bente, J. Development and Implementation of a Pharmacist-Led Proton Pump Inhibitor Deprescribing Algorithm in a Geriatric Ambulatory Office. Sr. Care Pharm. 2023, 38, 105–112. [Google Scholar] [CrossRef]
- Xie, M.; You, J.H.S. Deprescribing of proton pump inhibitors in older patients: A cost-effectiveness analysis. PLoS ONE 2024, 19, e0311658. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Drug/Class | Interaction with PPI | Mechanism | Clinical Implication |
|---|---|---|---|
| Tyrosine kinase inhibitors (Danetimib, Erlotinib) | ↓ Absorption | Increased gastric pH | Reduced efficacy |
| Protease inhibitors (Atazanavir, Indinavir) | ↓ Absorption | Increased gastric pH | Reduced antiviral activity |
| Antifungals (Ketoconazole, Itraconazole) | ↓ Absorption | Increased gastric pH | Reduced antifungal efficacy |
| Oral iron preparations | ↓ Absorption | Reduced solubility due to increased pH | Iron deficiency risk |
| Clopidogrel | ↓ Activation | CYP2C19 inhibition | Reduced antiplatelet efficacy |
| Prasugrel, Ticagrelor | No interaction | Not dependent on CYP2C19 | Safe co-administration |
| Methotrexate | ↓ Elimination | Delayed clearance | Increased toxicity risk |
| Phenytoin | ↑ Levels | CYP2C19 inhibition | Toxicity (CNS symptoms) |
| Diazepam | ↑ Levels | CYP2C19 inhibition | Prolonged sedation |
| Carbamazepine | ↑ Levels | CYP3A4 inhibition | Risk of toxicity |
| Cyclosporine | ↑ Levels | CYP3A4 inhibition | Nephrotoxicity risk |
| Vonoprazan (P-CAB) | N/A | Not affected by CYP2C19 | Alternative in PPI resistance |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Condur, L.M.; Chirila, S.I.; Alexandrescu, L.; Iancu, M.A.; Neculau, A.E.; Berariu, F.V.; Toma, L.; Nicoara, A.D. Proton Pump Inhibitor Use in Older Adult Patients with Multiple Chronic Conditions: Clinical Risks and Best Practices. J. Clin. Med. 2025, 14, 5318. https://doi.org/10.3390/jcm14155318
Condur LM, Chirila SI, Alexandrescu L, Iancu MA, Neculau AE, Berariu FV, Toma L, Nicoara AD. Proton Pump Inhibitor Use in Older Adult Patients with Multiple Chronic Conditions: Clinical Risks and Best Practices. Journal of Clinical Medicine. 2025; 14(15):5318. https://doi.org/10.3390/jcm14155318
Chicago/Turabian StyleCondur, Laura Maria, Sergiu Ioachim Chirila, Luana Alexandrescu, Mihaela Adela Iancu, Andrea Elena Neculau, Filip Vasile Berariu, Lavinia Toma, and Alina Doina Nicoara. 2025. "Proton Pump Inhibitor Use in Older Adult Patients with Multiple Chronic Conditions: Clinical Risks and Best Practices" Journal of Clinical Medicine 14, no. 15: 5318. https://doi.org/10.3390/jcm14155318
APA StyleCondur, L. M., Chirila, S. I., Alexandrescu, L., Iancu, M. A., Neculau, A. E., Berariu, F. V., Toma, L., & Nicoara, A. D. (2025). Proton Pump Inhibitor Use in Older Adult Patients with Multiple Chronic Conditions: Clinical Risks and Best Practices. Journal of Clinical Medicine, 14(15), 5318. https://doi.org/10.3390/jcm14155318