
Mechanical Thrombectomy in Stroke—Retrospective Comparison of Methods: Aspiration vs. Stent Retrievers vs. Combined Method—Is Aspiration the Best Starting Point?

 , , ,
, , ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Image Analysis
2.3. Thrombectomy Technique
2.4. Aim of the Study
2.5. Statistical Analysis
3. Results
Study Population

{kind=link}
| mRS 0-2 Age [Mean] | mRS 3-6 Age [Mean] | p | |
|---|---|---|---|
| AO | 72.1 ± 12.9 | 72.4 ± 11.4 | 0.921 |
| SO | 68.7 ± 11.5 | 77.3 ± 8.8 | 0.009 |
| CM | 66.1 ± 17.4 | 76.7 ± 12.7 | 0.00001 |
| Method | mRS-90 | IVT—Yes | IVT—No | Odds Ratio (95% CI), p |
|---|---|---|---|---|
| AO | mRS 0-2 | 27 (53%) | 11 (24%) | 2.45 (1.05–5.73) p = 0.038 |
| mRS 3+ | 34 (47%) | 34 (76%) | ||
| SO | mRS 0-2 | 14 (54%) | 5 (29%) | 2.80 (0.77–10.25) p = 0.120 |
| mRS 3+ | 12 (46%) | 12 (71%) | ||
| CM | mRS 0-2 | 37 (44%) | 18 (43%) | 1.03 (0.48–2.17) p = 0.943 |
| mRS 3+ | 48 (56%) | 24 (57%) | ||
| Total | mRS 0-2 | 78 (45%) | 34 (33%) | 1.71 (1.03–2.84) p = 0.039 |
| mRS 3+ | 94 (55%) | 70 (67%) |
| Method | mRS 90 | ≤65 Years | ≥66 Years | Odds Ratio (95% CI), p |
|---|---|---|---|---|
| AO | mRS 0-2 | 11 (46%) | 27 (33%) | 1.72 (0.68–4.35) p = 0.249 |
| mRS 3+ | 13 (54%) | 55 (67%) | ||
| SO | mRS 0-2 | 6 (60%) | 13 (39%) | 2.31 (0.54–9.79) p = 0.257 |
| mRS 3+ | 4 (40%) | 20 (61%) | ||
| CM | mRS 0-2 | 21 (64%) | 34 (36%) | 3.09 (1.35–7.04) p = 0.007 |
| mRS 3+ | 12 (36%) | 60 (64%) | ||
| Total | mRS 0-2 | 38 (57%) | 74 (35%) | 1.99 (1.17–3.38) p = 0.011 |
| mRS 3+ | 29 (43%) | 135 (65%) |
| Method | mRS-90 | FP TICI 3: Yes | FP TICI 3: No | Odds Ratio (95% CI), p |
|---|---|---|---|---|
| AO | mRS 0-2 | 18 (37%) | 20 (35%) | 1.07 (0.48–2.38) p = 0.860 |
| mRS 3+ | 31 (63%) | 37 (65%) | ||
| SO | mRS 0-2 | 7 (78%) | 13 (38%) | 5.65 (1.01–3.47) p = 0.048 |
| mRS 3+ | 2 (22%) | 21 (62%) | ||
| CM | mRS 0-2 | 31 (60%) | 24 (32%) | 3.13 (1.50–6.55) p = 0.002 |
| mRS 3+ | 21 (40%) | 51 (68%) | ||
| Total | mRS 0-2 | 56 (51%) | 57 (34%) | 1.98 (1.21–3.25) p = 0.006 |
| mRS 3+ | 54 (49%) | 109 (66%) |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jovin, T.G.; Chamorro, A.; Cobo, E.; De Miquel, M.A.; Molina, C.A.; Rovira, A.; Román, L.S.; Serena, J.; Abilleira, S.; Ribo, M.; et al. Thrombectomy within 8 Hours after Symptom Onset in Ischemic Stroke. N. Engl. J. Med. 2015, 372, 2296–2306. [Google Scholar] [CrossRef]
- Goyal, M.; Demchuk, A.M.; Menon, B.K.; Eesa, M.; Rempel, J.L.; Thornton, J.; Roy, D.; Jovin, T.G.; Willinsky, R.A.; Sapkota, B.L.; et al. Randomized Assessment of Rapid Endovascular Treatment of Ischemic Stroke. N. Engl. J. Med. 2015, 372, 1019–1030. [Google Scholar] [CrossRef]
- Berkhemer, O.A.; Fransen, P.S.S.; Beumer, D.; Berg, L.A.V.D.; Lingsma, H.F.; Yoo, A.J.; Schonewille, W.J.; Vos, J.A.; Nederkoorn, P.J.; Wermer, M.J.H.; et al. A Randomized Trial of Intraarterial Treatment for Acute Ischemic Stroke. N. Engl. J. Med. 2015, 372, 11–20. [Google Scholar] [CrossRef]
- Goyal, M.; Menon, B.K.; Van Zwam, W.H.; Dippel, D.W.J.; Mitchell, P.J.; Demchuk, A.M.; Dávalos, A.; Majoie, C.B.L.M.; Van Der Lugt, A.; De Miquel, M.A.; et al. Endovascular thrombectomy after large-vessel ischaemic stroke: A meta-analysis of individual patient data from five randomised trials. Lancet 2016, 387, 1723–1731. [Google Scholar] [CrossRef] [PubMed]
- Meder, G.; Świtońska, M.; Płeszka, P.; Palacz-Duda, V.; Dzianott-Pabijan, D.; Sokal, P. Endovascular Treatment of Stroke Caused by Carotid Artery Dissection. Brain Sci. 2020, 10, 800. [Google Scholar] [CrossRef]
- Meder, G.; Żuchowski, P.; Skura, W.; Palacz-Duda, V.; Świtońska, M.; Nowaczewska, M.; Sokal, P. Mechanical Thrombectomy in Stroke. Experience from Switching from Stent Retriever Only to Stent Retriever Combined with Aspiration Catheter. J. Clin. Med. 2021, 10, 1802. [Google Scholar] [CrossRef] [PubMed]
- Lapergue, B.; Blanc, R.; Gory, B.; Labreuche, J.; Duhamel, A.; Marnat, G.; Saleme, S.; Costalat, V.; Bracard, S.; Desal, H.; et al. Effect of endovascular contact aspiration vs stent retriever on revascularization in patients with acute ischemic stroke and large vessel occlusion: The ASTER randomized clinical trial. JAMA J. Am. Med. Assoc. 2017, 318, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Maus, V.; Henkel, S.; Riabikin, A.; Riedel, C.; Behme, D.; Tsogkas, I.; Hesse, A.C.; Abdullayev, N.; Jansen, O.; Wiesmann, M.; et al. The SAVE Technique: Large-Scale Experience for Treatment of Intracranial Large Vessel Occlusions. Clin. Neuroradiol. 2019, 29, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Maus, V.; Behme, D.; Kabbasch, C.; Borggrefe, J.; Tsogkas, I.; Nikoubashman, O.; Wiesmann, M.; Knauth, M.; Mpotsaris, A.; Psychogios, M.N. Maximizing First-Pass Complete Reperfusion with SAVE. Clin. Neuroradiol. 2018, 28, 327–338. [Google Scholar] [CrossRef] [PubMed]
- Meng, J.; Yan, Z.; Zhang, J.; Wang, W.; Tao, X.; Gu, F.; Yang, X.; Xue, T.; You, W.; Chen, Z.; et al. Comparative efficacy and safety of various mechanical thrombectomy strategies for patients with acute ischemic stroke: A Bayesian network meta-analysis. Ther. Adv. Neurol. Disord. 2023, 16, 17562864231181180. [Google Scholar] [CrossRef]
- Ye, G.; Cao, R.; Chen, P.; Wang, H.; Wang, D.; Chen, M.; Li, Z. Network meta-analysis of first-line thrombectomy strategy for acute posterior circulation strokes: A preliminary evaluation for combined approach. Front. Neurol. 2023, 14, 1279233. [Google Scholar] [CrossRef]
- Zaidat, O.O.; Yoo, A.J.; Khatri, P.; Tomsick, T.A.; von Kummer, R.; Saver, J.L.; Marks, M.P.; Prabhakaran, S.; Kallmes, D.F.; Fitzsimmons, B.-F.M.; et al. Recommendations on Angiographic Revascularization Grading Standards for Acute Ischemic Stroke: A consensus statement. Stroke 2013, 44, 2650–2663. [Google Scholar] [CrossRef]
- Goyal, M.; Fargen, K.M.; Turk, A.S.; Mocco, J.; Liebeskind, D.S.; Frei, D.; Demchuk, A.M. 2C or not 2C: Defining an improved revascularization grading scale and the need for standardization of angiography outcomes in stroke trials. J. Neurointerv. Surg. 2014, 6, 83–86. [Google Scholar] [CrossRef]
- Colasurdo, M.; Gabrieli, J.D.; Cester, G.; Edhayan, G.; Simonato, D.; Pieroni, A.; De Cassai, A.; Geraldini, F.; Baracchini, C.; Causin, F. SOFIA Nonwire Advancement techniKE 35 Technique: A Minimalist Approach to Stroke Thrombectomy. Neurosurg. 2022, 23, 482–488. [Google Scholar] [CrossRef]
- Heit, J.J.; Wong, J.H.; Mofaff, A.M.; A Telischak, N.; Dodd, R.L.; Marks, M.P.; Do, H.M. Sofia intermediate catheter and the SNAKE technique: Safety and efficacy of the Sofia catheter without guidewire or microcatheter construct. J. Neurointerv. Surg. 2018, 10, 401–406. [Google Scholar] [CrossRef]
- Volny, O.; Krajina, A.; Belaskova, S.; Bar, M.; Cimflova, P.; Herzig, R.; Sanak, D.; Tomek, A.; Köcher, M.; Rocek, M.; et al. Mechanical thrombectomy performs similarly in real world practice: A 2016 nationwide study from the Czech Republic. J. Neurointerv. Surg. 2017, 10, 741–745. [Google Scholar] [CrossRef]
- Saver, J.L.; Goyal, M.; Bonafe, A.; Diener, H.-C.; Levy, E.I.; Pereira, V.M.; Albers, G.W.; Cognard, C.; Cohen, D.J.; Hacke, W.; et al. Stent-Retriever Thrombectomy after Intravenous t-PA vs. t-PA Alone in Stroke. N. Engl. J. Med. 2015, 372, 2285–2295. [Google Scholar] [CrossRef]
- Słowik, A.; Wnuk, M.; Brzegowy, P.; Chrzanowska-Waśko, J.; Golenia, A.; Łasocha, B.; Włoch-Kopeć, D.; Ferens, A.; Serednicki, W.; Jarocki, P.; et al. Mechanical thrombectomy in acute stroke—Five years of experience in Poland. Neurol. Neurochir. Pol. 2017, 51, 339–346. [Google Scholar] [CrossRef]
- Brehm, A.; Maus, V.; Tsogkas, I.; Colla, R.; Hesse, A.C.; Gera, R.G.; Psychogios, M.-N. Stent-retriever assisted vacuum-locked extraction (SAVE) versus a direct aspiration first pass technique (ADAPT) for acute stroke: Data from the real-world. BMC Neurol. 2019, 19, 65. [Google Scholar] [CrossRef]
- Nikoubashman, O.; Nikoubashman, A.; Büsen, M.; Wiesmann, M. Necessary Catheter Diameters for Mechanical Thrombectomy with ADAPT. Am. J. Neuroradiol. 2017, 38, 2277–2281. [Google Scholar] [CrossRef]
- Machi, P.; Jourdan, F.; Ambard, D.; Reynaud, C.; Lobotesis, K.; Sanchez, M.; Bonafé, A.; Costalat, V. Experimental evaluation of stent retrievers’ mechanical properties and effectiveness. J. Neurointerv. Surg. 2017, 9, 257–263. [Google Scholar] [CrossRef]
- Massari, F.; Henninger, N.; Lozano, J.D.; Patel, A.; Kuhn, A.L.; Howk, M.; Perras, M.; Brooks, C.; Gounis, M.J.; Kan, P.; et al. ARTS (Aspiration–Retriever Technique for Stroke): Initial clinical experience. Interv. Neuroradiol. 2016, 22, 325–332. [Google Scholar] [CrossRef]
- Humphries, W.; Hoit, D.; Doss, V.T.; Elijovich, L.; Frei, D.; Loy, D.; Dooley, G.; Turk, A.S.; Chaudry, I.; Turner, R.; et al. Distal aspiration with retrievable stent assisted thrombectomy for the treatment of acute ischemic stroke. J. Neurointerv. Surg. 2015, 7, 90–94. [Google Scholar] [CrossRef]
- Lee, J.S.; Hong, J.M.; Lee, S.-J.; Joo, I.S.; Lim, Y.C.; Kim, S.Y. The combined use of mechanical thrombectomy devices is feasible for treating acute carotid terminus occlusion. Acta Neurochir. 2013, 155, 635–641. [Google Scholar] [CrossRef]
- A Munich, S.; Vakharia, K.; I Levy, E. Overview of Mechanical Thrombectomy Techniques. Clin. Neurosurg. 2019, 85, S60–S67. [Google Scholar] [CrossRef]
- Khatri, P.; Abruzzo, T.; Yeatts, S.D.; Nichols, C.; Broderick, J.P.; Tomsick, T.A. Good clinical outcome after ischemic stroke with successful revascularization is time-dependent. Neurology 2009, 73, 1066–1072. [Google Scholar] [CrossRef]
- Goyal, M.; Jadhav, A.P.; Bonafe, A.; Diener, H.; Pereira, V.M.; Levy, E.; Baxter, B.; Jovin, T.; Jahan, R.; Menon, B.K.; et al. Analysis of Workflow and Time to Treatment and the Effects on Outcome in Endovascular Treatment of Acute Ischemic Stroke: Results from the SWIFT PRIME Randomized Controlled Trial. Radiology 2016, 279, 888–897. [Google Scholar] [CrossRef]
- Shi, Z.-S.; Liebeskind, D.S.; Xiang, B.; Ge, S.G.; Feng, L.; Albers, G.W.; Budzik, R.; Devlin, T.; Gupta, R.; Jansen, O.; et al. Predictors of Functional Dependence Despite Successful Revascularization in Large-Vessel Occlusion Strokes. Stroke 2014, 45, 1977–1984. [Google Scholar] [CrossRef]
- Nikoubashman, O.; Dekeyzer, S.; Riabikin, A.; Keulers, A.; Reich, A.; Mpotsaris, A.; Wiesmann, M. True First-Pass Effect: First-Pass Complete Reperfusion Improves Clinical Outcome in Thrombectomy Stroke Patients. Stroke 2019, 50, 2140–2146. [Google Scholar] [CrossRef]
- Zaidat, O.O.; Castonguay, A.C.; Linfante, I.; Gupta, R.; Martin, C.O.; Holloway, W.E.; Mueller-Kronast, N.; English, J.D.; Dabus, G.; Malisch, T.W.; et al. First pass effect: A new measure for stroke thrombectomy devices. Stroke 2018, 49, 660–666. [Google Scholar] [CrossRef]
- Nguyen, T.N.; Malisch, T.; Castonguay, A.C.; Gupta, R.; Sun, C.-H.J.; Martin, C.O.; Holloway, W.E.; Mueller-Kronast, N.; English, J.D.; Linfante, I.; et al. Balloon Guide Catheter Improves Revascularization and Clinical Outcomes with the Solitaire Device. Stroke 2014, 45, 141–145. [Google Scholar] [CrossRef]
- Zaidat, O.O.; Mueller-Kronast, N.H.; Hassan, A.E.; Haussen, D.C.; Jadhav, A.P.; Froehler, M.T.; Jahan, R.; Aziz-Sultan, M.A.; Klucznik, R.P.; Saver, J.L.; et al. Impact of Balloon Guide Catheter Use on Clinical and Angiographic Outcomes in the STRATIS Stroke Thrombectomy Registry. Stroke 2019, 50, 697–704. [Google Scholar] [CrossRef]
- Velasco, A.; Buerke, B.; Stracke, C.P.; Berkemeyer, S.; Mosimann, P.J.; Schwindt, W.; Alcázar, P.; Cnyrim, C.; Niederstadt, T.; Chapot, R.; et al. Comparison of a Balloon Guide Catheter and a Non–Balloon Guide Catheter for Mechanical Thrombectomy. Radiology 2016, 280, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Brinjikji, W.; Starke, R.M.; Murad, M.H.; Fiorella, D.; Pereira, V.M.; Goyal, M.; Kallmes, D.F. Impact of balloon guide catheter on technical and clinical outcomes: A systematic review and meta-analysis. J. Neurointerv. Surg. 2018, 10, 335–339. [Google Scholar] [CrossRef] [PubMed]
- Goldhoorn, R.-J.B.; Duijsters, N.; Majoie, C.B.; Roos, Y.B.; Dippel, D.W.; van Es, A.C.; Vos, J.A.; Boiten, J.; van Oostenbrugge, R.J.; van Zwam, W.H. Balloon Guide Catheter in Endovascular Treatment for Acute Ischemic Stroke: Results from the MR CLEAN Registry. J. Vasc. Interv. Radiol. 2019, 30, 1759–1764.e6. [Google Scholar] [CrossRef] [PubMed]
- Hidaka, M.; Yamaguchi, S.; Koyanagi, Y.; Arakawa, S. Reocclusion of the treated vessel due to endothelial injury after mechanical thrombectomy in a patient with acute ischaemic stroke. BMJ Case Rep. 2019, 12, e228937. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Gu, F.; Ding, J.; Bian, J.; Wang, N.; Shu, R.; Li, Q.; Xu, X. The predictors and prognosis for unexpected reocclusion after mechanical thrombectomy: A meta-analysis. Ann. Transl. Med. 2020, 8, 1566. [Google Scholar] [CrossRef] [PubMed]
- Teng, D.; Pannell, J.S.; Rennert, R.C.; Li, J.; Li, Y.-S.; Wong, V.W.; Chien, S.; Khalessi, A.A. Endothelial Trauma from Mechanical Thrombectomy in Acute Stroke. Stroke 2015, 46, 1099–1106. [Google Scholar] [CrossRef] [PubMed]
- Hernández, D.; Cuevas, J.L.; Gragmegna, L.L.; Requena, M.; Piñana, C.; de Dios, M.; Coscojuela, P.; Esteves, M.; Li, J.; Gil, A.; et al. Increased Number of Passes and Double Stent Retriever Technique Induces Cumulative Injury on Arterial Wall After Mechanical Thrombectomy in a Swine Model. Transl. Stroke Res. 2022, 14, 425–433. [Google Scholar] [CrossRef]
- Dhoisne, M.; Puy, L.; Bretzner, M.; Bricout, N.; Behal, H.; Cordonnier, C.; Henon, H. Early reocclusion after successful mechanical thrombectomy for large artery occlusion–related stroke. Int. J. Stroke 2023, 18, 712–719. [Google Scholar] [CrossRef]
- Bourcier, R.; Saleme, S.; Labreuche, J.; Mazighi, M.; Fahed, R.; Blanc, R.; Gory, B.; Kyheng, M.; Marnat, G.; Bracard, S.; et al. More than three passes of stent retriever is an independent predictor of parenchymal hematoma in acute ischemic stroke. J. Neurointerv. Surg. 2019, 11, 625–629. [Google Scholar] [CrossRef]
- Texakalidis, P.; Giannopoulos, S.; Karasavvidis, T.; Rangel-Castilla, L.; Rivet, D.J.; Reavey-Cantwell, J. Mechanical Thrombectomy in Acute Ischemic Stroke: A Meta-Analysis of Stent Retrievers vs. Direct Aspiration vs. a Combined Approach. Neurosurgery 2020, 86, 464–477. [Google Scholar] [CrossRef]
- Baia, X.; Zhanga, X.; Gonga, H.; Wang, T.; Wang, X.; Wang, W.; Yang, K.; Yang, W.; Feng, Y.; Ma, Y.; et al. Different types of percutaneous endovascular interventions for acute ischemic stroke. Cochrane Database Syst. Rev. 2023, 2023, CD014676. [Google Scholar] [CrossRef]
- Rhiner, N.; Thut, M.Z.; Thurner, P.; Madjidyar, J.; Schubert, T.; Globas, C.; Wegener, S.; Luft, A.R.; Michels, L.; Kulcsar, Z. Impact of age on mechanical thrombectomy and clinical outcome in patients with acute ischemic stroke. J. Stroke Cerebrovasc. Dis. 2023, 32, 107248. [Google Scholar] [CrossRef]
- Alawieh, A.; Vargas, J.; Fargen, K.M.; Langley, E.F.; Starke, R.M.; De Leacy, R.; Chatterjee, R.; Rai, A.; Dumont, T.; Kan, P.; et al. Impact of Procedure Time on Outcomes of Thrombectomy for Stroke. J. Am. Coll. Cardiol. 2019, 73, 879–890. [Google Scholar] [CrossRef]
- Mandalà, M.; Cipolla, M.J. Aging-Related Structural and Functional Changes in Cerebral Arteries: Caloric Restriction (CR) Intervention. J. Vasc. Med. Surg. 2021, 9 (Suppl. S7), 1000002. [Google Scholar]
- Gariel, F.; Lapergue, B.; Bourcier, R.; Berge, J.; Barreau, X.; Mazighi, M.; Kyheng, M.; Labreuche, J.; Fahed, R.; Blanc, R.; et al. Mechanical Thrombectomy Outcomes with or without Intravenous Thrombolysis. Stroke 2018, 49, 2383–2390. [Google Scholar] [CrossRef]
- Yang, W.; Lee, R.P.; Hung, A.L.; Young, C.C.; Sattari, S.A.; Urrutia, V.; Gailloud, P.E.; Xu, R.; Caplan, J.; Gonzalez, L.F. Cost-Effectiveness of a Direct-Aspiration First-Pass Technique versus Stent Retriever in Mechanical Thrombectomy. World Neurosurg. 2023, in press. [Google Scholar] [CrossRef]
- Malhotra, A.; Boltyenkov, A.; Wu, X.; Matouk, C.C.; Forman, H.P.; Gandhi, D.; Sanelli, P. Endovascular Contact Aspiration versus Stent Retriever for Revascularization in Patients with Acute Ischemic Stroke and Large Vessel Occlusion: A Cost-Minimization Analysis. World Neurosurg. 2020, 139, e23–e31. [Google Scholar] [CrossRef]
| Parameter | Overall (n = 276) | SO (n = 43) | CM (n = 127) | AO (n = 106) | p-Value |
|---|---|---|---|---|---|
| Site of occlusion | |||||
| Carotid | 54 | 6 | 28 | 23 | 0.286 |
| M1 | 144 | 22 | 62 | 60 | |
| M2 | 69 | 12 | 20 | 37 | |
| Age (yrs ± SD) | 72.4 ± 1364 | 73.5 ± 10.9 | 72.1 ± 15.7 | 72.3 ± 11.9 | 0.838 |
| Male sex | 120 (44%) | 18 (42%) | 55 (43%) | 47 (44%) | 0.961 |
| Atrial fibrillation/ICD/PM | 127 (46%) | 22 (51%) | 60 (47%) | 45 (42%) | 0.584 |
| Arterial hypertension | 213 (77%) | 36 (84%) | 96 (76%) | 81 (76%) | 0.07 |
| Coronary heart disease | 68 (25%) | 12 (28%) | 33 (26%) | 23 (22%) | 0.649 |
| Dyslipidemia | 99 (36%) | 20 (47%) | 46 (36%) | 33 (31%) | 0.206 |
| ASPECTS median, (IQR) | 7 (6–8) | 8 (7–9) | 7 (6–8) | 7 (6–7) | <0.001 |
| NIHSS admission median, (IQR) | 16 (13–20) | 17 (13–21) | 15 (12–19) | 15 (14–20) | 0.222 |
| Symptom onset to thrombectomy in minutes (mean ± SD) | 268 ± 79 | 261 ± 79 | 268 ± 76 | 272 ± 84 | 0.755 |
| ivTPa | 172 (62.3%) | 26 (60.4%) | 85 (66.9%) | 61 (57.5%) | 0.326 |
| Goal | SO | CM | AO | p-Value |
|---|---|---|---|---|
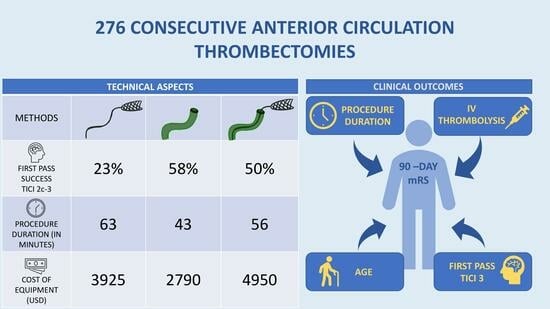
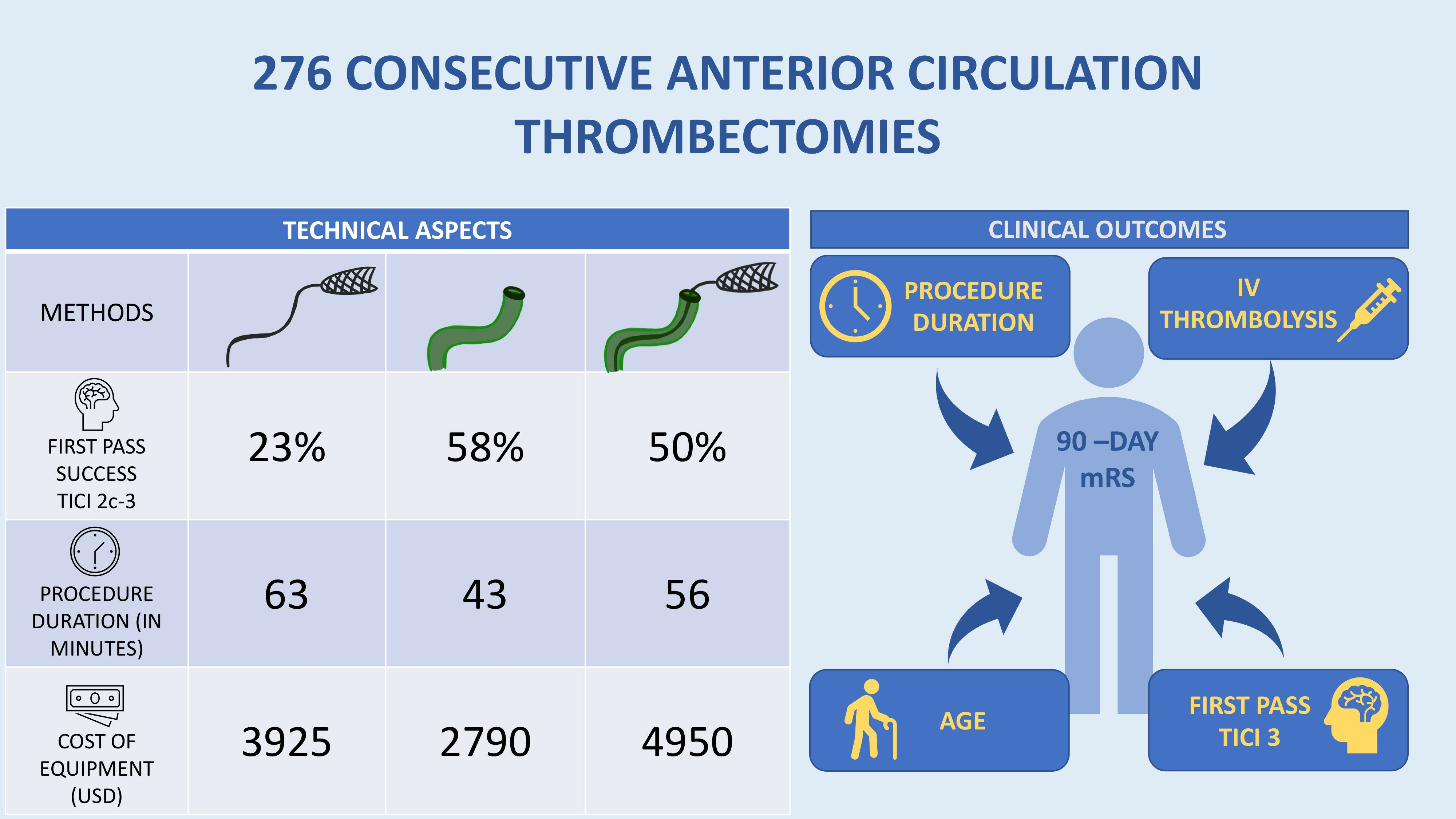
| First pass mTICI 3 | 9 (21%) | 52 (41%) | 49 (46%) | 0.016 |
| First pass mTICI 2c-3 | 10 (23%) | 63 (50%) | 61 (58%) | <0.001 |
| Procedure success mTICI 2b-3 | 38 (88%) | 114 (90%) | 101 (95%) | 0.62 |
| Mean number of passes needed | 2.1 ± 1.0 | 1.9 ± 1.4 | 1.6 ± 1.1 | 0.097 |
| Mean duration of the procedure (minutes ± SD) | 63 ± 32 | 56 ± 27 | 43 ± 23 | <0.0001 |
| 90-day mRS, median (IQR) | 3 (1-6) | 3 (1-6) | 4 (1-6) | 0.83 |
| ∂ NIHSS (± SD) (excluding deaths) | 7.5 ± 4.8 | 6.9 ± 5.9 | 7.1 ± 6.7 | 0.92 |
| In-hospital mortality | 12 (28%) | 34 (27%) | 34 (32%) | 0.66 |
| SICH (%) | 2 (5%) | 11 (9%) | 9 (8%) | 0.681 |
| ICH + SAH | 7 (16%) | 18 (14%) | 11 (10%) | 0.548 |
| mRS-90 (0-2) No (%) of Patients | mRS-90 (3-6) No (%) of Patients | p-Value | |
|---|---|---|---|
| AO | 38 (35.8) | 68 (64.2) | 0.448 |
| SO | 19 (44.1) | 24 (55.9) | |
| CM | 55 (43.3) | 72 (56.7) |
| mRS 0-2, Procedure Duration [Min] | mRS 3-6, Procedure Duration [Min] | p-Value | |
|---|---|---|---|
| AO | 43.1 ± 31.1 | 43.5 ± 24.3 | 0.931 |
| SO | 61.1 ± 31.1 | 65.8 ± 34.2 | 0.645 |
| CM | 49.1 ± 21.7 | 62.0 ± 29.1 | 0.007 |
| p-value | 0.024 | 0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meder, G.; Żuchowski, P.; Skura, W.; Płeszka, P.; Dura, M.; Rajewski, P.; Nowaczewska, M.; Meder, M.; Alexandre, A.M.; Pedicelli, A. Mechanical Thrombectomy in Stroke—Retrospective Comparison of Methods: Aspiration vs. Stent Retrievers vs. Combined Method—Is Aspiration the Best Starting Point? J. Clin. Med. 2024, 13, 1477. https://doi.org/10.3390/jcm13051477
Meder G, Żuchowski P, Skura W, Płeszka P, Dura M, Rajewski P, Nowaczewska M, Meder M, Alexandre AM, Pedicelli A. Mechanical Thrombectomy in Stroke—Retrospective Comparison of Methods: Aspiration vs. Stent Retrievers vs. Combined Method—Is Aspiration the Best Starting Point? Journal of Clinical Medicine. 2024; 13(5):1477. https://doi.org/10.3390/jcm13051477
Chicago/Turabian StyleMeder, Grzegorz, Paweł Żuchowski, Wojciech Skura, Piotr Płeszka, Marta Dura, Piotr Rajewski, Magdalena Nowaczewska, Magdalena Meder, Andrea M Alexandre, and Alessandro Pedicelli. 2024. "Mechanical Thrombectomy in Stroke—Retrospective Comparison of Methods: Aspiration vs. Stent Retrievers vs. Combined Method—Is Aspiration the Best Starting Point?" Journal of Clinical Medicine 13, no. 5: 1477. https://doi.org/10.3390/jcm13051477
APA StyleMeder, G., Żuchowski, P., Skura, W., Płeszka, P., Dura, M., Rajewski, P., Nowaczewska, M., Meder, M., Alexandre, A. M., & Pedicelli, A. (2024). Mechanical Thrombectomy in Stroke—Retrospective Comparison of Methods: Aspiration vs. Stent Retrievers vs. Combined Method—Is Aspiration the Best Starting Point? Journal of Clinical Medicine, 13(5), 1477. https://doi.org/10.3390/jcm13051477