
A Single Session of Temporomandibular Joint Soft Tissue Therapy and Its Effect on Pelvic Floor Muscles Activity in Women—A Randomized Controlled Trial


Abstract
1. Introduction
2. Materials and Methods
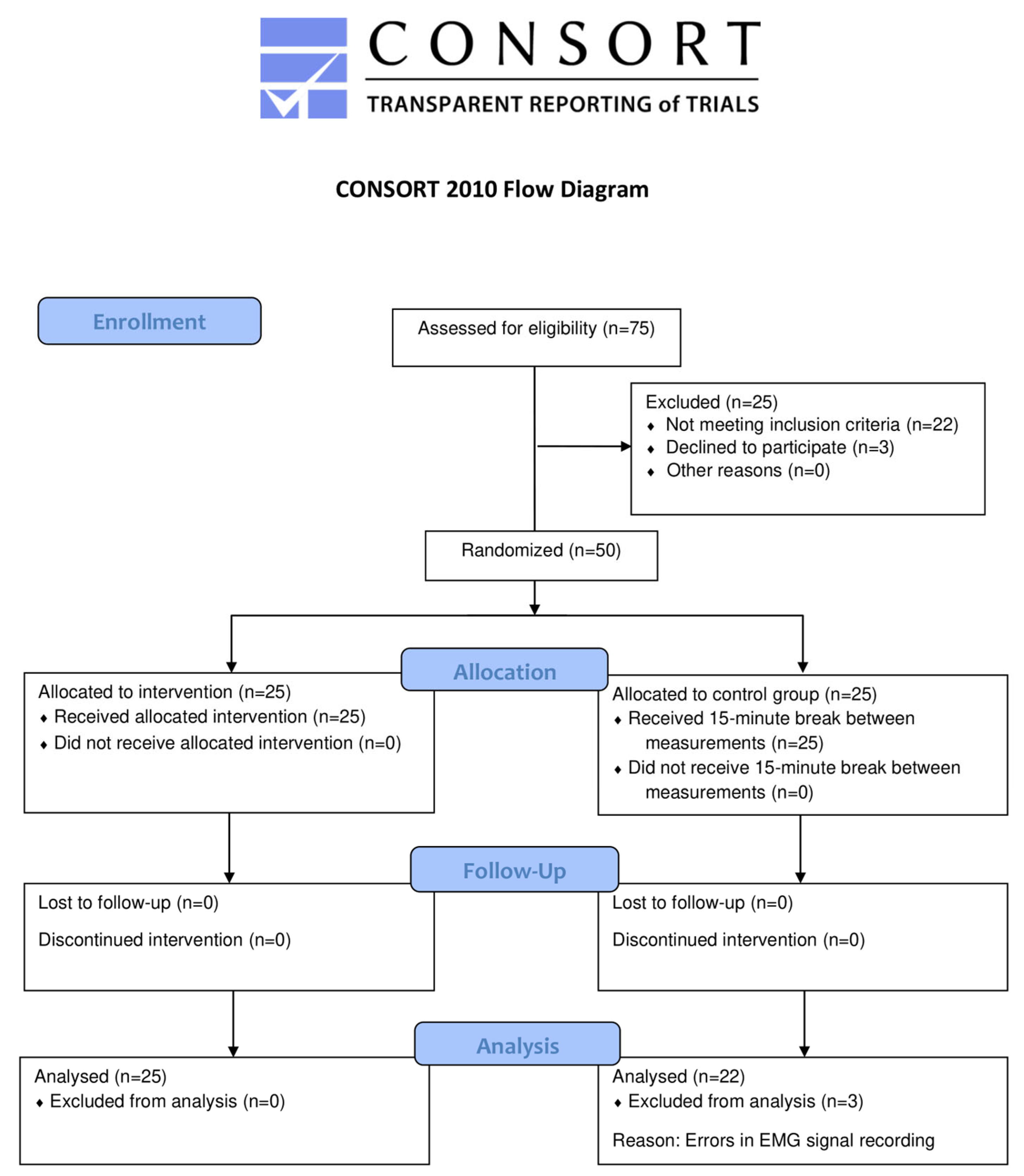
2.1. Study Design
2.2. Participants
2.3. Research Tools
2.3.1. Ultrasonography
2.3.2. Surface Electromyography (sEMG)
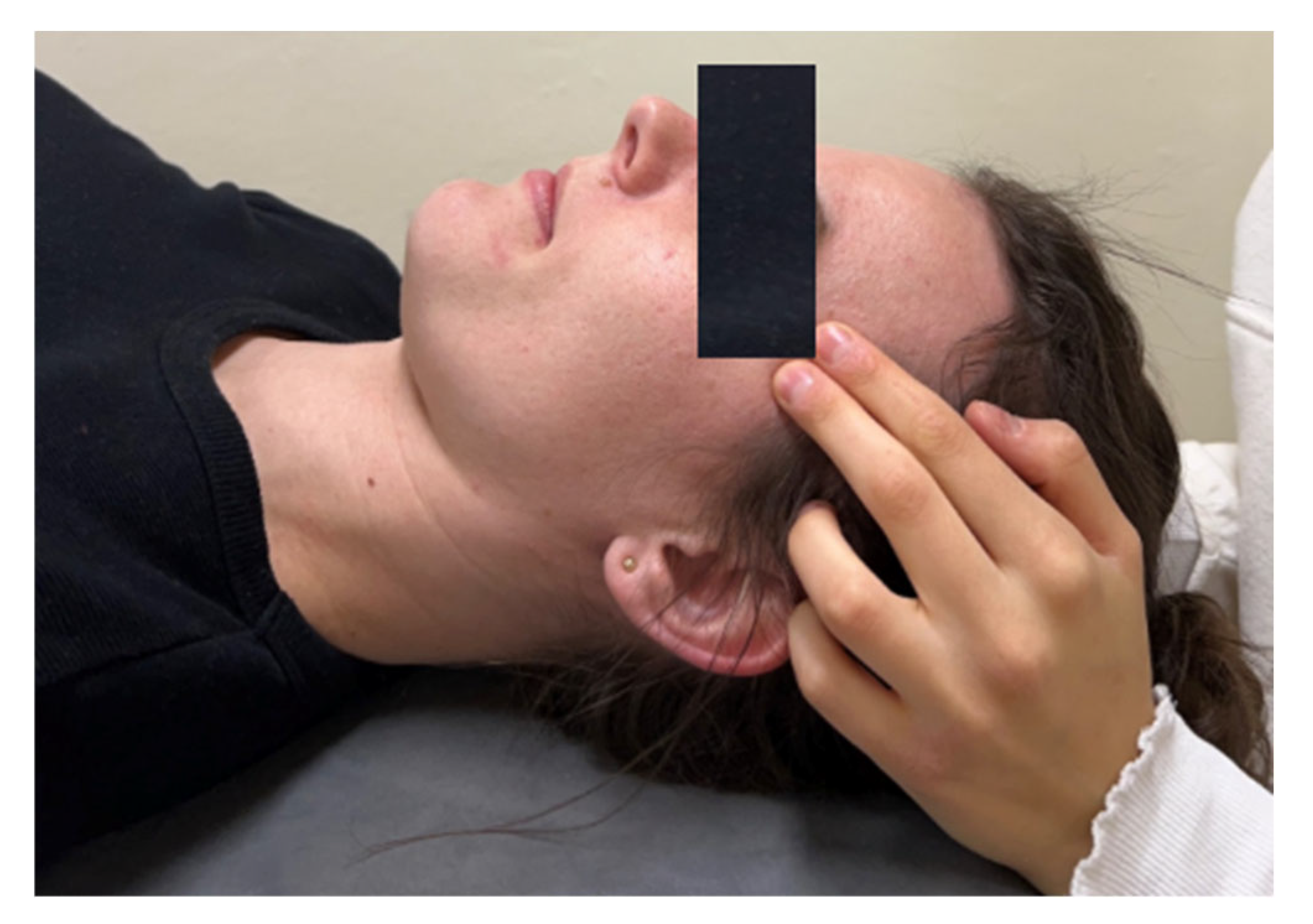
2.4. Intervention
- (A)
- Temporalis muscle relaxation:
- -
- Trigger point therapy on the temporalis muscle (technique duration: 1 minute).
- -
- Myofascial release along the path of the trigger point on the temporalis muscle (technique duration: 1 minute).
- -
- Positional relaxation of the temporalis muscle (technique duration: 30 seconds).
- -
- Myofascial release of the temporalis muscle; work along the muscle from top to bottom (technique duration: 30 s).
- (B)
- Masseter muscle relaxation: myofascial release along the path of the muscle from top to bottom (technique duration: 30 s).
- (A)
- Pterygoid muscle relaxation (technique duration: 1 minute).
- (B)
- Masseter muscle relaxation:
- -
- Myofascial release along the path of the muscle fibers (technique duration: 1 minute).
- -
- Trigger point release in the attachment area (technique duration: 1 minute).
2.5. Statistical Analysis
3. Results
3.1. Activation of the PFM Using USG Measurement
3.2. Bioelectrical Activity of the PFM
3.2.1. Resting Activity of the PFM During a 1-Minute Rest Period (First Phase of the Measurement Protocol—Pre-Exercise)
3.2.2. Activity of the PFM During 2-Second Phasic Contractions
3.2.3. Activity of the PFM During 10-Second Tonic Contractions
3.2.4. Activity of the PFM During 60-Second Endurance Contraction
3.2.5. Resting Activity of the PFM During a 1-Minute Rest Period (Last Phase of the Measurement Protocol—Post-Exercise)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Adamiak-Godlewska, A.; Rechberger, T. Evaluation of Pelvic Floor Muscle Anatomy and Function in Women: Modern Techniques. Menopausal Rev. 2012, 16, 259–263. [Google Scholar] [CrossRef]
- Baessler, K.; Schüssler, B.; Burgio, K.L.; Moore, K.H.; Norton, P.A.; Stanton, S.L. (Eds.) Pelvic Floor Re-Education. Principles and Practice, 2nd ed.; Springer: London, UK, 2008; ISBN 978-1-85233-968-5. [Google Scholar]
- Myers, T.W. Anatomy Trains: Myofascial Meridians for Manual and Movement Therapists; Elsevier, Churchill Livingstone: Medford, MA, USA, 2020. [Google Scholar]
- Ramin, A.; Macchi, V.; Porzionato, A.; De Caro, R.; Stecco, C. Fascial Continuity of the Pelvic Floor with the Abdominal and lumbar Region. Pelviperineology 2015, 35, 3–6. [Google Scholar]
- Tim, S.; Mazur-Bialy, A.I. The Most Common Functional Disorders and Factors Affecting Female Pelvic Floor. Life 2021, 11, 1397. [Google Scholar] [CrossRef] [PubMed]
- Blanpied, P.R.; Gross, A.R.; Elliott, J.M.; Devaney, L.L.; Clewley, D.; Walton, D.M.; Sparks, C.; Robertson, E.K. Neck Pain: Revision 2017. J. Orthop. Sports Phys. Ther. 2017, 47, A1–A83. [Google Scholar] [CrossRef] [PubMed]
- Jull, G.; Sterling, M.; Falla, D.; Treleaven, J.; O’Leary, S. Whiplash, Headache, and Neck Pain; Elsevier: Amsterdam, The Netherlands, 2008; ISBN 9780443100475. [Google Scholar]
- Szymańska, D. Ocena Zaburzeń Stawu Skroniowo-Żuchwowego w Aspekcie Aktywności Bioelektrycznej. Aktual. Probl. Biomech. 2014, 8, 151–156. [Google Scholar]
- Lee, Y.-J.; Park, J.-H.; Lee, S.-J.; Ryu, H.-M.; Kim, S.; Lee, Y.-J.; Yoon, H.-M.; Jang, S.-H.; Song, C.-H.; Kim, C.-H. Systematic Review of the Correlation Between Temporomandibular Disorder and Body Posture. J. Acupunct. Res. 2017, 34, 159–168. [Google Scholar] [CrossRef]
- Zieliński, G.; Ginszt, M.; Zawadka, M.; Rutkowska, K.; Podstawka, Z.; Szkutnik, J.; Majcher, P.; Gawda, P. The Relationship between Stress and Masticatory Muscle Activity in Female Students. J. Clin. Med. 2021, 10, 3459. [Google Scholar] [CrossRef]
- van Reijn-Baggen, D.A.; Han-Geurts, I.J.M.; Voorham-van der Zalm, P.J.; Pelger, R.C.M.; Hagenaars-van Miert, C.H.A.C.; Laan, E.T.M. Pelvic Floor Physical Therapy for Pelvic Floor Hypertonicity: A Systematic Review of Treatment Efficacy. Sex. Med. Rev. 2022, 10, 209–230. [Google Scholar] [CrossRef]
- Oliveira, A.B.B.; de Araujo, C.C.; Del Antonio, T.T.; Folster, N.M.; Da Silva, J.K.M. Prevalence of Temporomandibular Disorder and Its Relation with Plantar Pressures in University Students of Health-Related Courses. Man. Ther. Posturology Rehabil. J. 2020, 17, 1–5. [Google Scholar] [CrossRef]
- Rocha, C.P.; Croci, C.S.; Caria, P.H.F. Is There Relationship between Temporomandibular Disorders and Head and Cervical Posture? A Systematic Review. J. Oral Rehabil. 2013, 40, 875–881. [Google Scholar] [CrossRef]
- Mínguez-Esteban, I.; De-la-Cueva-Reguera, M.; Romero-Morales, C.; Martínez-Pascual, B.; Navia, J.A.; Bravo-Aguilar, M.; Abuín-Porras, V. Physical Manifestations of Stress in Women. Correlations between Temporomandibular and Pelvic Floor Disorders. PLoS ONE 2024, 19, e0296652. [Google Scholar] [CrossRef]
- Wójcik, M.; Goździewicz, T.; Hudáková, Z.; Siatkowski, I. Endometriosis and the Temporomandibular Joint—Preliminary Observations. J. Clin. Med. 2023, 12, 2862. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, L.; Derisavifard, S.; Alaiev, D.; Funaro, M.; Levy, M.; Kreshover, J.; Moldwin, R.; Bahani, S. Pelvic Floor Myalgia and Temporomandibular Joint Dysfunction: A Common and Clinically Important Relationship. J. Urol. 2021, 206, e35–e36. [Google Scholar] [CrossRef]
- Kalamir, A.; Bonello, R.; Graham, P.; Vitiello, A.L.; Pollard, H. Intraoral Myofascial Therapy for Chronic Myogenous Temporomandibular Disorder: A Randomized Controlled Trial. J. Manip. Physiol. Ther. 2012, 35, 26–37. [Google Scholar] [CrossRef] [PubMed]
- DeVocht, J.W.; Long, C.R.; Zeitler, D.L.; Schaeffer, W. Chiropractic Treatment of Temporomandibular Disorders Using the Activator Adjusting Instrument: A Prospective Case Series. J. Manip. Physiol. Ther. 2003, 26, 421–425. [Google Scholar] [CrossRef]
- Gębska, M.; Dalewski, B.; Pałka, Ł.; Kołodziej, Ł. Evaluation of the Efficacy of Manual Soft Tissue Therapy and Therapeutic Exercises in Patients with Pain and Limited Mobility TMJ: A Randomized Control Trial (RCT). Head Face Med. 2023, 19, 42. [Google Scholar] [CrossRef]
- Kasper-Jędrzejewska, M.; Starzec-Proserpio, M.; Paprocka-Borowicz, M.; Kawka, S.; Halski, T.; Ptaszkowski, K. The Effects of One-time Soft Tissue Therapy on Pelvic Floor Muscle Electromyographic Signals in Women with Urinary Incontinence: A Randomized Intervention Trial. Neurourol. Urodyn. 2024, 43, 320–328. [Google Scholar] [CrossRef]
- Weiss, J.M. Pelvic Floor Myofascial Trigger Points: Manual Therapy for Interstitial Cystitis and the Urgency-Frequency Syndrome. J. Urol. 2001, 166, 2226–2231. [Google Scholar] [CrossRef] [PubMed]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.-P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network and Orofacial Pain Special Interest Group. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef]
- Available online: https://www.graphpad.com/quickcalcs/randomize1/ (accessed on 1 June 2023).
- Sherburn, M.; Murphy, C.A.; Carroll, S.; Allen, T.J.; Galea, M.P. Investigation of Transabdominal Real-Time Ultrasound to Visualise the Muscles of the Pelvic Floor. Aust. J. Physiother. 2005, 51, 167–170. [Google Scholar] [CrossRef]
- Halski, T.; Ptaszkowski, K.; Słupska, L.; Dymarek, R. The Evaluation of Bioelectrical Activity of Pelvic Floor Muscles Depending on Probe Location: A Pilot Study. Biomed. Res. Int. 2013, 2013, 238312. [Google Scholar] [CrossRef] [PubMed]
- Oleksy, Ł.; Mika, A.; Sulowska-Daszyk, I.; Rosłoniec, E.; Kielnar, R.; Stolarczyk, A. The Reliability of Pelvic Floor Muscle Bioelectrical Activity (SEMG) Assessment Using a Multi-Activity Measurement Protocol in Young Women. Int. J. Environ. Res. Public Health 2021, 18, 765. [Google Scholar] [CrossRef]
- Cohen, J. A Power Primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Błudnicka, M.; Piernicka, M.; Kortas, J.; Biernacka, B.D.; Szumilewicz, A. Effects of a One-Time Biofeedback EMG Session on Neuromuscular Activity of the Pelvic Floor Muscles in Pregnant Women. Neurophysiology 2020, 52, 438–445. [Google Scholar] [CrossRef]
- de Paula Gomes, C.A.F.; Politti, F.; Andrade, D.V.; de Sousa, D.F.M.; Herpich, C.M.; Dibai-Filho, A.V.; de Oliveira Gonzalez, T.; Biasotto-Gonzalez, D.A. Effects of Massage Therapy and Occlusal Splint Therapy on Mandibular Range of Motion in Individuals With Temporomandibular Disorder: A Randomized Clinical Trial. J. Manip. Physiol. Ther. 2014, 37, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Fischer, M.J.; Riedlinger, K.; Gutenbrunner, C.; Bernateck, M. Influence of the Temporomandibular Joint on Range of Motion of the Hip Joint in Patients With Complex Regional Pain Syndrome. J. Manip. Physiol. Ther. 2009, 32, 364–371. [Google Scholar] [CrossRef] [PubMed]
- Freynhagen, R.; Parada, H.A.; Calderon-Ospina, C.A.; Chen, J.; Rakhmawati Emril, D.; Fernández-Villacorta, F.J.; Franco, H.; Ho, K.-Y.; Lara-Solares, A.; Li, C.C.-F.; et al. Current Understanding of the Mixed Pain Concept: A Brief Narrative Review. Curr. Med. Res. Opin. 2019, 35, 1011–1018. [Google Scholar] [CrossRef]
- Aukee, P.; Penttinen, J.; Immonen, P.; Airaksinen, O. Intravaginal Surface EMG Probe Design Test for Urinary Incontinence Patients. Acupunct. Electro-Ther. Res. 2002, 27, 37–44. [Google Scholar] [CrossRef]
- Naess, I.; Bø, K. Can Maximal Voluntary Pelvic Floor Muscle Contraction Reduce Vaginal Resting Pressure and Resting EMG Activity? Int. Urogynecol. J. 2018, 29, 1623–1627. [Google Scholar] [CrossRef]
- Błudnicka, M.; Piernicka, M.; Kortas, J.; Bojar, D.; Duda-Biernacka, B.; Szumilewicz, A. The Influence of One-Time Biofeedback Electromyography Session on the Firing Order in the Pelvic Floor Muscle Contraction in Pregnant Woman–A Randomized Controlled Trial. Front. Hum. Neurosci. 2022, 16, 944792. [Google Scholar] [CrossRef]
- Chmielewska, D.; Stania, M.; Kucab–Klich, K.; Błaszczak, E.; Kwaśna, K.; Smykla, A.; Hudziak, D.; Dolibog, P. Electromyographic Characteristics of Pelvic Floor Muscles in Women with Stress Urinary Incontinence Following SEMG-Assisted Biofeedback Training and Pilates Exercises. PLoS ONE 2019, 14, e0225647. [Google Scholar] [CrossRef] [PubMed]
- Chmielewska, D.; Stania, M.; Smykla, A.; Kwaśna, K.; Błaszczak, E.; Sobota, G.; Skrzypulec-Plinta, V. Bioelectrical Activity of the Pelvic Floor Muscles after 6-Week Biofeedback Training in Nulliparous Continent Women. Acta Bioeng. Biomech. 2016, 18, 105–113. [Google Scholar] [PubMed]
- Swann, E.; Graner, S.J. Uses of Manual-Therapy Techniques in Pain Management. Athl. Ther. Today 2002, 7, 14–17. [Google Scholar] [CrossRef]
- Szumilewicz, A.; Dornowski, M.; Piernicka, M.; Worska, A.; Kuchta, A.; Kortas, J.; Błudnicka, M.; Radzimiński, Ł.; Jastrzębski, Z. High-Low Impact Exercise Program Including Pelvic Floor Muscle Exercises Improves Pelvic Floor Muscle Function in Healthy Pregnant Women—A Randomized Control Trial. Front. Physiol. 2019, 9, 1867. [Google Scholar] [CrossRef] [PubMed]
- Allison, G.T.; Fujiwara, T. The Relationship between EMG Median Frequency and Low Frequency Band Amplitude Changes at Different Levels of Muscle Capacity. Clin. Biomech. 2002, 17, 464–469. [Google Scholar] [CrossRef]
- Cifrek, M.; Medved, V.; Tonković, S.; Ostojić, S. Surface EMG Based Muscle Fatigue Evaluation in Biomechanics. Clin. Biomech. 2009, 24, 327–340. [Google Scholar] [CrossRef]
- Zając, B.; Sulowska-Daszyk, I.; Mika, A.; Stolarczyk, A.; Rosłoniec, E.; Królikowska, A.; Rzepko, M.; Oleksy, Ł. Reliability of Pelvic Floor Muscle Assessment with Transabdominal Ultrasound in Young Nulliparous Women. J. Clin. Med. 2021, 10, 3449. [Google Scholar] [CrossRef]
- Thompson, J.A.; O’Sullivan, P.B.; Briffa, K.; Neumann, P.; Court, S. Assessment of Pelvic Floor Movement Using Transabdominal and Transperineal Ultrasound. Int. Urogynecol. J. 2005, 16, 285–292. [Google Scholar] [CrossRef]
- Tosun, O.C.; Solmaz, U.; Ekin, A.; Tosun, G.; Gezer, C.; Ergenoglu, A.M.; Yeniel, A.O.; Mat, E.; Malkoc, M.; Askar, N. Assessment of the Effect of Pelvic Floor Exercises on Pelvic Floor Muscle Strength Using Ultrasonography in Patients with Urinary Incontinence: A Prospective Randomized Controlled Trial. J. Phys. Ther. Sci. 2016, 28, 360–365. [Google Scholar] [CrossRef]
- Hagovska, M.; Svihra, J.; Urdzik, P. Predictive Value of Pelvic Floor Muscle Morphometry Using 3D/4D Ultrasound in Relation to the Success of Pelvic Floor Muscle Training in Women with Stress Urinary Incontinence. Int. J. Environ. Res. Public Health 2022, 19, 14757. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Experimental Group (n = 25) Mean ± SD | Control Group (n = 22) Mean ± SD | |
|---|---|---|
| Age [years] | 23.84 ± 1.97 | 23.50 ± 2.22 |
| High [cm] | 166.16 ± 5.71 | 166.45 ± 6.49 |
| Body mass [kg] | 58.06 ± 6.78 | 59.85 ± 9.06 |
| BMI [kg/m2] | 21.05 ± 2.46 | 21.59 ± 2.98 |
| Measurement | Experimental Group (n = 25) Mean ± SD | p | ES a | Control Group (n = 22) Mean ± SD | p | ES a | p * | ES b | |
|---|---|---|---|---|---|---|---|---|---|
| Activation of the pelvic floor muscles [cm] | Before | 0.34 ± 0.23 | 0.059 | 0.621 | 0.45 ± 0.34 | 0.990 | 0.099 | 0.203 | 0.379 |
| After | 0.52 ± 0.34 | 0.49 ± 0.46 | 0.785 | −0.074 |
| Measurement | Experimental Group (n = 25) | p | ES a | Control Group (n = 22) | p | ES a | p * | ES b | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | %MVC | Mean ± SD | %MVC | ||||||||
| Average mean amplitude (µV) | Before | 7.27 ± 3.99 | 16.74 ± 9.33 | 0.912 | 0.017 | 6.88 ± 3.94 | 15.49 ± 11.16 | 0.002 | −0.756 | 0.752 | −0.098 |
| After | 7.35 ± 5.29 | 14.78 ± 7.59 | 4.30 ± 2.79 | 10.26 ± 7.94 | 0.014 | −0.721 | |||||
| Measurement | Experimental Group (n = 25) | p | ES a | Control Group (n = 22) | p | ES a | p * | ES b | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | %MVC | Mean ± SD | %MVC | ||||||||
| Average peak amplitude (µV) | Before | 46.11 ± 28.83 | 84.45± 7.82 | 0.555 | −0.072 | 50.27 ± 36.88 | 83.87 ± 9.63 | 0.270 | −0.118 | 0.661 | 0.126 |
| After | 44.01 ± 29.48 | 72.34 ± 21.54 | 46.07 ± 34.04 | 78.10 ± 15.87 | 0.828 | 0.065 | |||||
| Time before peak (s) | Before | 31.98 ± 12.02 | - | 0.130 | 0.315 | 32.93 ± 12.49 | - | 0.759 | −0.071 | 0.813 | 0.078 |
| After | 36.43 ± 15.99 | - | 31.99 ± 13.83 | - | 0.271 | −0.297 | |||||
| Average resting tension between phasic contractions (µV) | Before | 8.39 ± 5.20 | 17.31 ± 8.88 | 0.005 | −0.430 | 6.43 ± 4.34 | 20.09 ± 17.60 | 0.136 | −0.333 | 0.125 | 0.409 |
| After | 6.27 ± 4.64 | 13.13 ± 9.07 | 5.26 ± 2.43 | 10.66 ± 6.91 | 0.426 | −0.273 | |||||
| Measurement | Experimental Group (n = 25) | p | ES a | Control Group (n = 22) | p | ES a | p * | ES b | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | %MVC | Mean ± SD | %MVC | ||||||||
| Average mean amplitude (µV) | Before | 21.86 ± 15.50 | 41.01 ± 11.81 | 0.756 | 0.036 | 23.28 ± 18.77 | 38.01 ± 14.61 | 0.834 | 0.020 | 0.784 | 0.082 |
| After | 22.42 ± 15.81 | 38.19 ± 16.35 | 23.68 ± 20.42 | 37.31 ± 16.69 | 0.807 | 0.069 | |||||
| Time before peak (s) | Before | 35.02 ± 19.14 | - | 0.375 | −0.222 | 37.67 ± 18.41 | - | 0.522 | −0.189 | 0.619 | 0.141 |
| After | 30.80 ± 18.86 | - | 34.43 ± 15.81 | - | 0.497 | 0.209 | |||||
| Average resting tension between tonic contractions (µV) | Before | 9.64 ± 6.11 | 19.28 ± 9.66 | 0.171 | −0.213 | 9.37 ± 6.26 | 22.34 ± 14.53 | 0.051 | −0.318 | 0.869 | −0.044 |
| After | 8.49 ± 4.59 | 17.10 ± 8.01 | 7.61 ± 4.70 | 15.45 ± 8.61 | 0.583 | −0.189 | |||||
| Measurement | Experimental Group (n = 25) | p | ES a | Control Group (n = 22) | p | ES a | p * | ES b | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | %MVC | Mean ± SD | %MVC | ||||||||
| Average mean amplitude (µV) | Before | 16.68 ± 11.32 | 33.52 ± 17.29 | 0.197 | 0.211 | 17.13 ± 14.62 | 31.50 ± 16.44 | 0.405 | −0.165 | 0.910 | 0.034 |
| After | 19.69 ± 16.70 | 31.05 ± 14.27 | 15.07 ± 9.89 | 27.99 ± 12.83 | 0.245 | −0.337 | |||||
| Median frequency (Hz) | Before | 61.24 ± 18.08 | - | 0.959 | 0.011 | 67.27 ± 25.09 | - | 0.507 | 0.129 | 0.393 | 0.276 |
| After | 61.48 ± 25.81 | - | 70.60 ± 26.53 | - | 0.198 | 0.348 | |||||
| Mean frequency (Hz) | Before | 80.95 ± 23.57 | - | 0.959 | −0.009 | 89.88 ± 33.56 | - | 0.235 | 0.167 | 0.330 | 0.308 |
| After | 80.71 ± 27.53 | - | 95.95 ± 38.86 | - | 0.098 | 0.453 | |||||
| F ratio | Before | 17.75 ± 2.96 | - | 0.424 | −0.257 | 16.28 ± 1.90 | - | 0.898 | −0.101 | 0.083 | 0.591 |
| After | 16.92 ± 3.48 | - | 16.05 ± 2.61 | - | 0.194 | 0.283 | |||||
| Measurement | Experimental Group (n = 25) | p | ES a | Control Group (n = 22) | p | ES a | p * | ES b | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | %MVC | Mean ± SD | %MVC | ||||||||
| Average mean amplitude (µV) | Before | 6.66 ± 4.16 | 15.01± 9.55 | 0.028 | −0.276 | 5.84 ± 3.72 | 16.25 ± 14.68 | 0.128 | −0.247 | 0.461 | −0.208 |
| After | 5.52 ± 4.11 | 12.31 ± 7.74 | 5.01 ± 2.96 | 11.56 ± 9.25 | 0.645 | −0.142 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sulowska-Daszyk, I.; Gamrot, S.; Handzlik-Waszkiewicz, P. A Single Session of Temporomandibular Joint Soft Tissue Therapy and Its Effect on Pelvic Floor Muscles Activity in Women—A Randomized Controlled Trial. J. Clin. Med. 2024, 13, 7037. https://doi.org/10.3390/jcm13237037
Sulowska-Daszyk I, Gamrot S, Handzlik-Waszkiewicz P. A Single Session of Temporomandibular Joint Soft Tissue Therapy and Its Effect on Pelvic Floor Muscles Activity in Women—A Randomized Controlled Trial. Journal of Clinical Medicine. 2024; 13(23):7037. https://doi.org/10.3390/jcm13237037
Chicago/Turabian StyleSulowska-Daszyk, Iwona, Sara Gamrot, and Paulina Handzlik-Waszkiewicz. 2024. "A Single Session of Temporomandibular Joint Soft Tissue Therapy and Its Effect on Pelvic Floor Muscles Activity in Women—A Randomized Controlled Trial" Journal of Clinical Medicine 13, no. 23: 7037. https://doi.org/10.3390/jcm13237037
APA StyleSulowska-Daszyk, I., Gamrot, S., & Handzlik-Waszkiewicz, P. (2024). A Single Session of Temporomandibular Joint Soft Tissue Therapy and Its Effect on Pelvic Floor Muscles Activity in Women—A Randomized Controlled Trial. Journal of Clinical Medicine, 13(23), 7037. https://doi.org/10.3390/jcm13237037