
Pilates Method and/or Photobiomodulation Therapy Combined to Static Magnetic Field in Women with Stress Urinary Incontinence: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics
2.2. Volunteers and Recruitment
2.3. Inclusion Criteria
2.4. Exclusion Criteria
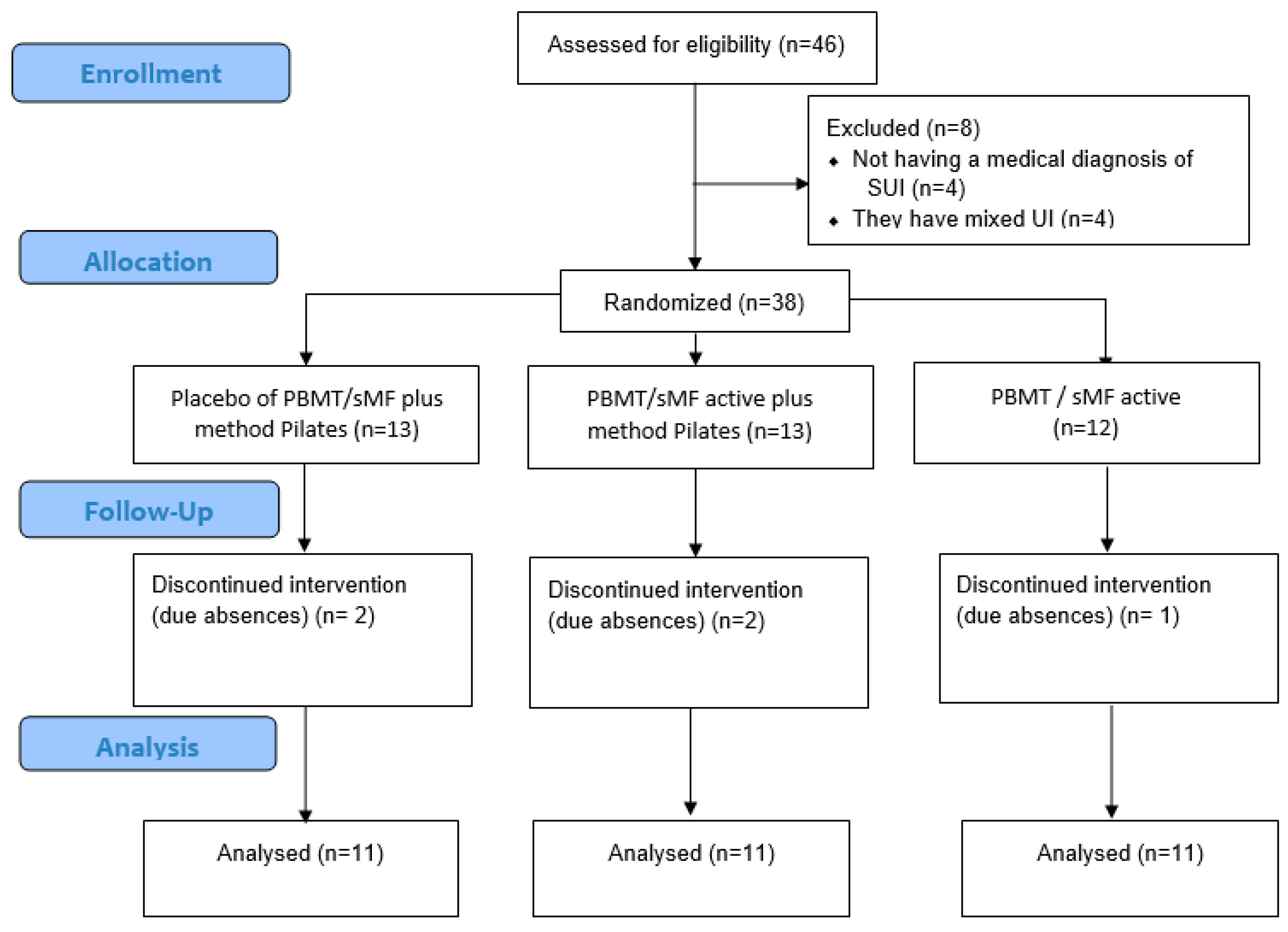
2.5. Composition of Groups and Randomization Process
- (1)
- placebo of PBMT/sMF plus method Pilates (PPG);
- (2)
- PBMT/sMF active plus method Pilates (PPActG);
- (3)
- and only PBMT/sMF active (PG).
2.6. Experimental Protocol
2.6.1. Evaluations and Informative Procedures
2.6.2. Personal Data and Anamnesis
2.7. Outcomes
2.7.1. Muscle Strength
2.7.2. Muscle Tone
2.7.3. International Consultation on Incontinence Questionnaire
2.7.4. Urinary Loss
2.8. Interventions
2.8.1. Photobiomodulation Therapy Combined to Static Magnetic Field (PBM/sMF)
2.8.2. Pilates Exercise Program
2.8.3. Characterisation of Sample
2.8.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Milsom, I.; Gyhagen, M. The prevalence of urinary incontinence. Climacteric 2019, 22, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Lukacz, E.S.; Santiago-Lastra, Y.; Albo, M.E.; Brubaker, L. Urinary Incontinence in Women: A Review. JAMA 2017, 318, 1592–1604. [Google Scholar] [CrossRef] [PubMed]
- Behnia-Willison, F.; Nguyen, T.T.T.; Mohamadi, B.; Vancaillie, T.G.; Lam, A.; Willison, N.N.; Zivkovic, J.; Woodman, R.J.; Skubisz, M.M. Fractional CO2 laser for treatment of stress urinary incontinence. Eur. J. Obstet. Gynecol. Reprod. Biol. X 2019, 1, 100004. [Google Scholar] [CrossRef]
- Duralde, E.R.; Rowen, T.S. Urinary Incontinence and Associated Female Sexual Dysfunction. Sex. Med. Rev. 2017, 5, 470–485. [Google Scholar] [CrossRef]
- Felde, G.; Engeland, A.; Hunskaar, S. Urinary incontinence associated with anxiety and depression: The impact of psychotropic drugs in a cross-sectional study from the Norwegian HUNT study. BMC Psychiatry 2020, 20, 521. [Google Scholar] [CrossRef]
- Wilson, L.; Brown, J.S.; Shin, G.P.; Luc, K.O.; Subak, L.L. Annual direct cost of urinary incontinence. Obstet. Gynecol. 2001, 98, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Nambiar, A.K.; Bosch, R.; Cruz, F.; Lemack, G.E.; Thiruchelvam, N.; Tubaro, A.; Bedretdinova, D.A.; Ambühl, D.; Farag, F.; Lombardo, R.; et al. EAU Guidelines on Assessment and Nonsurgical Management of Urinary Incontinence. Eur. Urol. 2018, 73, 596–609. [Google Scholar] [CrossRef]
- Kegel, A.H. Progressive resistance exercise in the functional restoration of the perineal muscles. Am. J. Obstet. Gynecol. 1948, 56, 238–249. [Google Scholar] [CrossRef]
- Dumoulin, C.; Cacciari, L.P.; Hay-Smith, E.J.C. Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database Syst. Rev. 2018, 10, CD005654. [Google Scholar] [CrossRef]
- García-Sánchez, E.; Ávila-Gandía, V.; López-Román, J.; Martínez-Rodríguez, A.; Rubio-Arias, J.Á. What Pelvic Floor Muscle Training Load is Optimal in Minimizing Urine Loss in Women with Stress Urinary Incontinence? A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 4358. [Google Scholar] [CrossRef]
- Bø, K. Urinary incontinence, pelvic floor dysfunction, exercise and sport. Sport. Med. 2004, 34, 451–464. [Google Scholar] [CrossRef]
- Torelli, L.; de Jarmy Di Bella, Z.I.; Rodrigues, C.A.; Stüpp, L.; Girão, M.J.; Sartori, M.G. Effectiveness of adding voluntary pelvic floor muscle contraction to a Pilates exercise program: An assessor-masked randomized controlled trial. Int. Urogynecol. J. 2016, 27, 1743–1752. [Google Scholar] [CrossRef]
- Kloubec, J. Pilates: How does it work and who needs it? Muscles Ligaments Tendons J. 2011, 1, 61–66. [Google Scholar] [PubMed]
- Chmielewska, D.; Stania, M.; Kucab-Klich, K.; Błaszczak, E.; Kwaśna, K.; Smykla, A.; Hudziak, D.; Dolibog, P. Electromyographic characteristics of pelvic floor muscles in women with stress urinary incontinence following sEMG-assisted biofeedback training and Pilates exercises. PLoS ONE 2019, 14, e0225647. [Google Scholar] [CrossRef] [PubMed]
- Culligan, P.J.; Scherer, J.; Dyer, K.; Priestley, J.; Guingon-White, G.; DelVecchio, D.; Vangeli, M. A randomized clinical trial comparing pelvic floor muscle training to a Pilates exercise program for improving pelvic muscle strength. Int. Urogynecol. J. 2010, 21, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Bø, K.; Herbert, R.D. There is not yet strong evidence that exercise regimens other than pelvic floor muscle training can reduce stress urinary incontinence in women: A systematic review. J. Physiother. 2013, 59, 159–168. [Google Scholar] [CrossRef]
- De Marchi, T.; Ferlito, J.V.; Ferlito, M.V.; Salvador, M.; Leal-Junior, E.C.P. Can Photobiomodulation Therapy (PBMT) Minimize Exercise-Induced Oxidative Stress? A Systematic Review and Meta-Analysis. Antioxidants 2022, 11, 1671. [Google Scholar] [CrossRef]
- De Marchi, T.; Schmitt, V.M.; Danúbia da Silva Fabro, C.; da Silva, L.L.; Sene, J.; Tairova, O.; Salvador, M. Phototherapy for Improvement of Performance and Exercise Recovery: Comparison of 3 Commercially Available Devices. J. Athl. Train. 2017, 52, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Miranda, E.F.; Tomazoni, S.S.; de Paiva, P.R.V.; Pinto, H.D.; Smith, D.; Santos, L.A.; Carvalho, P.D.T.C.D.; Leal-Junior, E.C.P. When is the best moment to apply photobiomodulation therapy (PBMT) when associated to a treadmill endurance-training program? A randomized, triple-blinded, placebo-controlled clinical trial. Lasers Med. Sci. 2018, 33, 719–727. [Google Scholar] [CrossRef]
- De Marchi, T.; Leal-Junior, E.C.P.; Lando, K.C.; Cimadon, F.; Vanin, A.A.; da Rosa, D.P.; Salvador, M. Photobiomodulation therapy before futsal matches improves the staying time of athletes in the court and accelerates post-exercise recovery. Lasers Med. Sci. 2019, 34, 139–148. [Google Scholar] [CrossRef] [PubMed]
- De Marchi, T.; Leal Junior, E.C.; Bortoli, C.; Tomazoni, S.S.; Lopes-Martins, R.A.; Salvador, M. Low-level laser therapy (LLLT) in human progressive-intensity running: Effects on exercise performance, skeletal muscle status, and oxidative stress. Lasers Med. Sci. 2012, 27, 231–236. [Google Scholar] [CrossRef]
- de Freitas, L.F.; Hamblin, M.R. Proposed Mechanisms of Photobiomodulation or Low-Level Light Therapy. IEEE J. Sel. Top. Quantum Electron. 2016, 22, 7000417. [Google Scholar] [CrossRef] [PubMed]
- Ferlito, J.V.; Ferlito, M.V.; Leal-Junior, E.C.P.; Tomazoni, S.S.; De Marchi, T. Comparison between cryotherapy and photobiomodulation in muscle recovery: A systematic review and meta-analysis. Lasers Med. Sci. 2022, 37, 1375–1388. [Google Scholar] [CrossRef] [PubMed]
- Leitner, M.; Moser, H.; Eichelberger, P.; Kuhn, A.; Radlinger, L. Pelvic floor muscle activity during fast voluntary contractions in continent and incontinent women. Neurourol. Urodyn. 2019, 38, 625–631. [Google Scholar] [CrossRef]
- Vieira, K.V.S.G.; Ciol, M.A.; Azevedo, P.H.; Pinfildi, C.E.; Renno, A.C.; Colantonio, E.; Tucci, H. Effects of Light-Emitting Diode Therapy on the Performance of Biceps Brachii Muscle of Young Healthy Males After 8 Weeks of Strength Training: A Randomized Controlled Clinical Trial. J. Strength Cond. Res. 2019, 33, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Vanin, A.A.; Miranda, E.F.; Machado, C.S.M.; de Paiva, P.R.V.; Albuquerque-Pontes, G.M.; Casalechi, H.L.; Carvalho, P.D.T.C.D.; Leal-Junior, E.C.P. What is the best moment to apply phototherapy when associated to a strength training program? A randomized, double-blinded, placebo-controlled trial: Phototherapy in association to strength training [published correction appears in Lasers Med. Sci. 2017, 32, 253]. Lasers Med. Sci. 2016, 31, 1555–1564. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D.; on behalf of the CONSORT group. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. Int. J. Surg. 2011, 9, 672–677. [Google Scholar] [CrossRef]
- Messelink, B.; Benson, T.; Berghmans, B.; Bø, K.; Corcos, J.; Fowler, C.; Laycock, J.; Lim, P.H.-C.; van Lunsen, R.; Nijeholt, G.L.Á.; et al. Standardization of terminology of pelvic floor muscle function and dysfunction: Report from the pelvic floor clinical assessment group of the International Continence Society. Neurourol. Urodyn. 2005, 24, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Chevalier, F.; Fernandez-Lao, C.; Cuesta-Vargas, A.I. Normal reference values of strength in pelvic floor muscle of women: A descriptive and inferential study. BMC Womens Health 2014, 14, 143. [Google Scholar] [CrossRef]
- Da Roza, T.; Mascarenhas, T.; Araujo, M.; Trindade, V.; Jorge, R.N. Oxford Grading Scale vs manometer for assessment of pelvic floor strength in nulliparous sports students. Physiotherapy 2013, 99, 207–211. [Google Scholar] [CrossRef]
- Dietz, H.P.; Shek, K.L. The quantification of levator muscle resting tone by digital assessment. Int. Urogynecol. J. Pelvic. Floor Dysfunct. 2008, 19, 1489–1493. [Google Scholar] [CrossRef]
- Bo, K.; Frawley, H.C.; Haylen, B.T.; Abramov, Y.; Almeida, F.G.; Berghmans, B.; Bortolini, M.; Dumoulin, C.; Gomes, M.; McClurg, D.; et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for the conservative and nonpharmacological management of female pelvic floor dysfunction. Neurourol. Urodyn. 2017, 36, 221–244. [Google Scholar] [CrossRef] [PubMed]
- Avery, K.; Donovan, J.; Peters, T.J.; Shaw, C.; Gotoh, M.; Abrams, P. ICIQ: A brief and robust measure for evaluating the symptoms and impact of urinary incontinence. Neurourol. Urodyn. 2004, 23, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Krhut, J.; Zachoval, R.; Smith, P.P.; Rosier, P.F.; Valanský, L.; Martan, A.; Zvara, P. Pad weight testing in the evaluation of urinary incontinence. Neurourol. Urodyn. 2014, 33, 507–510. [Google Scholar] [CrossRef]
- Ferreira, C.H.; Bø, K. The Pad Test for urinary incontinence in women. J. Physiother. 2015, 61, 98. [Google Scholar] [CrossRef]
- Ellsworth, A. Pilates Anatomy: A comprehensive Guide. Thunder Bay Press: San Diego, CA, USA, 2013; p. 160. [Google Scholar]
- Impact of global postural reeducation for treatment of female stress urinary incontinence. Rev. Assoc. Med. Bras. 2008, 54, 17–22. [CrossRef]
- Lemos, A.Q.; Brasil, C.A.; Valverde, D.; Ferreira, J.D.S.; Lordêlo, P.; Sá, K.N. The pilates method in the function of pelvic floor muscles: Systematic review and meta-analysis. J. Bodyw. Mov. Ther. 2019, 23, 270–277. [Google Scholar] [CrossRef]
- Ferla, L.; Paiva, L.L.; Darki, C.; Vieira, A. Comparison of the functionality of pelvic floor muscles in women who practice the Pilates method and sedentary women: A pilot study. Int. Urogynecol. J. 2016, 27, 123–128. [Google Scholar] [CrossRef]
- Kang, G.; Lee, H.; Shin, M.; Kim, J.; Lee, S.; Park, Y. The Efficacy of Pilates on Urinary Incontinence in Korean Women: A Metabolomics Approach. Metabolites 2021, 11, 118. [Google Scholar] [CrossRef]
- Pedriali, F.R.; Gomes, C.S.; Soares, L.; Urbano, M.R.; Moreira, E.C.; Averbeck, M.A.; de Almeida, S.H. Is pilates as effective as conventional pelvic floor muscle exercises in the conservative treatment of post-prostatectomy urinary incontinence? A randomised controlled trial. Neurourol. Urodyn. 2016, 35, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Bø, K. Pelvic floor muscle strength and response to pelvic floor muscle training for stress urinary incontinence. Neurourol. Urodyn. 2003, 22, 654–658. [Google Scholar] [CrossRef] [PubMed]
- Nakano, J.; Kataoka, H.; Sakamoto, J.; Origuchi, T.; Okita, M.; Yoshimura, T. Low-level laser irradiation promotes the recovery of atrophied gastrocnemius skeletal muscle in rats. Exp. Physiol. 2009, 94, 1005–1015. [Google Scholar] [CrossRef]
- Coletti, D.; Teodori, L.; Albertini, M.C.; Rocchi, M.; Pristerà, A.; Fini, M.; Molinaro, M.; Adamo, S. Static magnetic fields enhance skeletal muscle differentiation in vitro by improving myoblast alignment. Cytom. A 2007, 71, 846–856. [Google Scholar] [CrossRef] [PubMed]
- Tomazoni, S.S.; Machado, C.D.S.M.; De Marchi, T.; Casalechi, H.L.; Bjordal, J.M.; de Carvalho, P.T.C.; Leal-Junior, E.C.P. Infrared Low-Level Laser Therapy (Photobiomodulation Therapy) before Intense Progressive Running Test of High-Level Soccer Players: Effects on Functional, Muscle Damage, Inflammatory, and Oxidative Stress Markers-A Randomized Controlled Trial. Oxid. Med. Cell Longev. 2019, 2019, 6239058. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.X.; Rudnicki, M.A. Satellite cells, the engines of muscle repair. Nat. Rev. Mol. Cell Biol. 2011, 13, 127–133. [Google Scholar] [CrossRef]
- De Marchi, T.; Frâncio, F.; Ferlito, J.V.; Weigert, R.; de Oliveira, C.; Merlo, A.P.; Pandini, D.L.; Pasqual-Júnior, B.A.; Giovanella, D.; Tomazoni, S.S.; et al. Effects of Photobiomodulation Therapy Combined with Static Magnetic Field in Severe COVID-19 Patients Requiring Intubation: A Pragmatic Randomized Placebo-Controlled Trial. J. Inflamm. Res. 2021, 14, 3569–3585. [Google Scholar] [CrossRef]
- Kou, Y.T.; Liu, H.T.; Hou, C.Y.; Lin, C.Y.; Tsai, C.M.; Chang, H. A transient protective effect of low-level laser irradiation against disuse-induced atrophy of rats. Lasers Med. Sci. 2019, 34, 1829–1839. [Google Scholar] [CrossRef] [PubMed]
- Bień, A.; Rzońca, E.; Iwanowicz-Palus, G.; Pańczyk-Szeptuch, M. The influence of climacteric symptoms on women’s lives and activities. Int. J. Environ. Res. Public Health 2015, 12, 3835–3846. [Google Scholar] [CrossRef] [PubMed]
- Johnston, S.L. Pelvic floor dysfunction in midlife women. Climacteric 2019, 22, 270–276. [Google Scholar] [CrossRef]
- Aoki, Y.; Brown, H.W.; Brubaker, L.; Cornu, J.N.; Daly, J.O.; Cartwright, R. Urinary incontinence in women. Nat. Rev. Dis. Prim. 2017, 3, 17042. [Google Scholar] [CrossRef]
- de Mattos Lourenco, T.R.; Matsuoka, P.K.; Baracat, E.C.; Haddad, J.M. Urinary incontinence in female athletes: A systematic review. Int. Urogynecol. J. 2018, 29, 1757–1763. [Google Scholar] [CrossRef] [PubMed]
- Machado, L.D.S.; Marques Cerentini, T.; Laganà, A.S.; Viana da Rosa, P.; Fichera, M.; Telles da Rosa, L.H. Pelvic floor evaluation in CrossFit® athletes and urinary incontinence: A cross-sectional observational study. Women Health 2021, 61, 490–499. [Google Scholar] [CrossRef] [PubMed]
- Pires, T.F.; Pires, P.M.; Moreira, M.H.; Gabriel, R.E.C.D.; João, P.V.; Viana, S.A.; Viana, R.A. Pelvic Floor Muscle Training in Female Athletes: A Randomized Controlled Pilot Study. Int. J. Sports Med. 2020, 41, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Volløyhaug, I.; Mørkved, S.; Salvesen, Ø.; Salvesen, K.Å. Assessment of pelvic floor muscle contraction with palpation, perineometry and transperineal ultrasound: A cross-sectional study. Ultrasound Obstet. Gynecol. 2016, 47, 768–773. [Google Scholar] [CrossRef]
- Falah-Hassani, K.; Reeves, J.; Shiri, R.; Hickling, D.; McLean, L. The pathophysiology of stress urinary incontinence: A systematic review and meta-analysis. Int. Urogynecol. J. 2021, 32, 501–552. [Google Scholar] [CrossRef]
- Zhang, X.; Chen, Z.; Song, X.; Yuan, X.; Cai, D.; Chen, J.; Li, L.; Du, G.; Yang, W.; Ye, Z. Application of perineal ultrasound measurement and urodynamic study in the diagnosis and typing of stress urinary incontinence ultrasound and urodynamic study. Urologia 2013, 80, 233–238. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Class | 1M |
|---|---|
| Number of lasers | 1 Super-pulsed infrared |
| Wavelength (nm) | 905 (±1) |
| Frequency (Hz) | 250 |
| Peak power (W) | 50 |
| Average mean optical output (mW) | 1.25 |
| Power density (mW/cm2) | 2.84 |
| Energy density (J/cm2) | 0.085 |
| Dose (J) | 0.0375 |
| Spot size of laser (cm2) | 0.44 |
| Number of red LEDs | 3 Red |
| Wavelength of red LEDs (nm) | 640 (±10) |
| Frequency (Hz) | 2 |
| Average optical output (mW)—each | 66.67 |
| Power density (mW/cm2)—each | 74.08 |
| Energy density (J/cm2)—each | 2.22 |
| Dose (J)—each | 2.00 |
| Spot size of red LED (cm2)—each | 0.9 |
| Number of infrared LEDs | 3 Infrared |
| Wavelength of infrared LEDs (nm) | 875 (±10) |
| Frequency (Hz) | 16 |
| Average optical output (mW)—each | 83.33 |
| Power density (mW/cm2)—each | 92.59 |
| Energy density (J/cm2)—each | 2.77 |
| Dose (J)—each | 2.50 |
| Spot Size of LED (cm2)—each | 0.9 |
| Magnetic Field (mT) | 35 |
| Irradiation time per site (sec) | 60 |
| Total energy irradiated per site (J) | 13.5375 |
| Number of sites irradiated per treatment | 4 |
| Total energy irradiated per treatment (J) | 54.15 |
| Aperture of the device (cm2) | 4 |
| Application mode | Cluster probe held stationary in skin contact with a 90-degree angle and slight pressure |
| 1 to 8° Session | 9 to 16° Session | 17 to 24° Session | |
|---|---|---|---|
| Warming | 20 Breaths(inhale/exhale/center/contract) | 20 Breaths (inhale/exhale/center/contract) | 20 Breaths (inhale/exhale/center/contract) |
| StrengtheningThe rest between exercises was 5 breaths | Double leg stretch, single leg stretch, leg circles, hip raise on Swiss ball, Swiss ball pull-in, bird dog zipper, side flex (lateral flexion), side kick-front and back, side kick up and down, clamshell (6 x each exercise) | The swan, swan dive, book close series, ball hip raise, Swiss ball knee tuck, bird dog zipper, side flex (lateral flexion), side kick-front and back, side kick up and down, clamshell (6 x each exercise) | Leg pull back, rolling like a ball, swimming, roll over, leg pull front, bird dog zipper, side flex (lateral flexion), side kick-front and back, side kick up and down, clamshell(6 x each exercise) |
| Stretching | Swan, Neck Pull (one minute in each position) | Swan, Neck Pull (One minute in each position) | Swan, Neck Pull(One minute in each position) |
| Group 1 (n = 11) | Group 2 (n = 11) | Group 3 (n = 11) | |
|---|---|---|---|
| Age (years) | 45 ± 9.56 | 44.81 ± 10.77 | 51.19 ± 8.85 |
| Weight (kg) | 75 ± 12,31 | 74 ± 14. 49 | 74.5 ± 15.26 |
| Height (meters) | 1.63 ± 0.07 | 1.62 ± 0.04 | 1.61 ± 0.06 |
| BMI (kg/m2) | 28.75 ± 3.57 | 28.12 ± 5.19 | 28.76 ± 5.79 |
| Time of signs and symptoms of SUI (month) | |||
| <6 | - | - | - |
| <12 | - | - | 1/11 |
| >12 to 48 | 5/11 | 6/11 | 3/11 |
| >48 | 6/11 | 5/11 | 7/11 |
| Gestation (n) | 1.9 ± 1.04 | 1.6 ± 1.27 | 1.8 ± 0.98 |
| Menopause | |||
| Age (years) | 49 ± 4.28 | 51.3 ± 1.52 | 50.25 ± 1.26 |
| N/ total sample | 4/11 | 3/11 | 6/11 |
| Surgery (N/N total sample) | |||
| Hysterectomy | 1/11 | 2/11 | 1/11 |
| Colpoperineoplasty | - | - | 1/11 |
| Comorbidities (N/N total sample) | |||
| Diabetes | 1/11 | - | 2/11 |
| Systemic Arterial Hypertension | 1/11 | 1/11 | 1/11 |
| Thyroid Pathology | 1/11 | 1/11 | 2/11 |
| Depression | 2/11 | - | - |
| Group | Pre | Post 4 Weeks | Post 8 Weeks | Post 12 Weeks |
|---|---|---|---|---|
| PPG | 1.25 ± 0.63 | 0.66 ± 0.40 * | 0.46 ± 0.48 * | 0.31 ± 0.83 * |
| PPActG | 1.47 ± 0.78 | 0.88 ± 0.42 * | 0.64 ± 0.43 *,# | 0.40 ± 0.27 *,#,$ |
| PG | 1.34 ± 0.60 | 0.57 ± 0.48 * | 0.48 ± 0.58 * | 0.33 ± 0.33 * |
| Group | Variables | Time of Collection | Percentage of ChangeCompared to Pre | Cohen-d | Effect Rating |
| PPG | Strength | Post | 45.00 | 1.09 | Large |
| ICIQ | Post | −37.76 | 1.17 | Large | |
| Tonus | Post | 30.43 | 0.74 | Moderate | |
| Lost Urinary | Post 4 weeks | −47.25 | 1.14 | Large | |
| Post 8 weeks | −120.05 | 1.31 | Large | ||
| Post 12 weeks | −204.94 | 1.27 | Large | ||
| PPactG | Strength | Post | 73.33 | 1.02 | Large |
| ICIQ | Post | −24.50 | 0.96 | Large | |
| Tonus | Post | 18.18 | 0.40 | Small | |
| Lost Urinary | Post 4 weeks | −40.16 | 0.94 | Large | |
| Post 8 weeks | −94.60 | 1.32 | Large | ||
| Post 12 weeks | −167.82 | 1.83 | Large | ||
| PG | Strength | Post | 50.00 | 0.84 | Large |
| ICIQ | Post | −32.84 | 1.42 | Large | |
| Tonus | Post | 37.04 | 1.12 | Large | |
| Lost Urinary | Post 4 weeks | −57.69 | 1.39 | Large | |
| Post 8 weeks | −152.53 | 1.44 | Large | ||
| Post 12 weeks | −212.25 | 2.09 | Large |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Marchi, T.; Ferlito, J.V.; Turra, A.C.; Flamia, S.; de Bispo Magro, F.; Pavelecini Donida, M.L.; Dilkin, M.; da Silva, D.; Massia Ribas, V.; Leal Junior, E.C.P. Pilates Method and/or Photobiomodulation Therapy Combined to Static Magnetic Field in Women with Stress Urinary Incontinence: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. J. Clin. Med. 2023, 12, 1104. https://doi.org/10.3390/jcm12031104
De Marchi T, Ferlito JV, Turra AC, Flamia S, de Bispo Magro F, Pavelecini Donida ML, Dilkin M, da Silva D, Massia Ribas V, Leal Junior ECP. Pilates Method and/or Photobiomodulation Therapy Combined to Static Magnetic Field in Women with Stress Urinary Incontinence: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Journal of Clinical Medicine. 2023; 12(3):1104. https://doi.org/10.3390/jcm12031104
Chicago/Turabian StyleDe Marchi, Thiago, João Vitor Ferlito, Ariane Cristina Turra, Sheila Flamia, Franciele de Bispo Magro, Maribel Luiza Pavelecini Donida, Michele Dilkin, Djéssica da Silva, Vanessa Massia Ribas, and Ernesto Cesar Pinto Leal Junior. 2023. "Pilates Method and/or Photobiomodulation Therapy Combined to Static Magnetic Field in Women with Stress Urinary Incontinence: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial" Journal of Clinical Medicine 12, no. 3: 1104. https://doi.org/10.3390/jcm12031104
APA StyleDe Marchi, T., Ferlito, J. V., Turra, A. C., Flamia, S., de Bispo Magro, F., Pavelecini Donida, M. L., Dilkin, M., da Silva, D., Massia Ribas, V., & Leal Junior, E. C. P. (2023). Pilates Method and/or Photobiomodulation Therapy Combined to Static Magnetic Field in Women with Stress Urinary Incontinence: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Journal of Clinical Medicine, 12(3), 1104. https://doi.org/10.3390/jcm12031104