The Effectiveness of a Multimodal Brain Empowerment Program in Mild Cognitive Impairment: A Single-Blind, Quasi-Randomized Experimental Study


_H._You.png)
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
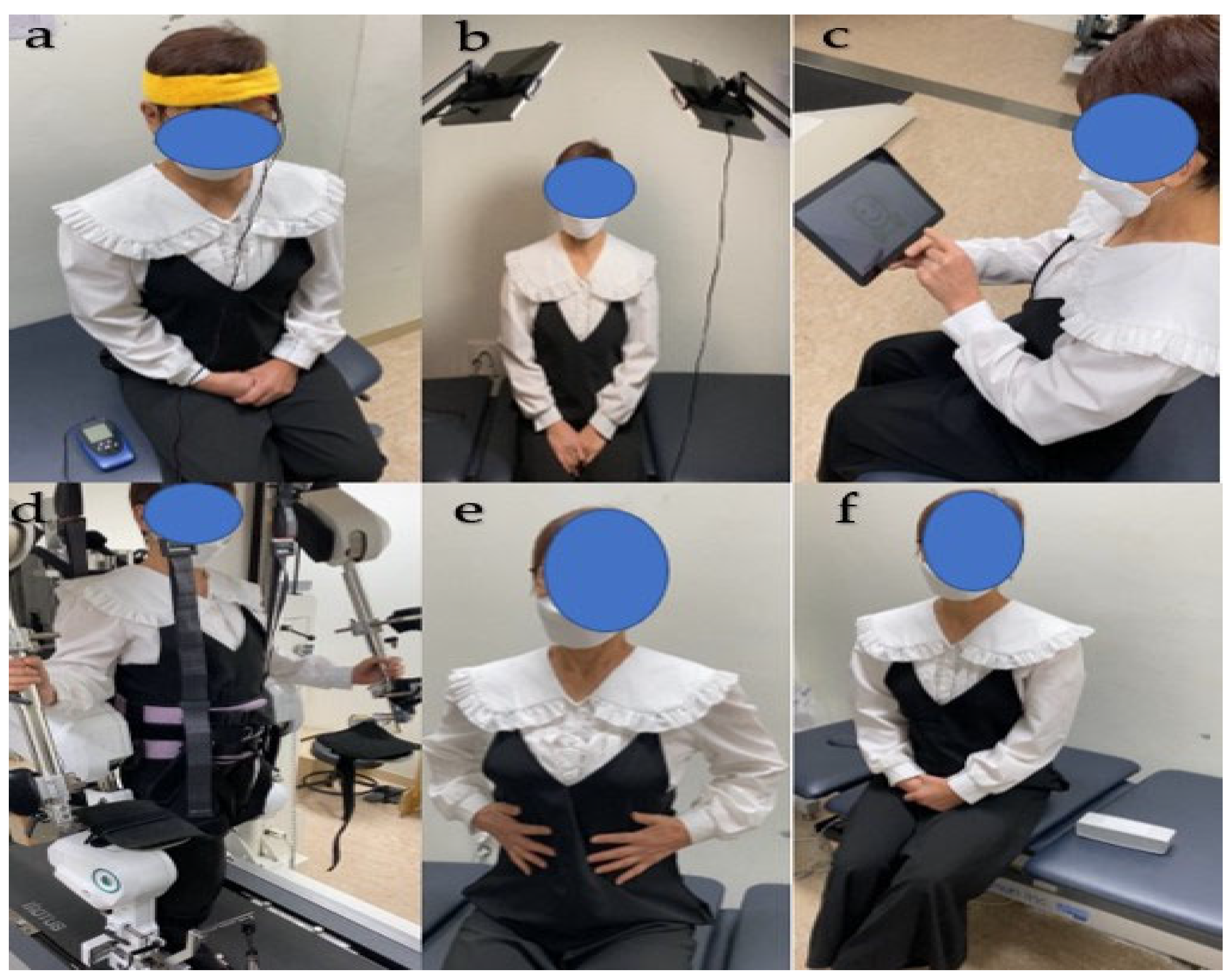
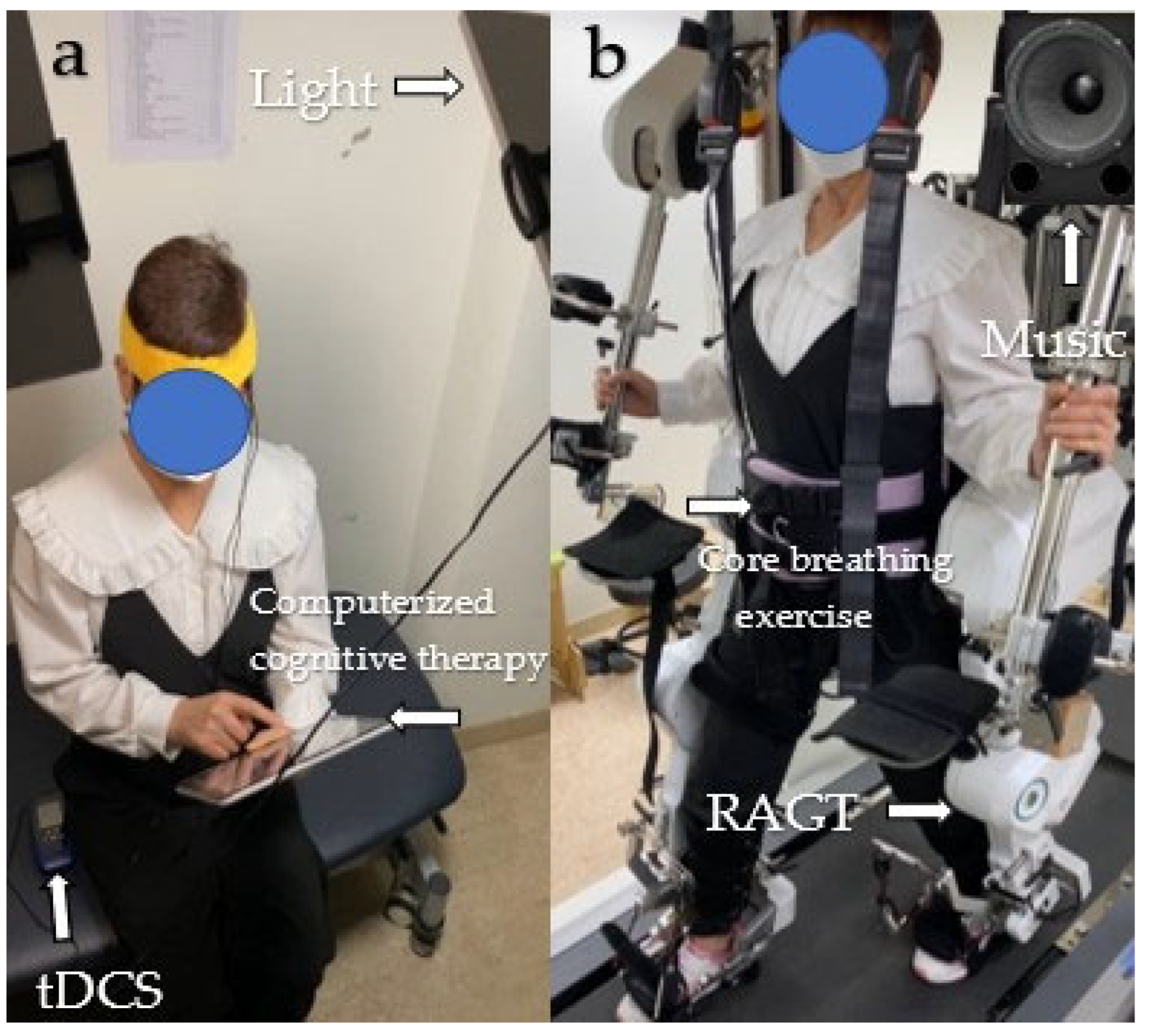
2.3. Intervention—MBE Program
2.4. Clinical Outcome Measures
2.4.1. EEG
2.4.2. EEG Analysis
2.5. Statistical Analysis
3. Results
3.1. Delta Band
3.2. Theta Band
3.3. Alpha Band
3.4. Beta Band
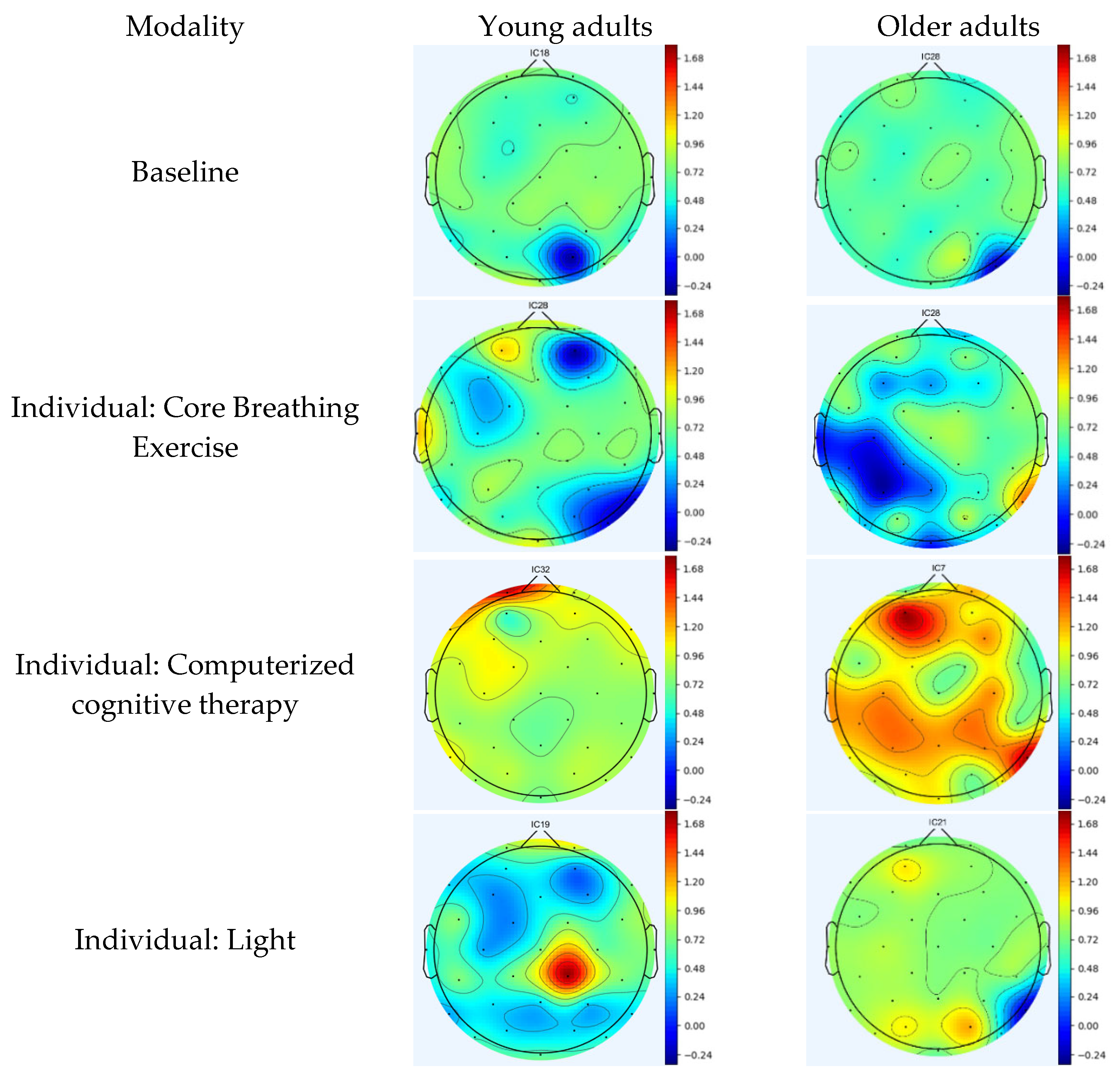
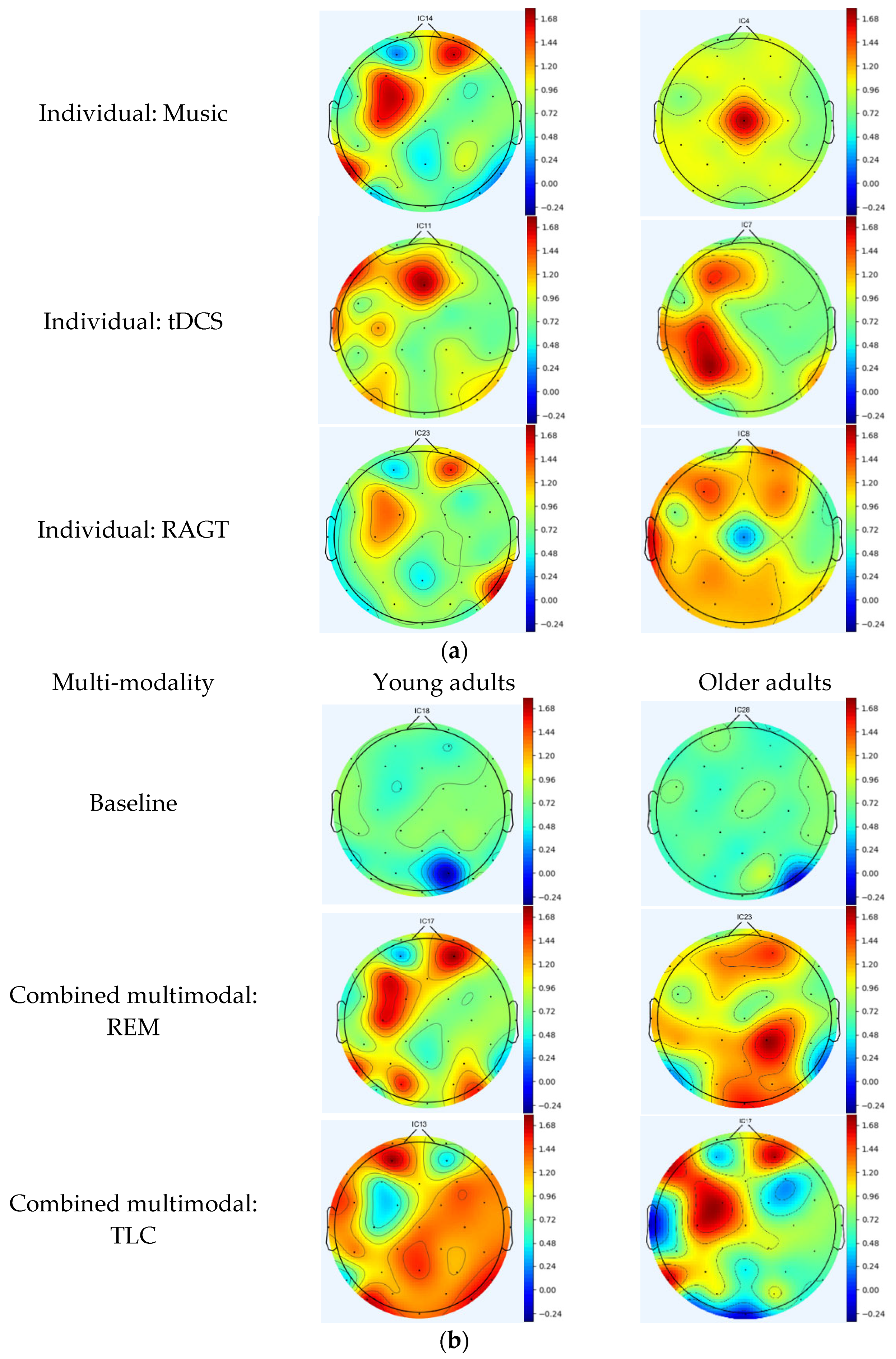
3.5. Topographic Maps
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Oh, W.; Kim, T.H.; You, J.S.H. Self-perception and anticipated efficacy of the anti-dementia multimodal program in 100 older adults with mild cognitive impairment. NeuroRehabilitation 2023, 52, 403–412. [Google Scholar] [CrossRef]
- Fotuhi, M.; Lubinski, B.; Trullinger, M.; Hausterman, N.; Riloff, T.; Hadadi, M.; Raji, C.A. A personalized 12-week “brain fitness program” for improving cognitive function and increasing the volume of hippocampus in elderly with mild cognitive impairment. J. Prev. Alzheimers Dis. 2016, 3, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Parvin, E.; Mohammadian, F.; Amani-Shalamzari, S.; Bayati, M.; Tazesh, B. Dual-task training affect cognitive and physical performances and brain oscillation ratio of patients with Alzheimer’s disease: A randomized controlled trial. Front. Aging Neurosci. 2020, 12, 605317. [Google Scholar] [CrossRef] [PubMed]
- Klados, M.A.; Styliadis, C.; Frantzidis, C.A.; Paraskevopoulos, E.; Bamidis, P.D. Beta-band functional connectivity is reorganized in mild cognitive impairment after combined computerized physical and cognitive training. Front. Neurosci. 2016, 10, 55. [Google Scholar] [CrossRef]
- Calabrò, R.S.; De Luca, R.; Leo, A.; Balletta, T.; Marra, A.; Bramanti, P. Lokomat training in vascular dementia: Motor improvement and beyond! Aging Clin. Exp. Res. 2015, 27, 935–937. [Google Scholar] [CrossRef]
- Chan, M.F.; Chan, E.A.; Mok, E. Effects of music on depression and sleep quality in elderly people: A randomised controlled trial. Complement Ther. Med. 2010, 18, 150–159. [Google Scholar] [CrossRef]
- Chu, H.; Yang, C.Y.; Lin, Y.; Ou, K.L.; Lee, T.Y.; O’Brien, A.P.; Chou, K.R. The impact of group music therapy on depression and cognition in elderly persons with dementia: A randomized controlled study. Biol. Res. Nurs. 2014, 16, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Im, J.J.; Jeong, H.; Bikson, M.; Woods, A.J.; Unal, G.; Oh, J.K.; Na, S.; Park, J.S.; Knotkova, H.; Song, I.U.; et al. Effects of 6-month at-home transcranial direct current stimulation on cognition and cerebral glucose metabolism in Alzheimer’s disease. Brain Stimul. 2019, 12, 1222–1228. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Kwak, H.S. Effect of Computerized Cognitive Therapy for the Elderly with Mild Cognitive Impairment in the Community on Cognitive Function and Instrumental Activities of Daily Living for Wellness. J. Korea Entertain. Ind. Assoc. 2021, 15, 215–223. [Google Scholar] [CrossRef]
- Lee, G.J.; Bang, H.J.; Lee, K.M.; Kong, H.H.; Seo, H.S.; Oh, M.; Bang, M. A comparison of the effects between 2 computerized cognitive training programs, Bettercog and COMCOG, on elderly patients with MCI and mild dementia: A single-blind randomized controlled study. Medicine 2018, 97, 45. [Google Scholar] [CrossRef]
- Riemersma-Van Der Lek, R.F.; Swaab, D.F.; Twisk, J.; Hol, E.M.; Hoogendijk, W.J.; Van Someren, E.J. Effect of bright light and melatonin on cognitive and noncognitive function in elderly residents of group care facilities: A randomized controlled trial. JAMA 2008, 299, 2642–2655. [Google Scholar] [CrossRef]
- Tsai, Y.F.; Wong, T.K.; Juang, Y.Y.; Tsai, H.H. The effects of light therapy on depressed elders. Int. J. Geriatr. Psychiatry 2004, 19, 545–548. [Google Scholar] [CrossRef] [PubMed]
- Yadav, G.; Mutha, P.K. Deep breathing practice facilitates retention of newly learned motor skills. Sci. Rep. 2016, 6, 37069. [Google Scholar] [CrossRef]
- Wong, G.H.; Ng, C.K.; Lai, C.K.; Lee, M.N.; Lum, T.Y.; Jiang, N.; Dai, D.L. Development of six arts, a culturally appropriate multimodal nonpharmacological intervention in dementia. Gerontologist 2015, 55, 865–874. [Google Scholar] [CrossRef][Green Version]
- Ip, I.M.H.; Honey, A.; McGrath, M. ‘Doing’dating: A cross-sectional survey of young adults (18–35 years) in Australia and Hong Kong. Aust. Occup. Ther. J. 2022, 69, 233–242. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, S.; Terada, S.; Oshima, E.; Sato, S.; Kurisu, K.; Takenoshita, S.; Yokota, O.; Yamada, N. Verbal or visual memory score and regional cerebral blood flow in Alzheimer disease. Dement. Geriatr. Cogn. Dis. Extra 2018, 8, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Herwig, U.; Satrapi, P.; Schönfeldt-Lecuona, C. Using the international 10-20 EEG system for positioning of transcranial magnetic stimulation. Brain Topogr. 2003, 16, 95–99. [Google Scholar] [CrossRef]
- Delorme, A.; Makeig, S. EEGLAB: An open source toolbox for analysis of single-trial EEG dynamics including independent component analysis. J. Neurosci. Methods 2004, 134, 9–21. [Google Scholar] [CrossRef]
- Luu, T.P.; Nakagome, S.; He, Y.; Contreras-Vidal, J.L. Real-time EEG-based brain-computer interface to a virtual avatar enhances cortical involvement in human treadmill walking. Sci. Rep. 2017, 7, 8895. [Google Scholar] [CrossRef]
- Cisneros, E.; de Guise, E.; Belleville, S.; McKerral, M. A controlled clinical efficacy trial of multimodal cognitive rehabilitation on episodic memory functioning in older adults with traumatic brain injury. Ann. Phys. Rehabil. Med. 2021, 64, 101563. [Google Scholar] [CrossRef]
- Stuss, D.T.; Benson, D.F. The frontal lobes and control of cognition and memory. In The Frontal Lobes Revisited; Psychology Press: New York, NY, USA, 2019; pp. 141–158. [Google Scholar]
- Barense, M.D.; Warren, J.D.; Bussey, T.J.; Saksida, L.M. The temporal lobes. In Oxford Textbook of Cognitive Neurology and De-mentia; Oxford University Press: Oxford, UK, 2016; pp. 39–49. [Google Scholar]
- Guy-Evans, O. Parietal Lobe: Definition, Functions, Structure & Location. Simply Psychol. 2023. [Google Scholar]
- Schafer, E. On the functions of the temporal and occipital lobes: A reply to Dr. Ferrier. Brain 1888, 11, 145–165. [Google Scholar] [CrossRef]
- Westwood, S.J.; Criaud, M.; Lam, S.L.; Lukito, S.; Wallace-Hanlon, S.; Kowalczyk, O.S.; Kostara, A.; Mathew, J.; Agbedjro, D.; Wexler, B.E.; et al. Transcranial direct current stimulation (tDCS) combined with cognitive training in adolescent boys with ADHD: A double-blind, randomised, sham-controlled trial. Psychol. Med. 2023, 53, 497–512. [Google Scholar] [CrossRef]
- Andrade, S.M.; da Silva Machado, D.G.; da Silva-Sauerc, L.; Regis, C.T.; Mendes, C.K.T.T.; de Araújo, J.S.S.; Costa, L.P.; Bezerra Sales Queiroz, M.E.; Leitão, M.M.; Fernández-Calvo, B. Effects of multisite anodal transcranial direct current stimulation combined with cognitive stimulation in patients with Alzheimer’s disease and its neurophysiological correlates: A double-blind randomized clinical trial. Neurophysiol. Clin. 2022, 52, 117–127. [Google Scholar] [CrossRef]
- Dong, L.; Ke, Y.; Liu, S.; Song, X.; Ming, D. Effects of HD-tDCS combined with working memory training on event-related potentials. In Proceedings of the 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; pp. 1–4. [Google Scholar]
- Münch, M.; Plomp, G.; Thunell, E.; Kawasaki, A.; Scartezzini, J.L.; Herzog, M.H. Different colors of light lead to different adaptation and activation as determined by high-density EEG. NeuroImage 2014, 101, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Buzsaki, G. Rhythms of the Brain; Oxford University Press: Oxford, UK, 2006. [Google Scholar]
- Ferrucci, R.; Brunoni, A.R.; Parazzini, M.; Vergari, M.; Rossi, E.; Fumagalli, M.; Mameli, F.; Rosa, M.; Giannicola, G.; Zago, S.; et al. Modulating human procedural learning by cerebellar transcranial direct current stimulation. Cerebellum 2013, 12, 485–492. [Google Scholar] [CrossRef]
- Petrides, M. Functional organization of the human frontal cortex for mnemonic processing: Evidence from neuroimaging studies. In Structure and Functions of the Human Prefrontal Cortex; New York Academy of Sciences: New York, NY, USA, 1995. [Google Scholar]
- Possti, D.; Fahoum, F.; Sosnik, R.; Giladi, N.; Hausdorff, J.M.; Mirelman, A.; Maidan, I. Changes in the EEG spectral power during dual-task walking with aging and Parkinson’s disease: Initial findings using Event-Related Spectral Perturbation analysis. J. Neurol. 2021, 268, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Breitling, D.; Guenther, W.; Rondot, P. Auditory perception of music measured by brain electrical activity mapping. Neuropsychologia 1987, 25, 765–774. [Google Scholar] [CrossRef]
- Formaggio, E.; Masiero, S.; Bosco, A.; Izzi, F.; Piccione, F.; Del Felice, A. Quantitative EEG evaluation during robot-assisted foot movement. IEEE Trans. Neural. Syst. Rehabil. Eng. 2016, 25, 1633–1640. [Google Scholar] [CrossRef]
- Patnaik, S.; Pandey, P.; Arun, I.; Yadav, G.; Miyapuram, K.P.; Lomas, D. EEG spectral correlates of rapid and deep slow breathing states and classification using ML. In Proceedings of the 2022 IEEE Region 10 Symposium (TENSYMP), Mumbai, India, 1–3 July 2022; pp. 1–6. [Google Scholar]
- Ferrarelli, F.; Smith, R.; Dentico, D.; Riedner, B.A.; Zennig, C.; Benca, R.M.; Lutz, A.; Davidson, R.J.; Tononi, G. Experienced mindfulness meditators exhibit higher parietal-occipital EEG gamma activity during NREM sleep. PLoS ONE 2013, 8, e73417. [Google Scholar] [CrossRef] [PubMed]
- Brunel, N. Dynamics and plasticity of stimulus-selective persistent activity in cortical network models. Cereb. Cortex 2003, 13, 1151–1161. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Brainwaves | Frequency (Hz) | Functions |
|---|---|---|
| Delta | 2–4 Hz | Deep sleep, dreaming, and coma |
| Theta | 4–8 Hz | Drowsy, meditation, and mental imagery |
| Alpha | 8–12 Hz | Relaxed, calm, and lucid |
| Beta | 12–30 Hz | Concentration, awake, alert, thinking, and mental activity |
| Characteristics | Older Adults with MCI (n = 20) | Young Adults (n = 20) | p-Value |
|---|---|---|---|
| Age (years) | 79 ± 8.25 | 25.2 ± 3.19 | 0.006 * |
| Height (cm) | 157.25 ± 8.45 | 169.65 ± 9.37 | 0.717 |
| Weight (kg) | 59.4 ± 7.3 | 67.7 ± 13.83 | 0.002 * |
| MMSE | 21 | 26 | 0.000 * |
| Gender (M/F) | 10/10 | 9/11 | 0.664 |
| (a) | |||
|---|---|---|---|
| Young Adults | p-Value | ||
| Delta, 2–4 | Baseline | Conditions | |
| Core breathing exercise | 2.64 ± 0.32 | 2.36 ± 0.20 | 0.000 ** |
| Computerized cognitive therapy | 2.64 ± 0.32 | 1.46 ± 0.70 | 0.000 ** |
| Light | 2.64 ± 0.32 | 1.50 ± 0.21 | 0.000 ** |
| Music | 2.64 ± 0.32 | 1.79 ± 0.64 | 0.000 ** |
| REM | 2.64 ± 0.32 | 1.22 ± 0.47 | 0.000 ** |
| tDCS | 2.64 ± 0.32 | 1.22 ± 0.14 | 0.000 ** |
| TLC | 2.64 ± 0.32 | 1.45 ± 0.33 | 0.000 ** |
| RAGT | 2.64 ± 0.32 | 1.17 ± 0.33 | 0.000 ** |
| Theta, 4–8 | Baseline | Conditions | |
| Core breathing exercise | 0.41 ± 0.37 | 1.07 ± 0.59 | 0.000 ** |
| Computerized cognitive therapy | 0.41 ± 0.37 | 0.48 ± 0.14 | 0.876 |
| Light | 0.41 ± 0.37 | 0.81 ± 0.48 | 0.000 ** |
| Music | 0.41 ± 0.37 | 0.91 ± 0.24 | 0.000 ** |
| REM | 0.41 ± 0.37 | 1.10 ± 0.31 | 0.000 ** |
| tDCS | 0.41 ± 0.37 | 1.29 ± 0.18 | 0.000 ** |
| TLC | 0.41 ± 0.37 | 1.28 ± 0.27 | 0.000 ** |
| RAGT | 0.41 ± 0.37 | 0.74 ± 0.36 | 0.000 ** |
| Alpha, 8–12 | Baseline | Conditions | |
| Core breathing exercise | −0.51 ± 0.41 | −0.45 ± 0.51 | 0.376 |
| Computerized cognitive therapy | −0.51 ± 0.41 | −0.37 ± 0.25 | 0.060 |
| Light | −0.51 ± 0.41 | −0.13 ± 0.22 | 0.000 ** |
| Music | −0.51 ± 0.41 | −0.38 ± 0.40 | 0.053 |
| REM | −0.51 ± 0.41 | 0.52 ± 0.26 | 0.000 ** |
| tDCS | −0.51 ± 0.41 | 0.16 ± 0.37 | 0.000 ** |
| TLC | −0.51 ± 0.41 | 0.77 ± 0.21 | 0.000 ** |
| RAGT | −0.51 ± 0.41 | −0.28 ± 0.22 | 0.001 ** |
| Beta, 12–30 | Baseline | Conditions | |
| Core breathing exercise | −0.56 ± 0.30 | −0.23 ± 0.28 | 0.000 ** |
| Computerized cognitive therapy | −0.56 ± 0.30 | −0.11 ± 0.31 | 0.000 ** |
| Light | −0.56 ± 0.30 | −0.17 ± 0.21 | 0.000 ** |
| Music | −0.56 ± 0.30 | −0.03 ± 0.26 | 0.000 ** |
| REM | −0.56 ± 0.30 | 0.09 ± 0.20 | 0.000 ** |
| tDCS | −0.56 ± 0.30 | −0.012 ± 0.27 | 0.000 ** |
| TLC | −0.56 ± 0.30 | 0.12 ± 0.18 | 0.000 ** |
| RAGT | −0.56 ± 0.30 | −0.2 ± 0.23 | 0.000 ** |
| (b) | |||
| Older Adults | p-Value | ||
| Delta, 2–4 | Baseline | Conditions | |
| Core breathing exercise | 2.62 ± 0.27 | 2.81 ± 0.31 | 0.000 ** |
| Computerized cognitive therapy | 2.62 ± 0.27 | 1.05 ± 0.29 | 0.000 ** |
| Light | 2.62 ± 0.27 | 1.86 ± 0.11 | 0.000 ** |
| Music | 2.62 ± 0.27 | 1.06 ± 0.53 | 0.000 ** |
| REM | 2.62 ± 0.27 | 1.55 ± 0.44 | 0.000 ** |
| tDCS | 2.62 ± 0.27 | 1.47 ± 0.23 | 0.000 ** |
| TLC | 2.62 ± 0.27 | 1.13 ± 0.41 | 0.000 ** |
| RAGT | 2.62 ± 0.27 | 2.22 ± 0.72 | 0.000 ** |
| Theta, 4–8 | Baseline | Conditions | |
| Core breathing exercise | 0.39 ± 0.45 | 1.14 ± 0.13 | 0.000 ** |
| Computerized cognitive therapy | 0.39 ± 0.45 | 1.04 ± 0.17 | 0.000 ** |
| Light | 0.39 ± 0.45 | 0.87 ± 0.36 | 0.000 ** |
| Music | 0.39 ± 0.45 | 1.15 ± 0.61 | 0.000 ** |
| REM | 0.39 ± 0.45 | 1.43 ± 0.37 | 0.000 ** |
| tDCS | 0.39 ± 0.45 | 0.55 ± 0.52 | 0.326 |
| TLC | 0.39 ± 0.45 | 0.73 ± 0.54 | 0.000 ** |
| RAGT | 0.39 ± 0.45 | 0.56 ± 0.49 | 0.031 * |
| Alpha, 8–12 | Baseline | Conditions | |
| Core breathing exercise | −0.67 ± 0.19 | −0.60 ± 0.31 | 0.268 |
| Computerized cognitive therapy | −0.67 ± 0.19 | 0.16 ± 0.12 | 0.000 ** |
| Light | −0.67 ± 0.19 | −0.46 ± 0.38 | 0.016 * |
| Music | −0.67 ± 0.19 | −0.12 ± 0.62 | 0.000 ** |
| REM | −0.67 ± 0.19 | 0.32 ± 0.51 | 0.000 ** |
| tDCS | −0.67 ± 0.19 | −0.43 ± 0.55 | 0.003 ** |
| TLC | −0.67 ± 0.19 | 0.23 ± 0.54 | 0.000 ** |
| RAGT | −0.67 ± 0.19 | −0.23 ± 0.28 | 0.001 ** |
| Beta, 12–30 | Baseline | Conditions | |
| Core breathing exercise | −0.41 ± 0.21 | −0.30 ± 0.25 | 0.007 ** |
| Computerized cognitive therapy | −0.41 ± 0.21 | 0.04 ± 0.32 | 0.000 ** |
| Light | −0.41 ± 0.21 | −0.33 ± 0.14 | 0.022 * |
| Music | −0.41 ± 0.21 | −0.23 ± 0.27 | 0.000 ** |
| REM | −0.41 ± 0.21 | 0.08 ± 0.33 | 0.000 ** |
| tDCS | −0.41 ± 0.21 | −0.26 ± 0.24 | 0.003 ** |
| TLC | −0.41 ± 0.21 | 0.09 ± 0.27 | 0.000 ** |
| RAGT | −0.41 ± 0.21 | −0.28 ± 0.41 | 0.001 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, W.; Park, H.; Hallett, M.; You, J.H. The Effectiveness of a Multimodal Brain Empowerment Program in Mild Cognitive Impairment: A Single-Blind, Quasi-Randomized Experimental Study. J. Clin. Med. 2023, 12, 4895. https://doi.org/10.3390/jcm12154895
Oh W, Park H, Hallett M, You JH. The Effectiveness of a Multimodal Brain Empowerment Program in Mild Cognitive Impairment: A Single-Blind, Quasi-Randomized Experimental Study. Journal of Clinical Medicine. 2023; 12(15):4895. https://doi.org/10.3390/jcm12154895
Chicago/Turabian StyleOh, Wonjun, Haeun Park, Mark Hallett, and Joshua (Sung) H. You. 2023. "The Effectiveness of a Multimodal Brain Empowerment Program in Mild Cognitive Impairment: A Single-Blind, Quasi-Randomized Experimental Study" Journal of Clinical Medicine 12, no. 15: 4895. https://doi.org/10.3390/jcm12154895
APA StyleOh, W., Park, H., Hallett, M., & You, J. H. (2023). The Effectiveness of a Multimodal Brain Empowerment Program in Mild Cognitive Impairment: A Single-Blind, Quasi-Randomized Experimental Study. Journal of Clinical Medicine, 12(15), 4895. https://doi.org/10.3390/jcm12154895