
Kidney Perfusion in Contrast-Enhanced Ultrasound (CEUS) Correlates with Renal Function in Living Kidney Donors


 , ,
, , 
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design and Patient Population
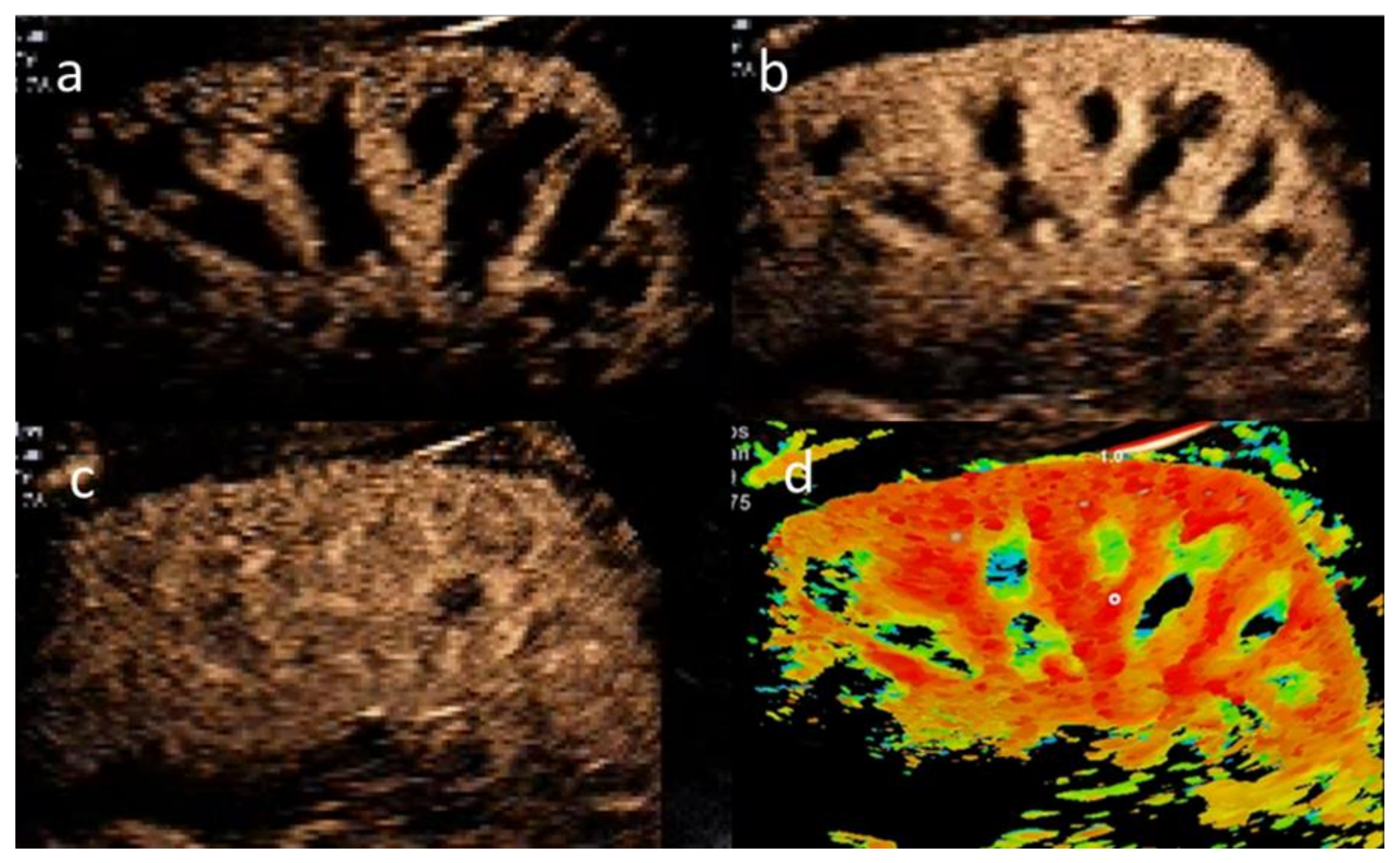
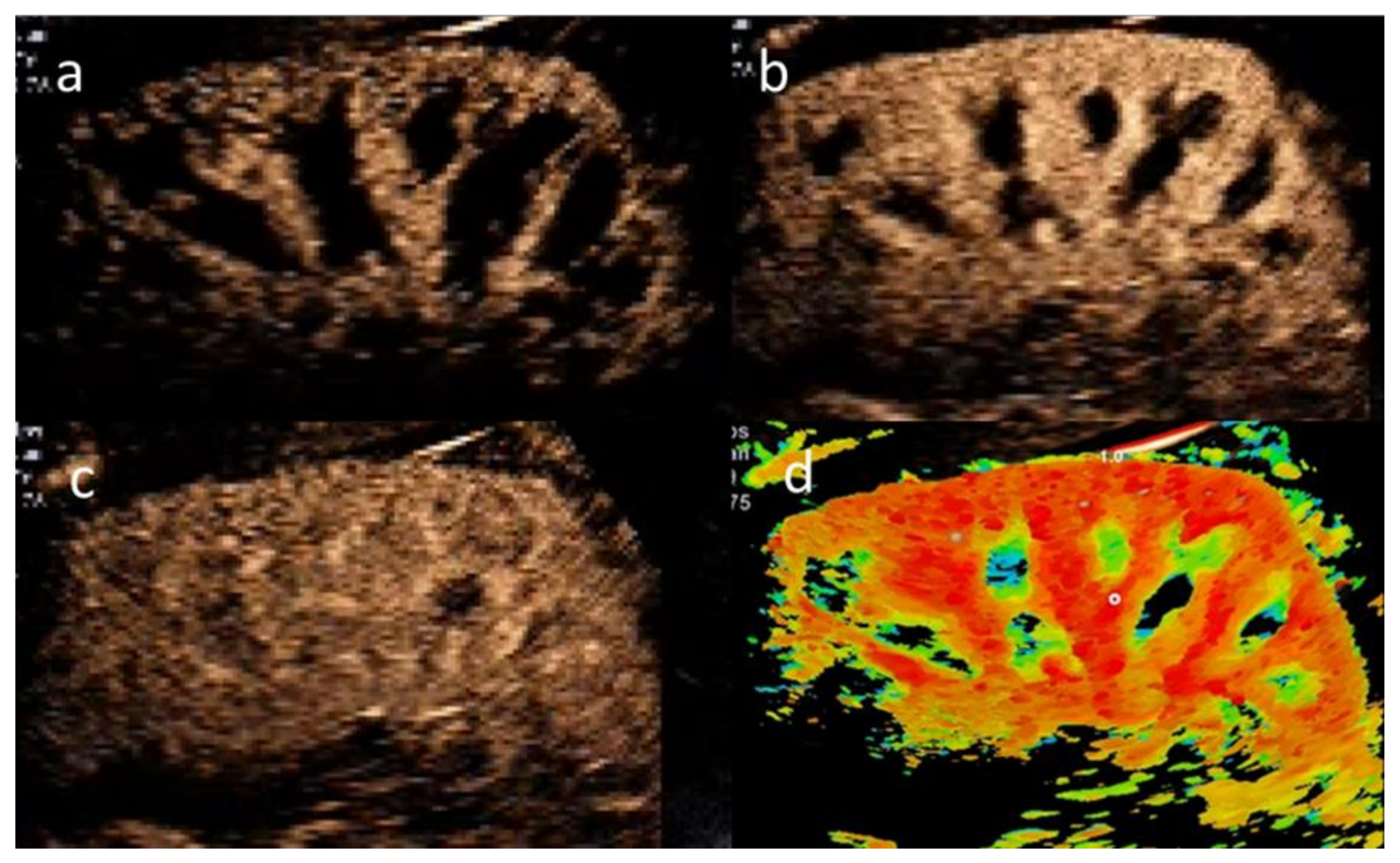
2.2. CEUS Examination Protocol
2.3. Ultrasound Settings
2.4. Quantitative Perfusion Analysis
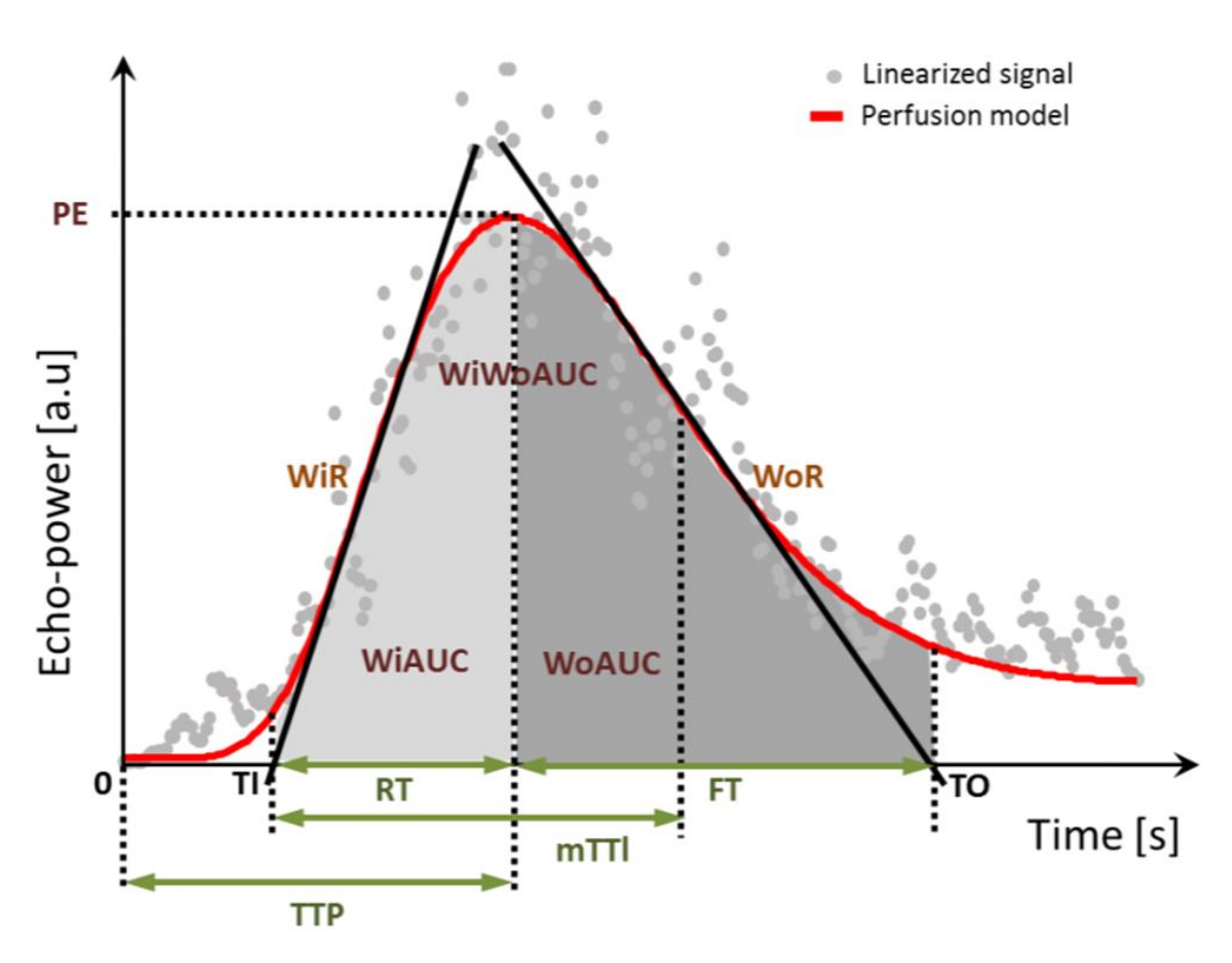
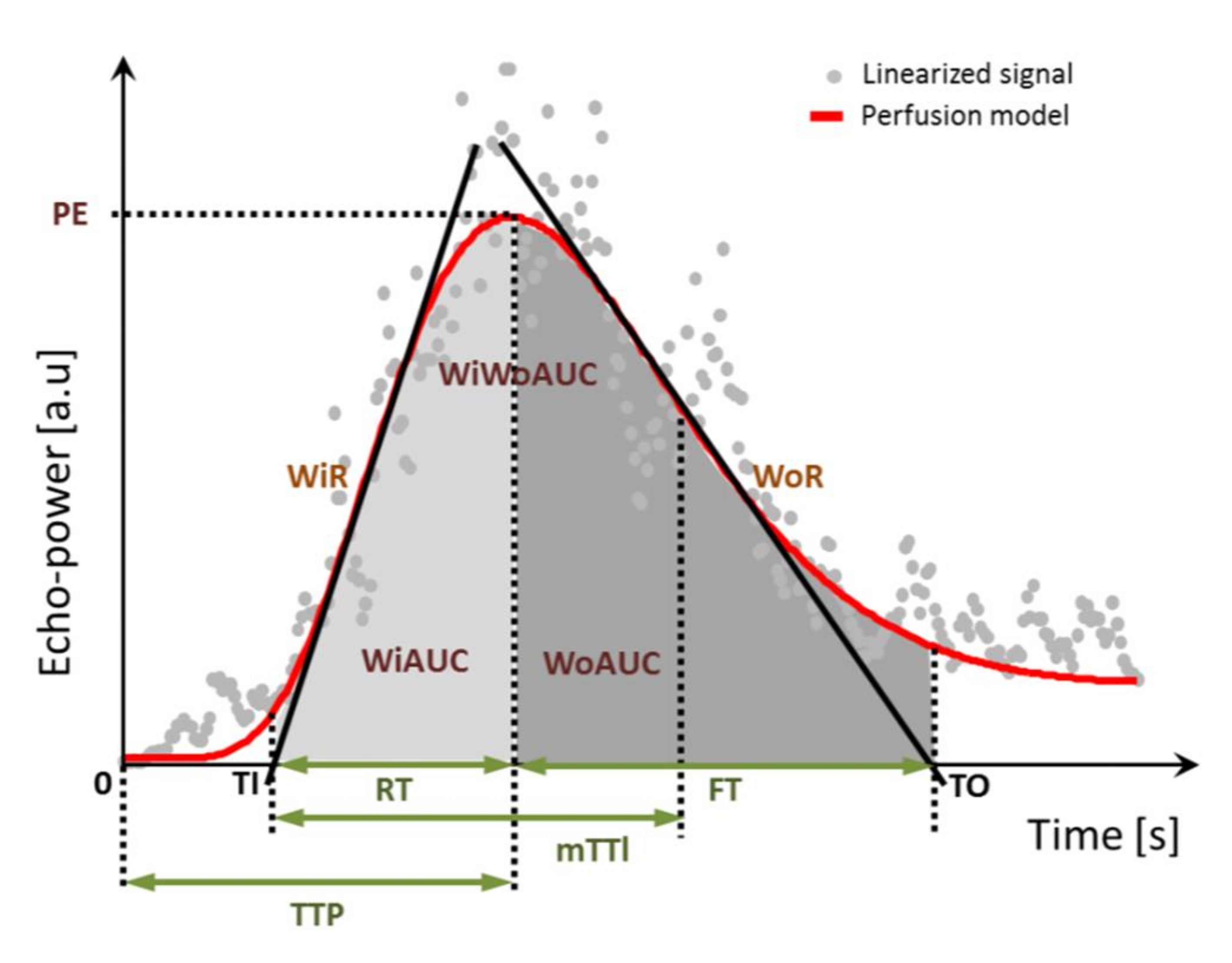
2.5. Perfusion Parameters
2.6. Patient Data and Methods for Assessment of Kidney Function
2.7. Statistical Analysis
3. Results
3.1. Epidemiology and Descriptive Presentation of Kidney Function Data
3.2. CEUS Parameters
3.3. Analysis of Total Kidney Function
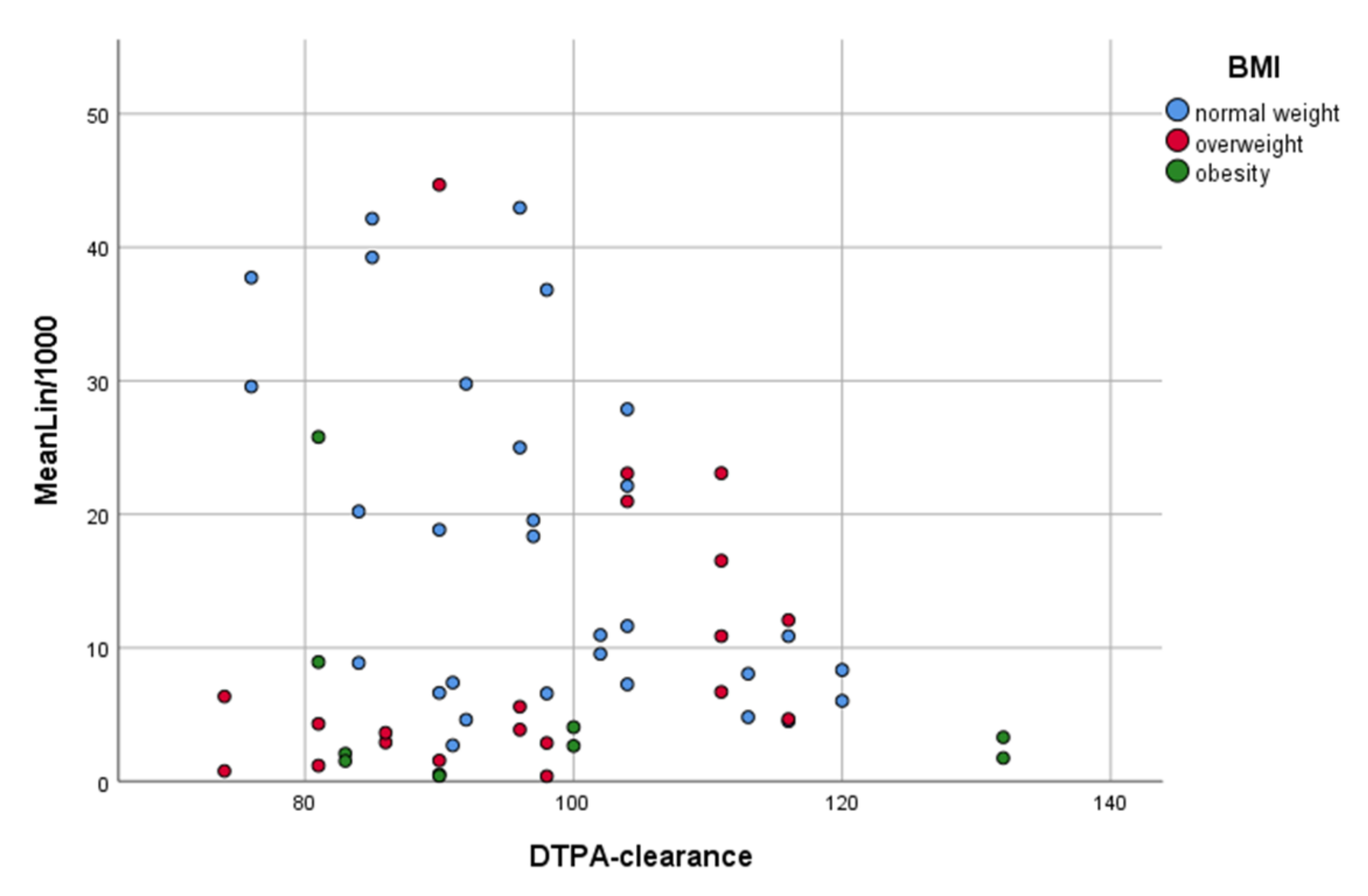
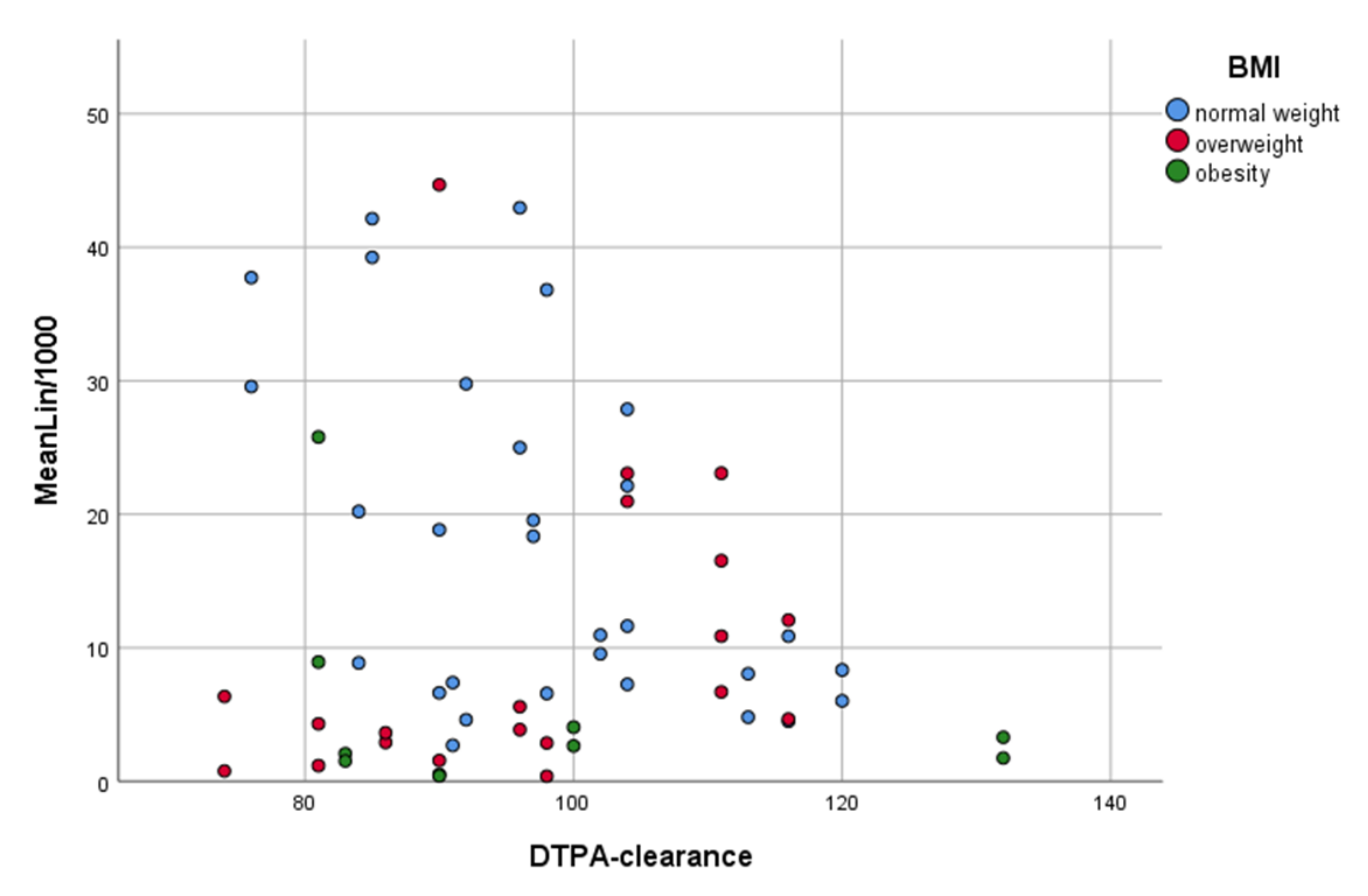
3.4. Comparison of CEUS and Kidney Function Parameters
3.5. Evaluation of Confounders
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Delmonico, F. A Report of the Amsterdam Forum On the Care of the Live Kidney Donor: Data and Medical Guidelines. Transplantation 2005, 79, S53–S66. [Google Scholar] [PubMed]
- Durand, E.; Müller-Suur, R. Zur Messung der Nierenfunktion durch Clearancebestimmungen: Methoden und Indikationen—Ein Update. Der Nukl. 2010, 33, 145–153. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., III; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D. A more accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Modification of Diet in Renal Disease Study Group. Ann. Intern. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef]
- Cockcroft, D.W.; Gault, M.H. Prediction of creatinine clearance from serum creatinine. Nephron 1976, 16, 31–41. [Google Scholar] [CrossRef]
- Levey, A.S.; Inker, L.A.; Coresh, J. GFR estimation: From physiology to public health. Am. J. Kidney Dis. 2014, 63, 820–834. [Google Scholar] [CrossRef] [Green Version]
- Lentine, K.L.; Kasiske, B.L.; Levey, A.S.; Adams, P.L.; Alberú, J.; Bakr, M.A.; Gallon, L.; Garvey, C.A.; Guleria, S.; Li, P.K.-T.; et al. Summary of Kidney Disease: Improving Global Outcomes (KDIGO) Clinical Practice Guideline on the Evaluation and Care of Living Kidney Donors. Transplantation 2017, 101, 1783–1792. [Google Scholar] [CrossRef] [Green Version]
- Abramowicz, D.; Cochat, P.; Claas, F.H.; Heemann, U.; Pascual, J.; Dudley, C.; Harden, P.; Hourmant, M.; Maggiore, U.; Salvadori, M.; et al. European Renal Best Practice Guideline on kidney donor and recipient evaluation and perioperative care. Nephrol. Dial. Transplant. 2015, 30, 1790–1797. [Google Scholar] [CrossRef]
- Andrews, P.A.; Burnapp, L.; Manas, D.; Bradley, J.A.; Dudley, C. Summary of the British Transplantation Society/Renal Association U.K. guidelines for living donor kidney transplantation. Transplantation 2012, 93, 666–673. [Google Scholar] [CrossRef]
- Halleck, F.; Diederichs, G.; Koehlitz, T.; Slowinski, T.; Engelken, F.; Liefeldt, L.; Friedersdorff, F.; Fuller, T.F.; Magheli, A.; Neumayer, H.-H.; et al. Volume matters: CT-based renal cortex volume measurement in the evaluation of living kidney donors. Transpl. Int. 2013, 26, 1208–1216. [Google Scholar] [CrossRef]
- Brar, A.; Jindal, R.M.; Abbott, K.C.; Hurst, F.P.; Salifu, M.O. Practice patterns in evaluation of living kidney donors in United Network for Organ Sharing-approved kidney transplant centers. Am. J. Nephrol. 2012, 35, 466–473. [Google Scholar] [CrossRef]
- Poggio, E.D.; Hila, S.; Stephany, B.; Fatica, R.; Krishnamurthi, V.; Del Bosque, C.; Goldfarb, D.; Herts, B.; Dennis, V.W.; Heeger, P.S.; et al. Donor kidney volume and outcomes following live donor kidney transplantation. Am. J. Transplant. 2006, 6, 616–624. [Google Scholar] [CrossRef] [PubMed]
- Paleologo, G.; Abdelkawy, H.; Barsotti, M.; Basha, A.; Bernabini, G.; Bianchi, A.; Caprio, F.; Emad, A.; Grassi, G.; Nerucci, B.; et al. Kidney dimensions at sonography are correlated with glomerular filtration rate in renal transplant recipients and in kidney donors. Transplant. Proc. 2007, 39, 1779–1781. [Google Scholar] [CrossRef]
- Buckley, D.L.; Shurrab, A.E.; Cheung, C.M.; Jones, A.P.; Mamtora, H.; Kalra, P.A. Measurement of single kidney function using dynamic contrast-enhanced MRI: Comparison of two models in human subjects. J. Magn. Reson. Imaging 2006, 24, 1117–1123. [Google Scholar] [CrossRef]
- Raptis, A.E.; Viberti, G. Pathogenesis of diabetic nephropathy. Exp. Clin. Endocrinol. Diabetes 2001, 109 (Suppl. 2), S424–S437. [Google Scholar] [CrossRef] [PubMed]
- Hughson, M.D.; Johnson, K.; Young, R.J.; Hoy, W.E.; Bertram, J.F. Glomerular size and glomerulosclerosis: Relationships to disease categories, glomerular solidification, and ischemic obsolescence. Am. J. Kidney Dis. 2002, 39, 679–688. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Wu, J.; Cheng, J.F.; Liu, X.-Y.; Ma, F.; Guo, L.-H.; Xu, J.-M.; Wu, T.; Mohan, C.; Peng, A.; et al. Diagnostic value of quantitative contrast-enhanced ultrasound (CEUS) for early detection of renal hyperperfusion in diabetic kidney disease. J. Nephrol. 2015, 28, 669–678. [Google Scholar] [CrossRef] [PubMed]
- Sidhu, P.S.; Cantisani, V.; Dietrich, C.F.; Gilja, O.H.; Saftoiu, A.; Bartels, E.; Bertolotto, M.; Calliada, F.; Clevert, D.A.; Cosgrove, D.; et al. The EFSUMB Guidelines and Recommendations for the Clinical Practice of Contrast-Enhanced Ultrasound (CEUS) in Non-Hepatic Applications: Update 2017 (Short Version). Ultraschall Med. 2018, 39, 154–180. [Google Scholar] [CrossRef] [Green Version]
- Spiesecke, P.; Fischer, T.; Maxeiner, A.; Hamm, B.; Lerchbaumer, M.H. Contrast-enhanced ultrasound (CEUS) reliably rules out neoplasm in developmental renal pseudotumor. Acta Radiol. 2020, 62, 821–829. [Google Scholar] [CrossRef]
- Greis, C. Ultrasound contrast agents as markers of vascularity and microcirculation. Clin. Hemorheol. Microcirc. 2009, 43, 1–9. [Google Scholar] [CrossRef]
- Greis, C. Quantitative evaluation of microvascular blood flow by contrast-enhanced ultrasound (CEUS). Clin. Hemorheol. Microcirc. 2011, 49, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Bracco. User Manual|CEUS—Contrast Enhanced Ultrasound: Bracco Suisse SA; Copyright© 2019 Bracco Suisse SA All Rights Reserved. Available online: https://www.contrastultrasound-modality.com/quantification-software/support/user-manual (accessed on 22 December 2020).
- Fleming, J.S.; Persaud, L.; Zivanovic, M.A. A general equation for estimating glomerular filtration rate from a single plasma sample. Nucl. Med. Commun. 2005, 26, 743–748. [Google Scholar] [CrossRef] [PubMed]
- Bubeck, B. Renal clearance determination with one blood sample: Improved accuracy and universal applicability by a new calculation principle. Semin. Nucl. Med. 1993, 23, 73–86. [Google Scholar] [CrossRef]
- Dietrich, C.F.; Averkiou, M.; Nielsen, M.B.; Barr, R.G.; Burns, P.N.; Calliada, F.; Cantisani, V.; Choi, B.; Chammas, M.C.; Clevert, D.A.; et al. How to perform Contrast-Enhanced Ultrasound (CEUS). Ultrasound Int. Open 2018, 4, E2–E15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kunz, P.; Kiesl, S.; Groß, S.; Kauczor, H.-U.; Schmidmaier, G.; Fischer, C. Intra-observer and Device-Dependent Inter-observer Reliability of Contrast-Enhanced Ultrasound for Muscle Perfusion Quantification. Ultrasound Med. Biol. 2020, 46, 275–285. [Google Scholar] [CrossRef]
- Krumm, P.; Hupka, T.; Haußmann, F.; Dittmann, H.; Mühlbacher, T.; Nadalin, S.; Königsrainer, A.; Nikolaou, K.; Heyne, N.; Kramer, U.; et al. Contrast-enhanced MRI for simultaneous evaluation of renal morphology and split renal function in living kidney donor candidates. Eur. J. Radiol. 2021, 142, 109864. [Google Scholar] [CrossRef]
- Tang, C.; Fang, K.; Guo, Y.; Li, R.; Fan, X.; Chen, P.; Chen, Z.; Liu, Q.; Zou, Y. Safety of Sulfur Hexafluoride Microbubbles in Sonography of Abdominal and Superficial Organs: Retrospective Analysis of 30,222 Cases. J. Ultrasound Med. 2017, 36, 531–538. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| CEUS Parameter | Label | Description | |
|---|---|---|---|
| Time-related parameters † | RT | Rise time | - |
| mTTl | Mean transit time local (mTT-Tl) | - | |
| TTP | Time to peak | - | |
| FT | Fall time | - | |
| Signal intensity parameters * | MeanLin | - | Mean signal intensity |
| PE | Peak enhancement | Maximum signal enhancement | |
| WiAUC | Wash-in area under the curve (AUC (TI:TTP)) | AUC (area under the curve) during wash-in of UCA (between TI and TTP) | |
| WiR | Wash-in rate | Maximum increase | |
| WiPI | Wash-in perfusion index | WiAUC/RT | |
| WoAUC | Wash-out AUC (AUC (TTP:TO)) | AUC (area under the curve) during wash-out of UCA (between TTP und TO) | |
| WiWoAUC | Wash-in and wash-out AUC | WiAUC + WiWoAUC | |
| WoR | Wash-out rate | Maximum decrease |
| Mean | Standard Deviation | Total | |||
|---|---|---|---|---|---|
| Total kidney function prior to nephrectomy | DTPA clearance (mL/min/1.73 m2) | 97 | 14 | 30 | |
| Serum creatinine (mg/dL) | 0.83 | 0.13 | 30 | ||
| eGFR (CG) (mL/min/1.73 m2) | 95 | 25 | 30 | ||
| eGFR (CKD-EPI) (mL/min/1.73 m2) | 87 | 14 | 30 | ||
| eGFR (MDRD) (mL/min/1.73 m2) | 84 | 14 | 30 | ||
| Total kidney volume (cm3) | 323 | 74 | 30 | ||
| Split kidney function prior to nephrectomy | Proportion in MAG3 (%) | right | 47.6 | 3.3 | 30 |
| left | 52.4 | 3.3 | 30 | ||
| Split DTPA clearance (mL/min/1.73 m2) | 49 | 8 | 60 | ||
| Split eGFR (CG) (mL/min/1.73 m2) | 47 | 13 | 60 | ||
| Split eGFR (CKD-EPI) (mL/min/1.73 m2) | 44 | 8 | 60 | ||
| Split eGFR (MDRD) (mL/min/1.73 m2) | 42 | 8 | 60 | ||
| Split kidney volume (cm3) | 162 | 38 | 60 | ||
| Total kidney function after nephrectomy | eGFR (CG) (mL/min/1.73 m2) | 59 | 17 | 30 | |
| eGFR (CKD-EPI) (mL/min/1.73 m2) | 50 | 11 | 30 | ||
| eGFR (MDRD) (mL/min/1.73 m2) | 49 | 9 | 30 | ||
| Parameter * | Mean | Interquartile Range | Correlation with MeanLin | Total |
|---|---|---|---|---|
| MeanLin † | 12.9 | 17.1 (3.7–20.8) | - | 60 |
| PE † | 27.6 | 38.1 (8–46.1) | r = 0.984; p < 0.001 | 59 |
| WiAUC † | 80 | 102.1 (22.4–124.5) | r = 0.987; p < 0.001 | 59 |
| WiR † | 8.8 | 13.4 (2.3–15.7) | r = 0.937; p < 0.001 | 59 |
| WiPI † | 17.5 | 23.8 (5.6–29.4) | r = 0.985; p < 0.001 | 59 |
| WoAUC † | 150.8 | 192.3 (41.3–233.6) | r = 0.983; p < 0.001 | 58 |
| WiWoAUC † | 230.6 | 292 (64–356) | r = 0.983; p < 0.001 | 58 |
| WoR † | 3.7 | 5.3 (0.9–6.2) | r = 0.930; p < 0.001 | 58 |
| Mean | Interquartile Range | Correlation with RT | Total | |
| RT ‡ | 4.7 | 1.2 (3.8–5) | - | 59 |
| mTTI ‡ | 25.8 | 17.1 (14–31.1) | r = 0.387; p = 0.002 | 59 |
| TTP ‡ | 7.4 | 2.1 (6.2–8.3) | r = 0.860; p < 0.001 | 59 |
| FT ‡ | 9.5 | 2.2 (7.5–9.7) | r = 0.898; p < 0.001 | 58 |
| Correlation with DTPA Clearance | p-Value | |
|---|---|---|
| eGFR (CG) | r = 0.531 | p = 0.003 |
| Total kidney volume | r = 0.472 | p = 0.008 |
| eGFR (CKD-EPI) | r = 0.470 | p = 0.009 |
| eGFR (MDRD) | r = 0.377 | p = 0.040 |
| Serum creatinine | r = −0.228 | p = 0.225 |
| Correlation with DTPA | Correlation with eGFR (CKD-EPI) | Correlation with eGFR (CG) | Correlation with Total Kidney Volume | |
|---|---|---|---|---|
| MeanLin | r = −0.170; p = 0.194 | r = −0.179; p = 0.172 | r = −0.345; p = 0.007 | r = −0.409; p = 0.001 |
| PE | r = −0.162; p = 0.221 | r = −0.182; p = 0.169 | r = −0.322; p = 0.013 | r = −0.392; p = 0.002 |
| WiAUC | r = −0.189; p = 0.152 | r = −0.214; p = 0.104 | r = −0.339; p = 0.009 | r = −0.402; p = 0.002 |
| WiR | r = −0.112; p = 0.399 | r = −0.111; p = 0.401 | r = −0.274; p = 0.036 | r = −0.357; p = 0.005 |
| WiPI | r = −0.160; p = 0.225 | r = −0.177; p = 0.179 | r = −0.319; p = 0.014 | r = −0.391; p = 0.014 |
| WoAUC | r = −0.174; p = 0.192 | r = −0.197; p = 0.138 | r = −0.321; p = 0.014 | r = −0.403; p = 0.002 |
| WiWoAUC | r = −0.160; p = 0.229 | r = −0.214; p = 0.106 | r = −0.346; p = 0.008 | r = −0.401; p = 0.002 |
| WoR | r = −0.123; p = 0.356 | r = −0.155; p = 0.245 | r = −0.306; p = 0.019 | r = −0.355; p = 0.006 |
| RT | r = 0.037; p = 0.782 | r = −0.118; p = 0.374 | r = −0.084; p = 0.528 | r = −0.018; p = 0.893 |
| mTTl | r = −0.160; p = 0.226 | r = 0.024; p = 0.860 | r = 0.045; p = 0.733 | r = −0.015; p = 0.913 |
| TTP | r = −0.007; p = 0.959 | r = −0.216; p = 0.100 | r = −0.178; p = 0.178 | r = −0.092; p = 0.489 |
| FT | r = 0.113; p = 0.398 | r = −0.105; p = 0.433 | r = −0.047; p = 0.724 | r = −0.013; p = 0.923 |
| Correlation with Split DTPA | Correlation with Split eGFR (CKD-EPI) | Correlation with Split eGFR (CG) | Correlation with Split Kidney Volume | |
|---|---|---|---|---|
| Preoperative split kidney function | ||||
| MeanLin | r = −0.150; p = 0.253 | r = −0.176; p = 0.179 | r = −0.331; p = 0.010 | r = −0.398; p = 0.002 |
| WiWoAUC | r = −0.151; p = 0.258 | r = −0.216; p = 0.104 | r = −0.338; p = 0.009 | r = −0.389; p = 0.003 |
| Postoperative kidney function | ||||
| MeanLin | n.A. | r = −0.133; p = 0.483 | r = −0.399; p = 0.029 | n.A. |
| WiWoAUC | n.A. | r = −0.148; p = 0.436 | r = −0.393; p = 0.032 | n.A. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El-Bandar, N.; Lerchbaumer, M.H.; Peters, R.; Maxeiner, A.; Kotsch, K.; Sattler, A.; Miller, K.; Schlomm, T.; Hamm, B.; Budde, K.; et al. Kidney Perfusion in Contrast-Enhanced Ultrasound (CEUS) Correlates with Renal Function in Living Kidney Donors. J. Clin. Med. 2022, 11, 791. https://doi.org/10.3390/jcm11030791
El-Bandar N, Lerchbaumer MH, Peters R, Maxeiner A, Kotsch K, Sattler A, Miller K, Schlomm T, Hamm B, Budde K, et al. Kidney Perfusion in Contrast-Enhanced Ultrasound (CEUS) Correlates with Renal Function in Living Kidney Donors. Journal of Clinical Medicine. 2022; 11(3):791. https://doi.org/10.3390/jcm11030791
Chicago/Turabian StyleEl-Bandar, Nasrin, Markus H. Lerchbaumer, Robert Peters, Andreas Maxeiner, Katja Kotsch, Arne Sattler, Kurt Miller, Thorsten Schlomm, Bernd Hamm, Klemens Budde, and et al. 2022. "Kidney Perfusion in Contrast-Enhanced Ultrasound (CEUS) Correlates with Renal Function in Living Kidney Donors" Journal of Clinical Medicine 11, no. 3: 791. https://doi.org/10.3390/jcm11030791
APA StyleEl-Bandar, N., Lerchbaumer, M. H., Peters, R., Maxeiner, A., Kotsch, K., Sattler, A., Miller, K., Schlomm, T., Hamm, B., Budde, K., Liefeldt, L., Fischer, T., & Friedersdorff, F. (2022). Kidney Perfusion in Contrast-Enhanced Ultrasound (CEUS) Correlates with Renal Function in Living Kidney Donors. Journal of Clinical Medicine, 11(3), 791. https://doi.org/10.3390/jcm11030791