
Effects of Low-Load Blood Flow Restriction Resistance Training on Muscle Strength and Hypertrophy Compared with Traditional Resistance Training in Healthy Adults Older Than 60 Years: Systematic Review and Meta-Analysis

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Selection Criteria
- Population: The study participants had to be healthy and older than 60 years, in accordance with the currently accepted thresholds for senescence [25], with no gender limitation. No participant was included who had engaged in structured training in the previous 3 months. We excluded the data from participants who had any disorders.
- Intervention and comparison: The included studies had to compare a BFR resistance training against (1) an active HL control group in which resistance training was performed without BFR at high intensities (≥70% of 1RM) or (2) an active LL control group in which resistance training was performed at 20–40% of 1RM without BFR. The minimum training period was 3 weeks, given that this is the minimum period for physiological adaptations to occur with BFR training [26]. BFR interventions on the lower and/or upper limb strength were included.
- Outcomes: The outcomes of interest were the muscle strength and hypertrophy; thus, all the included studies had to assess at least one of these factors. Muscle strength was assessed using maximal dynamic strength by 1RM tests (found directly or reliably estimated from 10RM [27]), measuring the maximal isometric and isokinetic strength. These measures have been found to be valid and reliable in the evaluation of muscle strength in older adults [28,29,30]. The muscle hypertrophy was evaluated by the muscle cross-sectional area, estimated muscle mass, muscle thickness, and body perimeters, all having proven to be valid and reliable methods [31,32,33,34]. These measurements could be performed anywhere on both the upper and lower limb musculature.
- Study design: Only randomized controlled trials and crossover trials were included. Articles were included if they were published in English, Spanish, or Portuguese.
2.2. Search Strategy
2.3. Selection Criteria and Data Extraction
2.4. Methodological Quality and Risk of Bias Assessment
2.5. Qualitative Analysis
2.6. Data Analysis
3. Results
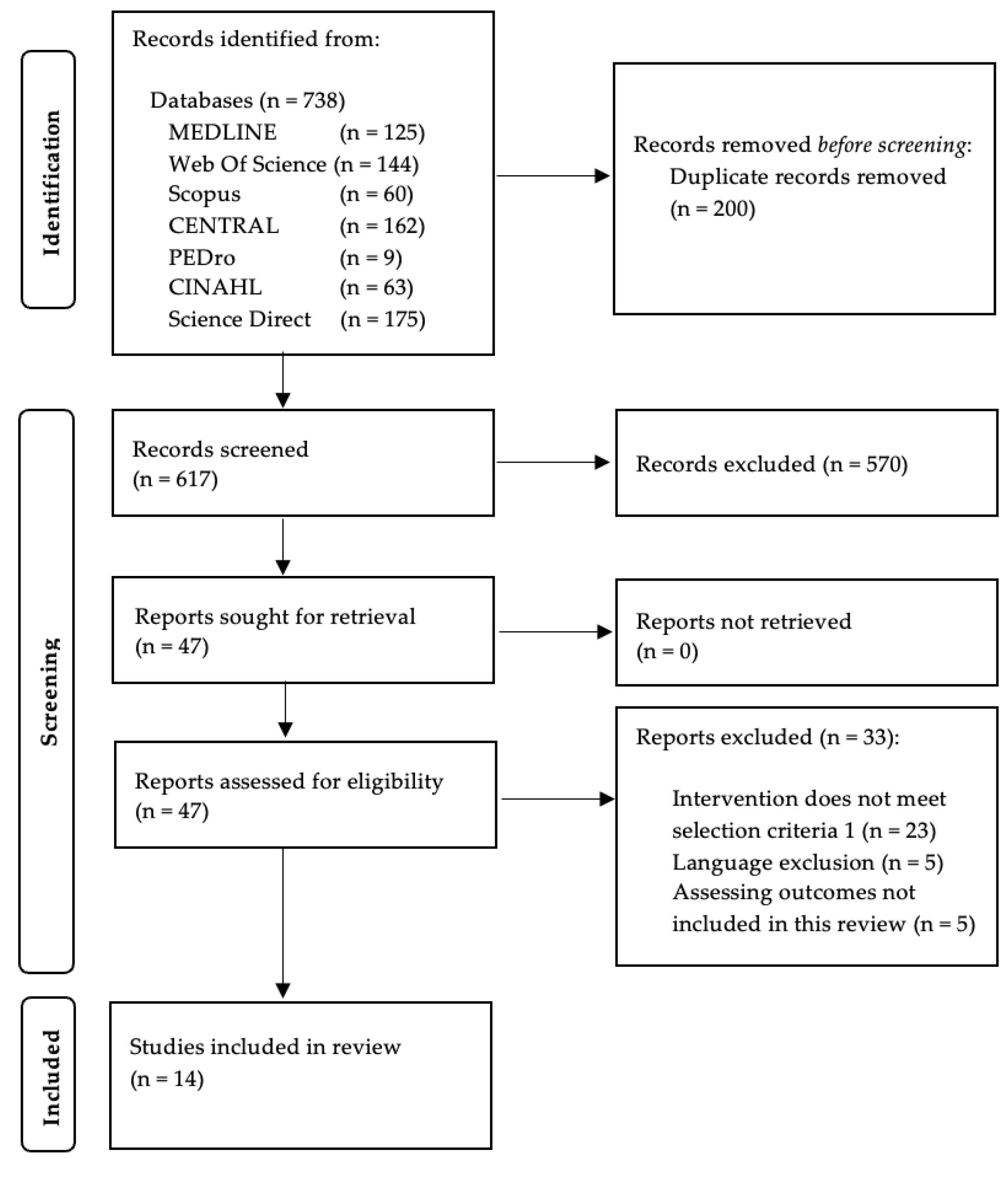
3.1. Study Selection
3.2. Characteristics of the Included Studies
3.3. Methodological Quality and Risk of Bias of the Included Studies
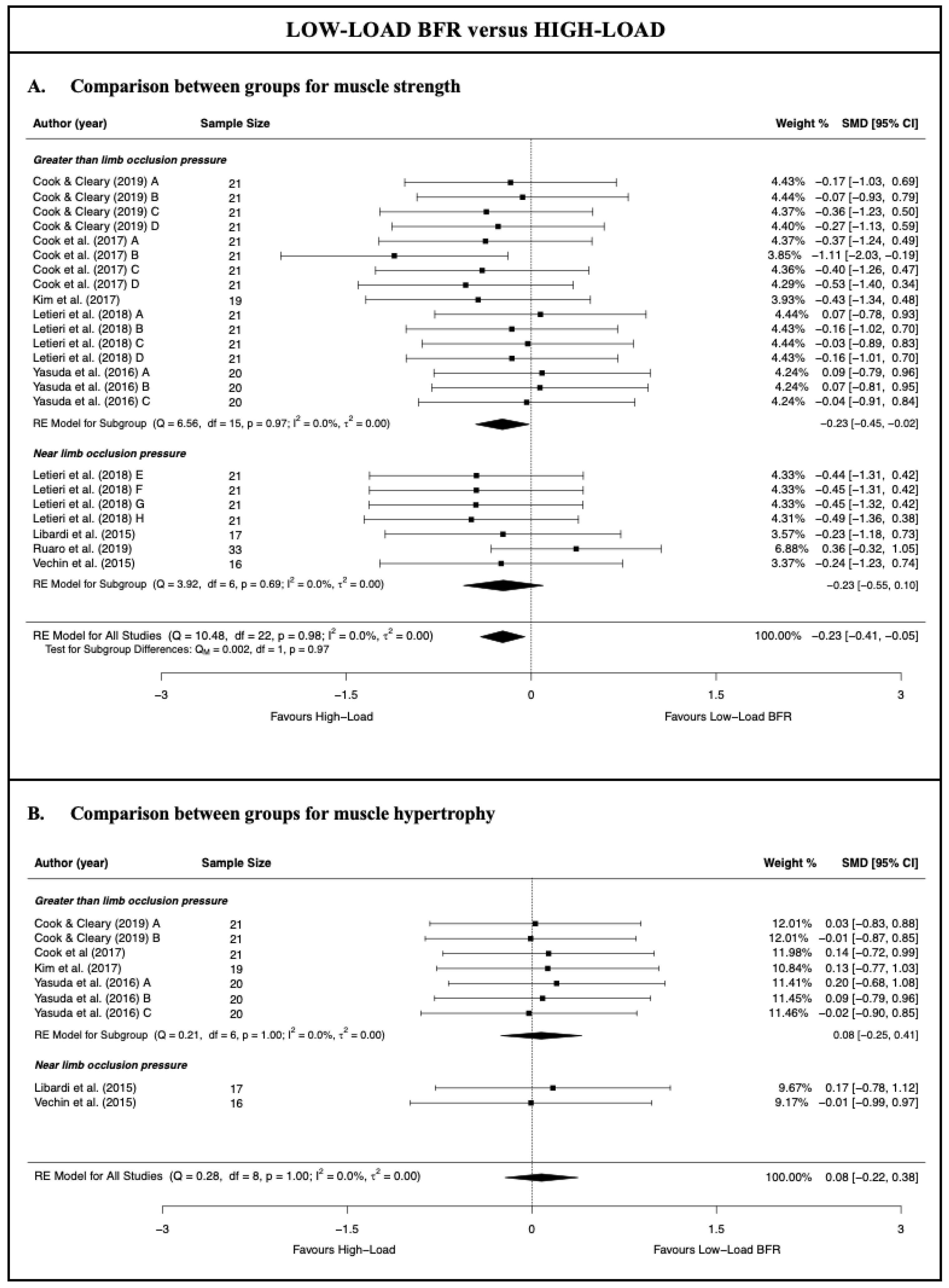
3.4. Low-Load Blood Flow Restriction Training versus High-Load Resistance Training
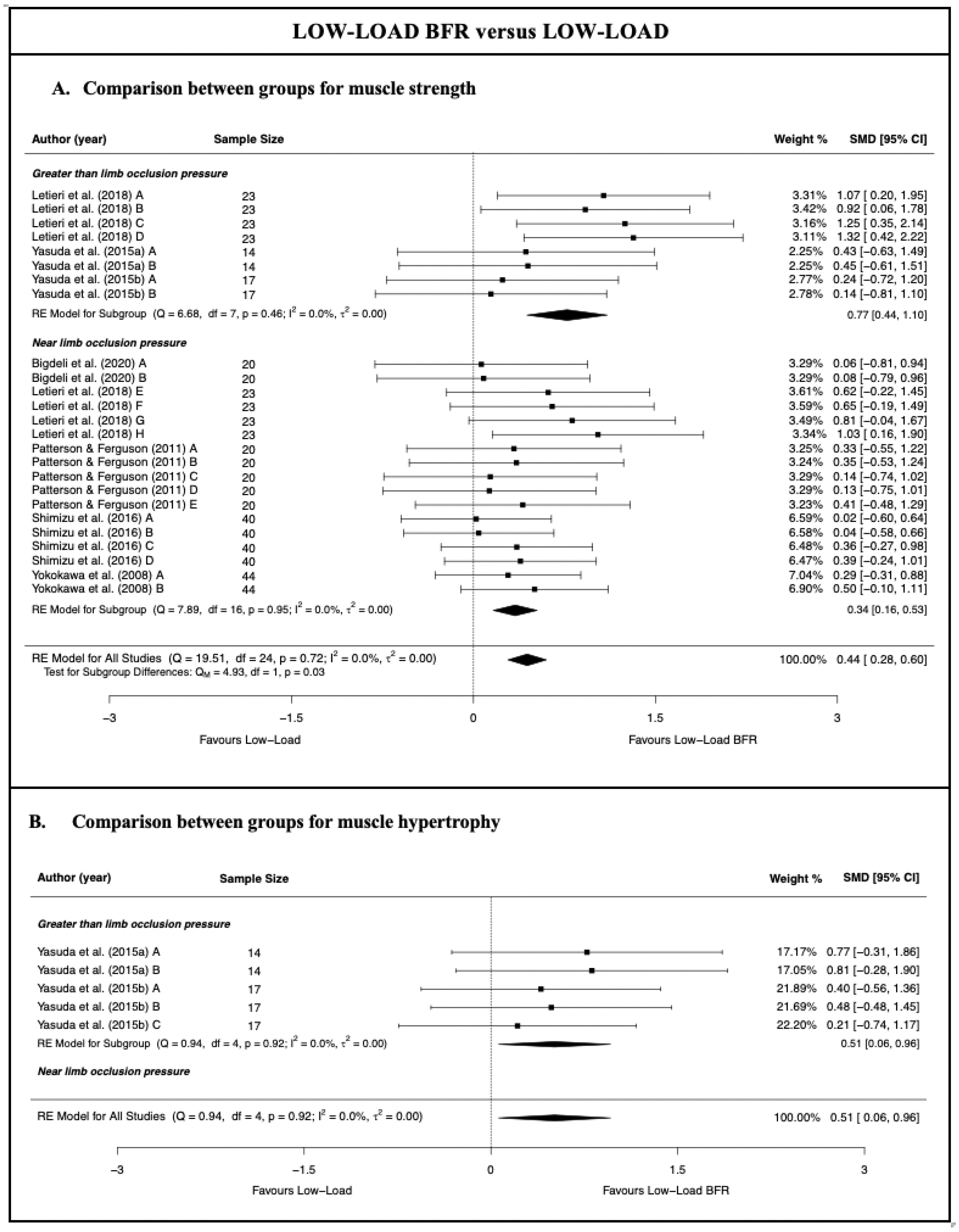
3.5. Low-Load Blood Flow Restriction versus Traditional Low-Load Resistance Training
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Ageing and Health; World Health Organization: Geneva, Switzerland, 2021.
- Janssen, I.; Heymsfield, S.B.; Ross, R. Low relative skeletal muscle mass (sarcopenia) in older persons is associated with functional impairment and physical disability. J. Am. Geriatr. Soc. 2002, 50, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef] [PubMed]
- McPhee, J.S.; French, D.P.; Jackson, D.; Nazroo, J.; Pendleton, N.; Degens, H. Physical activity in older age: Perspectives for healthy ageing and frailty. Biogerontology 2016, 17, 567–580. [Google Scholar] [CrossRef] [PubMed]
- Ryan, D.J.; Stebbings, G.K.; Onambele, G.L. The emergence of sedentary behaviour physiology and its effects on the cardiometabolic profile in young and older adults. Age 2015, 37, 1–11. [Google Scholar] [CrossRef]
- Grgic, J.; Garofolini, A.; Orazem, J.; Sabol, F.; Schoenfeld, B.J.; Pedisic, Z. Effects of Resistance Training on Muscle Size and Strength in Very Elderly Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Sport Med. 2020, 50, 1983–1999. [Google Scholar] [CrossRef]
- Fragala, M.S.; Cadore, E.L.; Dorgo, S.; Izquierdo, M.; Kraemer, W.J.; Peterson, M.D.; Ryan, E.D. Resistance Training for Older Adults: Position Statement From the National Strength and Conditioning Association. J. Strength Cond. Res. 2019, 33, 2019–2052. [Google Scholar] [CrossRef]
- Papa, E.V.; Dong, X.; Hassan, M. Resistance training for activity limitations in older adults with skeletal muscle function deficits: A systematic review. Clin. Interv. Aging 2017, 12, 955–961. [Google Scholar] [CrossRef]
- Csapo, R.; Alegre, L.M. Effects of resistance training with moderate vs heavy loads on muscle mass and strength in the elderly: A meta-analysis. Scand. J. Med. Sci. Sports 2016, 26, 995–1006. [Google Scholar] [CrossRef]
- Borde, R.; Hortobágyi, T.; Granacher, U. Dose-Response Relationships of Resistance Training in Healthy Old Adults: A Systematic Review and Meta-Analysis. Sports Med. 2015, 45, 1693–1720. [Google Scholar] [CrossRef]
- Steib, S.; Schoene, D.; Pfeifer, K. Dose-response relationship of resistance training in older adults: A meta-analysis. Med. Sci. Sports Exerc. 2010, 42, 902–914. [Google Scholar] [CrossRef]
- Valenzuela, T. Efficacy of progressive resistance training interventions in older adults in nursing homes: A systematic review. J. Am. Med. Dir. Assoc. 2012, 13, 418–428. [Google Scholar] [CrossRef]
- Kumar, V.; Selby, A.; Rankin, D.; Patel, R.; Atherton, P.; Hildebrandt, W.; Williams, J.; Smith, K.; Seynnes, O.; Hiscock, N.; et al. Age-related differences in the dose-response relationship of muscle protein synthesis to resistance exercise in young and old men. J. Physiol. 2009, 587, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, D.S.; Bailey, L.; Wilk, K.E.; Mangine, R.E.; Head, P.; Grindstaff, T.L.; Morrison, D.S. Blood Flow Restriction Training. J. Athl. Train. 2021, 56, 937–944. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Yasuda, T.; Midorikawa, T.; Sato, Y.; Kearns, C.F.; Inoue, K.; Koizumi, K.; Ishii, N. Skeletal muscle size and circulating IGF-1 are increased after two weeks of twice daily “KAATSU” resistance training. Int. J. KAATSU Train. Res. 2005, 1, 6–12. [Google Scholar] [CrossRef]
- Takarada, Y.; Tsuruta, T.; Ishii, N. Cooperative effects of exercise and occlusive stimuli on muscular function in low-intensity resistance exercise with moderate vascular occlusion. Jpn. J. Physiol. 2004, 54, 585–592. [Google Scholar] [CrossRef]
- Centner, C.; Wiegel, P.; Gollhofer, A.; König, D.; Koenig, D.; König, D. Effects of Blood Flow Restriction Training on Muscular Strength and Hypertrophy in Older Individuals: A Systematic Review and Meta-Analysis. Sports Med. 2019, 49, 95–108. [Google Scholar] [CrossRef]
- Zhang, T.; Wang, X.; Wang, J. Effect of blood flow restriction combined with low-intensity training on the lower limbs muscle strength and function in older adults: A meta-analysis. Exp. Gerontol. 2022, 164, 111827. [Google Scholar] [CrossRef]
- Rodrigo-Mallorca, D.; Loaiza-Betancur, A.F.; Monteagudo, P.; Blasco-Lafarga, C.; Chulvi-Medrano, I. Resistance Training with Blood Flow Restriction Compared to Traditional Resistance Training on Strength and Muscle Mass in Non-Active Older Adults: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Heal. 2021, 18, 11441. [Google Scholar] [CrossRef]
- Loenneke, J.P.; Kim, D.; Fahs, C.A.; Thiebaud, R.S.; Abe, T.; Larson, R.D.; Bemben, D.A.; Bemben, M.G. The effects of resistance exercise with and without different degrees of blood-flow restriction on perceptual responses. J. Sports Sci. 2015, 33, 1472–1479. [Google Scholar] [CrossRef]
- Yasuda, T.; Abe, T.; Brechue, W.F.; Iida, H.; Takano, H.; Meguro, K.; Kurano, M.; Fujita, S.; Nakajima, T. Venous blood gas and metabolite response to low-intensity muscle contractions with external limb compression. Metabolism 2010, 59, 1510–1519. [Google Scholar] [CrossRef]
- Kim, D.; Loenneke, J.; Thiebaud, R.; Abe, T.; Bemben, M. The acute muscular effects of cycling with and without different degrees of blood flow restriction. Acta Physiol. Hung. 2015, 102, 428–441. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [PubMed]
- Scherbov, S.; Sanderson, W. New Measures of Population Ageing; United Nations: Rome, Italy, 2020; pp. 1–90. [Google Scholar]
- Hill, E.C.; Housh, T.J.; Keller, J.L.; Smith, C.M.; Anders, J.V.; Schmidt, R.J.; Johnson, G.O.; Cramer, J.T. Patterns of responses and time-course of changes in muscle size and strength during low-load blood flow restriction resistance training in women. Eur. J. Appl. Physiol. 2021, 121, 1473–1485. [Google Scholar] [CrossRef] [PubMed]
- Brzycki, M. Strength Testing—Predicting a One-Rep Max from Reps-to-Fatigue. J. Phys. Educ. Recreat. Dance 1993, 64, 88–90. [Google Scholar] [CrossRef]
- Letieri, R.V.; Teixeira, A.M.; Furtado, G.E.; Lamboglia, C.G.; Rees, J.L.; Gomes, B.B. Effect of 16 weeks of resistance exercise and detraining comparing two methods of blood flow restriction in muscle strength of healthy older women: A randomized controlled trial. Exp. Gerontol. 2018, 114, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Capranica, L.; Battenti, M.; Demarie, S.; Figura, F. Reliability of isokinetic knee extension and flexion strength testing in elderly women. J. Sports Med. Phys. Fit. 1998, 38, 169–176. [Google Scholar]
- Katoh, M.; Isozaki, K. Reliability of Isometric Knee Extension Muscle Strength Measurements of Healthy Elderly Subjects Made with a Hand-held Dynamometer and a Belt. J. Phys. Ther. Sci. 2014, 26, 1855–1859. [Google Scholar] [CrossRef]
- Wu, Y.F.; Zhang, X.Y.; Ren, S.; Yu, Y.X.; Chang, C.Q. Measurement and evaluation of the quadriceps muscle mass in young men based on magnetic resonance imaging. J. Peking Univ. Health Sci. 2021, 53, 843–849. [Google Scholar] [CrossRef]
- Sanada, K.; Kearns, C.F.; Midorikawa, T.; Abe, T. Prediction and validation of total and regional skeletal muscle mass by ultrasound in Japanese adults. Eur. J. Appl. Physiol. 2006, 96, 24–31. [Google Scholar] [CrossRef]
- Meza-Valderrama, D.; Sánchez- Rodríguez, D.; Perkisas, S.; Duran, X.; Bastijns, S.; Dávalos-Yerovi, V.; Da Costa, E.; Marco, E. The feasibility and reliability of measuring forearm muscle thickness by ultrasound in a geriatric inpatient setting: A cross-sectional pilot study. BMC Geriatr. 2022, 22, 137. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.; Spenst, L.; Drinkwater, D.; Clarys, J. Anthropometric estimation of muscle mass in men. Med. Sci. Sports Exerc. 1990, 22, 729–733. [Google Scholar] [CrossRef] [PubMed]
- Russell-Rose, T.; Chamberlain, J. Expert Search Strategies: The Information Retrieval Practices of Healthcare Information Professionals. JMIR Med. Inform. 2017, 5, e33. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Sally, G. Cochrane Handbook for Systematic Reviews of Interventions, version 5.1.0; Cochrane Collaboration: Melbourne, Australia, 2012; pp. 199–255. [Google Scholar]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro Scale for Rating Quality of Randomized Controlled Trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Bhogal, S.K.; Teasell, R.W.; Foley, N.C.; Speechley, M.R. The PEDro scale provides a more comprehensive measure of methodological quality than the Jadad scale in stroke rehabilitation literature. J. Clin. Epidemiol. 2005, 58, 668–673. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Andrews, J.; Guyatt, G.; Oxman, A.D.; Alderson, P.; Dahm, P.; Falck-Ytter, Y.; Nasser, M.; Meerpohl, J.; Post, P.N.; Kunz, R.; et al. GRADE guidelines: 14. Going from evidence to recommendations: The significance and presentation of recommendations. J. Clin. Epidemiol. 2013, 66, 719–725. [Google Scholar] [CrossRef]
- Liu, Y.; Jiang, N.; Pang, F.; Chen, T. Resistance Training with Blood Flow Restriction on Vascular Function: A Meta-analysis. Int. J. Sports Med. 2021, 42, 577–587. [Google Scholar] [CrossRef]
- Hagger, M.S. Meta-analysis in sport and exercise research: Review, recent developments, and recommendations. Eur. J. Sport Sci. 2006, 6, 103–115. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Bown, M.J.; Sutton, A.J. Quality Control in Systematic Reviews and Meta-analyses. Eur. J. Vasc. Endovasc. Surg. 2010, 40, 669–677. [Google Scholar] [CrossRef] [PubMed]
- Viechtbauer, W.; Cheung, M.W.-L. Outlier and influence diagnostics for meta-analysis. Res. Synth. Methods 2010, 1, 112–125. [Google Scholar] [CrossRef] [PubMed]
- Riley, R.D.; Sutton, A.J.; Abrams, K.R.; Lambert, P.C. Sensitivity analyses allowed more appropriate and reliable meta-analysis conclusions for multiple outcomes when missing data was present. J. Clin. Epidemiol. 2004, 57, 911–924. [Google Scholar] [CrossRef] [PubMed]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Egger, M. Funnel plots for detecting bias in meta-analysis. J. Clin. Epidemiol. 2001, 54, 1046–1055. [Google Scholar] [CrossRef]
- Yasuda, T.; Fukumura, K.; Tomaru, T.; Nakajima, T. Thigh muscle size and vascular function after blood flow-restricted elastic band training in older women. Oncotarget 2016, 7, 33595–33607. [Google Scholar] [CrossRef]
- Vechin, F.C.; Libardi, C.A.; Conceição, M.S.; Damas, F.R.; Lixandrão, M.E.; Berton, R.P.B.; Tricoli, V.A.; Roschel, H.A.; Cavaglieri, C.R.; Chacon-Mikahil, M.P.T.; et al. Comparisons between low-intensity resistance training with blood flow restriction and high-intensity resistance training on quadriceps muscle mass and strength in elderly. J. Strength Cond. Res. 2015, 29, 1071–1076. [Google Scholar] [CrossRef]
- Ruaro, M.F.; Santana, J.O.; Gusmao, N.; De Franca, E.; Carvalho, B.N.; Farinazo, K.B.; Bonorino, S.L.; Corralo, V.; Antonio de Sá, C.; Caperuto, E.C. Effects of strength training with and without blood flow restriction on quality of life in elderly women. J. Phys. Educ. Sport 2019, 19, 531–539. [Google Scholar]
- Kim, J.; Lang, J.A.; Pilania, N.; Franke, W.D. Effects of blood flow restricted exercise training on muscular strength and blood flow in older adults. Exp. Gerontol. 2017, 99, 127–132. [Google Scholar] [CrossRef]
- Cook, S.B.; LaRoche, D.P.; Villa, M.R.; Barile, H.; Manini, T.M. Blood flow restricted resistance training in older adults at risk of mobility limitations. Exp. Gerontol. 2017, 99, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Cook, S.B.; Cleary, C.J. Progression of blood flow restricted resistance training in older adults at risk of mobility limitations. Front. Physiol. 2019, 10, 738. [Google Scholar] [CrossRef] [PubMed]
- Libardi, C.A.; Chacon-Mikahil, M.P.T.; Cavaglieri, C.R.; Tricoli, V.; Roschel, H.; Vechin, F.C.; Conceição, M.S.; Ugrinowitsch, C. Effect of concurrent training with blood flow restriction in the elderly. Front. Physiol. 2015, 36, 395–399. [Google Scholar] [CrossRef] [PubMed]
- Bigdeli, S.; Dehghaniyan, M.H.; Amani-Shalamzari, S.; Rajabi, H.; Gahreman, D.E. Functional training with blood occlusion influences muscle quality indices in older adults. Arch. Gerontol. Geriatr. 2020, 90, 104110. [Google Scholar] [CrossRef] [PubMed]
- Patterson, S.D.; Ferguson, R.A. Enhancing strength and postocclusive calf blood flow in older people with training with blood-flow restriction. J. Aging Phys. Act. 2011, 19, 201–213. [Google Scholar] [CrossRef]
- Shimizu, R.; Hotta, K.; Yamamoto, S.; Matsumoto, T.; Kamiya, K.; Kato, M.; Hamazaki, N.; Kamekawa, D.; Akiyama, A.; Kamada, Y.; et al. Low-intensity resistance training with blood flow restriction improves vascular endothelial function and peripheral blood circulation in healthy elderly people. Eur. J. Appl. Physiol. 2016, 116, 749–757. [Google Scholar] [CrossRef]
- Yasuda, T.; Fukumura, K.; Iida, H.; Nakajima, T. Effects of detraining after blood flow-restricted low-load elastic band training on muscle size and arterial stiffness in older women. Springerplus 2015, 4, 348. [Google Scholar] [CrossRef]
- Yasuda, T.; Fukumura, K.; Uchida, Y.; Koshi, H.; Iida, H.; Masamune, K.; Yamasoba, T.; Sato, Y.; Nakajima, T. Effects of Low-Load, Elastic Band Resistance Training Combined With Blood Flow Restriction on Muscle Size and Arterial Stiffness in Older Adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2015, 70, 950–958. [Google Scholar] [CrossRef]
- Yokokawa, Y.; Hongo, M.; Urayama, H.; Nishimura, T.; Kai, I. Effects of low-intensity resistance exercise with vascular occlusion on physical function in healthy elderly people. PubMed Biosci. Trends 2008, 2, 117–123. [Google Scholar]
- Barcot, O.; Boric, M.; Dosenovic, S.; Poklepovic Pericic, T.; Cavar, M.; Puljak, L. Risk of bias assessments for blinding of participants and personnel in Cochrane reviews were frequently inadequate. J. Clin. Epidemiol. 2019, 113, 104–113. [Google Scholar] [CrossRef]
- Buckner, S.L.; Dankel, S.J.; Mattocks, K.T.; Jessee, M.B.; Mouser, J.G.; Counts, B.R.; Loenneke, J.P. The problem Of muscle hypertrophy: Revisited. Muscle Nerve 2016, 54, 1012–1014. [Google Scholar] [CrossRef] [PubMed]
- Lixandrão, M.E.; Ugrinowitsch, C.; Berton, R.; Vechin, F.C.; Conceição, M.S.; Damas, F.; Libardi, C.A.; Roschel, H. Magnitude of Muscle Strength and Mass Adaptations Between High-Load Resistance Training Versus Low-Load Resistance Training Associated with Blood-Flow Restriction: A Systematic Review and Meta-Analysis. Sports Med. 2018, 48, 361–378. [Google Scholar] [CrossRef] [PubMed]
- Pearson, S.J.; Hussain, S.R. A Review on the Mechanisms of Blood-Flow Restriction Resistance Training-Induced Muscle Hypertrophy. Sports Med. 2015, 45, 187–200. [Google Scholar] [CrossRef]
- Adams, G.R. Invited Review: Autocrine/paracrine IGF-I and skeletal muscle adaptation. J. Appl. Physiol. 2002, 93, 1159–1167. [Google Scholar] [CrossRef] [PubMed]
- Cook, S.B.; Murphy, B.G.; Labarbera, K.E. Neuromuscular Function after a Bout of Low-Load Blood Flow–Restricted Exercise. Med. Sci. Sports Exerc. 2013, 45, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Narici, M.V.; Roi, G.S.; Landoni, L.; Minetti, A.E.; Cerretelli, P. Changes in force, cross-sectional area and neural activation during strength training and detraining of the human quadriceps. Eur. J. Appl. Physiol. Occup. Physiol. 1989, 59, 310–319. [Google Scholar] [CrossRef]
- Häkkinen, K.; Alen, M.; Kallinen, M.; Newton, R.U.; Kraemer, W.J. Neuromuscular adaptation during prolonged strength training, detraining and re-strength-training in middle-aged and elderly people. Eur. J. Appl. Physiol. 2000, 83, 51–62. [Google Scholar] [CrossRef]
- Bordessa, J.M.; Hearn, M.C.; Reinfeldt, A.E.; Smith, T.A.; Baweja, H.S.; Levy, S.S.; Rosenthal, M.D. Comparison of blood flow restriction devices and their effect on quadriceps muscle activation. Phys. Ther. Sport 2021, 49, 90–97. [Google Scholar] [CrossRef]
- Hughes, L.; Paton, B.; Rosenblatt, B.; Gissane, C.; Patterson, S.D. Blood flow restriction training in clinical musculoskeletal rehabilitation: A systematic review and meta-analysis. Br. J. Sports Med. 2017, 51, 1003–1011. [Google Scholar] [CrossRef]
- Fry, C.S.; Glynn, E.L.; Drummond, M.J.; Timmerman, K.L.; Fujita, S.; Abe, T.; Dhanani, S.; Volpi, E.; Rasmussen, B. Blood flow restriction exercise stimulates mTORC1 signaling and muscle protein synthesis in older men. J. Appl. Physiol. 2010, 108, 1199–1209. [Google Scholar] [CrossRef] [PubMed]
- Takarada, Y.; Nakamura, Y.; Aruga, S.; Onda, T.; Miyazaki, S.; Ishii, N. Rapid increase in plasma growth hormone after low-intensity resistance exercise with vascular occlusion. J. Appl. Physiol. 2000, 88, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Loenneke, J.P.; Fahs, C.A.; Rossow, L.M.; Abe, T.; Bemben, M.G. The anabolic benefits of venous blood flow restriction training may be induced by muscle cell swelling. Med. Hypotheses 2012, 78, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Schoenfeld, B.J. Does exercise-induced muscle damage play a role in skeletal muscle hypertrophy? J. Strength Cond. Res. 2012, 26, 1441–1453. [Google Scholar] [CrossRef] [PubMed]
- Barili, A.; da Corralo, V.S.; Cardoso, A.M.; Mânica, A.; da Bonadiman, B.S.R.; Bagatini, M.D.; Da Silva-Grigoletto, M.E.; de Oliveira, G.G.; De Sá, C.A. Acute responses of hemodynamic and oxidative stress parameters to aerobic exercise with blood flow restriction in hypertensive elderly women. Mol. Biol. Rep. 2018, 45, 1099–1109. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.-H.; Sohn, S.-M.; You, H.-J.; Yoon, E.-S.; Lee, B.-I.; Park, S.-H.; Kim, D.-W. Use of a biopsy punch for end-to-side anastomosis in free-tissue transfer. J. Plast. Surg. Hand Surg. 2020, 54, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Loenneke, J.P.; Kim, D.; Fahs, C.A.; Thiebaud, R.S.; Abe, T.; Larson, R.D.; Bemben, D.A.; Bemben, M.G. Effects of exercise with and without different degrees of blood flow restriction on torque and muscle activation. Muscle Nerve 2015, 51, 713–721. [Google Scholar] [CrossRef]
- Ozaki, H.; Loenneke, J.P.; Abe, T. Blood flow-restricted walking in older women: Does the acute hormonal response associate with muscle hypertrophy? Clin. Physiol. Funct. Imaging 2017, 37, 379–383. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author, Year and Design | Sample Characteristics | Intervention Groups | Resistance Training Protocol | Outcomes | Results |
|---|---|---|---|---|---|
| Bigdeli et al., 2020 [57] RCT | N = 20 Age: 67.7 ± 5.8 years | LL-BFR training (25–35% 1RM) (N = 10)
(25–35% 1RM) (N = 10) | Exercise mode 11 functional upper and lower limb exercises Volume (set × rep) 2–4 × 10 Frequency 6 weeks; 3 days/week | Assessments Pre–post training Muscle strength 1RM knee extension/chest press | Muscle strength No differences were observed in muscle strength between LL-BFR training and LL resistance training at 6 weeks. |
| Cook et al., 2017 [54] RCT | N = 24 Age: 75.6 years, 95% CI: [73.4–78.5] | LL-BFR training (30% 1RM) (N = 12)
(70% 1RM) (N = 12) | Exercise mode Leg extension, leg curl, leg press Volume (set × rep) 1–3 × failure Frequency 12 weeks: 2 days/week | Assessments Pre-6 weeks-post training Muscle strength 1RM leg extension/leg curl/leg press MVIC knee extension (60°) Muscle hypertrophy Quadriceps CSA | Muscle strength At 6 weeks, HL resistance training showed significant improvements in 1RM leg press and MVIC knee extension compared to LL-BFR training. At 12 weeks, HL resistance training only showed significant improvements for 1RM knee extension in favour of LL-BFR training. Muscle hypertrophy No significant differences were detected between LL-BFR training and HL resistance training at 12 weeks. |
| Cook and Cleary 2019 [55] RCT | N = 21 Age: 76.35 ± 7.78 years | LL-BFR training (30% 1RM) (N = 10)
(70% 1RM) (N = 11) | Exercise mode Leg flexion and extension, leg curl Volume (set × rep) 1–3 × failure Frequency 12 weeks: 2 days/week | Assessments Pre–post training Muscle strength 10RM knee flexion/extension MVIC knee flexion/extension Muscle hypertrophy Quadriceps CSA Hamstrings CSA | Muscle strength LL-BFR training only obtained significant improvements in 10RM knee extension compared to HL resistance training. Muscle hypertrophy No significant differences were observed in muscle CSA between groups at 12 weeks. |
| Kim et al., 2017 [53] RCT | N = 19 Age: 62.74 ± 1.01 years | LL-BFR training (20% MVC) (N = 9)
(75% MVC) (N = 10) | Exercise mode Isometric handgrip contractions Volume (set × rep) 3 × failure Frequency 4 weeks; 3 days/week | Assessments Pre–post training Muscle strength MVIC handgrip Muscle hypertrophy Forearm girth | Muscle strength No significant differences were observed in muscle strength between LL-BFR training and HL resistance training at 4 weeks. Muscle hypertrophy No significant differences were observed in muscle hypertrophy between LL-BFR training and HL resistance training at 4 weeks. |
| Letieri et al., 2018 [28] RCT | N = 44 Age: 68.8 ± 5.09 years | LL-BFR training high pressure (20–30% 1RM) (N = 11)
(20–30% 1RM (N = 11)
(70–80% 1RM) (N = 10) LL resistance training (20–30% 1RM) (N = 12) | Exercise mode Squat, leg press, knee extension and leg curl Volume (set × rep) LL-BFR: 3–4 × 15–30 LL: 3–4 × 15–30 HL: 3–4 × 6–8 Frequency 16 weeks; 3 days/week | Assessments Pre–post training and 6 weeks detraining Muscle strength Isokinetic peak torque of knee flexion/extension (60°/seg) | Muscle strength All groups presented greater increases in isokinetic peak torque of knee flexion/extension compared to LL resistance training at 16 weeks. No significant differences were observed in muscle strength between LL-BFR training either with high or low pressure and HL resistance training at 16 weeks. There were statistically significant detriments in muscle strength in the LL-BFR training with high pressure and HL resistance training group at 6 weeks detraining. |
| Libardi et al., 2015 [56] RCT | N = 18 Age: 64.7 ± 4.1 years | LL-BFR training (20–30% 1RM) (N = 10)
(70–80% 1RM) (N = 8) | Exercise mode Leg press Volume (set × rep) LL-BFR: 3 × 15 HL: 4 × 10 Frequency 12 weeks; 2 days/week | Assessments Pre–post training Muscle strength 1RM leg press Muscle hypertrophy Quadriceps CSA | Muscle strength No significant differences were observed in muscle strength between LL-BFR training and HL resistance training at 12 weeks. Muscle hypertrophy No significant differences were observed in muscle hypertrophy between LL-BFR training and HL resistance training at 12 weeks. |
| Patterson and Ferguson 2011 [58] Crossover trial | N = 10 Age: 67 ± 3 years | LL-BFR training (25% 1RM) (N = 10)
(25% 1RM) (N = 10) | Exercise mode Plantar flexion Volume (set × rep) 3 × failure Frequency 4 weeks; 3 days/week | Assessments Pre–post training Muscle strength MVIC plantar flexion (90°) Isokinetic peak torque of plantar flexion (30, 60 and 120°/s) 1RM plantar flexion | Muscle strength The LL-BFR leg showed a significant increase in muscle strength except for the isokinetic peak torque of plantar flexion at 60° and 120°/s. |
| Ruaro et al., 2019 [52] RCT | N = 33 Age: 65.94 ± 4.59 years | LL-BFR training (40% 1RM) (N = 16)
(70% 1RM) (N = 17) | Exercise mode Wrist flexion Volume (set × rep) 3 × 15 Frequency 14 weeks; 2 days/week | Assessments Pre–post training Muscle strength 1RM wrist flexion | Muscle strength LL-BFR training showed a significant improvement in muscle strength compared to HL resistance training. |
| Shimizu et al., 2016 [59] RCT | N = 40 Age: 71 ± 4 years | LL-BFR training (20% 1RM) (N = 20)
(20% 1RM) (N = 20) | Exercise mode Leg extension, leg press, rowing and chest press Volume (set × rep) 3 × 20 Frequency 4 weeks; 3 days/week | Assessments Pre–post training Muscle strength 1RM leg extension/leg press/rowing/chest press | Muscle strength No significant differences were observed in muscle strength between LL-BFR training and LL resistance training at 4 weeks. |
| Vechin et al., 2015 [51] RCT | N = 16 Age: 64.04 ± 3.81years | LL-BFR training (20–30% 1RM) (N = 8)
(70–80% 1RM) (N = 8) | Exercise mode Leg press Volume (set × rep) LL-BFR: 4 × 30–15 HL: 4 × 10 Frequency 12 weeks; 2 days/week | Assessments Pre–post training Muscle strength 1RM leg press Muscle hypertrophy Quadriceps CSA | Muscle strength HL resistance training obtained significant increases in 1RM leg press compared to LL-BFR training at 12 weeks. Muscle hypertrophy No significant differences in muscle hypertrophy between LL-BFR training and HL resistance training were observed at 12 weeks. |
| Yasuda et al., 2016 [50] RCT | N = 20 Age: 71.06 ± 6.61 years | LL-BFR training (35–45% 1RM) (N = 10)
(70–90% 1RM) (N = 10) | Exercise mode Squat and knee extension with elastic bands Volume (set × rep) LL-BFR: 3 × 30–15 HL: 3 × 12–13 Frequency 12 weeks; 2 days/week | Assessments Pre–post training Muscle strength 1RM leg press/knee extension MVIC knee flexion/extension (80°) Muscle hypertrophy Quadriceps/adductors/hamstrings/gluteus maximus CSA Mid-thigh and lower leg girth | Muscle strength There were only significant increases in the LL-BFR training regarding the MVIC knee extension compared to the HL resistance training at 12 weeks. Muscle hypertrophy There were only significant increases in the LL-BFR training regarding the quadriceps CSA compared to the HL resistance training at 12 weeks. |
| Yasuda et al., 2015a [60] RCT | N = 14 Age: 69.5 ± 7.06 years | LL-BFR training (26–30% 1RM) (N = 7)
(28–30% 1RM) (N = 7) | Exercise mode Arm curl and triceps press down with elastic bands Volume (set × rep) LL-BFR: 4 × 15–30 LL: 4 × 15–30 Frequency 12 weeks; 2 days/week | Assessments Pre–post training and 12-week detraining Muscle strength MVIC elbow flexion/extension (90°) Muscle hypertrophy Elbow flexors/extensors CSA | Muscle strength LL-BFR training showed significant increase in MVIC elbow extension, but not in flexion compared to LL resistance training at 12 weeks. No detraining appears in the MVIC elbow extension at 12 weeks post-intervention. Muscle hypertrophy LL-BFR training showed a significant improvement in both CSA outcomes compared to LL resistance training. No detraining appears in the elbow flexors CSA at 12 weeks post-intervention. |
| Yasuda et al., 2015b [61] RCT | N = 17 Age: 70.12 ± 5.95 years | LL-BFR training (26–30% 1RM) (N = 9)
(28–30% 1RM) (N = 8) | Exercise mode Arm curl and triceps press down with elastic bands Volume (set × rep) LL-BFR: 4 × 15–30 LL: 4 × 15–30 Frequency 12 weeks; 2 days/week | Assessments Pre–post training Muscle strength MVIC elbow flexion/extension (90°) Muscle hypertrophy Elbow flexors/extensors CSA - Upper arm girth | Muscle strength LL-BFR training showed a significant improvement in muscle strength compared to LL resistance training. Muscle hypertrophy LL-BFR training showed a significant improvement in both muscle hypertrophy outcomes compared to LL resistance training. |
| Yokokawa et al., 2008 [62] RCT | N = 44 Age: ≥65 years (~71.61 ± 4.34 years) | LL-BFR training (N = 19)
(N = 25) | Exercise mode Half squats, forward lunges, calf raises, knee lifts, crunches, knee flexion and extension Exercises to enhance posture and dynamic stability Volume 90 min/week Frequency LL-BFR: 8 weeks; 2 days/week LL: 8 weeks; 1 days/week | Assessments Pre–post training Muscle strength MVIC knee extension (90°)/handgrip | Muscle strength No significant differences were observed between LL-BFR training and LL resistance training at 8 weeks. |
| Study | Random Allocation | Concealed Allocation | Groups Similar at Baseline | Participant Blinding | Therapist Blinding | Assessor Blinding | <15% Dropouts | Intention- to-Treat Analysis | Intergroup Difference Reported | Point Estimate and Variability Reported | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Bigdeli et al., 2020 [57] | Y | N | Y | N | N | Y | Y | Y | Y | Y | 7 |
| Cook and Cleary 2019 [55] | Y | N | Y | N | N | N | Y | Y | Y | Y | 6 |
| Cook et al., 2017 [54] | Y | N | Y | N | N | Y | Y | N | Y | Y | 6 |
| Kim et al., 2017 [53] | Y | N | Y | N | N | N | N | N | Y | Y | 4 |
| Letieri et al., 2018 [28] | Y | N | Y | N | N | Y | Y | N | Y | Y | 6 |
| Libardi et al., 2015 [56] | Y | N | Y | N | N | N | Y | Y | Y | Y | 6 |
| Patterson and Ferguson 2011 [58] | N | N | Y | N | N | N | Y | Y | Y | Y | 5 |
| Ruaro et al., 2019 [52] | Y | Y | Y | N | N | N | N | N | Y | Y | 5 |
| Shimizu et al., 2016 [59] | Y | N | Y | N | N | N | Y | Y | Y | Y | 6 |
| Vechin et al., 2015 [51] | Y | N | Y | N | N | N | N | N | Y | Y | 4 |
| Yasuda et al., 2016 [50] | Y | N | Y | N | N | N | Y | Y | Y | Y | 6 |
| Yasuda et al., 2015a [60] | Y | N | Y | N | N | N | Y | Y | Y | Y | 6 |
| Yasuda et al., 2015b [61] | Y | N | Y | N | N | N | Y | Y | Y | Y | 6 |
| Yokokawa et al., 2008 [62] | Y | N | Y | N | N | N | Y | N | Y | Y | 5 |
| N = No, Y = Yes | Mean | 5.6 | |||||||||
| Outcome Comparison; Number of Studies (Comparisons); Sample Size | Risk of Bias | Inconsistency | Indirectness of Evidence | Imprecision | Publication Bias | SMD (95% CI) | Certainty of Evidence | |
|---|---|---|---|---|---|---|---|---|
| Muscle strength | ||||||||
| LL-BFR vs. HL (overall effect); 8 studies (23 comparisons); n = 189 | Not serious | Not serious | Not serious | Serious b | No | −0.23 (−0.41 to −0.05) * | ⨁⨁⨁◯ MODERATE | |
| Greater than limb OP; 5 studies (16 comparisons); n = 102 | Not serious | Not serious | Not serious | Serious b | No | −0.23 (−0.45 to −0.02) * | ⨁⨁⨁◯ MODERATE | |
| Near limb OP; 4 studies (7 comparisons); n = 87 | Not serious | Not serious | Not serious | Serious b | No | −0.23 (−0.55 to 0.10) | ⨁⨁⨁◯ MODERATE | |
| LL-BFR vs. LL (overall effect); 7 studies (25 comparisons); n = 201 | Not serious | Not serious | Not serious | Serious b | No | 0.44 (0.28 to 0.60) * | ⨁⨁⨁◯ MODERATE | |
| Greater than limb OP; 3 studies (8 comparisons); n = 54 | Not serious | Not serious | Not serious | Serious b | No | 0.77 (0.44 to 1.10) * | ⨁⨁⨁◯ MODERATE | |
| Near limb OP; 5 studies (17 comparisons); n = 147 | Not serious | Not serious | Not serious | Serious b | No | 0.34 (0.16 to 0.53) * | ⨁⨁⨁◯ MODERATE | |
| Muscle hypertrophy | ||||||||
| LL-BFR vs. HL (overall effect); 6 studies (9 comparisons); n = 114 | Serious a | Not serious | Not serious | Serious b | No | 0.08 (−0.22 to 0.38) | ⨁⨁◯◯ LOW | |
| Greater than limb OP; 4 studies (7 comparisons); n = 81 | Serious a | Not serious | Not serious | Serious b | No | 0.08 (−0.25 to 0.41) | ⨁⨁◯◯ LOW | |
| Near limb OP; 2 studies (2 comparisons); n = 33 | — | — | — | — | — | — | — | |
| LL-BFR vs. LL (overall effect); 2 studies (5 comparisons); n = 31 | Serious a | Not serious | Not serious | Serious b | No | 0.51 (0.06 to 0.96) * | ⨁⨁◯◯ LOW | |
| Greater than limb OP; 2 studies (5 comparisons); n = 31 | Serious a | Not serious | Not serious | Serious b | No | 0.51 (0.06 to 0.96) * | ⨁⨁◯◯ LOW | |
| Near limb OP; | — | — | — | — | — | — | — | — |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fabero-Garrido, R.; Gragera-Vela, M.; del Corral, T.; Izquierdo-García, J.; Plaza-Manzano, G.; López-de-Uralde-Villanueva, I. Effects of Low-Load Blood Flow Restriction Resistance Training on Muscle Strength and Hypertrophy Compared with Traditional Resistance Training in Healthy Adults Older Than 60 Years: Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 7389. https://doi.org/10.3390/jcm11247389
Fabero-Garrido R, Gragera-Vela M, del Corral T, Izquierdo-García J, Plaza-Manzano G, López-de-Uralde-Villanueva I. Effects of Low-Load Blood Flow Restriction Resistance Training on Muscle Strength and Hypertrophy Compared with Traditional Resistance Training in Healthy Adults Older Than 60 Years: Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(24):7389. https://doi.org/10.3390/jcm11247389
Chicago/Turabian StyleFabero-Garrido, Raúl, Miguel Gragera-Vela, Tamara del Corral, Juan Izquierdo-García, Gustavo Plaza-Manzano, and Ibai López-de-Uralde-Villanueva. 2022. "Effects of Low-Load Blood Flow Restriction Resistance Training on Muscle Strength and Hypertrophy Compared with Traditional Resistance Training in Healthy Adults Older Than 60 Years: Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 24: 7389. https://doi.org/10.3390/jcm11247389
APA StyleFabero-Garrido, R., Gragera-Vela, M., del Corral, T., Izquierdo-García, J., Plaza-Manzano, G., & López-de-Uralde-Villanueva, I. (2022). Effects of Low-Load Blood Flow Restriction Resistance Training on Muscle Strength and Hypertrophy Compared with Traditional Resistance Training in Healthy Adults Older Than 60 Years: Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 11(24), 7389. https://doi.org/10.3390/jcm11247389