
Neuropathic-like Pain Symptoms and Their Association with Muscle Strength in Patients with Chronic Musculoskeletal Pain


Abstract
1. Introduction
2. Materials and Methods
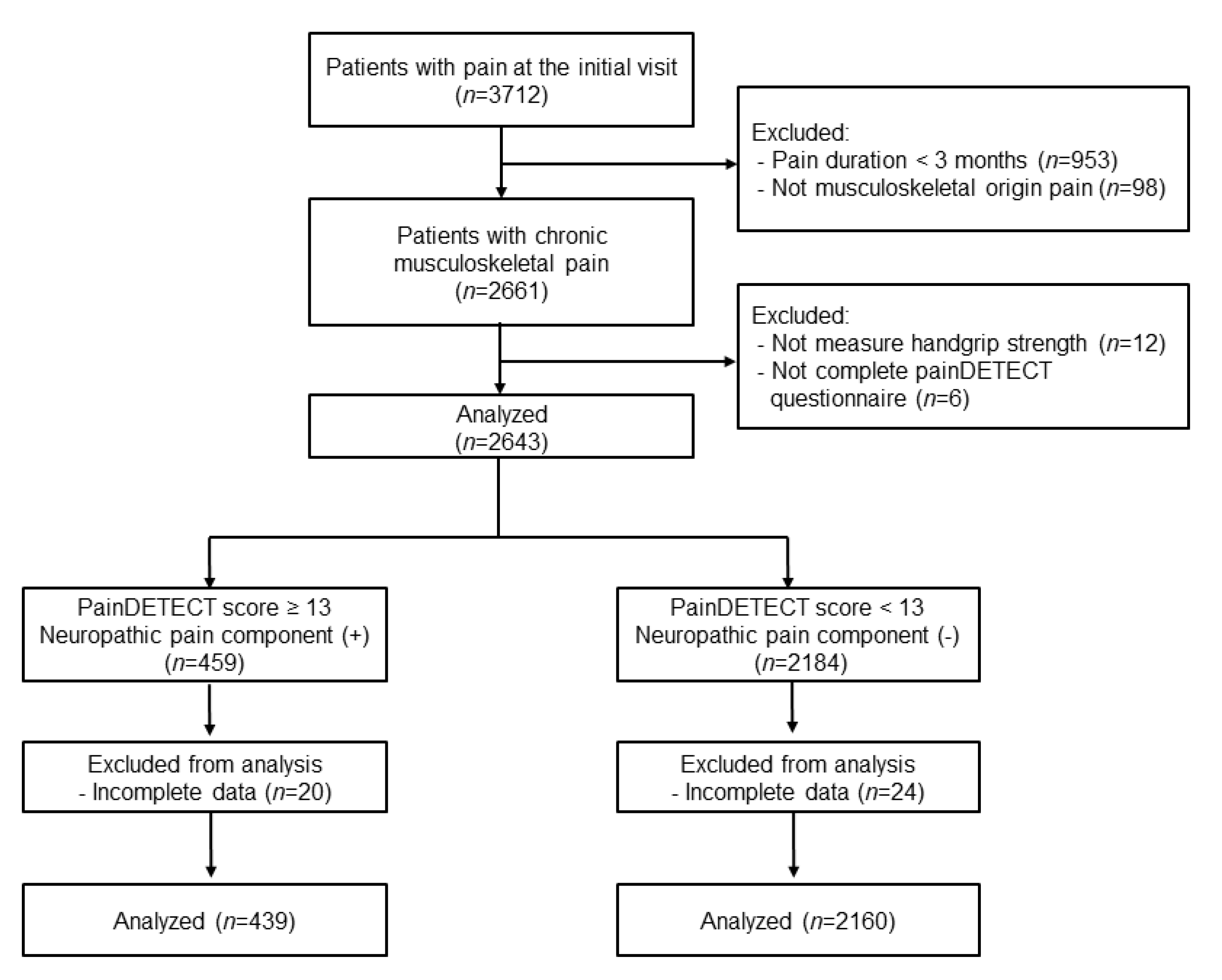
2.1. Study Population
2.2. PainDETECT Score Measurements
2.3. Handgrip Strength Measurement and Muscle Mass Estimation
2.4. Patient Demographics and Clinical Data Measurements
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e302. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef]
- Petermann-Rocha, F.; Balntzi, V.; Gray, S.R.; Lara, J.; Ho, F.K.; Pell, J.P.; Celis-Morales, C. Global prevalence of sarcopenia and severe sarcopenia: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2022, 13, 86–99. [Google Scholar] [CrossRef]
- McGrath, R.; Johnson, N.; Klawitter, L.; Mahoney, S.; Trautman, K.; Carlson, C.; Rockstad, E.; Hackney, K.J. What are the association patterns between handgrip strength and adverse health conditions? A topical review. SAGE Open Med. 2020, 8, 2050312120910358. [Google Scholar] [CrossRef]
- Yoo, J.I.; Choi, H.; Ha, Y.C. Mean Hand Grip Strength and Cut-off Value for Sarcopenia in Korean Adults Using KNHANES VI. J. Korean Med. Sci. 2017, 32, 868–872. [Google Scholar] [CrossRef]
- Shen, F.; Kim, H.J.; Lee, N.K.; Chun, H.J.; Chang, B.S.; Lee, C.K.; Yeom, J.S. The influence of hand grip strength on surgical outcomes after surgery for degenerative lumbar spinal stenosis: A preliminary result. Spine J. 2018, 18, 2018–2024. [Google Scholar] [CrossRef]
- Cabanas-Sánchez, V.; Esteban-Cornejo, I.; Parra-Soto, S.; Petermann-Rocha, F.; Gray, S.R.; Rodríguez-Artalejo, F.; Ho, F.K.; Pell, J.P.; Martínez-Gómez, D.; Celis-Morales, C. Muscle strength and incidence of depression and anxiety: Findings from the UK Biobank prospective cohort study. J. Cachexia Sarcopenia Muscle 2022, 13, 1983–2994. [Google Scholar] [CrossRef]
- Cohen, S.P.; Mao, J. Neuropathic pain: Mechanisms and their clinical implications. BMJ 2014, 348, f7656. [Google Scholar] [CrossRef]
- Cohen, S.P.; Vase, L.; Hooten, W.M. Chronic pain: An update on burden, best practices, and new advances. Lancet 2021, 397, 2082–2097. [Google Scholar] [CrossRef]
- Colloca, L.; Ludman, T.; Bouhassira, D.; Baron, R.; Dickenson, A.H.; Yarnitsky, D.; Freeman, R.; Truini, A.; Attal, N.; Finnerup, N.B.; et al. Neuropathic pain. Nat. Rev. Dis. Primers 2017, 3, 17002. [Google Scholar] [CrossRef]
- Kurien, T.; Arendt-Nielsen, L.; Petersen, K.K.; Graven-Nielsen, T.; Scammell, B.E. Preoperative Neuropathic Pain-like Symptoms and Central Pain Mechanisms in Knee Osteoarthritis Predicts Poor Outcome 6 Months After Total Knee Replacement Surgery. J. Pain 2018, 19, 1329–1341. [Google Scholar] [CrossRef]
- Freynhagen, R.; Baron, R.; Gockel, U.; Tölle, T.R. painDETECT: A new screening questionnaire to identify neuropathic components in patients with back pain. Curr. Med. Res. Opin. 2006, 22, 1911–1920. [Google Scholar] [CrossRef] [PubMed]
- Gudala, K.; Ghai, B.; Bansal, D. Usefulness of four commonly used neuropathic pain screening questionnaires in patients with chronic low back pain: A cross-sectional study. Korean J. Pain 2017, 30, 51–58. [Google Scholar] [CrossRef]
- König, S.L.; Prusak, M.; Pramhas, S.; Windpassinger, M. Correlation between the Neuropathic PainDETECT Screening Questionnaire and Pain Intensity in Chronic Pain Patients. Medicina 2021, 57, 353. [Google Scholar] [CrossRef]
- Lin, T.; Dai, M.; Xu, P.; Sun, L.; Shu, X.; Xia, X.; Zhao, Y.; Song, Q.; Guo, D.; Deng, C.; et al. Prevalence of Sarcopenia in Pain Patients and Correlation Between the Two Conditions: A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2022, 23, 902.e1–902.e20. [Google Scholar] [CrossRef]
- Imagama, S.; Ando, K.; Kobayashi, K.; Nakashima, H.; Seki, T.; Hamada, T.; Machino, M.; Ota, K.; Tanaka, S.; Morozumi, M.; et al. Risk Factors for Neuropathic Pain in Middle-Aged and Elderly People: A Five-Year Longitudinal Cohort in the Yakumo Study. Pain Med. 2020, 21, 1604–1610. [Google Scholar] [CrossRef] [PubMed]
- Bonanni, R.; Cariati, I.; Tancredi, V.; Iundusi, R.; Gasbarra, E.; Tarantino, U. Chronic Pain in Musculoskeletal Diseases: Do You Know Your Enemy? J. Clin. Med. 2022, 11, 2609. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.K.; Choi, J.H.; Jeong, J.; Kim, W.J.; Lee, D.J.; Lee, S.C.; Kim, Y.C.; Moon, J.Y. Korean Version of the painDETECT Questionnaire: A Study for Cultural Adaptation and Validation. Pain Pract. 2017, 17, 494–504. [Google Scholar] [CrossRef] [PubMed]
- Inoue, S.; Taguchi, T.; Yamashita, T.; Nakamura, M.; Ushida, T. The prevalence and impact of chronic neuropathic pain on daily and social life: A nationwide study in a Japanese population. Eur. J. Pain 2017, 21, 727–737. [Google Scholar] [CrossRef]
- Fountotos, R.; Munir, H.; Goldfarb, M.; Lauck, S.; Kim, D.; Perrault, L.; Arora, R.; Moss, E.; Rudski, L.G.; Bendayan, M.; et al. Prognostic Value of Handgrip Strength in Older Adults Undergoing Cardiac Surgery. Can. J. Cardiol. 2021, 37, 1760–1766. [Google Scholar] [CrossRef] [PubMed]
- Wen, X.; Wang, M.; Jiang, C.M.; Zhang, Y.M. Anthropometric equation for estimation of appendicular skeletal muscle mass in Chinese adults. Asia Pac. J. Clin. Nutr. 2011, 20, 551–556. [Google Scholar] [PubMed]
- Lee, J.H.; Cho, A.R.; Kwon, Y.J. Association between dairy protein and body composition in middle-aged and older women: A community-based, 12-year, prospective cohort study. Clin. Nutr. 2022, 41, 460–467. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.H.; Hébert, H.L.; Veluchamy, A. Neuropathic pain in the community: Prevalence, impact, and risk factors. Pain 2020, 161 (Suppl. S1), S127–S137. [Google Scholar] [CrossRef]
- Giske, L.; Bautz-Holter, E.; Sandvik, L.; Røe, C. Relationship between pain and neuropathic symptoms in chronic musculoskeletal pain. Pain Med. 2009, 10, 910–917. [Google Scholar] [CrossRef][Green Version]
- Kapuczinski, A.; Soyfoo, M.S.; De Breucker, S.; Margaux, J. Assessment of sarcopenia in patients with fibromyalgia. Rheumatol. Int. 2022, 42, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Koca, I.; Savas, E.; Ozturk, Z.A.; Boyaci, A.; Tutoglu, A.; Alkan, S.; Yildiz, H.; Kimyon, G. The evaluation in terms of sarcopenia of patients with fibromyalgia syndrome. Wien Klin. Wochenschr. 2016, 128, 816–821. [Google Scholar] [CrossRef] [PubMed]
- Bouhassira, D.; Lantéri-Minet, M.; Attal, N.; Laurent, B.; Touboul, C. Prevalence of chronic pain with neuropathic characteristics in the general population. Pain 2008, 136, 380–387. [Google Scholar] [CrossRef]
- Perrot, S.; Trouvin, A.P.; Rondeau, V.; Chartier, I.; Arnaud, R.; Milon, J.Y.; Pouchain, D. Kinesiophobia and physical therapy-related pain in musculoskeletal pain: A national multicenter cohort study on patients and their general physicians. Jt. Bone Spine 2018, 85, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Beenakker, K.G.; Ling, C.H.; Meskers, C.G.; de Craen, A.J.; Stijnen, T.; Westendorp, R.G.; Maier, A.B. Patterns of muscle strength loss with age in the general population and patients with a chronic inflammatory state. Ageing Res. Rev. 2010, 9, 431–436. [Google Scholar] [CrossRef]
- Hysing, E.B.; Smith, L.; Thulin, M.; Karlsten, R.; Bothelius, K.; Gordh, T. Detection of systemic inflammation in severely impaired chronic pain patients and effects of a multimodal pain rehabilitation program. Scand. J. Pain 2019, 19, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Clark, B.C.; Manini, T.M. Sarcopenia =/= dynapenia. J. Gerontol. A Biol. Sci. Med Sci. 2008, 63, 829–834. [Google Scholar] [CrossRef] [PubMed]
- Farina, D.; Arendt-Nielsen, L.; Merletti, R.; Graven-Nielsen, T. Effect of experimental muscle pain on motor unit firing rate and conduction velocity. J. Neurophysiol. 2004, 91, 1250–1259. [Google Scholar] [CrossRef]
- Teichtahl, A.J.; Urquhart, D.M.; Wang, Y.; Wluka, A.E.; Wijethilake, P.; O’Sullivan, R.; Cicuttini, F.M. Fat infiltration of paraspinal muscles is associated with low back pain, disability, and structural abnormalities in community-based adults. Spine J. 2015, 15, 1593–1601. [Google Scholar] [CrossRef] [PubMed]
- Leitzelar, B.N.; Koltyn, K.F. Exercise and Neuropathic Pain: A General Overview of Preclinical and Clinical Research. Sports Med. Open 2021, 7, 21. [Google Scholar] [CrossRef]
- Cooper, M.A.; Kluding, P.M.; Wright, D.E. Emerging Relationships between Exercise, Sensory Nerves, and Neuropathic Pain. Front Neurosci 2016, 10, 372. [Google Scholar] [CrossRef] [PubMed]
- Larsson, A.; Palstam, A.; Löfgren, M.; Ernberg, M.; Bjersing, J.; Bileviciute-Ljungar, I.; Gerdle, B.; Kosek, E.; Mannerkorpi, K. Resistance exercise improves muscle strength, health status and pain intensity in fibromyalgia--a randomized controlled trial. Arthritis Res. Ther. 2015, 17, 161. [Google Scholar] [CrossRef]
- Van Hecke, O.; Torrance, N.; Smith, B.H. Chronic pain epidemiology and its clinical relevance. Br. J. Anaesth. 2013, 111, 13–18. [Google Scholar] [CrossRef]
- Fernandes, G.S.; Valdes, A.M.; Walsh, D.A.; Zhang, W.; Doherty, M. Neuropathic-like knee pain and associated risk factors: A cross-sectional study in a UK community sample. Arthritis Res. Ther. 2018, 20, 215. [Google Scholar] [CrossRef]
- McMillin, S.L.; Minchew, E.C.; Lowe, D.A.; Spangenburg, E.E. Skeletal muscle wasting: The estrogen side of sexual dimorphism. Am. J. Physiol. Cell Physiol. 2022, 322, C24–C37. [Google Scholar] [CrossRef]
- Hong, Y.S.; Kim, H. Hand grip strength and health-related quality of life in postmenopausal women: A national population-based study. Menopause 2021, 28, 1330–1339. [Google Scholar] [CrossRef] [PubMed]
- Berthelot, J.M.; Biha, N.; Darrieutort-Laffite, C.; Le Goff, B.; Maugars, Y. Are painDETECT scores in musculoskeletal disorders associated with duration of daily pain and time elapsed since current pain onset? Pain Rep. 2019, 4, e739. [Google Scholar] [CrossRef]
- Tuna, T.; Van Obbergh, L.; Van Cutsem, N.; Engelman, E. Usefulness of the pain sensitivity questionnaire to discriminate the pain behaviour of chronic pain patients. Br. J. Anaesth. 2018, 121, 616–622. [Google Scholar] [CrossRef] [PubMed]
- Stocks, J.; Tang, N.K.; Walsh, D.A.; Warner, S.C.; Harvey, H.L.; Jenkins, W.; Abhishek, A.; Doherty, M.; Valdes, A.M. Bidirectional association between disturbed sleep and neuropathic pain symptoms: A prospective cohort study in post-total joint replacement participants. J. Pain Res. 2018, 11, 1087–1093. [Google Scholar] [CrossRef] [PubMed]
- Cappelleri, J.C.; Koduru, V.; Bienen, E.J.; Sadosky, A. Characterizing neuropathic pain profiles: Enriching interpretation of painDETECT. Patient Relat. Outcome Meas. 2016, 7, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Jensen, T.S.; Finnerup, N.B. Allodynia and hyperalgesia in neuropathic pain: Clinical manifestations and mechanisms. Lancet Neurol. 2014, 13, 924–935. [Google Scholar] [CrossRef]
- Vase, L.; Nikolajsen, L.; Christensen, B.; Egsgaard, L.L.; Arendt-Nielsen, L.; Svensson, P.; Jensen, T.S. Cognitive-emotional sensitization contributes to wind-up-like pain in phantom limb pain patients. Pain 2011, 152, 157–162. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | PainDETECT ≥ 13 (n = 439) | PainDETECT < 13 (n = 2160) | p-Value |
|---|---|---|---|
| Patient characteristics | |||
| Age, years | 59.46 ± 16.03 (20–98) | 60.02 ± 15.50 (20–89) | 0.487 |
| <45 years | 82 (18.7) | 352 (16.3) | 0.393 |
| 45–64 years | 171 (39.0) | 874 (40.5) | |
| ≥65 years | 186 (42.3) | 934 (43.2) | |
| Sex, M/F | 165 (37.6)/274 (62.4) | 894 (41.4)/1266 (58.6) | 0.139 |
| BMI, kg/m2 | 24.32 (21.91–26.01) | 24.03 (22.06–26.03) | 0.971 |
| <25 kg/m2 | 276 (62.9) | 1281 (59.3) | 0.347 |
| ≥25 kg/m2 | 163 (37.1) | 879 (40.7) | |
| Medical comorbidities, n | |||
| Hypertension | 131 (29.8) | 664 (30.7) | 0.755 |
| Diabetes mellitus | 81 (18.5) | 410 (19.0) | 0.830 |
| Cardiovascular disease | 19 (4.3) | 128 (5.9) | 0.193 |
| Mental health problems | 136 (31.0) | 545 (25.2) | 0.010 |
| Osteopenia/osteoporosis | 147 (33.5) | 723 (33.5) | 0.943 |
| Pain-related data | |||
| Pain duration, months | 8.00 (3.00–36.00) | 12.00 (6.00–48.00) | <0.001 |
| <12 months | 238 (54.2) | 813 (37.6) | <0.001 |
| ≥12 months | 201 (45.8) | 1347 (62.4) | |
| Pain score, NRS 0–10 | 6.71 ± 2.09 | 6.02 ± 2.16 | <0.001 |
| NRS < 7 | 185 (42.1) | 1176 (54.4) | <0.001 |
| NRS ≥ 7 | 254 (57.9) | 984 (45.6) | |
| Opioid usage, n | 80 (18.2) | 137 (6.3) | <0.001 |
| Primary pain location, n | <0.001 | ||
| Neck (cervical spine) | 80 (18.2) | 373 (17.3) | |
| Upper limbs (shoulder, elbow, wrist, hand) | 46 (10.5) | 172 (8.0) | |
| Back (thoracic spine), chest wall | 58 (13.2) | 158 (7.3) | |
| Lower back (lumbar spine) | 197 (44.9) | 1298 (60.1) | |
| Lower limbs (hip, knee, ankle, foot) | 58 (13.2) | 159 (7.4) | |
| Multiple pain sites, n | 118 (26.9) | 599 (27.7) | 0.716 |
| Sleep disturbance, n | 254 (57.9) | 816 (37.8) | <0.001 |
| Sarcopenia-related data | |||
| ASM, kg | 17.74 ± 4.79 | 18.30 ± 4.67 | 0.119 |
| SMI, kg/m2 | 6.71 ± 1.17 | 6.87 ± 1.15 | 0.082 |
| HGS, kg | 23.23 ± 10.57 | 24.82 ± 10.43 | 0.004 |
| Males | Females | |||||
|---|---|---|---|---|---|---|
| PainDETECT | PainDETECT | PainDETECT | PainDETECT | |||
| ≥13 | <13 | p-value | ≥13 | <13 | p-value | |
| (n = 165) | (n = 894) | (n = 274) | (n = 1266) | |||
| ASM, kg | 23.24 ± 2.83 | 22.61 ± 2.80 | 0.077 | 14.63 ± 2.13 | 14.68 ± 2.17 | 0.810 |
| SMI, kg/m2 | 8.00 ± 0.61 | 7.89 ± 0.66 | 0.166 | 5.98 ± 0.67 | 6.01 ± 0.67 | 0.693 |
| HGS, kg | 31.98 ± 10.73 | 33.38 ± 9.48 | 0.089 | 17.96 ± 5.99 | 18.78 ± 5.82 | 0.035 |
| Variables | Adjusted OR | 95% CI | p-Value |
|---|---|---|---|
| Female | 1.251 | 0.814–1.924 | 0.308 |
| Cardiovascular disease, yes | 0.824 | 0.372–1.828 | 0.635 |
| Mental health problems, yes | 1.216 | 0.873–1.693 | 0.248 |
| Pain duration, ≥12 months | 0.536 | 0.390–0.738 | <0.001 |
| Pain score, NRS ≥ 7 | 1.329 | 0.946–1.866 | 0.101 |
| Opioid usage, yes | 2.961 | 1.860–4.714 | <0.001 |
| Main pain location | |||
| Neck (cervical spine) | 1.000 | ||
| Upper limbs (shoulder, elbow, wrist, hand) | 1.464 | 0.780–2.750 | 0.236 |
| Back (thoracic spine) and chest wall | 1.447 | 0.757–2.766 | 0.264 |
| Low back (lumbar spine) | 0.904 | 0.564–1.448 | 0.675 |
| Lower limbs (hip, knee, ankle, foot) | 2.066 | 1.102–3.872 | 0.024 |
| Sleep disturbance, yes | 2.052 | 1.487–2.831 | <0.001 |
| ASM, kg | 1.046 | 0.977–1.120 | 0.195 |
| SMI, kg/m2 | 0.914 | 0.598–1.395 | 0.676 |
| HGS, kg | 0.976 | 0.960–0.993 | 0.005 |
| PainDETECT Items | Low HGS Group (n = 978) | Normal HGS Group (n = 1621) | p-Value |
|---|---|---|---|
| Gradation of pain (score of ≥3/5), n | |||
| Burning sensation | 113 (11.6) | 180 (11.1) | 0.725 |
| Tingling sensation | 424 (43.4) | 706 (43.6) | 0.921 |
| Pain by light touch | 85 (8.7) | 105 (6.5) | 0.036 |
| Electric shock-like pain | 326 (33.3) | 519 (32.0) | 0.488 |
| Pain on cold/heat stimulation | 54 (5.5) | 45 (2.8) | <0.001 |
| Numbness | 178 (18.2) | 249 (15.4) | 0.058 |
| Pain by slight pressure | 222 (22.7) | 345 (21.3) | 0.397 |
| Pain course pattern, n | |||
| Persistent pain with slight fluctuation | 491 (50.2) | 884 (54.5) | 0.032 |
| Persistent pain with pain attacks | 266 (27.2) | 392 (24.2) | 0.087 |
| Pain attacks without pain between them | 151 (15.4) | 258 (15.9) | 0.747 |
| Pain attacks with pain between them | 70 (7.2) | 87 (5.4) | 0.063 |
| Radiating pain, n | 387 (39.6) | 572 (35.3) | 0.029 |
| Categorization by total score, n | |||
| ≤12 | 784 (80.2) | 1376 (84.9) | |
| 13–18 | 140 (14.3) | 179 (11.0) | |
| ≥19 | 54 (5.5) | 66 (4.1) | |
| Total PainDETECT score | 7.32 ± 6.28 | 6.73 ± 5.65 | 0.016 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.J.; Ban, M.G.; Yoon, K.B.; Jeon, W.; Kim, S.H. Neuropathic-like Pain Symptoms and Their Association with Muscle Strength in Patients with Chronic Musculoskeletal Pain. J. Clin. Med. 2022, 11, 5471. https://doi.org/10.3390/jcm11185471
Kim HJ, Ban MG, Yoon KB, Jeon W, Kim SH. Neuropathic-like Pain Symptoms and Their Association with Muscle Strength in Patients with Chronic Musculoskeletal Pain. Journal of Clinical Medicine. 2022; 11(18):5471. https://doi.org/10.3390/jcm11185471
Chicago/Turabian StyleKim, Hee Jung, Min Gi Ban, Kyung Bong Yoon, Woohyuk Jeon, and Shin Hyung Kim. 2022. "Neuropathic-like Pain Symptoms and Their Association with Muscle Strength in Patients with Chronic Musculoskeletal Pain" Journal of Clinical Medicine 11, no. 18: 5471. https://doi.org/10.3390/jcm11185471
APA StyleKim, H. J., Ban, M. G., Yoon, K. B., Jeon, W., & Kim, S. H. (2022). Neuropathic-like Pain Symptoms and Their Association with Muscle Strength in Patients with Chronic Musculoskeletal Pain. Journal of Clinical Medicine, 11(18), 5471. https://doi.org/10.3390/jcm11185471