
Anterior-First Approach for Latissimus Dorsi Myocutaneous Flap Breast Reconstruction: A Refined Elevation Method with Detailed Video Instructions

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics Statement and Patient Selection
2.2. Study Design
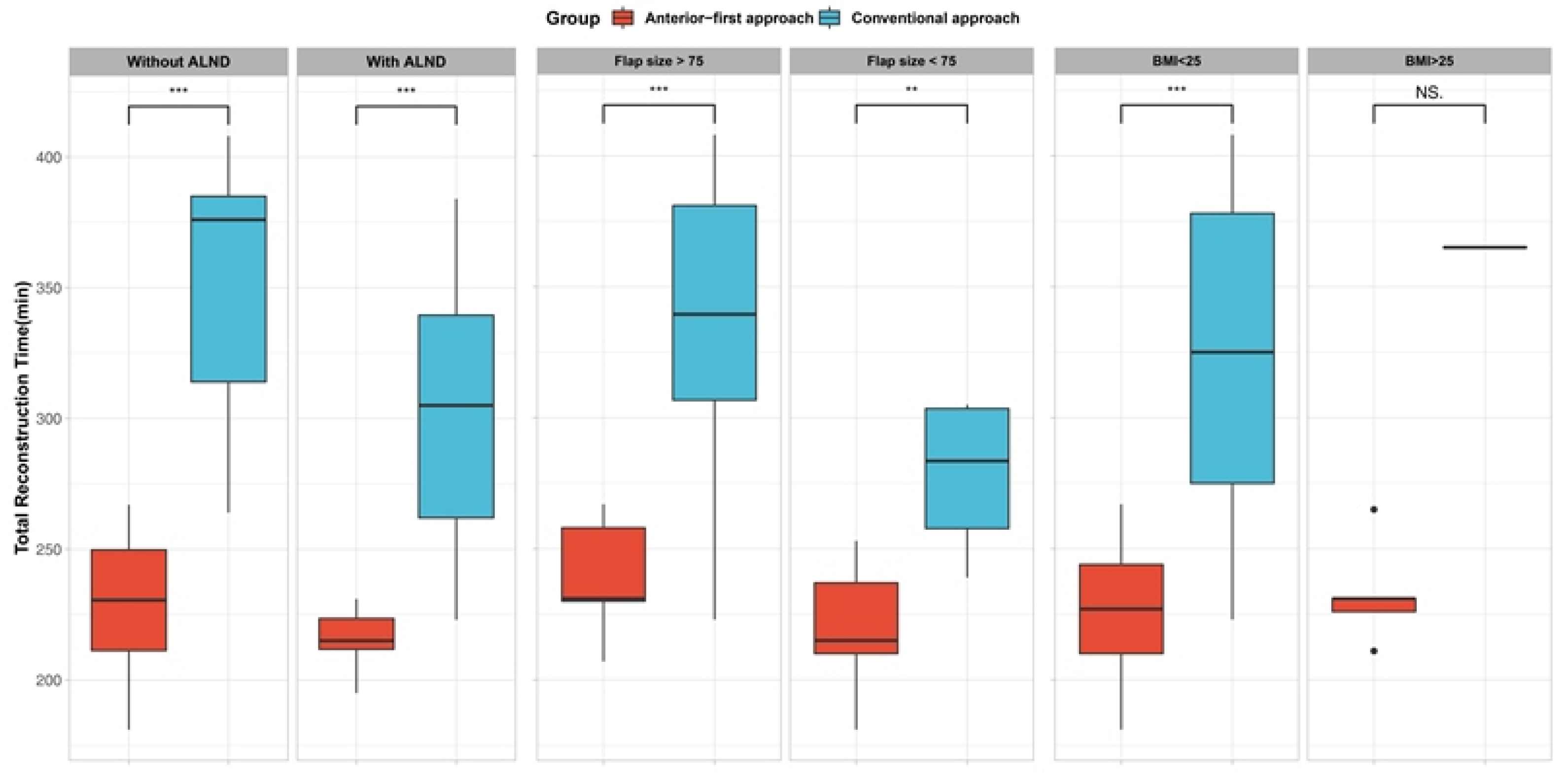
2.3. Statistical Analysis
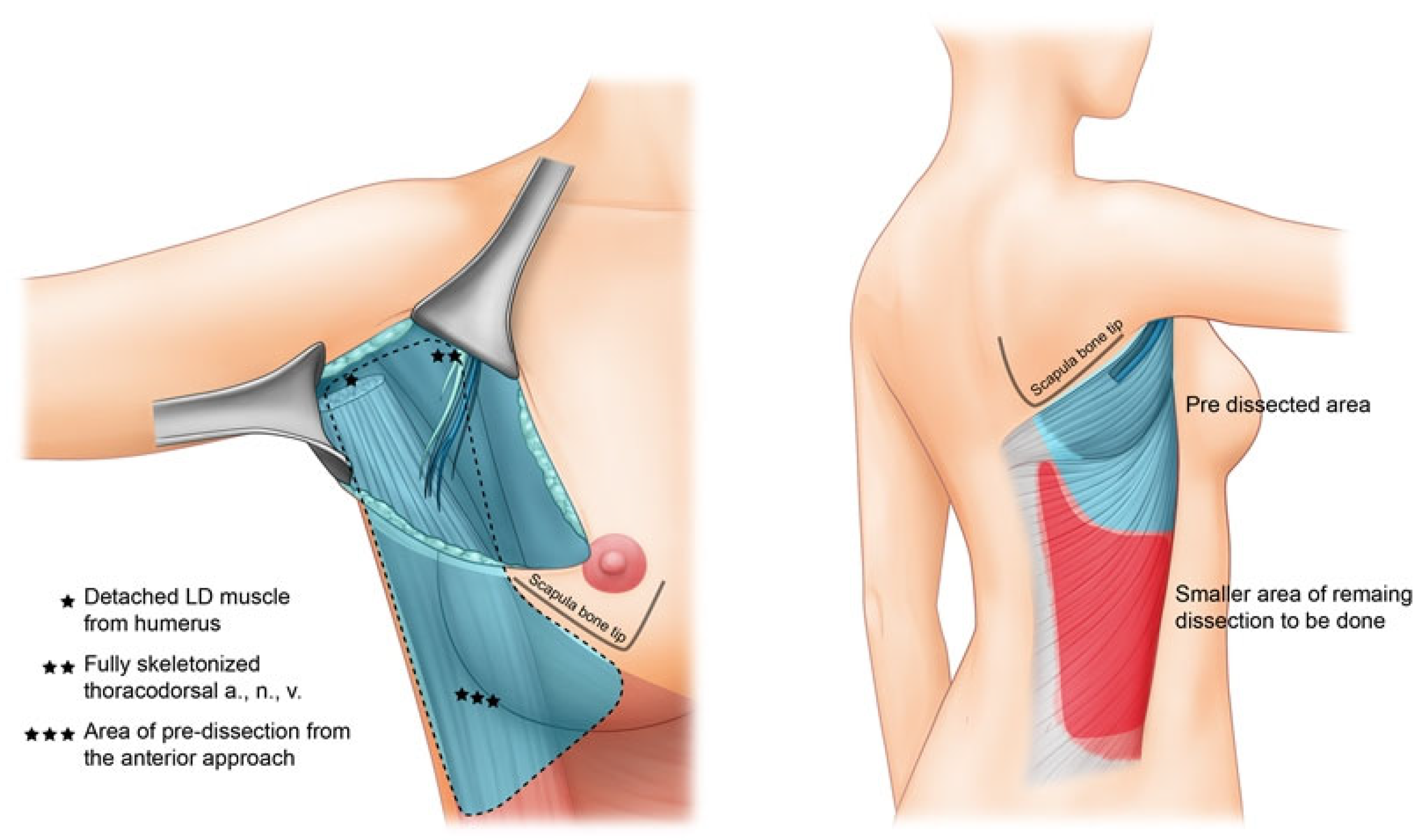
2.4. Operative Procedure
3. Results
3.1. Demographic and Oncologic Data
3.2. Operative Outcomes Data
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- DeLong, M.R.; Tandon, V.J.; Rudkin, G.H.; Da Lio, A.L. Latissimus Dorsi Flap Breast Reconstruction-A Nationwide Inpatient Sample Review. Ann. Plast. Surg. 2017, 78, S185–S188. [Google Scholar] [CrossRef] [PubMed]
- Black, C.K.; Zolper, E.G.; Economides, J.M.; Abadeer, A.; Fan, K.L.; Song, D.H. Comparison of the Pedicled Latissimus Dorsi Flap with Immediate Fat Transfer versus Abdominally Based Free Tissue Transfer for Breast Reconstruction. Plast. Reconstr. Surg. 2020, 146, 137e–146e. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Jung, J.H.; Kim, W.W.; Park, C.S.; Lee, R.K.; Park, H.Y. Endoscopy-assisted muscle-sparing Latissimus Dorsi muscle flap harvesting for partial breast reconstruction. BMC Surg. 2020, 20, 192. [Google Scholar] [CrossRef] [PubMed]
- Sood, R.; Easow, J.M.; Konopka, G.; Panthaki, Z.J. Latissimus Dorsi Flap in Breast Reconstruction: Recent innovations in the workhorse flap. Cancer Control 2018, 25, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Cha, W.; Jeong, W.-J.; Ahn, S.-H. Latissimus dorsi muscle free flap revisited: A novel endoscope-assisted approach. Laryngoscope 2013, 123, 613–617. [Google Scholar] [CrossRef] [PubMed]
- Maselli, A.M.; Mella, J.R.; Guo, L. Refining the Latissimus Dorsi Flap: A Useful Tool to Salvage Complex Breast Defects. Ann. Plast. Surg. 2019, 83, S11–S16. [Google Scholar] [CrossRef] [PubMed]
- Schmauss, D.; Machens, H.-G.; Harder, Y. Breast Reconstruction after Mastectomy. Front. Surg. 2016, 2, 71. [Google Scholar] [CrossRef] [PubMed]
- Team, R.C. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2017. [Google Scholar]
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer-Verlag: New York, NY, USA, 2009. [Google Scholar]
- Thomsen, J.B.; Rindom, M.B.; Rancati, A.; Angrigiani, C. Thoracodorsal artery flaps for breast reconstruction–the variants and its approach. Arch. Plast. Surg. 2021, 48, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.; Kim, H.; Lee, J.H.; Son, D. Anatomical Study of the Close Association between Latissimus Dorsi and Surrounding Muscles. How to Safely Harvest the Muscle? Arch. Plast. Surg. 2022, 49, 596–603. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.C.; Han, H.H.; Kim, E.K. Use of a Vertical Muscle-Sparing Latissimus Dorsi Flap in Implant-Based Breast Reconstruction Without Position Change. Ann. Plast. Surg. 2018, 81, 152–155. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Ryu, J.Y.; Choi, K.Y.; Yang, J.D.; Chung, H.Y.; Cho, B.C.; Kang, B.; Lee, J.; Park, H.Y.; Lee, J.S. Useful vertical latissimus dorsi flap for partial breast reconstruction in every tumor location. BMC Surg. 2022, 22, 294. [Google Scholar] [CrossRef] [PubMed]
- Perez, S.; Delay, E.; Sinna, R.; Savu, T.; Vaucher, R.; Frobert, P. Short-Scar Latissimus Dorsi With a Lateral Approach: A Game Changer in Breast Reconstruction? Aesthet. Surg. J. 2021, 41, NP1166–NP1175. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Seo, J.Y.; Jung, Y.J.; Choo, K.S.; Kim, M.W.; Park, T.S.; Bae, Y.C.; Nam, S.B.; Kim, H.Y. Volumetric changes of the latissimus dorsi muscle after postoperative chemotherapy in cases of immediate breast reconstruction with an extended latissimus dorsi musculocutaneous flap and implant. Gland. Surg. 2019, 8, 501–506. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.C.; Lee, J.; Park, S.-H.; Yoon, E.-S. The Hybrid Latissimus Dorsi Flap in Immediate Breast Reconstruction: A Comparative Study With the Abdominal-Based Flap. Ann. Plast. Surg. 2021, 86, 394–399. [Google Scholar] [CrossRef] [PubMed]
- Piat, J.M.; Tomazzoni, G.; Giovinazzo, V.; Dubost, V.; Maiato, A.P.; Ho Quoc, C. Lipofilled Mini Dorsi Flap: An Efficient Less Invasive Concept for Immediate Breast Reconstruction. Ann. Plast. Surg. 2020, 85, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Gonfiotti, A.; Salvicchi, A.; Voltolini, L. Chest-Wall Tumors and Surgical Techniques: State-of-the-Art and Our Institutional Experience. J. Clin. Med. 2022, 11, 5516. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Anterior-First Approach, n = 28 1 | Conventional Approach, n = 20 1 | p-Value 2 |
|---|---|---|---|
| Age | 45 (40, 51) | 42 (38, 48) | 0.2 |
| Type of mastectomy | <0.001 | ||
| MRM | 1 (3.6%) | 7 (35%) | |
| NSM | 14 (50%) | 1 (5.0%) | |
| SSM | 13 (46%) | 12 (60%) | |
| BMI | 21.8 (20.9, 24.2) | 20.0 (19.1, 21.3) | 0.004 |
| DM | 1 (3.6%) | 0 (0%) | >0.9 |
| Smoking | 0 (0%) | 0 (0%) | |
| Adjuvant chemotherapy | 3 (11%) | 2 (10%) | >0.9 |
| Axillary node dissection | 6 (21%) | 11 (55%) | 0.017 |
| Mastectomy weight | 247 (161, 341) | 235 (150, 303) | 0.8 |
| Flap surface area | 68 (51, 75) | 82 (77, 93) | 0.010 |
| Operative Phase | Anterior-First Approach | Conventional Approach |
|---|---|---|
| Flap elevation | 1st sub-phase: Elevation of axillary and lateral portion of LDMC flap without position change | N/A |
| Position change | Position change (supine → lateral) | Position change (supine → lateral) |
| Flap elevation | 2nd sub-phase: Elevate remaining distal area of the flap | Initiation of flap elevation from the lateral position |
| Position change | Position change (lateral → supine) | Position change (lateral → supine) |
| Inset and Closure | Flap inset and closure | Flap inset and closure |
| Characteristic | Anterior-First Approach, n = 28 1 | Conventional Approach, n = 20 1 | p-Value 2 |
|---|---|---|---|
| Flap elevation (minutes) | 139 (129, 145) | 200 (165, 228) | <0.001 |
| Anterior dissection | 33 (29, 37) | 0 (0, 0) | |
| Lateral dissection | 104 (98, 116) | 200 (165, 228) | <0.001 |
| Inset and closure (minutes) | 82 (71, 100) | 124 (100, 150) | <0.001 |
| Total reconstruction time (minutes) | 228 (211, 243) | 330 (280, 377) | <0.001 |
| Complication (%) | 0.14 | ||
| Hematoma | 1 (3.6%) | 1 (5.0%) | |
| Nipple color change | 0 (0%) | 1 (5.0%) | |
| Seroma | 0 (0%) | 2 (10%) | |
| Drain removal (days) | 7.0 (5.0, 12.2) | 8.0 (6.0, 10.0) | >0.9 |
| Flap size (cm2) | 68 (51, 75) | 82 (77, 93) | 0.010 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, J.; Ko, E.J.; Kim, S.A.; Choi, J.Y.; Moon, S.-H.; Jun, Y.J.; Byeon, J.H.; Oh, D.Y. Anterior-First Approach for Latissimus Dorsi Myocutaneous Flap Breast Reconstruction: A Refined Elevation Method with Detailed Video Instructions. J. Clin. Med. 2022, 11, 7387. https://doi.org/10.3390/jcm11247387
Choi J, Ko EJ, Kim SA, Choi JY, Moon S-H, Jun YJ, Byeon JH, Oh DY. Anterior-First Approach for Latissimus Dorsi Myocutaneous Flap Breast Reconstruction: A Refined Elevation Method with Detailed Video Instructions. Journal of Clinical Medicine. 2022; 11(24):7387. https://doi.org/10.3390/jcm11247387
Chicago/Turabian StyleChoi, Jangyoun, Eun Jeong Ko, Sung Ae Kim, Jong Yun Choi, Suk-Ho Moon, Young Joon Jun, Jun Hee Byeon, and Deuk Young Oh. 2022. "Anterior-First Approach for Latissimus Dorsi Myocutaneous Flap Breast Reconstruction: A Refined Elevation Method with Detailed Video Instructions" Journal of Clinical Medicine 11, no. 24: 7387. https://doi.org/10.3390/jcm11247387
APA StyleChoi, J., Ko, E. J., Kim, S. A., Choi, J. Y., Moon, S.-H., Jun, Y. J., Byeon, J. H., & Oh, D. Y. (2022). Anterior-First Approach for Latissimus Dorsi Myocutaneous Flap Breast Reconstruction: A Refined Elevation Method with Detailed Video Instructions. Journal of Clinical Medicine, 11(24), 7387. https://doi.org/10.3390/jcm11247387