
Saliva Is a Valid Alternative to Nasopharyngeal Swab in Chemiluminescence-Based Assay for Detection of SARS-CoV-2 Antigen

 , , ,
, , ,  ,
, 
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Saliva Samples
2.2. Preparation of Virus-Spiked Saliva Samples from Healthy Donors
2.3. Lumipulse® G SARS-CoV-2 Ag Assay on Saliva Samples
2.4. Simplexa™ COVID-19 Direct Assay on Saliva Samples
2.5. Statistical Analysis
3. Results
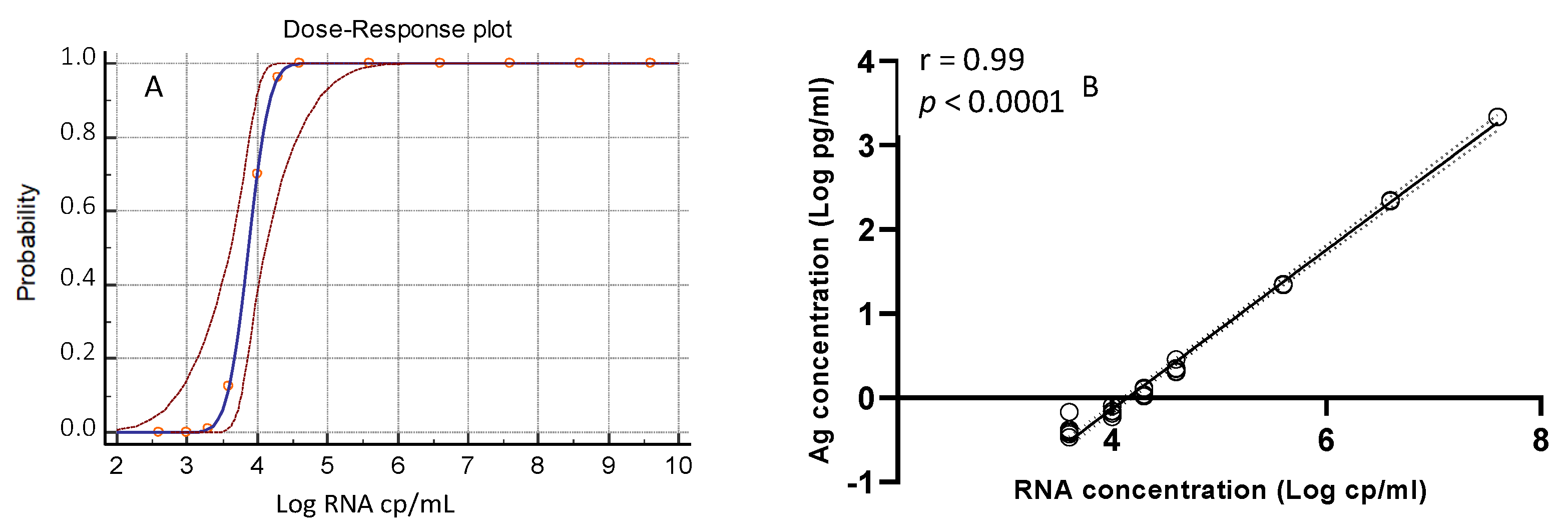
3.1. Analytical Sensitivity of the Lumipulse® G SARS-CoV-2 Ag Assay
3.2. Performance of the Lumipulse® G SARS-CoV-2 Ag Assay with Frozen Saliva Samples
3.3. Performance of the Lumipulse® G SARS-CoV-2 Ag Assay with Fresh Saliva Samples
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Laboratory Testing for 2019 Novel Coronavirus (2019-nCoV) in Suspected Human Cases. Available online: https://www.who.int/publications-detail/laboratory-testing-for-2019-novel-coronavirus-in-suspected-human-cases-20200117 (accessed on 17 January 2020).
- Mina, M.J.; Parker, R.; Larremore, D.B. Rethinking Covid-19 test sensitivity—A strategy for containment. N. Engl. J. Med. 2020, 383, e120. [Google Scholar] [CrossRef]
- Porte, L.; Legarraga, P.; Vollrath, V.; Aguilera, X.; Munita, J.M.; Araos, R. Evaluation of a novel antigen-based rapid detection test for the diagnosis of SARS-CoV-2 in respiratory samples. Int. J. Infect. Dis. 2020, 99, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Lambert-Niclot, S.; Cuffel, A.; Le Pape, S.; Vauloup-Fellous, C.; Morand-Joubert, L.; Roque-Afonso, A.-M.; Le Goff, J.; Delaugerre, C. Evaluation of a Rapid Diagnostic Assay for Detection of SARS-CoV-2 Antigen in Nasopharyngeal Swabs. J. Clin. Microbiol. 2020, 58, e00977-20. [Google Scholar] [CrossRef]
- Mak, G.C.; Cheng, P.K.; Lau, S.S.; Wong, K.K.; Lau, C.S.; Lam, E.T.; Chan, R.C.; Tsang, D.N. Evaluation of rapid antigen test for detection of SARS-CoV-2 virus. J. Clin. Virol. 2020, 129, 104500. [Google Scholar] [CrossRef]
- Scohy, A.; Anantharajah, A.; Bodéus, M.; Kabamba-Mukadi, B.; Verroken, A.; Rodriguez-Villalobos, H. Low performance of rapid antigen detection test as frontline testing for COVID-19 diagnosis. J. Clin. Virol. 2020, 129, 104455. [Google Scholar] [CrossRef]
- Moreno-Contreras, J.; Espinoza, M.A.; Sandoval-Jaime, C.; Cantú-Cuevas, M.A.; Barón-Olivares, H.; Ortiz-Orozco, O.D.; Muñoz-Rangel, A.V.; La Cruz, M.H.-D.; Eroza-Osorio, C.M.; Arias, C.F.; et al. Saliva Sampling and Its Direct Lysis, an Excellent Option To Increase the Number of SARS-CoV-2 Diagnostic Tests in Settings with Supply Shortages. J. Clin. Microbiol. 2020, 58, 1659–1720. [Google Scholar] [CrossRef] [PubMed]
- Williams, E.; Bond, K.; Zhang, B.; Putland, M.; Williamson, D.A. Saliva as a Noninvasive Specimen for Detection of SARS-CoV-2. J. Clin. Microbiol. 2020, 58. [Google Scholar] [CrossRef]
- Nagura-Ikeda, M.; Imai, K.; Tabata, S.; Miyoshi, K.; Murahara, N.; Mizuno, T.; Horiuchi, M.; Kato, K.; Imoto, Y.; Iwata, M.; et al. Clinical Evaluation of Self-Collected Saliva by Quantitative Reverse Transcription-PCR (RT-qPCR), Direct RT-qPCR, Reverse Transcription–Loop-Mediated Isothermal Amplification, and a Rapid Antigen Test to Diagnose COVID-19. J. Clin. Microbiol. 2020, 58, e01438–e01520. [Google Scholar] [CrossRef]
- Iwasaki, S.; Fujisawa, S.; Nakakubo, S.; Kamada, K.; Yamashita, Y.; Fukumoto, T.; Sato, K.; Oguri, S.; Taki, K.; Senjo, H.; et al. Comparison of SARS-CoV-2 detection in nasopharyngeal swab and saliva. J. Infect. 2020, 81, e145–e147. [Google Scholar] [CrossRef] [PubMed]
- Azzi, L.; Carcano, G.; Gianfagna, F.; Grossi, P.; Gasperina, D.D.; Genoni, A.; Fasano, M.; Sessa, F.; Tettamanti, L.; Carinci, F.; et al. Saliva is a reliable tool to detect SARS-CoV-2. J. Infect. 2020, 81, e45–e50. [Google Scholar] [CrossRef] [PubMed]
- Bordi, L.; Sberna, G.; Lalle, E.; Piselli, P.; Colavita, F.; Nicastri, E.; Antinori, A.; Boumis, E.; Petrosillo, N.; Marchioni, L.; et al. Frequency and Duration of SARS-CoV-2 Shedding in Oral Fluid Samples Assessed by a Modified Commercial Rapid Molecular Assay. Viruses 2020, 12, 1184. [Google Scholar] [CrossRef] [PubMed]
- Capobianchi, M.; Rueca, M.; Messina, F.; Giombini, E.; Carletti, F.; Colavita, F.; Castilletti, C.; Lalle, E.; Bordi, L.; Vairo, F.; et al. Molecular characterization of SARS-CoV-2 from the first case of COVID-19 in Italy. Clin. Microbiol. Infect. 2020, 26, 954–956. [Google Scholar] [CrossRef] [PubMed]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Eurosurveillance 2020, 25, 2000045. [Google Scholar] [CrossRef]
- Ogawa, T.; Fukumori, T.; Nishihara, Y.; Sekine, T.; Okuda, N.; Nishimura, T.; Fujikura, H.; Hirai, N.; Imakita, N.; Kasahara, K. Another false-positive problem for a SARS-CoV-2 antigen test in Japan. J. Clin. Virol. 2020, 131, 104612. [Google Scholar] [CrossRef] [PubMed]
- Hirotsu, Y.; Maejima, M.; Shibusawa, M.; Nagakubo, Y.; Hosaka, K.; Amemiya, K.; Sueki, H.; Hayakawa, M.; Mochizuki, H.; Tsutsui, T.; et al. Comparison of automated SARS-CoV-2 antigen test for COVID-19 infection with quantitative RT-PCR using 313 nasopharyngeal swabs, including from seven serially followed patients. Int. J. Infect. Dis. 2020, 99, 397–402. [Google Scholar] [CrossRef] [PubMed]
- Liotti, F.M.; Menchinelli, G.; Lalle, E.; Palucci, I.; Marchetti, S.; Colavita, F.; La Sorda, M.; Sberna, G.; Bordi, L.; Sanguinetti, M.; et al. Performance of a novel diagnostic assay for rapid SARS-CoV-2 antigen detection in nasopharynx samples. Clin. Microbiol. Infect. 2021, 27, 487–488. [Google Scholar] [CrossRef] [PubMed]
- Liotti, F.M.; Menchinelli, G.; Marchetti, S.; Morandotti, G.A.; Sanguinetti, M.; Posteraro, B.; Cattani, P. Evaluation of three commercial assays for SARS-CoV-2 molecular detection in upper respiratory tract samples. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 269–277. [Google Scholar] [CrossRef]
- Aoki, K.; Nagasawa, T.; Ishii, Y.; Yagi, S.; Okuma, S.; Kashiwagi, K.; Maeda, T.; Miyazaki, T.; Yoshizawa, S.; Tateda, K. Clinical validation of quantitative SARS-CoV-2 antigen assays to estimate SARS-CoV-2 viral loads in nasopharyngeal swabs. J. Infect. Chemother. 2021, 27, 613–616. [Google Scholar] [CrossRef] [PubMed]
- Menchinelli, G.; Bordi, L.; Marzia Liotti, F.; Palucci, I.; Capobianchi, M.R.; Sberna, G.; Lalle, E.; Romano, L.; de Angelis, G.; Marchetti, S.; et al. Lumipulse G SARS-CoV-2 Ag Assay Evaluation for SARS-CoV-2 Antigen Detection Using 594 Nasopharyngeal Swab Samples from Different Testing Groups. medRxiv 2021. [Google Scholar] [CrossRef]
- Kashiwagi, K.; Ishii, Y.; Aoki, K.; Yagi, S.; Maeda, T.; Miyazaki, T.; Yoshizawa, S.; Aoyagi, K.; Tateda, K. Immunochromatographic test for the detection of SARS-CoV-2 in saliva. J. Infect. Chemother. 2021, 27, 384–386. [Google Scholar] [CrossRef] [PubMed]
- Muller, D.A.; Depelsenaire, A.C.; Young, P.R. Clinical and Laboratory Diagnosis of Dengue Virus Infection. J. Infect. Dis. 2017, 215, S89–S95. [Google Scholar] [CrossRef] [PubMed]
- Interim Guidance for Antigen Testing for SARS-CoV-2 CDC. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/resources/antigen-tests-guidelines.html (accessed on 16 December 2020).
- Options for the Use of Rapid Antigen Tests for COVID-19 in the EU/EEA and the UK. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/Options-use-of-rapid-antigen-tests-for-COVID-19_0.pdf (accessed on 19 November 2020).



{kind=link}
{kind=link}
| Samples Data | Patients’ Frozen Samples | Patients’ Fresh Samples | Healthy Donors’ Samples |
|---|---|---|---|
| Number of Donors | 82 | 55 | 21 |
| Number of Samples | 169 | 87 | 40 |
| Age (mean (min-max)) | 50 (19–87) | 52 (20–89) | 41 (25–54) |
| Gender (%F; (n. F/n. Donors)) | 25.6%; 21/82 | 43.6%; 24/55 | 76.2%; 16/21 |
| Days from symptom onset (mean (min-max)) | 11 (0–37) | 14 (1–43) | N.A. |
| Days ≤ 7 (n; %) | 20; 46.5% | 19; 24.7% | N.A. |
| Days > 7 (n; %) | 23; 53.5% | 58; 75.3% | N.A. |
| Viral Preparation (TCID50/mL) | RNA cp/mL * | Lumipulse G SARS-CoV-2 Ag |
|---|---|---|
| Overall % Determinations (Replicates) | ||
| 1,000,000 | 4 × 109 | 100% (3/3) |
| 100,000 | 4 × 108 | 100% (3/3) |
| 10,000 | 4 × 107 | 100% (3/3) |
| 1000 | 4 × 106 | 100% (3/3) |
| 100 | 4 × 105 | 100% (3/3) |
| 10 | 4 × 104 | 100% (5/5) |
| 5 | 2 × 104 | 100% (5/5) |
| 2.5 | 1 × 104 | 60% (3/5) |
| 1 | 4 × 103 | 16.67% (1/6) |
| 0.1 | 4 × 102 | 0% (0/3) |
| Probit analysis | ||
| LOD: TCID50/mL | 4.46 | |
| LOD: RNA cp/mL | 18,197 | |
| Comparison of Frozen Saliva Samples | Lumipulse G SARS-CoV-2 Ag | |||
|---|---|---|---|---|
| Positive | Negative | Total | ||
| Simplexa™ COVID-19 Direct | Positive | 36 | 31 | 67 |
| Negative | 3 | 99 | 102 | |
| Total | 39 | 130 | 169 | |
| Proportion # | Percentage (95% CI) | |||
| Sensitivity | 36/67 | 53.7% (41.12–66.0%) | ||
| Specificity vs. RT-PCR reference test | 99/102 | 97.1% (96–99.4%) | ||
| Ct Ranges | Ag Positive Samples/Total Positive PCR | Positivity % with Lumipulse G SARS-CoV-2 Ag |
|---|---|---|
| <20 | 4/8 | 50.0% |
| 20–25 | 11/15 | 73.3% |
| 25.01–30 | 13/16 | 81.3% |
| >30 | 8/28 | 28.6% |
| Comparison of Fresh Saliva Samples | Lumipulse G SARS-CoV-2 Ag | |||
|---|---|---|---|---|
| Positive | Negative | Total | ||
| Simplexa™ COVID-19 Direct | Positive | 22 | 20 | 42 |
| Negative | 5 | 80 | 85 | |
| Total | 27 | 100 | 127 | |
| Proportion # | Percentage (95% CI) | |||
| Sensitivity | 22/42 | 52.4% (36.4–68.0%) | ||
| Specificity vs. RT-PCR reference test | 80/85 | 94.1% (86.8–98.1%) | ||
| Specificity vs. stage of infection | 45/45 | 100% (92.1–100.0%) | ||
| Ct Range | N° of Ag Positive Samples/Total Positive PCR | Positivity % with Lumipulse G SARS-CoV-2 Ag |
|---|---|---|
| <20 | 3/3 | 100% |
| 20–25 | 10/11 | 90.9% |
| 25.01–30 | 8/14 | 57.1% |
| >30 | 1/14 | 7.1% |
| Value 95% of CI | Prevalence of Infection | Positive Predictive Value * | Negative Predictive Value * | Accuracy * |
|---|---|---|---|---|
| Value | 0.5% | 4.28% | 99.75% | 93.91% |
| 95% CI | 1.79–9.90% | 99.65–99.82% | 88.23–97.38% | |
| Value | 1% | 8.25% | 99.49% | 93.70% |
| 95% CI | 3.54–18.08% | 99.30–99.63% | 87.96–97.24% | |
| Value | 2% | 15.38% | 98.98% | 93.28% |
| 95% CI | 6.89–30.85% | 98.60–99.26% | 87.44–96.96% | |
| Value | 10% | 49.73% | 94.68% | 89.94% |
| 95% CI | 28.73–70.83% | 92.80–96.08% | 83.35–94.57% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amendola, A.; Sberna, G.; Lalle, E.; Colavita, F.; Castilletti, C.; Menchinelli, G.; Posteraro, B.; Sanguinetti, M.; Ippolito, G.; Bordi, L.; et al. Saliva Is a Valid Alternative to Nasopharyngeal Swab in Chemiluminescence-Based Assay for Detection of SARS-CoV-2 Antigen. J. Clin. Med. 2021, 10, 1471. https://doi.org/10.3390/jcm10071471
Amendola A, Sberna G, Lalle E, Colavita F, Castilletti C, Menchinelli G, Posteraro B, Sanguinetti M, Ippolito G, Bordi L, et al. Saliva Is a Valid Alternative to Nasopharyngeal Swab in Chemiluminescence-Based Assay for Detection of SARS-CoV-2 Antigen. Journal of Clinical Medicine. 2021; 10(7):1471. https://doi.org/10.3390/jcm10071471
Chicago/Turabian StyleAmendola, Alessandra, Giuseppe Sberna, Eleonora Lalle, Francesca Colavita, Concetta Castilletti, Giulia Menchinelli, Brunella Posteraro, Maurizio Sanguinetti, Giuseppe Ippolito, Licia Bordi, and et al. 2021. "Saliva Is a Valid Alternative to Nasopharyngeal Swab in Chemiluminescence-Based Assay for Detection of SARS-CoV-2 Antigen" Journal of Clinical Medicine 10, no. 7: 1471. https://doi.org/10.3390/jcm10071471
APA StyleAmendola, A., Sberna, G., Lalle, E., Colavita, F., Castilletti, C., Menchinelli, G., Posteraro, B., Sanguinetti, M., Ippolito, G., Bordi, L., Capobianchi, M. R., & on behalf of INMI COVID-19 Study Group. (2021). Saliva Is a Valid Alternative to Nasopharyngeal Swab in Chemiluminescence-Based Assay for Detection of SARS-CoV-2 Antigen. Journal of Clinical Medicine, 10(7), 1471. https://doi.org/10.3390/jcm10071471