
Serum Anti-Heart and Anti-Intercalated Disk Autoantibodies: Novel Autoimmune Markers in Cardiac Sarcoidosis

 ,
,  , ,
, ,  ,
, 

Abstract
1. Introduction
2. Methods
2.1. Study Patients with Sarcoidosis
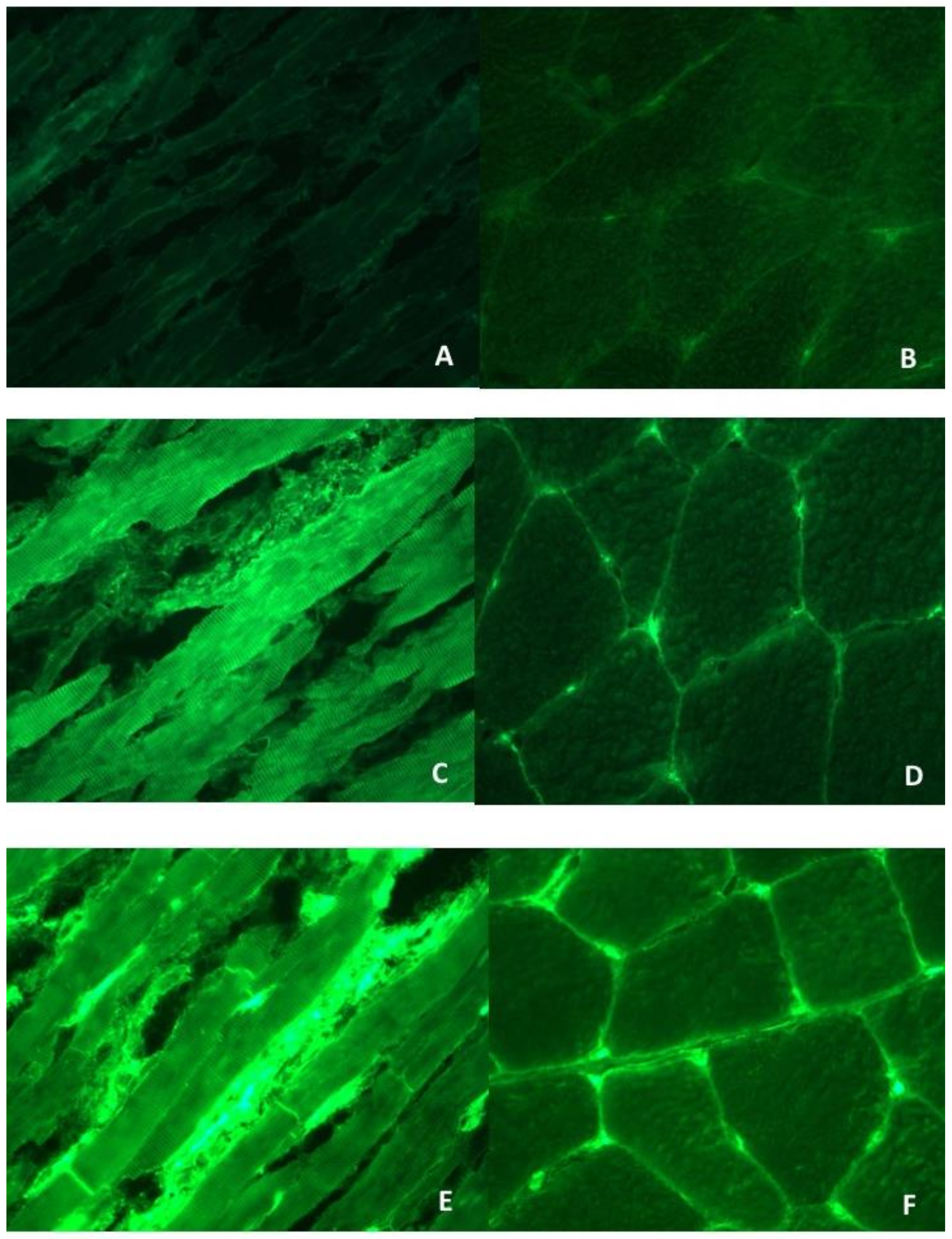
2.2. Serum AHAs and AIDAs Testing by Indirect Immunofluorescence (IFL)
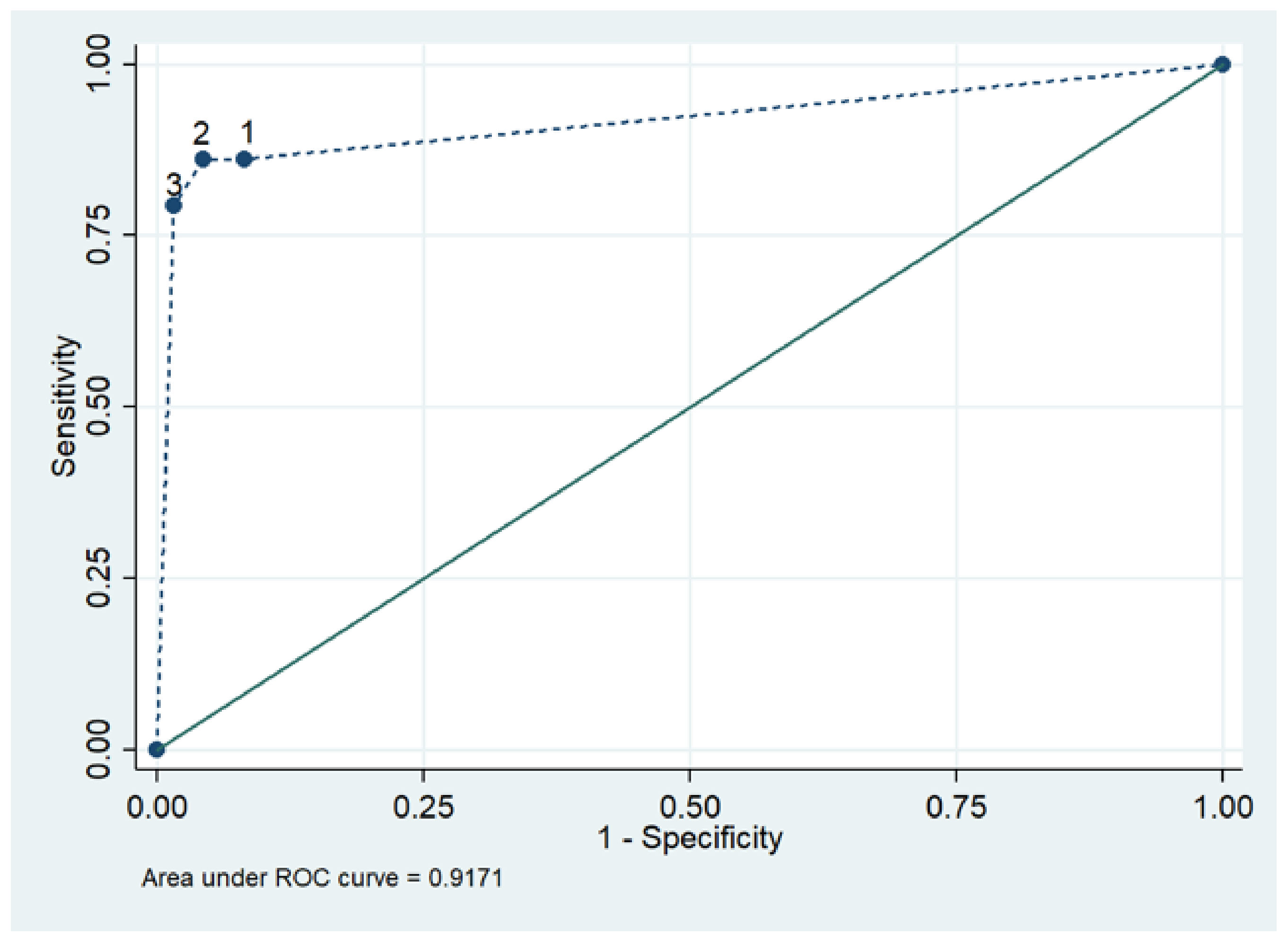
2.3. Statistical Analysis
3. Results
3.1. Clinical, Diagnostic and Imaging Features in Sarcoidosis Patients
3.2. AHA and AIDA Frequency in Sarcoidosis and Association with Clinical and Diagnostic Features
4. Discussion
4.1. Significance and Specificity of AHAs and AIDAs in Cardiac Sarcoidosis
4.2. AHAs and AIDAs as Potential Diagnostic/Prognostic Markers in Cardiac Sarcoidosis
4.3. Cardiac Sarcoidosis, Organ-Specific Myocarditis and Arrhythmogenic Right Ventricular Cardiomyopathy: Evidence for a Common Autoimmune Pathogenetic Pathway
4.4. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AHA | Anti-heart autoantibodies |
| AIDA | anti-intercalated disk autoantibodies |
| CMR | cardiac magnetic resonance |
| FDG-PET | 18-fluorodeoxyglucose positron emission tomography |
| IFL | indirect immunofluorescence |
| IHF | ischemic heart failure |
| LGE | late gadolinium enhancement |
| LVEF | left ventricular ejection fraction |
| NDB | normal blood donors |
| NICD | noninflammatory cardiac disease |
References
- Valeyre, D.; Prasse, A.; Nunes, H.; Uzunhan, Y.; Brillet, P.Y.; Muller-Quernheim, J. Sarcoidosis. Lancet 2014, 383, 1155–1167. [Google Scholar] [CrossRef]
- Hamzeh, N.; Steckman, D.A.; Sauer, W.H.; Judson, M.A. Pathophysiology and clinical management of cardiac sarcoidosis. Nat. Rev. Cardiol. 2015, 12, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Caforio, A.L.; Adler, Y.; Agostini, C.; Allanore, Y.; Anastasakis, A.; Arad, M.; Böhm, M.; Charron, P.; Elliott, P.M.; Eriksson, U.; et al. Diagnosis and management of myocardial involvement in systemic immune-mediated diseases: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Disease. Eur. Heart J. 2017, 38, 2649–2662. [Google Scholar] [CrossRef] [PubMed]
- Semenzato, G.; Bortoli, M.; Agostini, C. Applied clinical immunology in sarcoidosis. Curr. Opin. Pulm. Med. 2002, 8, 441–444. [Google Scholar] [CrossRef]
- Iwai, K.; Tachibana, T.; Takemura, T.; Matsui, Y.; Kitalchi, M.; Kawabata, Y. Pathological studies on sarcoidosis autopsy. I. Epidemiological features of 320 cases in Japan. Pathol. Int. 1993, 43, 372–376. [Google Scholar] [CrossRef]
- Kandolin, R.; Lehtonen, J.; Airaksinen, J.; Vihinen, T.; Miettinen, H.; Ylitalo, K.; Kaikkonen, K.; Tuohinen, S.; Haataja, P.; Kerola, T.; et al. Cardiac sarcoidosis: Epidemiology, characteristics, and outcome over 25 years in a nationwide study. Circulation 2015, 131, 624–632. [Google Scholar] [CrossRef]
- Chen, E.S.; Moller, D.R. Etiology of Sarcoidosis. Clin. Chest Med. 2008, 29, 365–377. [Google Scholar] [CrossRef]
- Smedema, J.-P.; Snoep, G.; van Kroonenburgh, M.P.; van Geuns, R.-J.; Dassen, W.R.; Gorgels, A.P.; Crijns, H.J. Evaluation of the Accuracy of Gadolinium-Enhanced Cardiovascular Magnetic Resonance in the Diagnosis of Cardiac Sarcoidosis. J. Am. Coll. Cardiol. 2005, 45, 1683–1690. [Google Scholar] [CrossRef]
- Broos, C.E.; Van Nimwegen, M.; Hoogsteden, H.C.; Hendriks, R.W.; Kool, M.; Blink, B.V.D. Granuloma Formation in Pulmonary Sarcoidosis. Front. Immunol. 2013, 4. [Google Scholar] [CrossRef]
- Birnie, D.H.; Kandolin, R.; Nery, P.B.; Kupari, M. Cardiac manifestations of sarcoidosis: Diagnosis and management. Eur. Heart J. 2016, 38, 2663–2670. [Google Scholar] [CrossRef]
- Birnie, D.H.; Sauer, W.H.; Bogun, F.; Cooper, J.M.; Culver, D.A.; Duvernoy, C.S.; Judson, M.A.; Kron, J.; Mehta, D.; Nielsen, J.C.; et al. HRS Expert Consensus Statement on the Diagnosis and Management of Arrhythmias Associated With Cardiac Sarcoidosis. Heart Rhythm. 2014, 11, 1304–1323. [Google Scholar] [CrossRef]
- Sadek, M.M.; Yung, D.; Birnie, D.H.; Beanlands, R.S.; Nery, P.B. Corticosteroid Therapy for Cardiac Sarcoidosis: A Systematic Review. Can. J. Cardiol. 2013, 29, 1034–1041. [Google Scholar] [CrossRef]
- Nagai, S.; Yokomatsu, T.; Tanizawa, K.; Ikezoe, K.; Handa, T.; Ito, Y.; Ogino, S.; Izumi, T. Treatment with methotrexate and low-dose corticosteroids in sarcoidosis patients with cardiac lesions. Intern. Med. 2014, 53, 2761. [Google Scholar] [CrossRef]
- Nakamura, H.; Genma, R.; Mikami, T.; Kitahara, A.; Natsume, H.; Andoh, S.; Nagasawa, S.; Nishiyama, K.; Chida, K.; Sato, A.; et al. High Incidence of Positive Autoantibodies against Thyroid Peroxidase and Thyroglobulin in Patients with Sarcoidosis. Clin. Endocrinol. 1997, 46, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Amital, H.; Klemperer, I.; Blank, M.; Yassur, Y.; Palestine, A.; Nussenblatt, R.; Shoenfeld, Y. Analysis of Autoantibodies among Patients with Primary and Secondary Uveitis: High Incidence in Patients with Sarcoidosis. Int. Arch. Allergy Immunol. 1992, 99, 34–36. [Google Scholar] [CrossRef]
- Malli, F.; Bargiota, A.; Theodoridou, K.; Florou, Z.; Bardaka, F.; Koukoulis, G.; Gourgoulianis, K.; Daniil, Z. Increased primary autoimmune thyroid diseases and thyroid antibodies in sarcoidosis: Evidence for an under-recognised extrathoracic involvement in sarcoidosis? Hormones 2012, 11, 436–443. [Google Scholar] [CrossRef]
- Caforio, A.L.; Bonifacio, E.; Stewart, J.T.; Neglia, D.; Parodi, O.; Bottazzo, G.F.; McKenna, W.J. Novel organ-specific circulating cardiac autoantibodies in dilated cardiomyopathy. J. Am. Coll. Cardiol. 1990, 15, 1527–1534. [Google Scholar] [CrossRef]
- Caforio, A.; Keeling, P.; McKenna, W.; Mann, J.; Bottazzo, G.; Zachara, E.; Mestroni, L.; Camerini, F. Evidence from family studies for autoimmunity in dilated cardiomyopathy. Lancet 1994, 344, 777. [Google Scholar] [CrossRef]
- Caforio, A.L.; Mahon, N.G.; Baig, M.K.; Tona, F.; Murphy, R.T.; Elliott, P.M.; McKenna, W.J. Prospective familial assessment in dilated cardiomyopathy: Cardiac autoantibodies predict disease development in asymptomatic relatives. Circulation 2007, 115, 76–83. [Google Scholar] [CrossRef]
- Caforio, A.L.; Calabrese, F.; Angelini, A.; Tona, F.; Vinci, A.; Bottaro, S.; Ramondo, A.; Carturan, E.; Iliceto, S.; Thiene, G.; et al. A prospective study of biopsy-proven myocarditis: Prognostic relevance of clinical and aetiopathogenetic features at diagnosis. Eur. Heart J. 2007, 28, 1326–1333. [Google Scholar] [CrossRef]
- Caforio, A.L.; Grazzini, M.; Mann, J.M.; Keeling, P.J.; Bottazzo, G.F.; McKenna, W.J.; Schiaffino, S. Identification of alpha- and beta-cardiac myosin heavy chain isoforms as major autoantigens in dilated cardiomyopathy. Circulation 1992, 85, 1734–1742. [Google Scholar] [CrossRef] [PubMed]
- Caforio, A.L.P.; Brucato, A.; Doria, A.; Brambilla, G.; Angelini, A.; Ghirardello, A.; Bottaro, S.; Tona, F.; Betterle, C.; Daliento, L.; et al. Anti-heart and anti-intercalated disk autoantibodies: Evidence for autoimmunity in idiopathic recurrent acute pericarditis. Heart 2010, 96, 779–784. [Google Scholar] [CrossRef] [PubMed]
- Caforio, A.L.P.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Heliö, T.; Heymans, S.; Jahns, R.; et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2013, 34, 2636–2648. [Google Scholar] [CrossRef] [PubMed]
- Ramstein, J.; Broos, C.E.; Simpson, L.J.; Ansel, K.M.; Sun, S.A.; Ho, M.E.; Woodruff, P.G.; Bhakta, N.R.; Christian, L.; Nguyen, C.P.; et al. IFN-γ–Producing T-Helper 17.1 Cells Are Increased in Sarcoidosis and Are More Prevalent than T-Helper Type 1 Cells. Am. J. Respir. Crit. Care Med. 2016, 193, 1281–1291. [Google Scholar] [CrossRef] [PubMed]
- Kamphuis, L.S.; Van Zelm, M.C.; Lam, K.H.; Rimmelzwaan, G.F.; Baarsma, G.S.; Dik, W.A.; Thio, H.B.; Van Daele, P.L.; Van Velthoven, M.E.; Batstra, M.R.; et al. Perigranuloma localization and abnormal maturation of B cells: Emerging key players in sarcoidosis? Am. J. Respir. Crit. Care Med. 2013, 187, 406–416. [Google Scholar] [CrossRef]
- Tschöpe, C.; Ammirati, E.; Bozkurt, B.; Caforio, A.L.P.; Cooper, L.T.; Felix, S.B.; Hare, J.M.; Heidecker, B.; Heymans, S.; Hübner, N.; et al. Myocarditis and inflammatory cardiomyopathy: Current evidence and future directions. Nat. Rev. Cardiol. 2021, 18, 169–193. [Google Scholar] [CrossRef]
- Liang, J.J.; Hebl, V.B.; DeSimone, C.V.; Madhavan, M.; Nanda, S.; Kapa, S.; Maleszewski, J.J.; Edwards, W.D.; Reeder, G.; Cooper, L.T.; et al. Electrogram guidance: A method to increase the precision and diagnostic yield of endomyocardial biopsy for suspected cardiac sarcoidosis and myocarditis. JACC Heart Fail 2014, 2, 466–473. [Google Scholar] [CrossRef]
- Nery, P.B.; Keren, A.; Healey, J.; Leug, E.; Beanlands, R.S.; Birnie, D.H. Isolated Cardiac Sarcoidosis: Establishing the Diagnosis With Electroanatomic Mapping-Guided Endomyocardial Biopsy. Can. J. Cardiol. 2013, 29, 1015.e1. [Google Scholar] [CrossRef]
- Caforio, A.L.; Re, F.; Avella, A.; Marcolongo, R.; Baratta, P.; Seguso, M.; Gallo, N.; Plebani, M.; Izquierdo-Bajo, A.; Cheng, C.Y.; et al. Evidence from family studies for autoimmunity in arrhythmogenic right ventricular cardiomyopathy: Associations of circulating anti-heart and anti-intercalated disk autoantibodies with disease severity and family history. Circulation 2020, 141, 1238–1248. [Google Scholar] [CrossRef]
- Cooper, L.T., Jr.; Hare, J.M.; Tazelaar, H.D.; Edwards, W.D.; Starling, R.C.; Deng, M.C.; Menon, S.; Mullen, G.M.; Jaski, B.; Bailey, K.R.; et al. Giant Cell Myocarditis Treatment Trial Investigators. Usefulness of immunosuppression for giant cell myocarditis. Am. J. Cardiol. 2008, 102, 1535–1539. [Google Scholar] [CrossRef]
- Cunningham, M.W. Turning point in myocarditis. Circ. Res. 2009, 105, 403–405. [Google Scholar] [CrossRef]
- Marin-Neto, J.A.; Cunha-Neto, E.; Maciel, B.C.; Simões, M.V. Pathogenesis of chronic Chagas heart disease. Circulation 2007, 115, 1109–1123. [Google Scholar] [CrossRef]
- Chatterjee, D.; Fatah, M.; Akdis, D.; Spears, D.A.; Koopmann, T.T.; Mittal, K.; Rafiq, M.A.; Cattanach, B.M.; Zhao, Q.; Healey, J.S.; et al. An autoantibody identifies arrhythmogenic right ventricular cardiomyopathy and participates in its pathogenesis. Eur. Heart J. 2018, 39, 3932–3944. [Google Scholar] [CrossRef]
- Chatterjee, D.; Pieroni, M.; Fatah, M.; Charpentier, F.; Cunningham, K.S.; Spears, D.A.; Chatterjee, D.; Suna, G.; Bos, J.M.; Ackerman, M.J.; et al. An autoantibody profile detects Brugada syndrome and identifies abnormally expressed myocardial proteins. Eur. Heart J. 2020, 41, 2878–2890. [Google Scholar] [CrossRef]
- Komarowska, I.; Coe, D.; Wang, G.; Haas, R.; Mauro, C.; Kishore, M.; Cooper, D.; Nadkarni, S.; Fu, H.; Steinbruchel, D.A.; et al. Hepatocyte Growth Factor Receptor c-Met Instructs T Cell Cardiotropism and Promotes T Cell Migration to the Heart via Autocrine Chemokine Release. Immunity 2015, 42, 1087–1099. [Google Scholar] [CrossRef]
- Honda, Y.; Nagai, T.; Ikeda, Y.; Sakakibara, M.; Asakawa, N.; Nagano, N.; Nakai, M.; Nishimura, K.; Sugano, Y.; Ohta-Ogo, K.; et al. Myocardial Immunocompetent Cells and Macrophage Phenotypes as Histopathological Surrogates for Diagnosis of Cardiac Sarcoidosis in Japanese. J. Am. Heart Assoc. 2016, 5, e004019. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Age at diagnosis of sarcoidosis, mean ± standard deviation | 46 ± 12 |
| Age at diagnosis of cardiac sarcoidosis, mean ± standard deviation | 49 ± 11 |
| Female sex, n (%) | 9 (31) |
| Race, n (%) Caucasian African American Hispanic | 22 (76) 5 (17) 2 (7) |
| Former or active smoker | 8 (28) |
| Dyspnea, n (%) | 4 (14) |
| Chest pain, n (%) | 3 (10) |
| Palpitations, n (%) | 9 (31) |
| Syncope, n (%) | 4 (14) |
| Pericardial effusion, n (%) | 1 (3) |
| More than one symptom, n (%) | 2 (7) |
| Implantable cardioverter defibrillator, n (%) | 20 (69) |
| Arrhythmia at onset, n (%): Complete heart block Ventricular tachycardia | 1 (3) 1 (3) |
| Lung involvement, n (%) | 25 (86) |
| Eye involvement, n (%) | 4 (14) |
| Liver involvement, n (%) | 3 (10) |
| Skin involvement, n (%) | 7 (24) |
| Small fiber neuropathy, n (%) | 1 (3) |
| Pulmonary hypertension, n (%) | 1 (3) |
| Other organ involvement, n (%) | 7 (24) |
| Number of involved organs, mean ± standard deviation | 1.8 ± 1.1 |
| 12-lead electrocardiogram, n, (%): | |
| Sinus rhythm Atrial fibrillation Pacemaker | 24(83) 2 (7) 3 (10) |
| Atrioventricular block, 1st degree Atrioventricular block, 2nd degree Atrioventricular block, 3rd degree | 3 (10) 0 (0) 3 (10) |
| QRS morphology: Right bundle branch block Left bundle branch or left ventricular anterior hemiblock Nonspecific intraventricular block | 11 (38) 3 (10) 2 (7) |
| 24 h Holter monitoring (n = 21), n (%): | |
| Frequent ventricular ectopy (<6% of total) | 5 (24) |
| Nonsustained ventricular tachycardia | 4 (19) |
| Sustained ventricular tachycardia | 2 (10) |
| 2D transthoracic echocardiography: | |
| LVEF, mean ± standard deviation Left ventricular hypertrophy, n (%) Left ventricular dilatation, n (%) Left ventricular diastolic dysfunction, n (%) Right ventricular dilatation, n (%) Right ventricular dysfunction, n (%) Left atrial dilatation, n (%) | 60 ± 7.6 1 (3) 1 (3) 13 (46) 6 (21) 3 (10) 6 (21) |
| Normal coronary angiography, (n = 9) *remainder not done | 9 (100%) |
| Cardiac magnetic resonance imaging (n = 23): Left ventricular ejection fraction, mean (SD) Late gadolinium enhancement, present, n (%) Edema, present, n (%) Late gadolinium enhancement, distribution, n (%): Septum Anterior wall Lateral wall Inferior wall Right ventricle >1 location Late gadolinium enhancement pattern, n (%): Spots Intramural striae Subepicardial striae Subendocardial striae Overall heart involvement, n (%) | 60 ± 8.2 20 (87) 4 (17) 6 (26) 3 (13) 2 (9) 1 (4) 1 (4) 6 (26) 9 (39) 3 (13) 1 (4) 2 (9) 19 (83%) |
| Positron emission tomography hypermetabolism (n = 18): Right atrial, n (%) Left atrial, n (%) Left ventricular septum, n (%) Left ventricular anterior wall, n (%) Left ventricular inferolateral wall, n (%) Left ventricular >1 location, n (%) Right ventricle, n (%) Overall heart involvement, n (%) | 1 (6) 2 (11) 1 (6) 2 (11) 2 (11) 6 (33) 6 (33) 12 (67) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caforio, A.L.P.; Baritussio, A.; Marcolongo, R.; Cheng, C.-Y.; Pontara, E.; Bison, E.; Cattini, M.G.; Gallo, N.; Plebani, M.; Iliceto, S.; et al. Serum Anti-Heart and Anti-Intercalated Disk Autoantibodies: Novel Autoimmune Markers in Cardiac Sarcoidosis. J. Clin. Med. 2021, 10, 2476. https://doi.org/10.3390/jcm10112476
Caforio ALP, Baritussio A, Marcolongo R, Cheng C-Y, Pontara E, Bison E, Cattini MG, Gallo N, Plebani M, Iliceto S, et al. Serum Anti-Heart and Anti-Intercalated Disk Autoantibodies: Novel Autoimmune Markers in Cardiac Sarcoidosis. Journal of Clinical Medicine. 2021; 10(11):2476. https://doi.org/10.3390/jcm10112476
Chicago/Turabian StyleCaforio, Alida L. P., Anna Baritussio, Renzo Marcolongo, Chun-Yan Cheng, Elena Pontara, Elisa Bison, Maria Grazia Cattini, Nicoletta Gallo, Mario Plebani, Sabino Iliceto, and et al. 2021. "Serum Anti-Heart and Anti-Intercalated Disk Autoantibodies: Novel Autoimmune Markers in Cardiac Sarcoidosis" Journal of Clinical Medicine 10, no. 11: 2476. https://doi.org/10.3390/jcm10112476
APA StyleCaforio, A. L. P., Baritussio, A., Marcolongo, R., Cheng, C.-Y., Pontara, E., Bison, E., Cattini, M. G., Gallo, N., Plebani, M., Iliceto, S., Semenzato, G., Maier, L., & Hamzeh, N. (2021). Serum Anti-Heart and Anti-Intercalated Disk Autoantibodies: Novel Autoimmune Markers in Cardiac Sarcoidosis. Journal of Clinical Medicine, 10(11), 2476. https://doi.org/10.3390/jcm10112476