
Characteristics and Survival of Intensive Care Unit Patients with Coronavirus Disease in Osaka, Japan: A Retrospective Observational Study

 , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Population, Design, and Setting
2.2. Measurements
2.3. Outcomes and Follow-Up Period
2.4. Statistical Analysis
3. Results
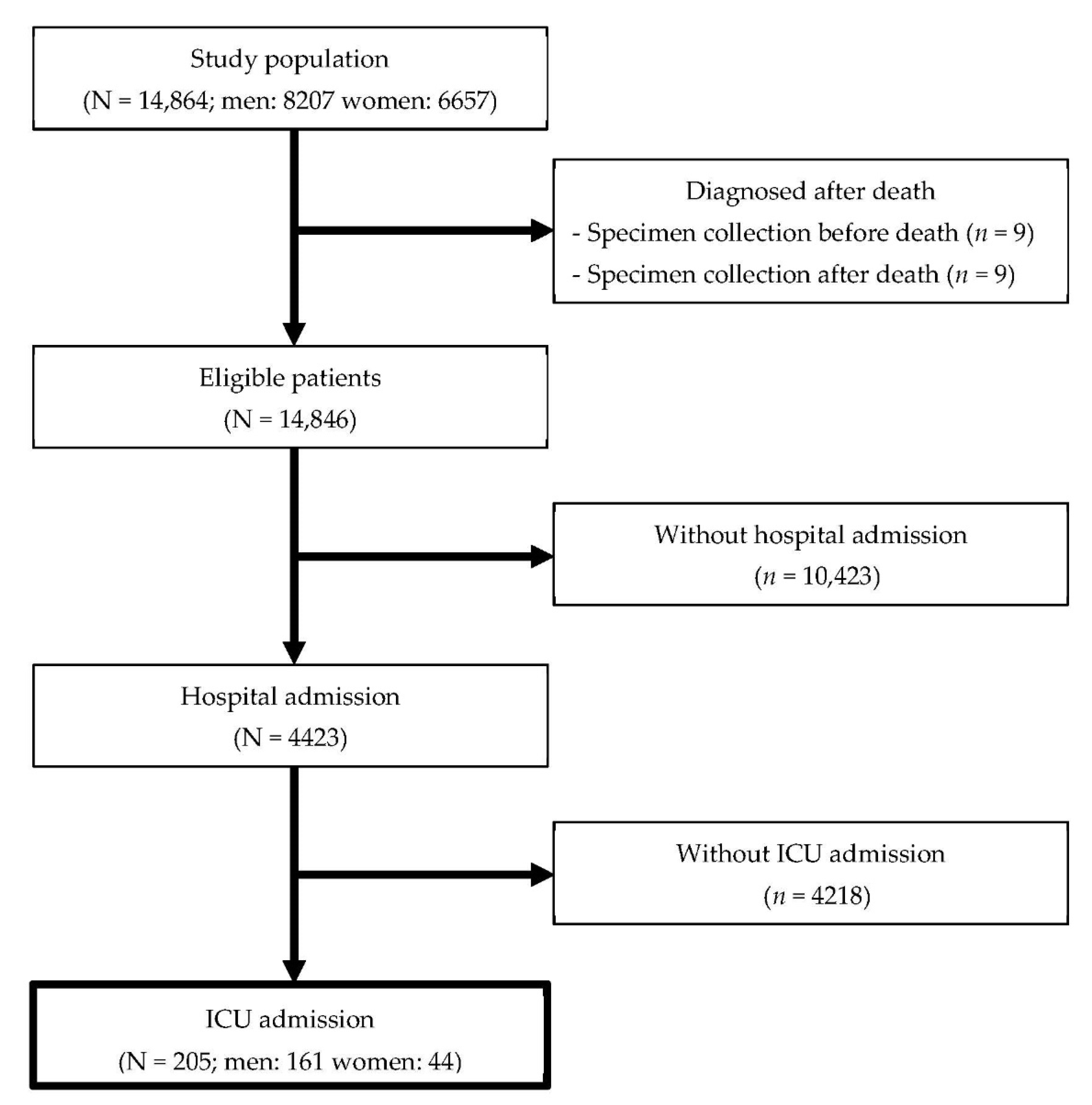
3.1. Eligible Patients
3.2. The Description of Baseline Features
3.3. The Description of Clinical Features
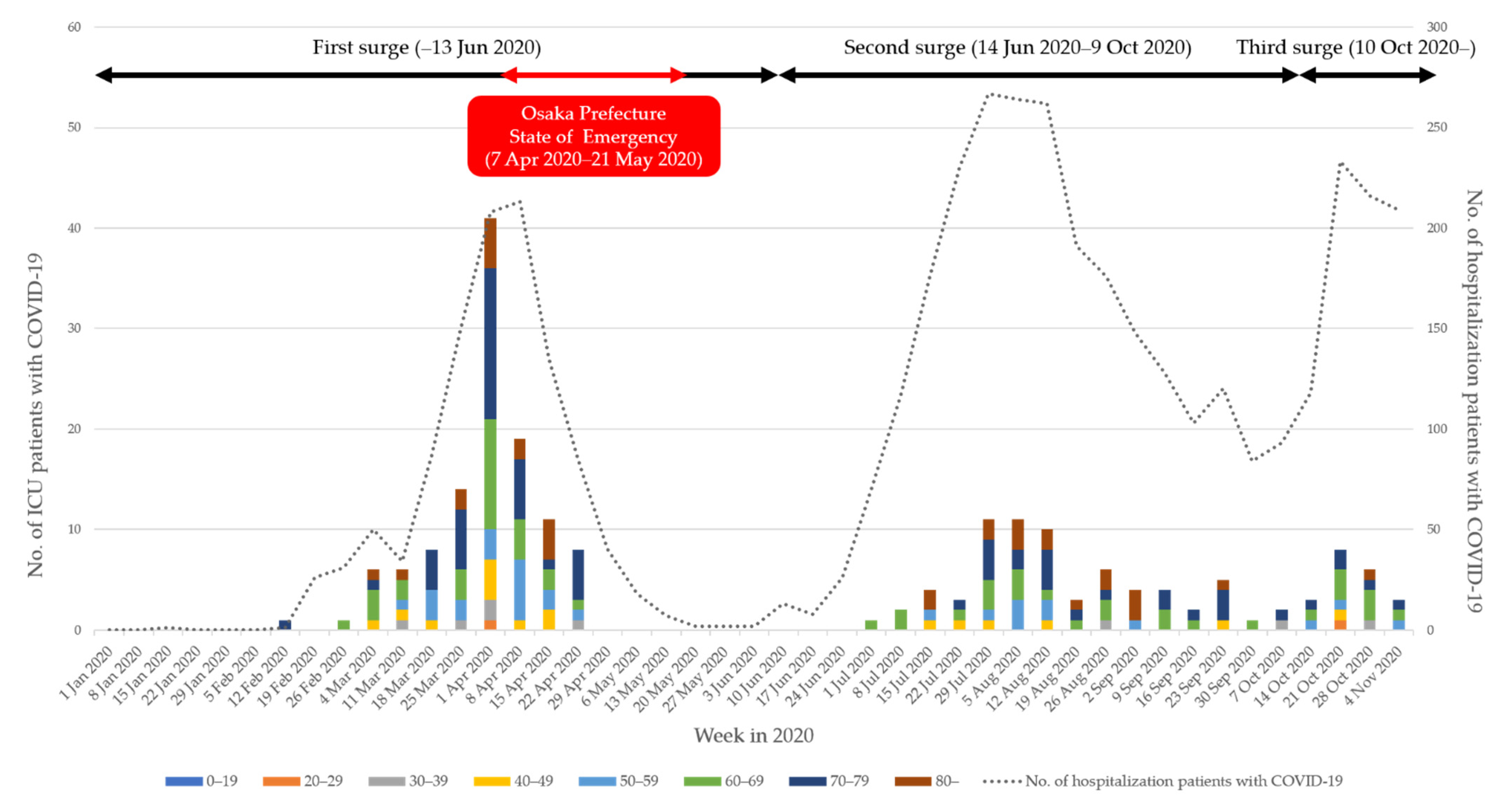
3.4. Weekly Incident Pattern of ICU Patients with COVID-19
3.5. Factors Related to Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Covid-19 Coronavirus Pandemic. Available online: https://www.worldometers.info/coronavirus/ (accessed on 23 March 2021).
- Rieg, S.; von Cube, M.; Kalbhenn, J.; Utzolino, S.; Pernice, K.; Bechet, L.; Baur, J.; Lang, C.N.; Wagner, D.; Wolkewitz, M. COVID-19 in-hospital mortality and mode of death in a dynamic and non-restricted tertiary care model in Germany. PLoS ONE 2020, 15, e0242127. [Google Scholar] [CrossRef] [PubMed]
- Laake, J.H.; Buanes, E.A.; Småstuen, M.C.; Kvåle, R.; Olsen, B.F.; Rustøen, T.; Strand, K.; Sørensen, V.; Hofsø, K. Characteristics, management and survival of ICU patients with coronavirus disease-19 in Norway, March-June 2020. A prospective observational study. Acta Anaesthesiol. Scand. 2021, 65, 618–628. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Greco, M.; Zanella, A.; Albano, G.; Antonelli, M.; Bellani, G.; Bonanomi, E.; Cabrini, L.; Carlesso, E.; Castelli, G. Risk factors associated with mortality among patients with COVID-19 in intensive care units in Lombardy, Italy. JAMA Intern. Med. 2020, 180, 1345–1355. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Bulletin Board. Available online: https://covid-2019.live/?from=groupmessage (accessed on 23 March 2021).
- Matsunaga, N.; Hayakawa, K.; Terada, M.; Ohtsu, H.; Asai, Y.; Tsuzuki, S.; Suzuki, S.; Toyoda, A.; Suzuki, K.; Endo, M. Clinical Epidemiology of Hospitalized Patients With Coronavirus Disease 2019 (COVID-19) in Japan: Report of the COVID-19 Registry Japan. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Osaka Prefectural Government Press Release on Providing New Coronavirus Patient Data to Academic Research Institutes. Available online: http://www.pref.osaka.lg.jp/hodo/index.php?site=fumin&Pageid=39707 (accessed on 10 March 2021).
- Ministry of Health, Labour and Welfare Treatment guidelines Version 4.2 of COVID-19 Infection. 2021. Available online: https://www.mhlw.go.jp/content/000742297.pdf (accessed on 10 March 2021).
- Osaka Prefectural Government Monthly Estimated Population of Osaka Prefecture. Available online: http://www.pref.osaka.lg.jp/toukei/jinkou/ (accessed on 10 March 2021).
- Hirayama, A.; Masui, J.; Murayama, A.; Fujita, S.; Okamoto, J.; Tanaka, J.; Hirayama, T.; Ohara, T.; Hoffmann, E.N.; Zhang, J. The characteristics and clinical course of patients with COVID-19 who received invasive mechanical ventilation in Osaka, Japan. Int. J. Infect. Dis. 2021, 102, 282–284. [Google Scholar] [CrossRef] [PubMed]
- Osaka Prefectural Government Osaka Prefecture New Coronavirus Countermeasures Headquarters Meeting. Available online: http://www.pref.osaka.lg.jp/kikaku_keikaku/sarscov2/ (accessed on 10 March 2021).
- National Institute of Infectious Diseases Guidelines for Conducting Active Epidemiological Surveillance of Patients with Novel Coronavirus Infections. Available online: https://www.niid.go.jp/niid/images/epi/corona/COVID19-02-210108.pdf (accessed on 10 March 2021).
- Takeuchi, T.; Imanaka, T.; Katayama, Y.; Kitamura, T.; Sobue, T.; Shimazu, T. Profile of patients with novel coronavirus disease 2019 (COVID-19) in Osaka Prefecture, Japan: A population-based descriptive study. J. Clin. Med. 2020, 9, 2925. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; Yu, T. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef]
- Bhatraju, P.K.; Ghassemieh, B.J.; Nichols, M.; Kim, R.; Jerome, K.R.; Nalla, A.K.; Greninger, A.L.; Pipavath, S.; Wurfel, M.M.; Evans, L. Covid-19 in critically ill patients in the Seattle region—case series. N. Engl. J. Med. 2020, 382, 2012–2022. [Google Scholar] [CrossRef] [PubMed]
- House, N.; Holborn, H.; Wc, L. ICNARC report on COVID-19 in critical care. ICNARC 2020, 17, 1–26. [Google Scholar]
- Argenziano, M.G.; Bruce, S.L.; Slater, C.L.; Tiao, J.R.; Baldwin, M.R.; Barr, R.G.; Chang, B.P.; Chau, K.H.; Choi, J.J.; Gavin, N. Characterization and clinical course of 1000 patients with coronavirus disease 2019 in New York: Retrospective case series. BMJ 2020, 369. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, T.; Kitamura, T.; Hirayama, A.; Katayama, Y.; Shimazu, T.; Sobue, T. Characteristics of patients with novel coronavirus disease (COVID-19) during the first surge versus the second surge of infections in Osaka Prefecture, Japan. Glob. Health Med. 2020. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group. Dexamethasone in hospitalized patients with Covid-19—preliminary report. N. Engl. J. Med. 2020, 384, 693–704. [Google Scholar]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S. Remdesivir for the treatment of Covid-19. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Factor | Total | Survivors | Deaths | p-Value | ||
|---|---|---|---|---|---|---|
| N | N | (%) | N | (%) | ||
| No. of patients | 205 | 147 | (71.7) | 58 | (28.3) | |
| Sex | 0.584 a | |||||
| Men | 161 | 114 | (70.8) | 47 | (29.2) | |
| Women | 44 | 33 | (75.0) | 11 | (25.0) | |
| Age group, y | <0.001 b | |||||
| 0–19 | 1 | 1 | (100.0) | 0 | (0.0) | |
| 20–29 | 2 | 2 | (100.0) | 0 | (0.0) | |
| 30–39 | 8 | 8 | (100.0) | 0 | (0.0) | |
| 40–49 | 16 | 14 | (87.5) | 2 | (12.5) | |
| 50–59 | 29 | 26 | (89.7) | 3 | (10.3) | |
| 60–69 | 53 | 42 | (79.2) | 11 | (20.8) | |
| 70–79 | 64 | 41 | (64.1) | 23 | (35.9) | |
| ≥80 | 32 | 13 | (40.6) | 19 | (59.4) | |
| Geographic area | 0.814 b | |||||
| Osaka City | 128 | 92 | (71.9) | 36 | (28.1) | |
| Other areas in Osaka Prefecture | 73 | 51 | (69.9) | 22 | (30.1) | |
| Outside Osaka Prefecture | 3 | 3 | (100.0) | 0 | (0.0) | |
| Unknown | 1 | 1 | (100.0) | 0 | (0.0) | |
| Comorbidities | 0.013 a | |||||
| No | 88 | 71 | (80.7) | 17 | (19.3) | |
| Yes | 117 | 76 | (65.0) | 41 | (35.0) | |
| Symptoms at diagnosis | 0.010 b | |||||
| Asymptomatic | 0 | 0 | NA | 0 | NA | |
| Mild | 131 | 101 | (77.1) | 30 | (22.9) | |
| Moderate | 3 | 1 | (33.3) | 2 | (66.7) | |
| Severe | 69 | 45 | (65.2) | 24 | (34.8) | |
| Unknown | 2 | 0 | (0.0) | 2 | (100.0) | |
| Surge | ||||||
| First (~13 June) | 116 | 77 | (66.4) | 39 | (33.6) | 0.120 a |
| Second (14 June ~9 October) | 67 | 54 | (80.6) | 13 | (19.4) | |
| Third (10 October~) | 22 | 16 | (72.7) | 6 | (27.3) | |
| Cluster | ||||||
| No | 203 | 146 | (71.9) | 57 | (28.1) | 0.487 b |
| Yes | 2 | 1 | (50.0) | 1 | (50.0) | |
| Close contact | ||||||
| No | 173 | 126 | (72.8) | 47 | (27.2) | 0.406 a |
| Yes | 32 | 21 | (65.6) | 11 | (34.4) | |
| Factor | Total | Survivors | Deaths | p-Value | |||
|---|---|---|---|---|---|---|---|
| No. of patients, n (%) | 205 | 147 | (71.7) | 58 | (28.3) | ||
| Days from onset date to ICU admission, median days (IQR) | 10 | (7, 12) | 10 | (8, 12) | 8 | (5, 11) | 0.023 a |
| Length of ICU stay, median days (IQR) | 14 | (9, 25) | 13 | (9, 21) | 18 | (9, 28) | 0.177 a |
| Oxygen therapy, n (%) | |||||||
| No | 9 | 4 | (44.4) | 5 | (55.6) | 0.063 b | |
| Yes | 196 | 143 | (73.0) | 53 | (27.0) | ||
| Length of oxygen therapy, median days (IQR) c | 16 | (10, 27) | 14.5 | (10, 27) | 18 | (10, 26) | 0.373 a |
| Mechanical ventilator d, n (%) | |||||||
| No | 18 | 13 | (72.2) | 5 | (27.8) | 0.960 b | |
| Yes | 187 | 134 | (71.7) | 53 | (28.3) | ||
| Length of mechanical ventilator, median days (IQR) | 13 | (8, 23) | 13 | (8, 22) | 17 | (10, 26.5) | 0.030 a |
| Dialysis, n (%) | |||||||
| No | 196 | 143 | (73.0) | 53 | (27.0) | 0.063 b | |
| Yes | 9 | 4 | (44.4) | 5 | (55.6) | ||
| Length of tracheal intubation, median days (IQR) | 14 | (13, 18) | 14 | (13, 14) | 18 | (12, 21) | 0.507 a |
| Extracorporeal membrane oxygenation, n (%) | |||||||
| No | 173 | 125 | (72.3) | 48 | (27.7) | 0.690 b | |
| Yes | 32 | 22 | (68.8) | 10 | (31.3) | ||
| Length of ECMO, median days (IQR) | 15 | (10, 19) | 15 | (10, 17.5) | 12 | (2, 20) | 0.705 a |
| Variables | No. of Deaths | Person-Days | Crude Rate | Univariable | Multivariable | ||
|---|---|---|---|---|---|---|---|
| (Per 100) | HR | (95% CI) | HR | (95% CI) | |||
| Sex | |||||||
| Men | 47 | 4449 | 1.06 | Reference | Reference | ||
| Women | 11 | 1429 | 0.77 | 0.75 | (0.36–1.46) | 0.60 | (0.30–1.22) |
| Age group, y | |||||||
| 0–59 | 5 | 1320 | 0.38 | Reference | Reference | ||
| 60–69 | 11 | 1719 | 0.64 | 1.74 | (0.60–5.03) | 2.00 | (0.68–5.84) |
| 70–79 | 23 | 1829 | 1.26 | 3.03 | (1.15–8.02) | 3.13 | (1.15–8.48) |
| ≥80 | 19 | 1010 | 1.88 | 4.84 | (1.80–12.99) | 6.02 | (2.10–17.25) |
| Residence | |||||||
| Osaka City | 36 | 3685 | 0.98 | Reference | Reference | ||
| Other cities | 22 | 2193 | 1.00 | 1.04 | (0.61–1.77) | 1.34 | (0.74–2.42) |
| Comorbidities | |||||||
| No | 17 | 2447 | 0.69 | Reference | Reference | ||
| Yes | 41 | 3431 | 1.19 | 1.83 | (1.04–3.22) | 1.43 | (0.76–2.69) |
| Symptoms at diagnosis, n (%) | |||||||
| Mild | 30 | 3445 | 0.87 | Reference | Reference | ||
| Moderate~Severe | 26 | 2377 | 1.09 | 1.34 | (0.79–2.27) | 1.27 | (0.72–2.24) |
| Unknown | 2 | 56 | 3.57 | 3.91 | (0.93–16.43) | 2.49 | (0.53–11.64) |
| Surge | |||||||
| First (~13 June) | 39 | 3717 | 1.05 | Reference | Reference | ||
| Second (14 June~9 October) | 13 | 1697 | 0.77 | 0.74 | (0.39–1.39) | 0.56 | (0.28–1.10) |
| Third (10 October~) | 6 | 464 | 1.29 | 1.19 | (0.50–2.83) | 1.43 | (0.58–3.54) |
| Cluster | |||||||
| No | 57 | 5844 | 0.98 | Reference | Reference | ||
| Yes | 1 | 34 | 2.94 | 3.26 | (0.45–23.92) | 4.23 | (0.49–36.41) |
| Close contact | |||||||
| No | 47 | 5006 | 0.94 | Reference | Reference | ||
| Yes | 11 | 872 | 1.26 | 1.31 | (0.68–2.54) | 1.20 | (0.58–2.45) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zha, L.; Sobue, T.; Takeuchi, T.; Tanaka, K.; Katayama, Y.; Komukai, S.; Hirayama, A.; Shimazu, T.; Kitamura, T.; the COVID-19 Epidemiology Research Group of Osaka University. Characteristics and Survival of Intensive Care Unit Patients with Coronavirus Disease in Osaka, Japan: A Retrospective Observational Study. J. Clin. Med. 2021, 10, 2477. https://doi.org/10.3390/jcm10112477
Zha L, Sobue T, Takeuchi T, Tanaka K, Katayama Y, Komukai S, Hirayama A, Shimazu T, Kitamura T, the COVID-19 Epidemiology Research Group of Osaka University. Characteristics and Survival of Intensive Care Unit Patients with Coronavirus Disease in Osaka, Japan: A Retrospective Observational Study. Journal of Clinical Medicine. 2021; 10(11):2477. https://doi.org/10.3390/jcm10112477
Chicago/Turabian StyleZha, Ling, Tomotaka Sobue, Taro Takeuchi, Kenta Tanaka, Yusuke Katayama, Sho Komukai, Atsushi Hirayama, Takeshi Shimazu, Tetsuhisa Kitamura, and the COVID-19 Epidemiology Research Group of Osaka University. 2021. "Characteristics and Survival of Intensive Care Unit Patients with Coronavirus Disease in Osaka, Japan: A Retrospective Observational Study" Journal of Clinical Medicine 10, no. 11: 2477. https://doi.org/10.3390/jcm10112477
APA StyleZha, L., Sobue, T., Takeuchi, T., Tanaka, K., Katayama, Y., Komukai, S., Hirayama, A., Shimazu, T., Kitamura, T., & the COVID-19 Epidemiology Research Group of Osaka University. (2021). Characteristics and Survival of Intensive Care Unit Patients with Coronavirus Disease in Osaka, Japan: A Retrospective Observational Study. Journal of Clinical Medicine, 10(11), 2477. https://doi.org/10.3390/jcm10112477