
Poor Vaccine Effectiveness against Influenza B-Related Severe Acute Respiratory Infection in a Temperate North Indian State (2019–2020): A Call for Further Data for Possible Vaccines with Closer Match


Abstract
:1. Introduction
2. Methods
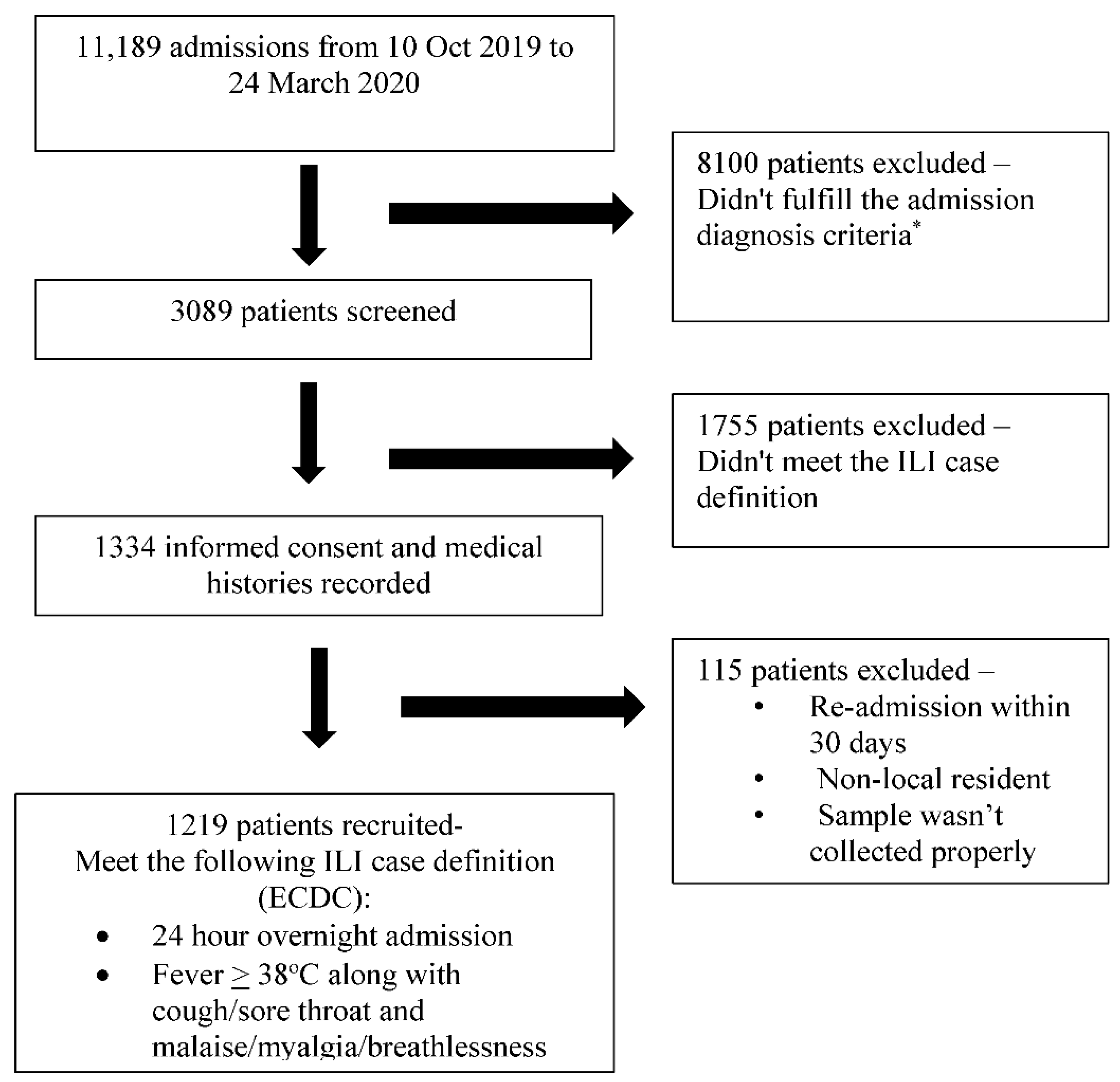
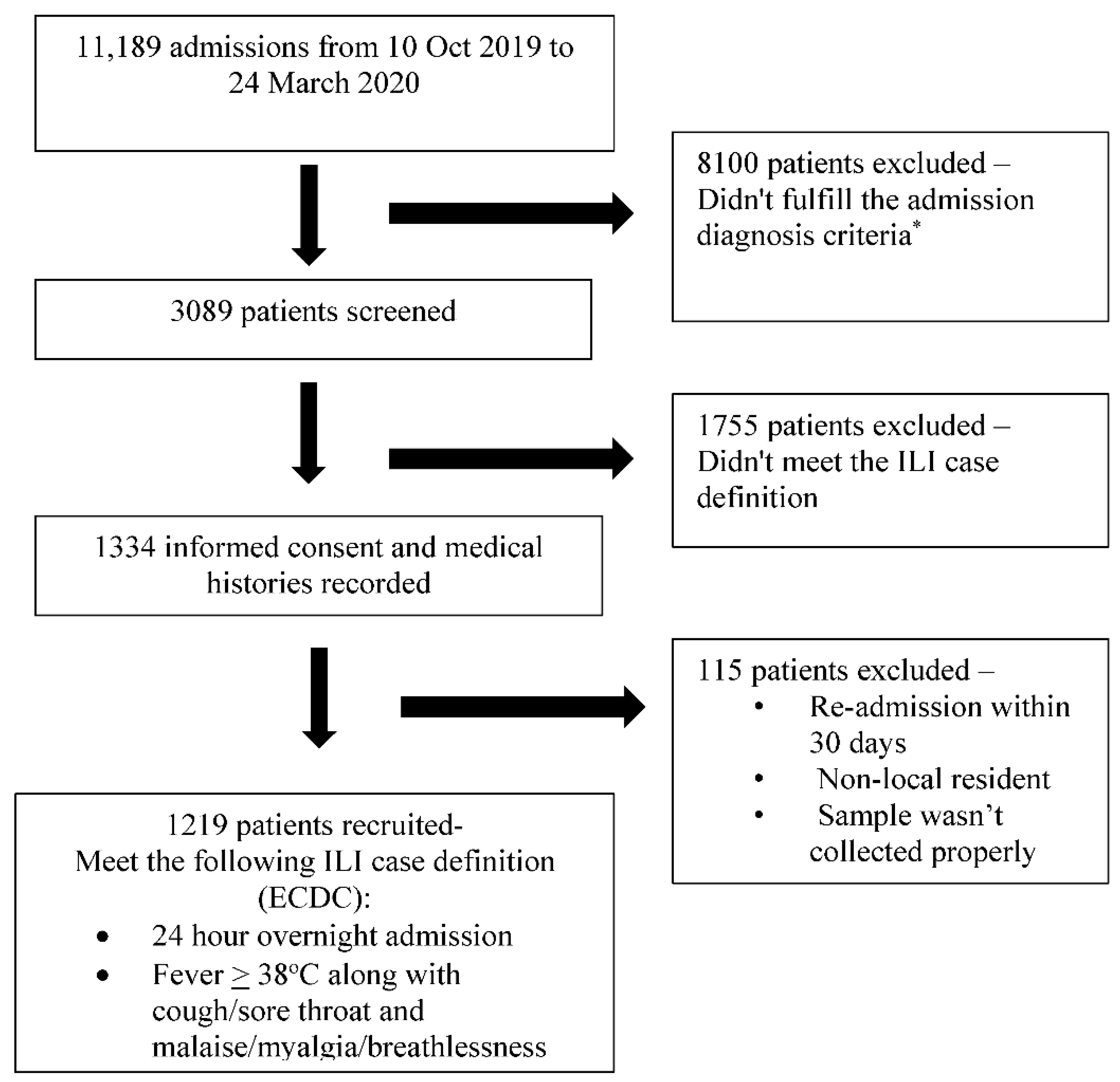
2.1. Setting and Study Population
2.2. Influenza Vaccine Composition for 2019–2020 Season
2.3. Laboratory Investigations
2.4. Estimation of Vaccine Effectiveness (VE)
2.5. Ethics Approval
3. Results
4. Discussion
5. Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Iuliano, A.D.; Roguski, K.M.; Chang, H.H.; Muscatello, D.J.; Palekar, R.; Tempia, S.; Cohen, C.; Gran, J.M.; Schanzer, D.; Cowling, B.; et al. Estimates of global seasonal influenza-associated respiratory mortality: A modelling study. Lancet 2017, 391, 1285–1300. [Google Scholar] [CrossRef]
- Lafond, K.E.; Porter, R.M.; Whaley, M.J.; Suizan, Z.; Ran, Z.; Aleem, M.A.; Thapa, B.; Sar, B.; Proschle, V.S.; Peng, Z.; et al. Global burden of influenza-associated lower respiratory tract infections and hospitalizations among adults: A systematic review and meta-analysis. PLoS Med. 2021, 18, e1003550. [Google Scholar] [CrossRef] [PubMed]
- Koul, P.A.; Mir, M.A.; Bali, N.K.; Sarkar, M.C.; Sarkar, M.; Kaushik, S.; Khan, U.H.; Ahmad, F.; Garten, R.; Lal, R.B.; et al. Pandemic and seasonal flu viruses amongst patients with acute respiratory illness in Kashmir (India). Influenza Other Respir. Viruses 2011, 5, e521–e527. [Google Scholar] [CrossRef] [Green Version]
- Narayan, V.V.; Iuliano, A.D.; Roguski, K.; Bhardwaj, R.; Chadha, M.; Saha, S.; Khan, U.H.; Ahmad, F.; Garten, R.; Lal, R.B.; et al. Burden of influenza-associated respiratory and circulatory mortality in India, 2010–2013. J. Glob. Health 2020, 10, 010402. [Google Scholar] [CrossRef] [PubMed]
- Bali, N.K.; Ashraf, M.; Ahmad, F.; Khan, U.H.; Widdowson, M.-A.; Lal, R.B.; Koul, P.A. Knowledge, attitude, and practices about the seasonal influenza vaccination among healthcare workers in Srinagar, India. Influenza Other Respir. Viruses 2012, 7, 540–545. [Google Scholar] [CrossRef]
- Koul, P.A.; Ali, S.; Mir, H.; Ahmad, S.J.; Bhat, S.A.; Bhat, M.A. Influenza vaccination in north Indian patients with heart failure. Indian Heart J. 2016, 69, 28–31. [Google Scholar] [CrossRef] [Green Version]
- Gnatiuc, L.; Buist, A.S.; Kato, B.; Janson, C.; Aït-Khaled, N.; Nielsen, R.; Koul, P.A.; Nizankowska-Mogilnicka, E.; Obaseki, D.; Idolor, L.F.; et al. Gaps in using bronchodilators, inhaled corticosteroids and influenza vaccine among 23 high- and low-income sites. Int. J. Tuberc. Lung Dis. 2015, 19, 21–30. [Google Scholar] [CrossRef] [Green Version]
- Koul, P.A.; Bhat, M.A.; Ali, S.; Rahim, S.; Ahmad, S.; Masoodi, S.R. Influennza and Pneumococcal vaccination in patients with diabetes. J. Diabetol. 2014, 2, 5. [Google Scholar]
- Koul, P.A.; Bali, N.K.; Ali, S.; Ahmad, S.J.; Bhat, M.A.; Mir, H. Poor influenza vaccination in pregnant females in north India. Int. J. Gynecol. Obstet. 2014, 127, 234–237. [Google Scholar] [CrossRef] [PubMed]
- Muruganathan, A.; Guha, S.; Munjal, Y.P.; Agarwal, S.S.; Parikh, K.K.; Jha, V. Recommendations for Vaccination Against Sea-sonal Influenza in Adult High Risk Groups: South Asian Recommendations. J. Assoc. Physicians India 2016, 64, 3–11. [Google Scholar] [PubMed]
- Koul, P.A.; Swaminathan, S.; Rajgopal, T.; Ramsubramanian, V.; Joseph, B.; Shanbhag, S.; Mishra, A.; Raut, S.K. Adult immunization in occupational settings: A consensus on indian experts. Indian J. Occup. Environ. Med. 2020, 24, 3–15. [Google Scholar] [CrossRef]
- Koul, P.A. Clinical practice guidelines for influenza and pneumococcal vaccination: The Indian perspective. Lung India 2020, 37, S1–S3. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Family Welfare Directorate General of Health Services. Seasonal Influenza: Guidelines for Vaccination with Influenza Vaccine. Available online: https://main.mohfw.gov.in/sites/default/files/30580390001493710612.pdf (accessed on 22 July 2021).
- Koul, P.A.; Mir, H. The biggest barrier to influenza vaccination in pregnant females in India: Poor sensitization of the care providers. Vaccine 2018, 36, 3569–3570. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Interim adjusted of seasonal influenza vaccine effectiveness-United States, February 2014. Morb. Mortal. Wkly. Rep. 2014, 62, 119–123. [Google Scholar]
- Baselga-Moreno, V.; Trushakova, S.; McNeil, S.; Sominina, A.; Nunes, M.C.; Draganescu, A.; Unal, S.; Koul, P.; Kyncl, J.; Zhang, T.; et al. Influenza epidemiology and influenza vaccine effectiveness during the 2016–2017 season in the Global Influenza Hospital Surveillance Network (GIHSN). BMC Public Health 2019, 19, 487. [Google Scholar] [CrossRef] [PubMed]
- Puig-Barberà, J.; Mira-Iglesias, A.; Burtseva, E.; Cowling, B.J.; Serhat, U.; Ruiz-Palacios, G.M.; Launay, O.; Kyncl, J.; Koul, P.; Siqueira, M.M.; et al. Influenza epidemiology and influenza vaccine effectiveness during the 2015–2016 season: Results from the Global Influenza Hospital Surveillance Network. BMC Infect. Dis. 2019, 19, 415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koul, P.A.; Broor, S.; Saha, S.; Barnes, J.; Smith, C.; Shaw, M.; Chadha, M.; Lal, R.B. Differences in Influenza Seasonality by Latitude, Northern India. Emerg. Infect. Dis. 2014, 20, 1746–1749. [Google Scholar] [CrossRef] [Green Version]
- Gomez, G.B.; Mahé, C.; Chaves, S.S. Uncertain effects of the pandemic on respiratory viruses. Science 2021, 372, 1043–1044. [Google Scholar] [CrossRef]
- Puig-Barberà, J.; Tormos, A.; Trushakova, S.; Sominina, A.; Pisareva, M.; Ciblak, M.A.; Badur, S.; Yu, H.; Cowling, B.; Burtseva, E.; et al. The Global Influenza Hospital Surveillance Network (GIHSN): A new platform to describe the epidemiology of severe influenza. Influenza Other Respir. Viruses 2015, 9, 277–286. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Influenza Case Definitions. 2005–2017. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32018D0945&from=EN#page=24 (accessed on 2 November 2012).
- WHO. WHO Recommendations on the Composition of Influenza Virus Vaccines. Available online: https://www.who.int/influenza/vaccines/virus/recommendations/en/ (accessed on 3 June 2019).
- World Health Organization. CDC Protocol of Real-Time RTPCR for Influenza A (H1N1); World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Gaglani, M.; Pruszynki, J.; Murthy, K.; Clipper, L.; Robertson, A.; Reis, M.; Chung, J.R.; Piedra, P.A.; Avadhanula, V.; Nowalk, M.P.; et al. Influenza vaccine effectiveness against 2009 pandemic influenza A (H1N1) virus dif-fered by vaccine type during 2013–14 in the United States. J. Infect Dis. 2016, 213, 1546–1556. [Google Scholar] [CrossRef]
- Flannery, B.; Thaker, S.N.; Clippard, J.; Monto, A.S.; Ohmit, S.E.; Zimmerman, R.K.; Nowalk, M.P.; Gaglani, M.; Jackson, M.L.; Jackson, L.A.; et al. Interim estimates 2013–14 seasonal influenza vaccine effectiveness United States, February 2016. Morb. Mortal. Wkly. Rep. 2014, 63, 137–142. [Google Scholar]
- McLean, H.Q.; Thomson, M.G.; Sundaram, M.E.; Kieke, B.A.; Gaglani, M.; Murthy, K.; Piedra, P.A.; Zimmerman, R.K.; Nowalk, M.P.; Raviotta, J.M.; et al. Influenza vaccine effectiveness in the United States during 2012–13: Variable protection by age and virus type. J. Infect. Dis. 2015, 211, 1529–1540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rose, A.; Kissling, E.; Emborg, H.-D.; Larrauri, A.; McMenamin, J.; Pozo, F.; Trebbien, R.; Mazagatos, C.; Whitaker, H.; Valenciano, M.; et al. Interim 2019/20 influenza vaccine effectiveness: Six European studies, September 2019 to January 2020. Eurosurveillance 2020, 25, 2000153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skowronski, D.M.; Zou, M.; Sabaiduc, S.; Murti, M.; Olsha, R.; Dickinson, J.A.; Gubbay, J.B.; Croxen, M.; Charest, H.; Jassem, A.; et al. Interim estimates of 2019/20 vaccine effectiveness during early-season co-circulation of influenza A and B viruses, Canada, February 2020. Eurosurveillance 2020, 25, 2000103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dawood, F.S.; Chung, J.R.; Kim, S.S.; Zimmerman, R.K.; Nowalk, M.P.; Jackson, M.L.; Jackson, L.A.; Monto, A.S.; Martin, E.T.; Belongia, E.A.; et al. Interim Estimates of 2019–20 Seasonal Influenza Vaccine Effectiveness—United States, February 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 177–182. [Google Scholar] [CrossRef] [Green Version]
- Belongia, E.A.; Simpson, M.D.; King, J.; Sundaram, M.E.; Kelley, N.S.; Osterholm, M.T.; McLean, H.Q. Variable influenza vaccine effectiveness by subtype: A systematic review and meta-analysis of test-negative design studies. Lancet Infect. Dis. 2016, 16, 942–951. [Google Scholar] [CrossRef]
- Skowronski, D.M.; Chambers, C.; De Serres, G.; Sabaiduc, S.; Winter, A.-L.; Dickinson, J.A.; Gubbay, J.B.; Drews, S.J.; Fonseca, K.; Charest, H.; et al. Vaccine Effectiveness Against Lineage-matched and -mismatched Influenza B Viruses Across 8 Seasons in Canada, 2010–2011 to 2017–2018. Clin. Infect. Dis. 2018, 68, 1754–1757. [Google Scholar] [CrossRef] [Green Version]
- Skowronski, D.M.; Janjua, N.; De Serres, G.; Sabaiduc, S.; Eshaghi, A.; Dickinson, J.; Fonseca, K.; Winter, A.-L.; Gubbay, J.B.; Krajden, M.; et al. Low 2012–13 Influenza Vaccine Effectiveness Associated with Mutation in the Egg-Adapted H3N2 Vaccine Strain Not Antigenic Drift in Circulating Viruses. PLoS ONE 2014, 9, e92153. [Google Scholar] [CrossRef] [Green Version]
- Flannery, B.; Chung, J.R.; Monto, A.S.; Martin, E.T.; Belongia, E.; McLean, H.Q.; Gaglani, M.; Murthy, K.; Zimmerman, R.K.; Nowalk, M.P.; et al. Influenza Vaccine Effectiveness in the United States During the 2016–2017 Season. Clin. Infect. Dis. 2018, 68, 1798–1806. [Google Scholar] [CrossRef]
- Koul, P.A.; Potdar, V.; Showkat, M.; Mir, H.; Chadha, M.S. Influenza B in a temperate region of northern India 2010–2016: Co-circulation of the two lineages with northern hemispherical seasonality. Virus Dis. 2018, 29, 553–559. [Google Scholar] [CrossRef]
- Neher, R.; Bedford, T.; Daniels, R.S.; Russell, C.A.; Shraiman, B.I. Prediction, dynamics, and visualization of antigenic phenotypes of seasonal influenza viruses. Proc. Natl. Acad. Sci. USA 2016, 113, E1701–E1709. [Google Scholar] [CrossRef] [Green Version]
- Flannery, B.; Zimmerman, R.K.; Gubareva, L.V.; Garten, R.J.; Chung, J.R.; Nowalk, M.P.; Jackson, M.L.; Jackson, L.A.; Monto, A.S.; Ohmit, S.E.; et al. Enhanced Genetic Characterization of Influenza A(H3N2) Viruses and Vaccine Effectiveness by Genetic Group, 2014–2015. J. Infect. Dis. 2016, 214, 1010–1019. [Google Scholar] [CrossRef] [Green Version]
- Flannery, B.; Kondor, R.J.G.; Chung, J.R.; Gaglani, M.; Reis, M.; Zimmerman, R.K.; Nowalk, M.P.; Jackson, M.L.; Jackson, L.A.; Monto, A.S.; et al. Spread of Antigenically Drifted Influenza A(H3N2) Viruses and Vaccine Effectiveness in the United States During the 2018–2019 Season. J. Infect. Dis. 2019, 221, 8–15. [Google Scholar] [CrossRef]
- Skowronski, D.M.; Chambers, C.; Sabaiduc, S.; De Serres, G.; Winter, A.-L.; Dickinson, J.; Krajden, M.; Gubbay, J.B.; Drews, S.J.; Martineau, C.; et al. A Perfect Storm: Impact of Genomic Variation and Serial Vaccination on Low Influenza Vaccine Effectiveness During the 2014–2015 Season. Clin. Infect. Dis. 2016, 63, 21–32. [Google Scholar] [CrossRef]
- Morris, D.H.; Gostic, K.M.; Pompei, S.; Bedford, T.; Łuksza, M.; Neher, R.A.; Grenfell, B.T.; Lässig, M.; McCauley, J.W. Predictive Modeling of Influenza Shows the Promise of Applied Evolutionary Biology. Trends Microbiol. 2017, 26, 102–118. [Google Scholar] [CrossRef]
- Virk, R.K.; Jayakumar, J.; Mendenhall, I.H.; Moorthy, M.; Lam, P.; Linster, M.; Lim, J.; Lin, C.; Oon, L.L.E.; Lee, H.K.; et al. Divergent evolutionary trajectories of influenza B viruses underlie their contemporaneous epidemic activity. Proc. Natl. Acad. Sci. USA 2019, 117, 619–628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Recommended Composition of Influenza Virus Vaccines for Use in the 2020 Southern Hemisphere Influenza Season. Available online: https://www.who.int/influenza/vaccines/virus/recommendations/201909_recommendation.pdf (accessed on 22 July 2021).
- WHO. Recommended Composition of Influenza Virus Vaccines for Use in the 2020–2021 Northern Hemisphere Influenza Season. Available online: https://www.who.int/influenza/vaccines/virus/recommendations/202002_recommendation.pdf?ua=1. (accessed on 22 July 2021).
- US Food and Drug Administration. CDC Human Influenza Virus Real-time RT-PCR Diagnostic Panel: Influenza A/B Typing Kit, Influenza A Subtyping Kit (VER 2), Influenza B Lineage Genotyping Kit (VER 1.1 and VER 2), Influenza A/H5 Subtyping Kit (VER 3); Center for Disease Control and Prevention: Atlanta, GA, USA, 2019. Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf19/K190302.pdf (accessed on 23 September 2021).
- Lo, C.-Y.; Misplon, J.A.; Li, X.; Price, G.E.; Ye, Z.; Epstein, S.L. Universal influenza vaccine based on conserved antigens provides long-term durability of immune responses and durable broad protection against diverse challenge virus strains in mice. Vaccine 2021, 39, 4628–4640. [Google Scholar] [CrossRef]
- McLean, H.Q.; Belongia, E.A. Influenza Vaccine Effectiveness: New Insights and Challenges. Cold Spring Harb. Perspect. Med. 2020, 11, a038315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartley, J.M.; Cadar, A.N.; Martin, D.E. Better, Faster, Stronger: mRNA Vaccines Show Promise for Influenza Vaccination in Older Adults. Immunol. Investig. 2021, 50, 810–820. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Alvarez, J.J.S.; Ng, S.H.; Nielsen, R.; Zhai, W. Passage Adaptation Correlates with the Reduced Efficacy of the Influenza Vaccine. Clin. Infect. Dis. 2018, 69, 1198–1204. [Google Scholar] [CrossRef]
- Belongia, E.A.; Skowronski, D.M.; McLean, H.Q.; Chambers, C.; Sundaram, M.E.; De Serres, G. Repeated annual influenza vaccination and vaccine effectiveness: Review of evidence. Expert Rev. Vaccines 2017, 16, 723–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skowronski, D.M.; Chambers, C.; De Serres, G.; Sabaiduc, S.; Winter, A.-L.; Dickinson, J.; Gubbay, J.B.; Fonseca, K.; Drews, S.J.; Charest, H.; et al. Serial Vaccination and the Antigenic Distance Hypothesis: Effects on Influenza Vaccine Effectiveness During A(H3N2) Epidemics in Canada, 2010–2011 to 2014–2015. J. Infect. Dis. 2017, 215, 1059–1099. [Google Scholar] [CrossRef]
- Ramsay, L.C.; Buchan, S.A.; Stirling, R.G.; Cowling, B.J.; Feng, S.; Kwong, J.C.; Warshawsky, B.F. The impact of repeated vaccination on influenza vaccine effectiveness: A systematic review and meta-analysis. BMC Med. 2019, 17, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Moss, A.J.; Gaughran, F.; Karasu, A.; Gilbert, A.S.; Mann, A.J.; Gelder, C.M.; Oxford, J.S.; Stephens, H.A.; Lambkin-Williams, R. Correlation between Human Leukocyte Antigen Class II Alleles and HAI Titers Detected Post-Influenza Vaccination. PLoS ONE 2013, 8, e71376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, S.; Wei, H.; Liao, Q.; Li, M.; Zhong, S.; Cheng, Y.; Huang, W.; Wang, D.; Shu, Y. Identification of Two Novel Candidate Genetic Variants Associated with the Responsiveness to Influenza Vaccination. Front. Immunol. 2021, 12, 2472. [Google Scholar] [CrossRef] [PubMed]
- Foppa, I.M.; Ferdinands, J.M.; Chaves, S.S.; Haber, M.J.; Reynolds, S.B.; Flannery, B.; Fry, A.M. The case test-negative design for studies of the effectiveness of influenza vaccine in inpatient settings. Int. J. Epidemiol. 2016, 45, 2052–2059. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Symptoms | Vaccinated (n = 99) | Non-Vaccinated (n = 1120) |
|---|---|---|
| Fever | 57 (57.5) | 781 (69.7) |
| Malaise | 65 (65.6) | 617 (55) |
| Headache | 47 (47.5) | 543 (48.4) |
| Myalgias | 68 (68.6) | 825 (73.6) |
| Cough | 92 (92.9) | 1039 (92.7) |
| Sore throat | 54 (54.5) | 505 (45) |
| Breathlessness | 74 (74.7) | 789 (70.4) |
| Age Group (years) | Influenza Positives (N) | Influenza Positives Vaccinated (N) | Influenza Negatives Total (N) | Influenza Negatives Vaccinated (N) | Unadjusted VE (%) | 95% CI | Adjusted VE (%) | 95% CI | ||
|---|---|---|---|---|---|---|---|---|---|---|
| All ages | 336 | 23 | 883 | 76 | 22 | −27 to 52 | 0.315 | 14 *,† | −41 to 47 | 0.549 |
| 5–17 | 28 | 0 | 35 | 0 | - | - | - | - | ||
| 18–49 | 162 | 9 | 351 | 25 | 23 | −68 to 65 | 0.508 | 24 ‡ | −66 to 66 | 0.485 |
| 50–64 | 65 | 3 | 219 | 19 | 49 | −78 to 85 | 0.290 | 49 ‡ | −78 to 85 | 0.291 |
| >65 | 81 | 11 | 278 | 32 | −21 | −152 to 42 | 0.614 | −67 ‡ | −145 to 44 | 0.683 |
| Virus type | ||||||||||
| A/H1N1 | 155 | 6 | 883 | 76 | 57 | 0 to 82 | 0.050 | 55 * | −6 to 81 | 0.068 |
| B/Victoria | 163 | 14 | 883 | 76 | 0 | −81 to 45 | 0.994 | −12 * | −106 to 39 | 0.708 |
| Site | Influenza-Positive | Influenza-Negative | Adjusted VE, % (95% CI) | ||
|---|---|---|---|---|---|
| Total | Vaccinated | Total | Vaccinated | ||
| N | N (%) | N | N(%) | ||
| European Union [27] | |||||
| EU (PC) Influenza B | 12 | 4 (NC) | 313 | 199 (64) | 60 (−69 to 90) |
| Influenza B/Victoria | 209 | 5 (2) | 1190 | 141 (12) | −12 to 86 |
| EU (H) Influenza A | 122 | 50 (41) | 473 | 312 (66) | 62 (41 to 76) |
| United States [29] | |||||
| All influenza types | 1060 | 390 (37) | 3052 | 1682 (55) | 45 (36–53) |
| Influenza B/Victoria | 634 | 211 (33) | 2968 | 1641 (55) | 50 (39–59) |
| Influenza A(H1N1)pdm09 | 336 | 138 (42) | 3052 | 1682 (55) | 37 (19 to 52) |
| Canada [28] | |||||
| All influenza types | 1411 | 191 (14) | 1397 | 399 (29) | 58 (47 to 66) |
| Influenza A | 731 | 131 (18) | 1397 | 399 (29) | 49 (34 to 60) |
| Influenza B | 683 | 60 (9) | 1397 | 399 (29) | 69 (57 to 77) |
| Present study | |||||
| Any influenza (A + B) | 336 | 23 (7) | 883 | 76 (9) | 14 (−41 to 47) |
| Influenza B/Victoria | 163 | 14 (9) | 883 | 76 (9) | −12 (−106 to 39) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mir, H.; Haq, I.; Koul, P.A. Poor Vaccine Effectiveness against Influenza B-Related Severe Acute Respiratory Infection in a Temperate North Indian State (2019–2020): A Call for Further Data for Possible Vaccines with Closer Match. Vaccines 2021, 9, 1094. https://doi.org/10.3390/vaccines9101094
Mir H, Haq I, Koul PA. Poor Vaccine Effectiveness against Influenza B-Related Severe Acute Respiratory Infection in a Temperate North Indian State (2019–2020): A Call for Further Data for Possible Vaccines with Closer Match. Vaccines. 2021; 9(10):1094. https://doi.org/10.3390/vaccines9101094
Chicago/Turabian StyleMir, Hyder, Inaamul Haq, and Parvaiz A. Koul. 2021. "Poor Vaccine Effectiveness against Influenza B-Related Severe Acute Respiratory Infection in a Temperate North Indian State (2019–2020): A Call for Further Data for Possible Vaccines with Closer Match" Vaccines 9, no. 10: 1094. https://doi.org/10.3390/vaccines9101094
APA StyleMir, H., Haq, I., & Koul, P. A. (2021). Poor Vaccine Effectiveness against Influenza B-Related Severe Acute Respiratory Infection in a Temperate North Indian State (2019–2020): A Call for Further Data for Possible Vaccines with Closer Match. Vaccines, 9(10), 1094. https://doi.org/10.3390/vaccines9101094