Coverage of HPV Vaccination and Influencing Factors Among Female College Students in Northern China

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection and Questionnaire
2.3. Ethical Approval
2.4. HPV-Related Knowledge Level
2.5. Health Belief Model
2.6. Reliability and Validity Analysis
2.7. Statistical Methods
2.8. Quality Control
3. Results
3.1. General Participants‘ Information
3.2. Level of Knowledge Regarding HPV and Related Information
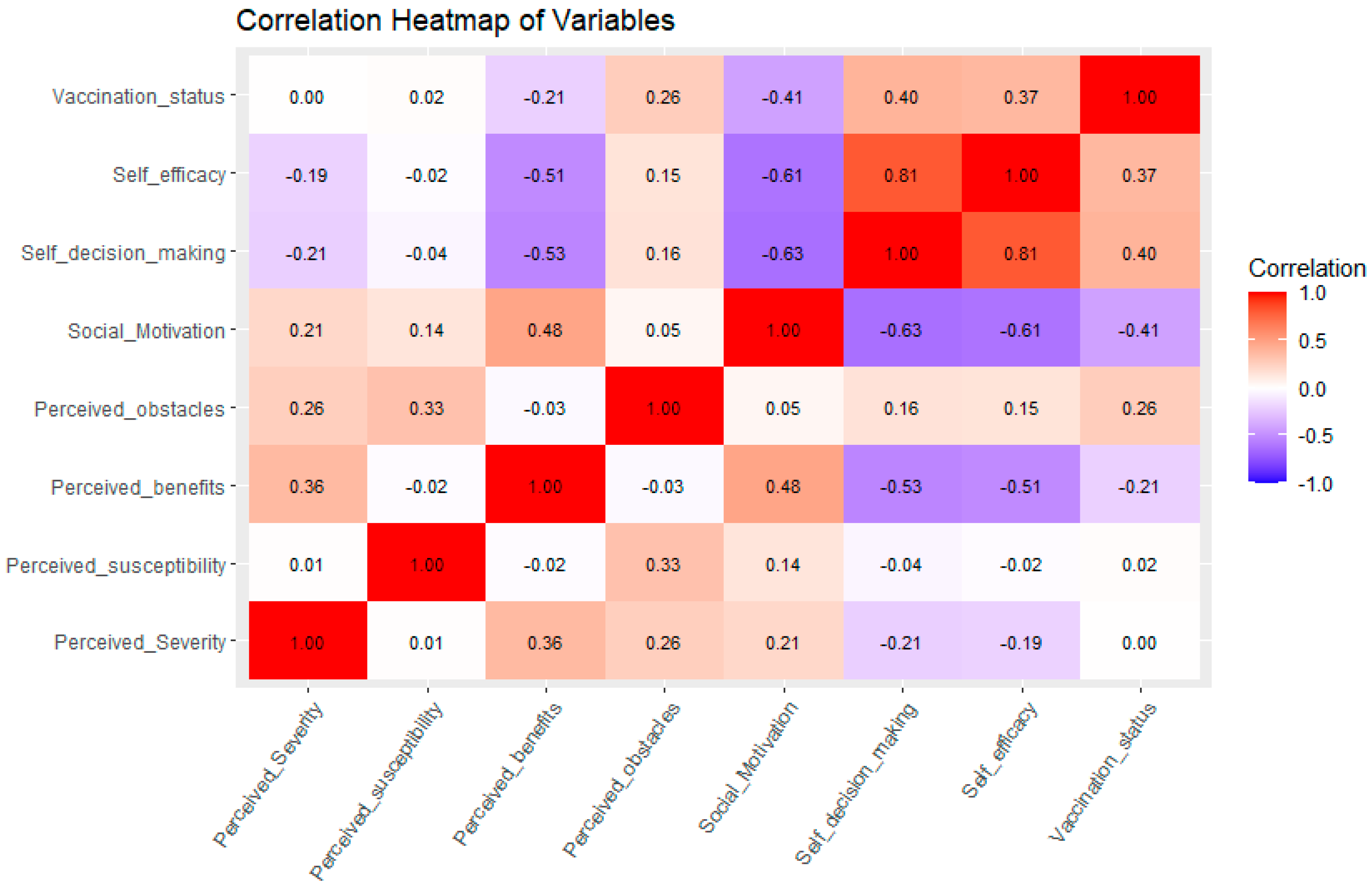
3.3. Analysis of Health Beliefs Associated with HPV Vaccination
3.4. Multivariate Analysis of Factors Influencing HPV Vaccination Status
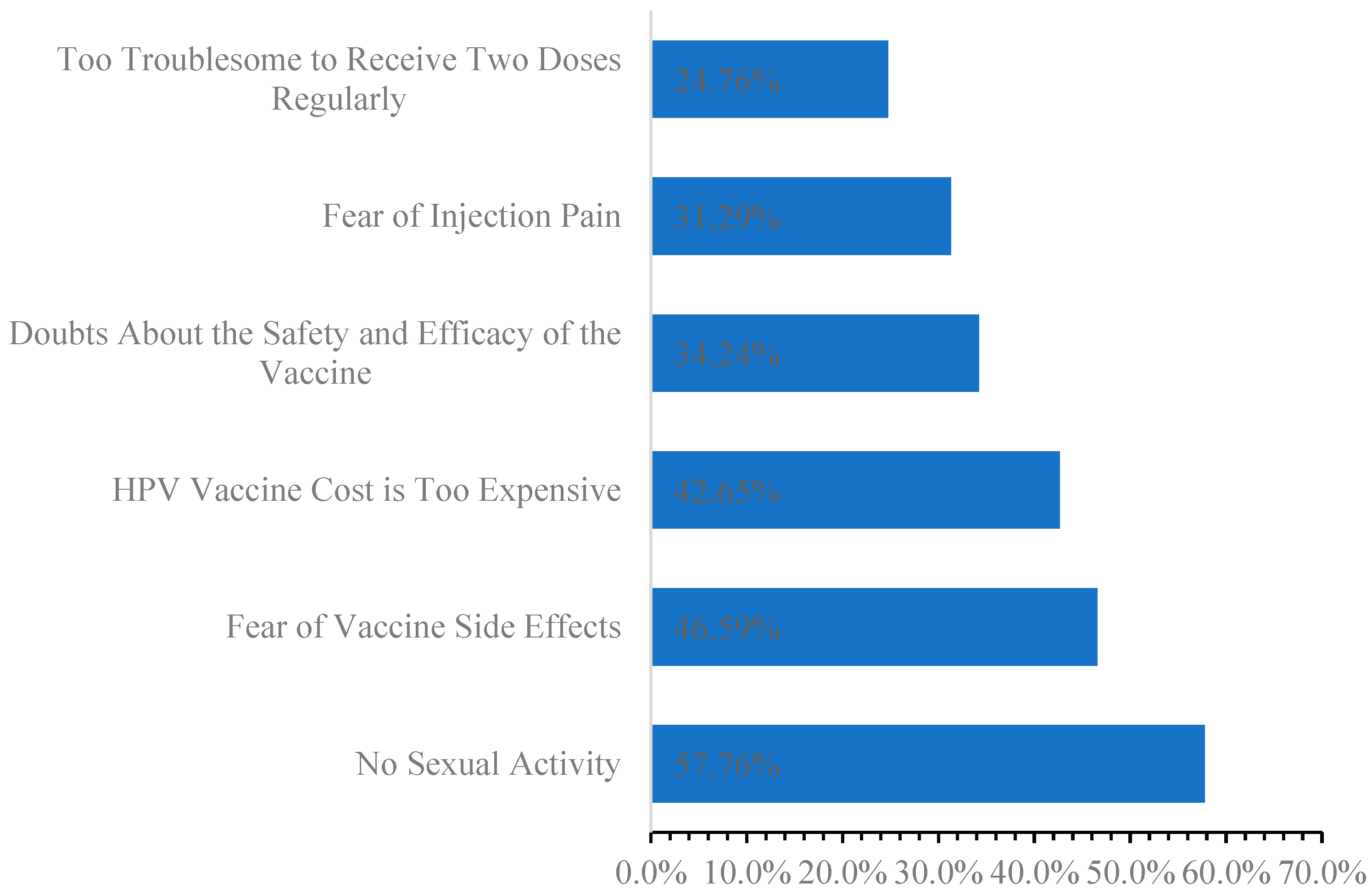
3.5. Reasons for Female College Students’ Unwillingness to Receive Vaccinations
4. Discussion
4.1. Key Findings and Implications
4.2. Study Limitations
4.3. Future Research Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wu, J.; Jin, Q.; Zhang, Y.; Ji, Y.; Li, J.; Liu, X.; Duan, H.; Feng, Z.; Liu, Y.; Zhang, Y.; et al. Global burden of cervical cancer: Current estimates, temporal trend and future projections based on the GLOBOCAN 2022. J. Natl. Cancer Cent. 2025. [Google Scholar] [CrossRef]
- Plotzker, R.E.; Vaidya, A.; Pokharel, U.; Stier, E.A. Sexually Transmitted Human Papillomavirus: Update in Epidemiology, Prevention, and Management. Infect. Dis. Clin. N. Am. 2023, 37, 289–310. [Google Scholar] [CrossRef]
- Zhang, L.; Zhao, Y.; Tu, Q.; Xue, X.; Zhu, X.; Zhao, K.-N. The Roles of Programmed Cell Death Ligand-1/ Programmed Cell Death-1 (PD-L1/PD-1) in HPV-induced Cervical Cancer and Potential for their Use in Blockade Therapy. Curr. Med. Chem. 2021, 28, 893–909. [Google Scholar] [CrossRef]
- Włoszek, E.; Krupa, K.; Skrok, E.; Budzik, M.P.; Deptała, A.; Badowska-Kozakiewicz, A. HPV and Cervical Cancer—Biology, Prevention, and Treatment Updates. Curr. Oncol. 2025, 32, 122. [Google Scholar] [CrossRef] [PubMed]
- Kjaer, S.K.; Nygård, M.; Sundström, K.; Dillner, J.; Tryggvadottir, L.; Munk, C.; Berger, S.; Enerly, E.; Hortlund, M.; Ágústsson, Á.I.; et al. Final analysis of a 14-year long-term follow-up study of the effectiveness and immunogenicity of the quadrivalent human papillomavirus vaccine in women from four nordic countries. EClinicalMedicine 2020, 23, 100401. [Google Scholar] [CrossRef]
- Simms, K.T.; Steinberg, J.; Caruana, M.; Smith, M.A.; Lew, J.B.; Soerjomataram, I.; Castle, P.E.; Bray, F.; Canfell, K. Impact of scaled up human papillomavirus vaccination and cervical screening and the potential for global elimination of cervical cancer in 181 countries, 2020–2099: A modelling study. Lancet Oncol. 2019, 20, 394–407. [Google Scholar] [CrossRef] [PubMed]
- Alsulami, F.T.; Sanchez, J.; Rabionet, S.E.; Popovici, I.; Baraka, M.A. Predictor of HPV Vaccination Uptake among Foreign-Born College Students in the U.S.: An Exploration of the Role of Acculturation and the Health Belief Model. Vaccines 2023, 11, 422. [Google Scholar] [CrossRef]
- Liu, Y.; Di, N.; Tao, X. Knowledge, practice and attitude towards HPV vaccination among college students in Beijing, China. Hum. Vaccin. Immunother. 2020, 16, 116–123. [Google Scholar] [CrossRef]
- Song, D.; Liu, P.; Wu, D.; Zhao, F.; Wang, Y.; Zhang, Y. Knowledge and Attitudes towards Human Papillomavirus Vaccination (HPV) among Healthcare Providers Involved in the Governmental Free HPV Vaccination Program in Shenzhen, Southern China. Vaccines 2023, 11, 997. [Google Scholar] [CrossRef]
- Zhao, X.L.; Hu, S.Y.; Hu, J.W.; Wang, H.H.; Wen, T.M.; Feng, Y.S.; Qiao, Y.L.; Zhao, F.H.; Zhang, Y. Tackling barriers to scale up human papillomavirus vaccination in China: Progress and the way forward. Infect. Dis. Poverty 2023, 12, 86. [Google Scholar] [CrossRef]
- Wang, S.; Wu, H.; Zhang, H.; Niu, X.; Pan, L.; Wang, X.; Qin, W.; Hu, F.; Li, L.; Yang, H.; et al. Gender differences in sexual health knowledge, attitude and behavior among Chinese college students and the influencing factors of sexual behavior. Chin. J. Dis. Control Prev. 2024, 28, 417–423. [Google Scholar]
- Azim, K.A.; Happel-Parkins, A.; Moses, A.; Haardoerfer, R. Exploring Relationships Between Genito-Pelvic Pain/Penetration Disorder, Sex Guilt, and Religiosity Among College Women in the U.S. J. Sex. Med. 2021, 18, 770–782. [Google Scholar] [CrossRef]
- Hansen, B.T.; Kjær, S.K.; Arnheim-Dahlström, L.; Liaw, K.L.; Juul, K.E.; Thomsen, L.T.; Frederiksen, K.; Elfström, K.M.; Munk, C.; Nygård, M. Age at first intercourse, number of partners and sexually transmitted infection prevalence among Danish, Norwegian and Swedish women: Estimates and trends from nationally representative cross-sectional surveys of more than 100,000 women. Acta Obs. Gynecol. Scand. 2020, 99, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.; Xu, X.; Zhang, Y.; Liu, Y.; Yang, C.; Wang, Y.; Wang, Y.; Yu, Y.; Hong, Y.; Zhang, X.; et al. A nationwide post-marketing survey of knowledge, attitude and practice toward human papillomavirus vaccine in general population: Implications for vaccine roll-out in mainland China. Vaccine 2021, 39, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Liu, C.R.; Wang, Z.Z.; Ren, Z.F.; Feng, X.X.; Ma, W.; Gao, X.H.; Zhang, R.; Brown, M.D.; Qiao, Y.L.; et al. Effect of a school-based educational intervention on HPV and HPV vaccine knowledge and willingness to be vaccinated among Chinese adolescents: A multi-center intervention follow-up study. Vaccine 2020, 38, 3665–3670. [Google Scholar] [CrossRef]
- Glanz, K.; Rimer, B.K.; Lewis, F.M. Health Behavior and Health Education: Theory, Research, and Practice; Jossey-Bass: Hoboken, NJ, USA, 1997. [Google Scholar]
- Rosenstock, I.M. Historical Origins of the Health Belief Model. Health Educ. Monogr. 1974, 2, 328–335. [Google Scholar] [CrossRef]
- Finfgeld, D.L.; Wongvatunyu, S.; Conn, V.S.; Grando, V.T.; Russell, C.L. Health Belief Model and Reversal Theory: A comparative analysis. J. Adv. Nurs. 2010, 43, 288–297. [Google Scholar] [CrossRef]
- Krebs, P.; Prochaska, J.O.; Rossi, J.S. A meta-analysis of computer-tailored interventions for health behavior change. Prev. Med. 2010, 51, 214–221. [Google Scholar] [CrossRef]
- Jinan Municipal Government. Jinan, a City of Springs Overview[EB/OL]. (25 February 2025). Available online: http://english.jinan.gov.cn/col/col108341/index.html (accessed on 28 February 2025).
- China Daily. Jinan Honored as ‘2023 Annual Dynamic City’ [EB/OL]. (28 December 2023). Available online: http://shandong.chinadaily.com.cn/2023-12/28/c_951937.htm (accessed on 28 February 2025).
- Dang, J.H.; Stewart, S.L.; Blumberg, D.A.; Rodriguez, H.P.; Chen, M.S. Patient and clinician factors associated with uptake of the human papillomavirus (HPV) vaccine among adolescent patients of a primary care network. Vaccine 2021, 39, 3528–3535. [Google Scholar] [CrossRef]
- Dai, Z.; Si, M.; Su, X.; Wang, W.; Zhang, X.; Gu, X.; Ma, L.; Li, J.; Zhang, S.; Ren, Z.; et al. Willingness to human papillomavirus (HPV) vaccination and influencing factors among male and female university students in China. J. Med. Virol. 2022, 94, 2776–2786. [Google Scholar] [CrossRef]
- Hui, C. Evaluation of a Web-Based Health Education Based on IMB Model in Improving Female College Students’ Knowledge on HPV Vaccines and Their Willingness to be Vaccinated; Sichuan University: Chengdu, China, 2021. [Google Scholar]
- Si, M. An IMB Model-Based Study on Influencing Factors and Intervention on HPV Vaccination Among College Girls; Peking Union Medical College: Beijing, China, 2021. [Google Scholar]
- Bai, Y.; Ip, P.; Chan, K.; Ngan, H.; Yip, P. HPV Vaccination Intentions of Female Students in Chinese Universities: A Systematic Literature Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 10207. [Google Scholar] [CrossRef] [PubMed]
- Charalambous, I.; Ioannou, G.; Nikolaou, S.; Theologou, R.; Yiallourou, A.; Papatheodorou, S.; Pantavou, K.G.; Nikolopoulos, G.K. State of knowledge of human papillomavirus (HPV), HPV vaccine and testing: A cross-sectional study among female university students in Cyprus. Women Health 2020, 60, 26–42. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, P.S.D.; Gonçalves, C.V.; Watte, G.; Costa, J.S.D.D. Vaccination coverage against human papillomavirus (HPV) and associated factors in female academics from a university in southwestern Goiás, Brazil. Rev. Saude Publica 2021, 55, 65. [Google Scholar] [CrossRef]
- Cheema, S.; Abraham, A.; Maisonneuve, P.; Jithesh, A.; Chaabna, K.; Al Janahi, R.; Sarker, S.; Hussain, A.; Rao, S.; Lowenfels, A.B.; et al. HPV infection and vaccination: A cross-sectional study of knowledge, perception, and attitude to vaccine uptake among university students in Qatar. BMC Public Health 2024, 24, 2316. [Google Scholar] [CrossRef]
- Sallam, M.; Al-Mahzoum, K.; Eid, H.; Assaf, A.M.; Abdaljaleel, M.; Al-Abbadi, M.; Mahafzah, A. Attitude towards HPV Vaccination and the Intention to Get Vaccinated among Female University Students in Health Schools in Jordan. Vaccines 2021, 9, 1432. [Google Scholar] [CrossRef]
- Zhao, R.; Zhang, L. Sexual and reproductive health related knowledge, attitude and behavior among senior high school and college students in 11 provinces and municipalities of China. Chin. J. Public Health 2019, 35, 1330–1338. [Google Scholar]
- Ardekani, A.; Taherifard, E.; Mollalo, A.; Hemadi, E.; Roshanshad, A.; Fereidooni, R.; Rouholamin, S.; Rezaeinejad, M.; Farid-Mojtahedi, M.; Razavi, M.; et al. Human Papillomavirus Infection during Pregnancy and Childhood: A Comprehensive Review. Microorganisms 2022, 10, 1932. [Google Scholar] [CrossRef]
- Drolet, M.; Laprise, J.-F.; Martin, D.; Jit, M.; Bénard, É.; Gingras, G.; Boily, M.-C.; Alary, M.; Baussano, I.; Hutubessy, R.; et al. Optimal human papillomavirus vaccination strategies to prevent cervical cancer in low-income and middle-income countries in the context of limited resources: A mathematical modelling analysis. Lancet Infect. Dis. 2021, 21, 1598–1610. [Google Scholar] [CrossRef]
- Gostin, L.; Hodge, J.G.; Bloom, B.R.; El-Mohandes, A.; Fielding, J.; Hotez, P.; Kurth, A.; Larson, H.J.; A Orenstein, W.; Rabin, K.; et al. The public health crisis of underimmunisation: A global plan of action. Lancet Infect. Dis. 2020, 20, e11–e16. [Google Scholar] [CrossRef]
- NSW Health. Human Papillomavirus (HPV) Vaccine-Parent Information [EB/OL]. (13 March 2024) [3/5]. Available online: https://www.health.nsw.gov.au/immunisation/Pages/parent-info-hpv.aspx (accessed on 28 February 2025).
- Kim, S.J.; Schiffelbein, J.E.; Imset, I.; Olson, A.L. Countering Antivax Misinformation via Social Media: Message-Testing Randomized Experiment for Human Papillomavirus Vaccination Uptake. J. Med. Internet Res. 2022, 24, e37559. [Google Scholar] [CrossRef]
- Bracko, M.; Simon, U.K. Virus-related Knowledge in Covid-19 Times—Results from two Cross-sectional Studies in Austria and Implications for School. Int. J. Biol. Sci. 2022, 18, 1627–1650. [Google Scholar] [CrossRef] [PubMed]
- Gong, X.; Xu, J.; He, Y.; Zou, G.; Liu, J. Socioeconomic inequalities in human papillomavirus knowledge and vaccine uptake: Evidence from a cross-sectional study in China. Front. Public. Health 2024, 12, 1399192. [Google Scholar] [CrossRef] [PubMed]
- Getachew, T.; Negash, A.; Degefa, M.; Lami, M.; Balis, B.; Debela, A.; Gemechu, K.; Shiferaw, K.; Nigussie, K.; Bekele, H.; et al. COVID-19 vaccine acceptance and associated factors among adult clients at public hospitals in eastern Ethiopia using the health belief model: Multicentre cross-sectional study. BMJ Open 2023, 13, e70551. [Google Scholar] [CrossRef]
- Han, Y.; Yin, J.; Zeng, Y.; Chu, C.-I.; Chiang, Y.-C.; Fang, Y. Determinants of Parental Intentions to Vaccinate Kindergarten Children Against Seasonal Influenza in Xiamen, China. J. Prim. Prev. 2019, 40, 325–342. [Google Scholar] [CrossRef]
- Zomordi, G.; Moradi, M.; Hasanzadeh, M.; Ghavami, V. The effect of education based on the theory of planned behavior on the intention of vaccination against human papillomavirus in female students: A controlled educational trial. J. Educ. Health Promot. 2022, 11, 237. [Google Scholar] [CrossRef] [PubMed]
- Shmueli, L. Predicting intention to receive COVID-19 vaccine among the general population using the health belief model and the theory of planned behavior model. BMC Public Health 2021, 21, 804. [Google Scholar] [CrossRef]
- Ma, A.; Savani, K.; Liu, F.; Tai, K.; Kay, A.C. The mutual constitution of culture and psyche: The bidirectional relationship between individuals’ perceived control and cultural tightness-looseness. J. Pers. Soc. Psychol. 2023, 124, 901–916. [Google Scholar] [CrossRef]
- Zhou, W.; Hou, J.; Sun, M.; Wang, C. The Impact of Family Socioeconomic Status on Elderly Health in China: Based on the Frailty Index. Int. J. Environ. Res. Public Health 2022, 19, 968. [Google Scholar] [CrossRef]
- Glassman, L.W.; Szymczak, J.E. The influence of social class and institutional relationships on the experiences of vaccine-hesitant mothers: A qualitative study. BMC Public Health 2022, 22, 2309. [Google Scholar] [CrossRef]
- Umman, V.; Girgin, T.; Baki, B.E.; Bozbiyik, O.; Akbulut, S.; Yoldas, T. Impact of pandemic and socioeconomic influences on decision-making for emergency ostomy procedures: Key factors affecting hospital visit decisions. Medicine 2024, 103, e38706. [Google Scholar] [CrossRef]
- Hatfield, E. Information Overload and the COVID-19 Vaccine. In Pandemic Resilience: Vaccination Resistance and Hesitance, Lessons from COVID-19; Berube, D.M., Ed.; Springer Nature: Cham, Switzerland, 2024; pp. 321–329. [Google Scholar]
- Singh, L.; Bao, L.; Bode, L.; Budak, C.; Pasek, J.; Raghunathan, T.; Traugott, M.; Wang, Y.; Wycoff, N. Understanding the rationales and information environments for early, late, and nonadopters of the COVID-19 vaccine. Npj Vaccines 2024, 9, 168. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Wang, L.; Huang, Y.; Zhang, L. Risk perception and trust in the relationship between knowledge and HPV vaccine hesitancy among female university students in China: A cross-sectional study. BMC Public Health 2024, 24, 667. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Dimensions | Serial Numbering | Items |
|---|---|---|
| Perceived Severity | M1 | I feel anxious when thinking about HPV infection. |
| M2 | HPV infection is perceived as a serious condition that may affect my academic life. | |
| M3 | A cervical cancer diagnosis would be devastating to me. | |
| M4 | Cervical cancer would have a significant impact on my life. | |
| Perceived Susceptibility | M5 | I believe I am at risk of HPV infection. |
| M6 | I believe I am at risk of developing cervical cancer. | |
| Perceived Benefits | M7 | HPV vaccination should be recommended even after sexual initiation. |
| M8 | HPV vaccination helps protect against HPV infection. | |
| M9 | HPV vaccination can reduce the risk of cervical cancer. | |
| Perceived Barriers | M10 | I am skeptical about the safety and efficacy of the HPV vaccine. |
| M11 | I find it challenging to decide whether to receive the HPV vaccine. | |
| M12 | I am concerned about the pain associated with the HPV vaccine injection. | |
| M13 | The cost of HPV vaccination is perceived as high. | |
| M14 | I am concerned about potential side effects of the HPV vaccine. | |
| Perceived Motivation | M15 | Other individuals my age are considering HPV vaccination. |
| M16 | My family believes I should receive the HPV vaccine. | |
| M17 | My friends believe I should receive the HPV vaccine. | |
| Self-decision-making | B1 | Even if the vaccination is expensive, I am confident that I can complete the HPV vaccination. |
| B2 | Even if the injection is painful, I am confident that I can complete the HPV vaccination. | |
| B3 | Even though I am slightly concerned about potential side effects, I am confident that I can complete the HPV vaccination. | |
| B4 | Even if it means having to receive three doses regularly, I am confident that I can complete the HPV vaccination. | |
| Self-efficacy | B5 | I can comfortably discuss the topic of HPV vaccination with my parents/guardians/nurses/doctors. |
| B6 | I know the vaccination sites or would search online or call to confirm the location | |
| B7 | I am aware that the HPV vaccine is a self-funded vaccine, and the cost is affordable. | |
| B8 | If I need to get vaccinated, I would set reminders on my calendar to ensure I complete all three doses on schedule. |
| Variables | ||
|---|---|---|
| Ethnicity | X1 | Han = 1; Others = 0 |
| Domicile | X2 | Urban = 1; Village = 0 |
| Religion | X3 | Yes = 1; No = 0 |
| Age | X4 | ≤20 = 0; >21 = 1 |
| Monthly disposable fund (RMB) | X5 | <1500 = 0; 1501~ = 1; 2001~ = 2; > 2501 = 3 |
| Whether one of your parents is a healthcare worker | X6 | Yes = 1; No = 0 |
| Paternal educational level | X7 | Junior high school and below = 0; High school/vocational and technical schools = 1; University/ junior college = 2; Graduate students and above = 3 |
| Whether there is a family or friend history of cervical cancer | X8 | Yes = 1; I don’t know/No = 0 |
| Acceptance of premarital sex | X9 | Yes = 1; No = 0 |
| Whether you have ever engaged in sexual activity | X10 | Yes = 1; No = 0 |
| Whether you have received sex education | X11 | Yes = 1; No = 0 |
| Whether you have ever heard of HPV | X12 | Yes = 1; No = 0 |
| Whether you have ever actively searched for or consulted about the HPV vaccine | X13 | Yes = 1; No = 0 |
| Whether the knowledge of HPV is adequate | X14 | ≥7 = 1; <7 = 0 |
| Perceived severity | X15 | Continuous variables |
| Perceived susceptibility | X16 | Continuous variables |
| Perceived benefits | X17 | Continuous variables |
| Perceived barriers | X18 | Continuous variables |
| Social motivation | X19 | Continuous variables |
| Self-decision-making | X20 | Continuous variables |
| Self-efficacy | X21 | Continuous variables |
| Variables | Total (N = 4076, %) | VG (N = 738, %) | WTG (N = 1638, %) | UTG (N = 1700, %) | χ2 | p Values |
|---|---|---|---|---|---|---|
| Total (n, %) | ||||||
| Ethnicity | 0.745 | 0.689 | ||||
| Han | 3945 (96.78) | 717 (97.15) | 1581 (96.52) | 1647 (96.88) | ||
| Others | 131 (3.21) | 21 (2.85) | 57 (3.48) | 55 (3.21) | ||
| Domicile | 188.449 | <0.001 | ||||
| Urban | 1431 (35.11) | 417 (56.50) | 535 (32.66) | 479 (28.18) | ||
| Village | 2645 (64.89) | 321 (43.50) | 1103 (67.34) | 1221 (71.65) | ||
| Religion | 2.336 | 0.311 | ||||
| Yes | 46 (1.15) | 8 (1.08) | 14 (0.85) | 24 (1.41) | ||
| No | 4030 (98.87) | 730 (98.92) | 1624 (99.15) | 1686 (98.59) | ||
| Age | 95.534 | <0.001 | ||||
| ≤20 | 3591 (88.10) | 574 (77.78) | 1499 (91.51) | 1518 (89.29) | ||
| >21 | 485 (11.90) | 164 (22.22) | 139 (8.49) | 182 (10.71) | ||
| Monthly disposable fund (RMB) | 151.303 | <0.001 | ||||
| ≤1500 | 1971 (48.36) | 232 (31.44) | 787 (48.05) | 952 (56.00) | ||
| 1501–2000 | 1482 (36.36) | 317 (42.95) | 627 (38.28) | 538 (31.65) | ||
| 2001–2500 | 402 (9.86) | 116 (15.72) | 143 (8.73) | 143 (8.41) | ||
| >2500 | 221 (5.42) | 73 (9.89) | 81 (4.95) | 67 (3.94) | ||
| Whether one of your parents is a healthcare worker | 39.733 | <0.001 | ||||
| Yes | 124 (3.04) | 48 (6.50) | 39 (2.38) | 37 (2.18) | ||
| No | 3952 (96.96) | 690 (93.50) | 1599 (97.62) | 1663 (97.82) | ||
| Paternal educational level | 200.057 | <0.001 | ||||
| Junior high school and below | 1467 (35.99) | 156 (21.14) | 611 (37.30) | 700 (41.18) | ||
| High school (including vocational and technical schools) | 1483 (36.38) | 234 (31.71) | 604 (36.87) | 645 (37.94) | ||
| University (including junior college and undergraduate) | 1053 (25.83) | 323 (43.77) | 390 (23.81) | 340 (20.00) | ||
| Graduate students and above | 73 (1.79) | 25 (3.39) | 33 (2.01) | 15 (0.88) | ||
| Acceptance of premarital sex | 73.003 | <0.001 | ||||
| Yes | 1681 (41.24) | 392 (53.12) | 697 (42.55) | 592 (34.82) | ||
| No | 2395 (58.76) | 346 (46.88) | 941 (57.45) | 1108 (65.18) | ||
| Whether you have ever engaged in sexual activity | 55.079 | <0.001 | ||||
| Yes | 290 (7.11) | 99 (13.41) | 101 (6.17) | 90 (5.29) | ||
| No | 3786 (92.89) | 639 (86.59) | 1537 (93.83) | 1610 (94.71) | ||
| Whether there is a family or friend history of cervical cancer | 66.918 | <0.001 | ||||
| Yes | 71 (1.74) | 23 (3.12) | 27 (1.65) | 21 (1.24) | ||
| No | 3292 (80.77) | 621 (84.15) | 1380 (84.25) | 1291 (75.94) | ||
| I don’t know | 713 (17.49) | 94 (12.74) | 231 (14.10) | 388 (22.82) | ||
| Whether you have received sex education | 30.755 | <0.001 | ||||
| Yes | 3567 (87.51) | 676 (91.60) | 1458 (89.01) | 1433 (84.29) | ||
| No | 509 (12.49) | 62 (8.40) | 180 (10.99) | 267 (15.71) | ||
| Whether you have ever heard of HPV | 69.060 | <0.001 | ||||
| Yes | 3864 (94.80) | 712 (96.48) | 1598 (97.56) | 1544 (91.41) | ||
| No | 212 (5.20) | 26 (3.52) | 40 (2.44) | 146 (8.59) | ||
| Whether you have ever actively searched for or consulted about the HPV vaccine | 325.771 | <0.001 | ||||
| Yes | 2563 (62.88) | 619 (83.88) | 1128 (68.86) | 816 (48.00) | ||
| No | 1513 (37.12) | 119 (16.12) | 510 (31.14) | 884 (52.00) |
| Variables | Total (N = 4076) | VG (N = 738) | WTG (N = 1638) | UTG (N = 1700) | F | p Values |
|---|---|---|---|---|---|---|
| Knowledge | 5.659 ± 2.975 | 6.664 ± 2.670 | 6.135 ± 2.704 | 4.762 ± 3.104 | 150.413 | <0.001 |
| Knowledge of HPV | 4.915 ± 2.459 | 5.745 ± 2.167 | 5.316 ± 2.201 | 4.169 ± 2.606 | 152.566 | <0.001 |
| Knowledge of cervical cancer | 0.743 ± 0.846 | 0.918 ± 0.886 | 0.819 ± 0.856 | 0.594 ± 0.793 | 50.025 | <0.001 |
| Motivation | ||||||
| Perceived severity | 2.121 ± 0.851 | 2.140 ± 0.906 | 2.109 ± 0.851 | 2.123 ± 0.825 | 0.358 | 0.699 |
| Perceived susceptibility | 3.826 ± 1.069 | 3.919 ± 1.056 | 3.773 ± 1.074 | 3.836 ± 1.069 | 4.856 | 0.008 |
| Perceived benefits | 1.910 ± 0.746 | 1.736 ± 0.754 | 1.785 ± 0.676 | 2.105 ± 0.761 | 106.317 | 0.000 |
| Perceived obstacles | 2.952 ± 0.773 | 3.33 ± 0.805 | 2.986 ± 0.771 | 2.756 ± 0.691 | 155.840 | <0.001 |
| Social motivation | 2.392 ± 0.735 | 1.925 ± 0.686 | 2.257 ± 0.672 | 2.724 ± 0.657 | 2.392 ± 0.735 | <0.001 |
| Behavioral skills | ||||||
| Self-decision-making | 3.801 ± 0.789 | 4.275 ± 0.733 | 3.95 ± 0.696 | 3.452 ± 0.742 | 391.962 | <0.001 |
| Self-efficacy | 3.768 ± 0.754 | 4.24 ± 0.727 | 3.857 ± 0.691 | 3.477 ± 0.696 | 328.42 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, L.; Xing, C.; Yu, X.; Xu, Y.; Wang, W.; Chang, C.; Lu, Q. Coverage of HPV Vaccination and Influencing Factors Among Female College Students in Northern China. Vaccines 2025, 13, 598. https://doi.org/10.3390/vaccines13060598
Yang L, Xing C, Yu X, Xu Y, Wang W, Chang C, Lu Q. Coverage of HPV Vaccination and Influencing Factors Among Female College Students in Northern China. Vaccines. 2025; 13(6):598. https://doi.org/10.3390/vaccines13060598
Chicago/Turabian StyleYang, Li, Chen Xing, Xue Yu, Yanrui Xu, Weibing Wang, Caiyun Chang, and Qingbin Lu. 2025. "Coverage of HPV Vaccination and Influencing Factors Among Female College Students in Northern China" Vaccines 13, no. 6: 598. https://doi.org/10.3390/vaccines13060598
APA StyleYang, L., Xing, C., Yu, X., Xu, Y., Wang, W., Chang, C., & Lu, Q. (2025). Coverage of HPV Vaccination and Influencing Factors Among Female College Students in Northern China. Vaccines, 13(6), 598. https://doi.org/10.3390/vaccines13060598