
Selection of Resin-Based Dental Restorative Materials: A Pilot Study on Professional Characteristics, Knowledge, and Selection Criteria



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Questionnaire Design
2.3. Bias Control Strategies
2.4. Data Collection and Processing
3. Results
3.1. Demographics
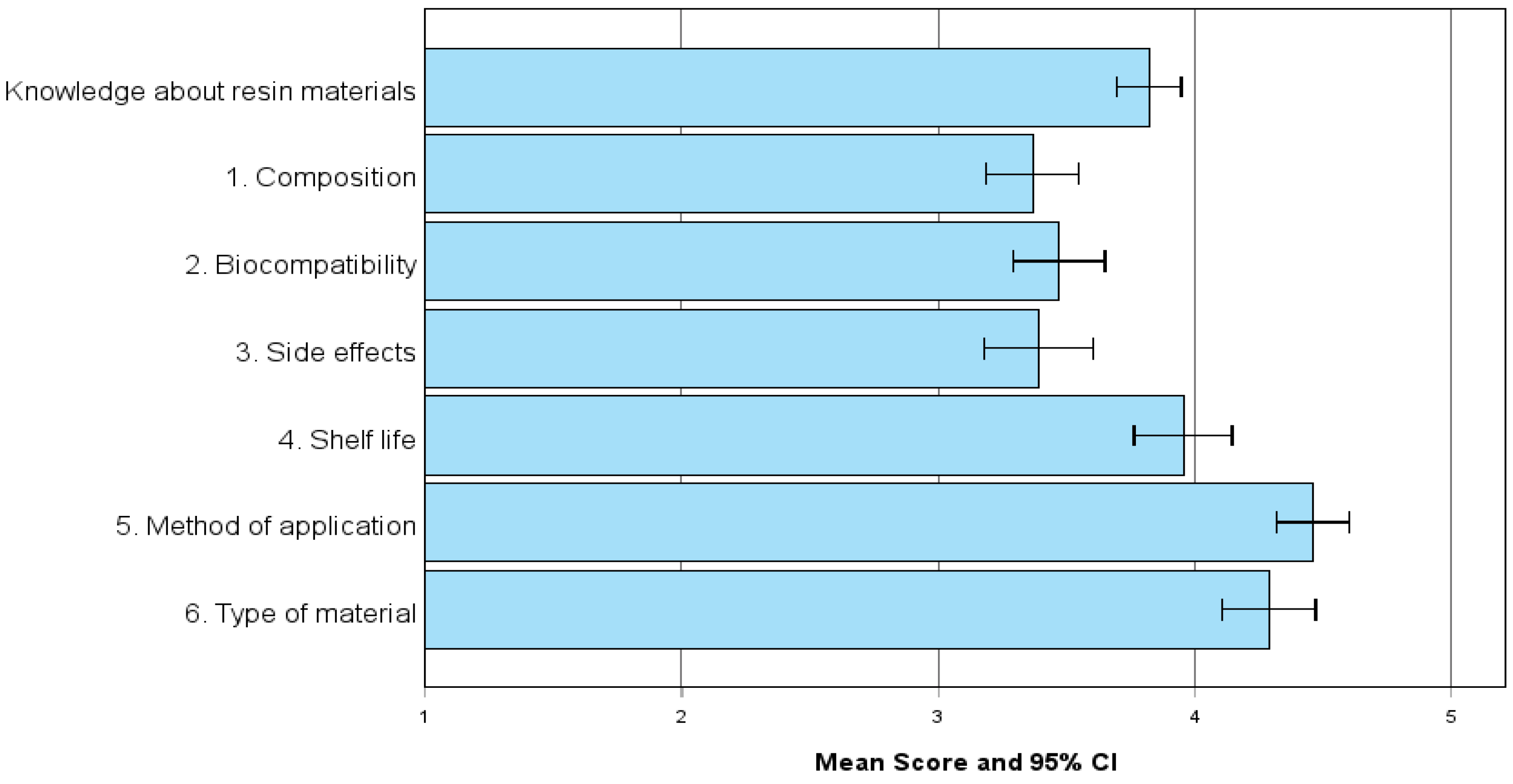
3.2. Knowledge About Resin Materials
3.2.1. Knowledge Levels in Resin Materials and Correlation with Professional Characteristics
3.2.2. Dentists’ Familiarity and Priorities in Resin Material Selection: Specifications, Features, and Sustainability
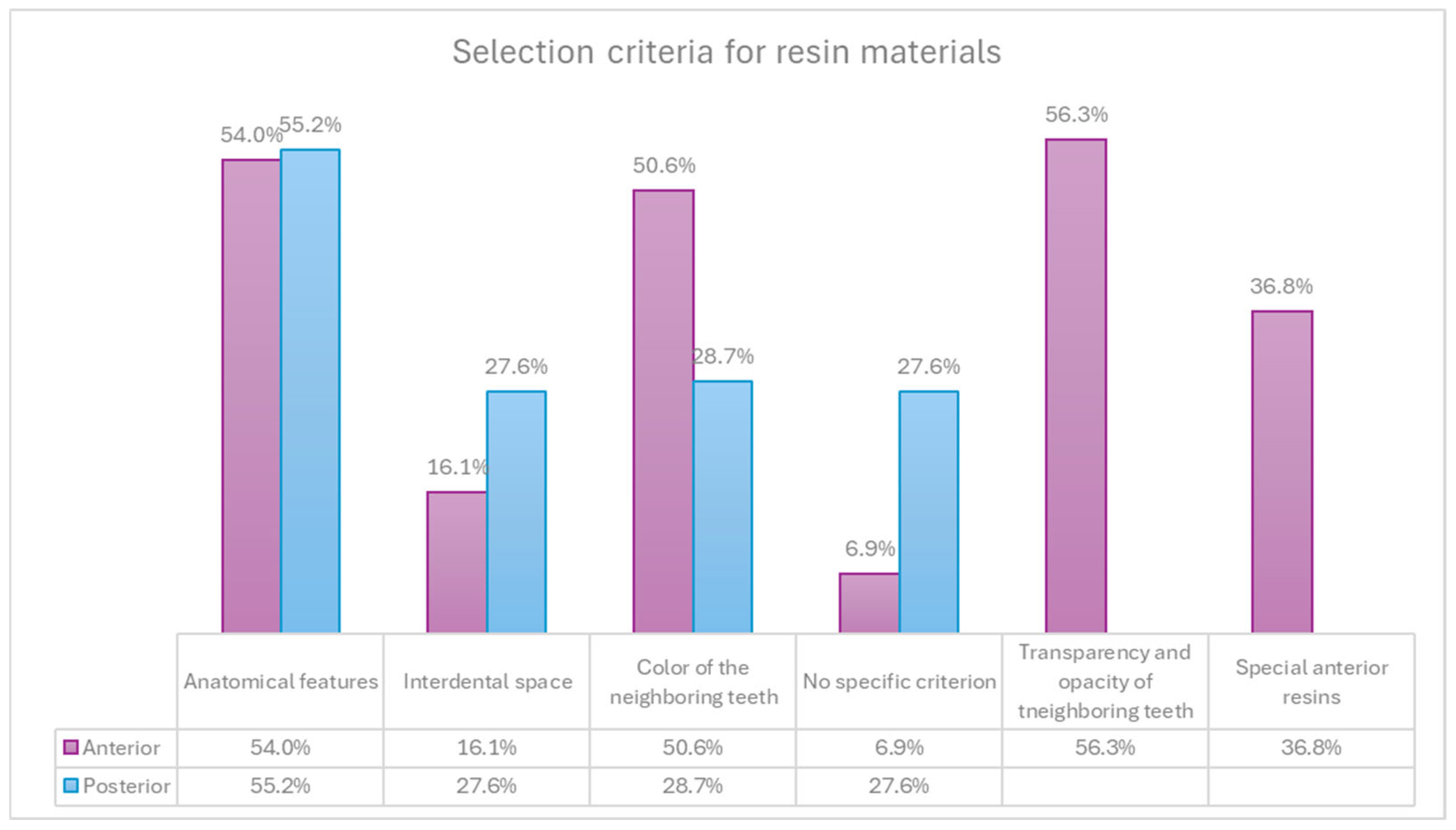
3.3. Selection of Resin Materials
Resin Selection in Anterior and Posterior Restorations
3.4. Professional Characteristics and Resin Material Selection
4. Discussion
4.1. Influence of Professional Characteristics on Material Selection
4.2. Tooth Regional Differences in Resin Material Criteria
4.3. Procurement Responsibility and Specification Awareness
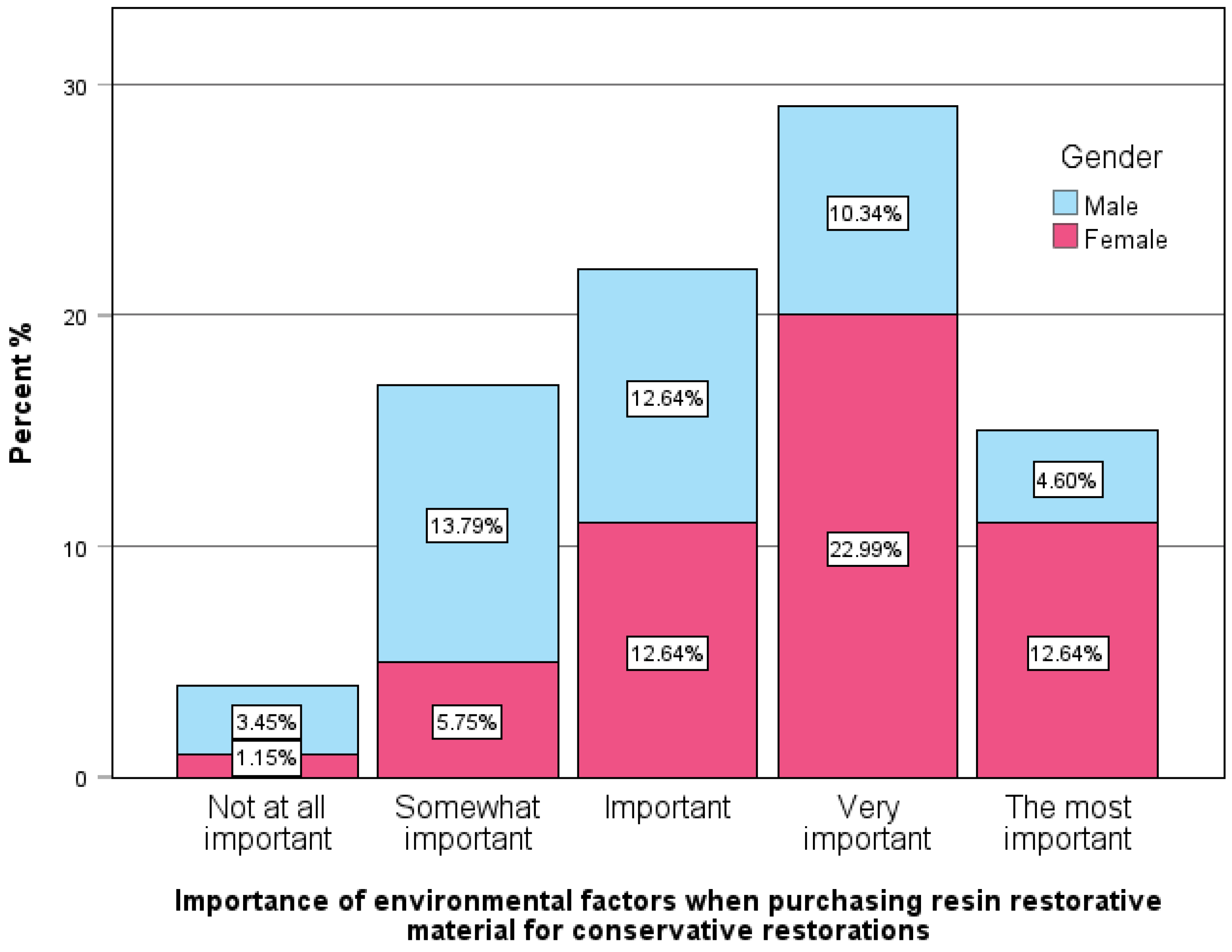
4.4. Sustainability and Gender-Based Preferences
4.5. Implications for Clinical Education and Future Research
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Study Questionnaire
- -
- Q1.1. Male
- -
- Q1.2. Female
- -
- Q1.3. Other
- -
- Q2.1. 24–35
- -
- Q2.2. 36–45
- -
- Q2.3. 46–55
- -
- Q2.4. 56–65
- -
- Q2.5. 66–75
- -
- Q3.1. Graduate of a dental school in Greece
- -
- Q3.2. Graduate of a dental school abroad
- -
- Q3.3. Master’s degree in dentistry
- -
- Q3.4. Master’s degree in a related field
- -
- Q3.5. Doctorate (PhD) in dentistry
- -
- Q3.6. Doctorate (PhD) in a related field
- -
- Q3.7. Additional degree in another discipline outside of dentistry
- -
- Q4.1. Private dental office (own practice)
- -
- Q4.2. Work at a colleague’s dental office
- -
- Q4.3. Work in a group practice with more than 3 dentists
- -
- Q4.4. Work in a university clinic
- -
- Q4.5. Work in a public institution
- -
- Q4.6. Other
- -
- Q5.1. 0–5
- -
- Q5.2. 6–10
- -
- Q5.3. 11–15
- -
- Q5.4. 16–20
- -
- Q5.5. 21–25
- -
- Q5.6. 26–30
- -
- Q5.7. More than 31
- -
- Q6.1. Once per year
- -
- Q6.2. Twice per year
- -
- Q6.3. More than twice per year
- -
- Q6.4. I stock up when there are special offers
- -
- Q6.5. Whenever the previous stock runs out
- -
- Q6.6. I do not purchase materials myself; someone else handles procurement
- -
- Q6.7. I do not purchase resin-based materials because I specialize in an area that does not use them
- -
- Q7.1. Fewer than 20
- -
- Q7.2. 20–50
- -
- Q7.3. More than 50
- -
- Q7.4. I don’t know/prefer not to answer
- -
- Q7.5. Other: __________
- -
- Q8.1. Its composition
- -
- Q8.2. Its biocompatibility
- -
- Q8.3. Its potential adverse effects
- -
- Q8.4. Its lifespan
- -
- Q8.5. Its application method
- -
- Q8.6. Its type (hybrid, nanofilled, etc.)
- -
- Q9.1. Increased orders of resin-based materials
- -
- Q9.2. Decreased orders of resin-based materials
- -
- Q9.3. Greater interest in materials with easy and fast workflows
- -
- Q9.4. Less interest in materials with easy and fast workflows
- -
- Q9.5. More interest in trying new materials
- -
- Q9.6. Less interest in trying new materials
- -
- Q9.7. No significant change in preferences
- -
- Q9.8. I don’t know/prefer not to answer
- -
- Q9.9. Other: __________
- -
- Q10.1. Desired anatomical features
- -
- Q10.2. Available interdental space
- -
- Q10.3. Shade of adjacent teeth
- -
- Q10.4. Translucency and opacity of adjacent teeth
- -
- Q10.5. No specific criteria; I use whatever is in stock
- -
- Q10.6. Use only specialized anterior resins
- -
- Q10.7. I don’t know/prefer not to answer
- -
- Q10.8. Other: __________
- -
- Q11.1. Desired anatomical features
- -
- Q11.2. Available interdental space
- -
- Q11.3. Shade of adjacent teeth
- -
- Q11.4. No specific criteria; I use whatever is in stock
- -
- Q11.5. I don’t know/prefer not to answer
- -
- Q11.6. Other: __________
- -
- Q12.1. Amalgam
- -
- Q12.2. High-viscosity (packable) composite resin
- -
- Q12.3. Flowable composite resin
- -
- Q12.4. Bulk-fill resin composite
- -
- Q12.5. Glass ionomer cement
- -
- Q12.6. Other: __________
- -
- Q13.1. Price
- -
- Q13.2. Quality
- -
- Q13.3. Manufacturer’s reputation
- -
- Q13.4. Material properties (e.g., biocompatibility, strength)
- -
- Q13.5. Ease of handling
- -
- Q13.6. Availability on the market
- -
- Q13.7. Compliance with standards
- -
- Q13.8. Patient safety
- -
- Q13.9. Staff safety
- -
- Q13.10. Environmental reasons
- -
- Q14.1. Yes
- -
- Q14.2. No
- -
- Q14.3. I don’t know/prefer not to answer
- -
- Q15.1. Very important
- -
- Q15.2. Quite important
- -
- Q15.3. Moderately important
- -
- Q15.4. Indifferent
- -
- Q15.5. Not important
- -
- Q16.1. Biocompatibility
- -
- Q16.2. Depth of cure
- -
- Q16.3. Flexural strength
- -
- Q16.4. Water sorption
- -
- Q16.5. Solubility
- -
- Q16.6. Radiopacity
- -
- Q16.7. None
- -
- Q16.8. I don’t know/prefer not to answer
- -
- Q17.1. Lower cost
- -
- Q17.2. From a trusted brand
- -
- Q17.3. Easier to handle
- -
- Q17.4. With longer shelf life
- -
- Q17.5. Most important for me is that it meets ISO standards
- -
- Q17.6. I don’t know/prefer not to answer
- -
- Q17.7. Other: __________
- -
- Q18.1. Has greater color stability
- -
- Q18.2. Requires less curing time and thus less working time
- -
- Q18.3. Has greater radiopacity than dentin and is more visible on radiographs
- -
- Q18.4. I do not consider flexural strength important
- -
- Q18.5. I would not choose a material lacking this property for posterior teeth
- -
- Q18.6. I would not choose a material with inferior physical and mechanical properties
- -
- Q18.7. I don’t know/prefer not to answer
- -
- Q18.8. Other: __________
- -
- Q19.1. I like to try new materials frequently to see what works best.
- -
- Q19.2. I look for published studies on effectiveness and longevity before trying a new material.
- -
- Q19.3. I prefer materials with a long record of clinical success before adopting them.
- -
- Q19.4. I rarely try new aesthetic materials.
- -
- Q19.5. I am interested in trying new generations of materials I already trust.
- -
- Q19.6. I almost never change the aesthetic resin materials I use unless they become unavailable.
- -
- Q19.7. I trust the materials I learned to use during dental school.
- -
- Q19.8. I generally trust materials that offer longer working time.
- -
- Q19.9. I trust materials that colleagues often speak positively about.
- -
- Q19.10. I trust materials promoted through printed advertising.
- -
- Q19.11. I trust materials promoted through digital media.
- -
- Q19.12. I have not noticed any conscious behavior when choosing direct aesthetic materials.
- -
- Q20.1. Compliance with ISO standards
- -
- Q20.2. Opinion of a trusted colleague about the product
- -
- Q20.3. Any discount offer from my supplier
- -
- Q20.4. Shelf life of the material
- -
- Q20.5. The carbon footprint of the product
- -
- Q20.6. Longevity of clinical restorations with the material
- -
- Q21.1. Appearance of the packaging
- -
- Q21.2. Environmental footprint of the packaging
- -
- Q21.3. Extensive promotional activities
- -
- Q21.4. Ease of procurement
- -
- Q21.5. Volume of packaging waste
- -
- Q21.6. Compliance with ISO standards
References
- Yadav, R.; Lee, H.H. Ranking and selection of dental restorative composite materials using FAHP-FTOPSIS technique: An application of multi criteria decision making technique. J. Mech. Behav. Biomed. Mater. 2022, 132, 105298. [Google Scholar] [CrossRef]
- Demarco, F.F.; Cenci, M.S.; Montagner, A.F.; de Lima, V.P.; Correa, M.B.; Moraes, R.R.; Opdam, N.J. Longevity of composite restorations is definitely not only about materials. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2023, 39, 1–12. [Google Scholar] [CrossRef]
- Shaw, K.; Martins, R.; Hadis, M.A.; Burke, T.; Palin, W. ‘Own-Label’ Versus Branded Commercial Dental Resin Composite Materials: Mechanical And Physical Property Comparisons. Eur. J. Prosthodont. Restor. Dent. 2016, 24, 122–129. [Google Scholar] [PubMed]
- Pratap, B.; Gupta, R.K.; Bhardwaj, B.; Nag, M. Resin based restorative dental materials: Characteristics and future perspectives. Jpn. Dent. Sci. Rev. 2019, 55, 126–138. [Google Scholar] [CrossRef] [PubMed]
- Heintze, S.D.; Ilie, N.; Hickel, R.; Reis, A.; Loguercio, A.; Rousson, V. Laboratory mechanical parameters of composite resins and their relation to fractures and wear in clinical trials—A systematic review. Dent. Mater. 2017, 33, e101–e114. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Ren, L.; Cheng, Y.; Xu, M.; Luo, W.; Zhan, D.; Sano, H.; Fu, J. Evaluation of the Color Stability, Water Sorption, and Solubility of Current Resin Composites. Materials 2022, 15, 6710. [Google Scholar] [CrossRef]
- Aminoroaya, A.; Neisiany, R.E.; Khorasani, S.N.; Panahi, P.; Das, O.; Madry, H.; Cucchiarini, M.; Ramakrishna, S. A review of dental composites: Challenges, chemistry aspects, filler influences, and future insights. Compos. Part B Eng. 2021, 216, 108852. [Google Scholar] [CrossRef]
- Schmalz, G.; Watts, D.C.; Darvell, B.W. Dental materials science: Research, testing and standards. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2021, 37, 379–381. [Google Scholar] [CrossRef]
- Schmalz, G.; Schwendicke, F.; Hickel, R.; Platt, J. Alternative Direct Restorative Materials for Dental Amalgam: A Concise Review Based on an FDI Policy Statement. Inter. Dent. J. 2023, 74, 661–668. [Google Scholar] [CrossRef]
- Soni, N.; Bairwa, S.; Sumita, S.; Goyal, N.; Choudhary, S.; Gupta, M.; Khurana, M. Mechanical Properties of Dental Resin Composites: A Review. Inter. J. Res. Publ. Rev. 2024, 5, 7675–7683. [Google Scholar] [CrossRef]
- Scopes-ISO/TC 106; Dentistry Subcommittees 1 and 2. International Organization for Standardization: Geneva, Switzerland, 1962. Available online: https://www.iso.org/committee/51218.html (accessed on 3 May 2025).
- ADA Division of Science ACoSA. Resin-based composites. J. Am. Dent. 2003, 134, 510–512. [Google Scholar] [CrossRef]
- ISO 4049:2019; Dentistry-Polymer-Based Restorative Materials. International Organization for Standardization: Geneva, Switzerland, 2019.
- Cho, K.; Rajan, G.; Farrar, P.; Prusty, G. Dental resin composites: A review on materials to product realizations. Compos. Part B Eng. 2021, 230, 109495. [Google Scholar] [CrossRef]
- Ferracane, J.L.; Hilton, T.J.; Stansbury, J.W.; Watts, D.C.; Silikas, N.; Ilie, N.; Heintze, S.; Cadenaro, M.; Hickel, R. Academy of Dental Materials guidance-Resin composites: Part II-Technique sensitivity (handling, polymerization, dimensional changes). Dent. Mater. Off. Publ. Acad. Dent. Mater. 2017, 33, 1171–1191. [Google Scholar] [CrossRef]
- Ilie, N.; Hilton, T.J.; Heintze, S.D.; Hickel, R.; Watts, D.C.; Silikas, N.; Stansbury, J.W.; Cadenaro, M.; Ferracane, J.L. Academy of Dental Materials guidance-Resin composites: Part I-Mechanical properties. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2017, 33, 880–894. [Google Scholar] [CrossRef]
- Yap, A.U.; Eweis, A.H.; Yahya, N.A. Dynamic and Static Flexural Appraisal of Resin-based Composites: Comparison of the ISO and Mini-flexural Tests. Oper. Dent. 2018, 43, E223–E231. [Google Scholar] [CrossRef] [PubMed]
- Shaabin, N.M.S.; Khayyat, R.H.; Al-Ahmadi, H.S.; Halal, R.N.; Tawati, A.A.; Shaabin, M.M.S.; Addas, N.A.; Linjawi, M.S.; Balubaid, W.S.; Garanbish, M.F.; et al. Material Selection for Posterior Restorations: An Observational Study Evaluating Dentists’ Preferences in Jeddah, Saudi Arabia. J. Popul. Ther. Clin. Pharmacol. 2022, 30, 649–659. [Google Scholar]
- Ghoneim, A.; Yu, B.; Lawrence, H.; Glogauer, M.; Shankardass, K.; Quiñonez, C. What influences the clinical decision-making of dentists? A cross-sectional study. PLoS ONE 2020, 15, e0233652. [Google Scholar] [CrossRef] [PubMed]
- Arandi, N.Z. Current trends in placing posterior composite restorations: Perspectives from Palestinian general dentists: A questionnair study. J. Inter. Soc. Prev. Community Dent. 2024, 14, 112–120. [Google Scholar] [CrossRef]
- Nascimento, G.G.; Correa, M.B.; Opdam, N.; Demarco, F.F. Do clinical experience time and postgraduate training influence the choice of materials for posterior restorations? Results of a survey with Brazilian general dentists. Braz. Dent. J. 2013, 24, 642–646. [Google Scholar] [CrossRef]
- Khaleefa, S.; Yeslam, H.; Hasanain, F. Knowledge and Attitude of Recent Dental Graduates towards Smart/Bioactive Dental Composites. J. Pharm. Res. Inter. 2021, 33, 34–44. [Google Scholar]
- ALmalki, W.D.; Ingle, N.; Assery, M.; Alsanea, J. Dentists’ Knowledge, Attitude, and Practice Regarding Evidence-Based Dentistry Practice in Riyadh, Saudi Arabia. J. Pharm. Bioallied Sci. 2019, 11 (Suppl. S3), S507–S514. [Google Scholar] [CrossRef]
- Ogiemwonyi, O.; Alam, M.; Alshareef, R.; Alsolamy, M.; Azizan, N.; Mat, N. Environmental factors affecting green purchase behaviors of the consumers: Mediating role of environmental attitude. Clean. Environ. Syst. 2023, 10, 100130. [Google Scholar] [CrossRef]
- Ririn, Y.; Rahmat, S.T.Y.; Rina, A. How packaging, product quality and promotion affect the purchase intention? Russ. J. Agric. Socio-Econ. Sci. 2019, 92, 46–55. [Google Scholar]
- Rundh, B. Linking packaging to marketing: How packaging is influencing the marketing strategy. Br. Food J. 2013, 115, 1547–1563. [Google Scholar] [CrossRef]
- Duane, B.; Ramasubbu, D.; Harford, S.; Steinbach, I.; Stancliffe, R.; Croasdale, K.; Pasdeki-Clewer, E. Environmental sustainability and procurement: Purchasing products for the dental setting. Br. Dent. J. 2019, 226, 453–458. [Google Scholar] [CrossRef]
- Moshkbid, E.; Cree, D.E.; Bradford, L.; Zhang, W. Biodegradable Alternatives to Plastic in Medical Equipment: Current State, Challenges, and the Future. J. Compos. Sci. 2024, 8, 342. [Google Scholar] [CrossRef]
- Mulimani, P. Green dentistry: The art and science of sustainable practice. Br. Dent. J. 2017, 222, 954–961. [Google Scholar] [CrossRef]
- Maier, C.; Thatcher, J.; Grover, V.; Dwivedi, Y. Cross-sectional research: A critical perspective, use cases, and recommendations for IS research. Inter. J. Inf. Manag. 2023, 70, 102625. [Google Scholar] [CrossRef]
- Ahmed, A.; Pereira, L.; Jane, K. Mixed Methods Research: Combining both qualitative and quantitative approaches. Available online: https://www.researchgate.net/publication/384402328_Mixed_Methods_Research_Combining_both_qualitative_and_quantitative_approaches (accessed on 1 June 2024).
- Chai, H.H.; Gao, S.S.; Chen, K.J.; Duangthip, D.; Lo, E.C.M.; Chu, C.H. A Concise Review on Qualitative Research in Dentistry. Int. J. Environ. Res. Public Health 2021, 18, 942. [Google Scholar] [CrossRef]
- Ranganathan, P.; Caduff, C. Designing and validating a research questionnaire—Part 1. Perspect. Clin. Res. 2023, 14, 152–155. [Google Scholar] [CrossRef]
- Khanal, B.; Chhetri, D. A Pilot Study Approach to Assessing the Reliability and Validity of Relevancy and Efficacy Survey Scale. Janabhawana Res. J. 2024, 3, 35–49. [Google Scholar] [CrossRef]
- Brewster, J.; Roberts, H.W. 12-Month flexural mechanical properties of conventional and self-adhesive flowable resin composite materials. Dent. Mater. J. 2023, 42, 598–609. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, L.; Fabiano, F.; Bonaccorsi, L.M.; Fabiano, V.; Borsellino, C. Evaluation of the Clinical Impact of ISO 4049 in Comparison with Miniflexural Test on Mechanical Performances of Resin Based Composite. Int. J. Biomater. 2015, 2015, 149798. [Google Scholar] [CrossRef] [PubMed]
- Erickson, R.L.; Barkmeier, W.W. Comparisons of ISO depth of cure for a resin composite in stainless-steel and natural-tooth molds. Eur. J. Oral Sci. 2019, 127, 556–563. [Google Scholar] [CrossRef]
- Fan, P.L.; Schumacher, R.M.; Azzolin, K.; Geary, R.; Eichmiller, F.C. Curing-light intensity and depth of cure of resin-based composites tested according to international standards. J. Am. Dent. Assoc. 2002, 33, 429–434, quiz 91–93. [Google Scholar] [CrossRef]
- Flury, S.; Hayoz, S.; Peutzfeldt, A.; Hüsler, J.; Lussi, A. Depth of cure of resin composites: Is the ISO 4049 method suitable for bulk fill materials? Dent. Mater. Off. Publ. Acad. Dent. Mater. 2012, 28, 521–528. [Google Scholar] [CrossRef]
- Heintze, S.; Zimmerli, B. Relevance of in-vitro tests of adhesive and composite dental materials. A review in 3 parts. Part 2: Non-standardized tests of composite materials. Schweiz. Monatsschrift Zahnmed. 2011, 121, 916–930. [Google Scholar]
- Heintze, S.D.; Zimmerli, B. Relevance of in vitro tests of adhesive and composite dental materials, a review in 3 parts. Part 1: Approval requirements and standardized testing of composite materials according to ISO specifications. Schweiz. Monatsschrift Zahnmed. 2011, 121, 804–816. [Google Scholar]
- Ilie, N. ISO 4049 versus NIST 4877: Influence of stress configuration on the outcome of a three-point bending test in resin-based dental materials and interrelation between standards. J. Dent. 2021, 110, 103682. [Google Scholar] [CrossRef]
- Moore, B.K.; Platt, J.A.; Borges, G.; Chu, T.M.; Katsilieri, I. Depth of cure of dental resin composites: ISO 4049 depth and microhardness of types of materials and shades. Oper. Dent. 2008, 33, 408–412. [Google Scholar] [CrossRef]
- Zhang, N.; Xie, C. Polymerization shrinkage, shrinkage stress, and mechanical evaluation of novel prototype dental composite resin. Dent. Mater. J. 2020, 39, 1064–1071. [Google Scholar] [CrossRef]
- Burke, F.J. The evidence base for ‘own label’ resin-based dental restoratives. Dent. Update 2013, 40, 5–6. [Google Scholar] [CrossRef] [PubMed]
- Klaiman, K.; Ortega, D.; Garnache, C. Consumer preferences and demand for packaging material and recyclability. Resour. Conserv. Recycl. 2016, 115, 1–8. [Google Scholar] [CrossRef]
- Mallinson, D.J.; Hatemi, P.K. The effects of information and social conformity on opinion change. PLoS ONE 2018, 13, e0196600. [Google Scholar] [CrossRef] [PubMed]
- Megremis, S.J. Assuring the Safety of Dental Materials: The Usefulness and Application of Standards. Dent. Clin. North Am. 2022, 66, 673–689. [Google Scholar] [CrossRef]
- Mittal, R.; Maheshwari, R.; Tripathi, S.; Pandey, S. Eco-friendly dentistry: Preventing pollution to promoting sustainability. Indian J. Dent. Sci. 2020, 12, 251. [Google Scholar] [CrossRef]
- Prudnikov, Y.; Nazarenko, A. The role of content marketing in the promotion of medical goods and services. Health Econ. Manag. Rev. 2021, 2, 23–29. [Google Scholar] [CrossRef]
- Zaware, P.D.N. Exploration of market potential towards dental material brands: An assessment with preferences of dentists in India. Int. J. Psychosoc. Rehabil. 2020, 24, 4015–4026. [Google Scholar] [CrossRef]
- Bujang, M.A.; Omar, E.; Foo, D.; Hon, Y.K. Sample size determination for conducting a pilot study to assess reliability of a questionnaire. Restor. Dent. Endod. 2024, 49, e3. [Google Scholar] [CrossRef]
- Hussey, I.; Alsalti, T.; Bosco, F.; Elson, M.; Arslan, R. An Aberrant Abundance of Cronbach’s Alpha Values at.70. Adv. Methods Pract. Psychol. Sci. 2025, 8, 25152459241287123. [Google Scholar] [CrossRef]
- Tavakol, M.; Dennick, R. Making Sense of Cronbach’s Alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, A.A.; Prakash, N.; Almagbol, M.; Alobaid, M.; Alqarni, A.; Altamni, H. Synoptic review on existing and potential sources for bias in dental research methodology with methods on their prevention and remedies. World J. Methodol. 2023, 13, 426–438. [Google Scholar] [CrossRef]
- Vaidyanathan, A.K. Controlling bias in research. J. Indian Prosthodont. Soc. 2022, 22, 311–313. [Google Scholar] [CrossRef] [PubMed]
- Bispo Júnior, J.P. Social desirability bias in qualitative health research. Rev. Saude Publica 2022, 56, 101. [Google Scholar] [CrossRef] [PubMed]
- Latkin, C.A.; Edwards, C.; Davey-Rothwell, M.A.; Tobin, K.E. The relationship between social desirability bias and self-reports of health, substance use, and social network factors among urban substance users in Baltimore, Maryland. Addict. Behav. 2017, 73, 133–136. [Google Scholar] [CrossRef]
- Guo, M.; Wang, Y.; Yang, Q.; Li, R.; Zhao, Y.; Li, C.; Zhu, M.; Cui, Y.; Jiang, X.; Sheng, S.; et al. Normal Workflow and Key Strategies for Data Cleaning Toward Real-World Data: Viewpoint. Interact. J. Med. Res. 2023, 12, e44310. [Google Scholar] [CrossRef]
- Ranganathan, P.; Hunsberger, S. Handling missing data in research. Perspect. Clin. Res. 2024, 15, 99–101. [Google Scholar] [CrossRef]
- Ahmed, I.; Ishtiaq, S. Reliability and validity: Importance in Medical Research. JPMA J. Pak. Med. Assoc. 2021, 71, 2401–2406. [Google Scholar] [CrossRef]
- Sengupta, A.; Naka, O.; Mehta, S.B.; Banerji, S. The clinical performance of bulk-fill versus the incremental layered application of direct resin composite restorations: A systematic review. Evid. Based Dent. 2023, 24, 143. [Google Scholar] [CrossRef]
- Chesterman, J.; Jowett, A.; Gallacher, A.; Nixon, P. Bulk-fill resin-based composite restorative materials: A review. BDJ 2017, 222, 337–344. [Google Scholar] [CrossRef]
- Matos, J.D.; Nakano, L.J.; Lopes, G.R.; Bottino, M.A.; Vasconcelos, J.E.; Jesus, R.H.; Maciel, L.C. Characterization of Bulk-Fill Resin Composites in Terms of Physical, Chemical, Mechanical and Optical Properties and Clinical Behavior. Int. J. Odontostomatol. 2021, 15, 226–233. [Google Scholar] [CrossRef]
- Sikka, N.; Brizuela, M. Glass Ionomer Cement. In StatPearls; StatPearls Publishing LLC: Treasure Island, FL, USA, 2025. [Google Scholar]
- Ulku, S.G.; Unlu, N. Factors influencing the longevity of posterior composite restorations: A dental university clinic study. Heliyon 2024, 10, e27735. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, J.; Wilhelm, C.; Urich, J.; Weigl, P.; Sader, R. Different Esthetic Assessment of Anterior Restorations by Patient and Expert: A Prospective Clinical Study. J. Esthet. Restor. Dent. 2025, 37, 1113–1118. [Google Scholar] [CrossRef] [PubMed]
- A Al-Asmar, A.; Al-Hiyasat, A.S.; Abu-Awwad, M.; Mousa, H.N.; A Salim, N.; Almadani, W.; Rihan, F.; A Sawair, F.; Pitts, N.B.; Dioguardi, M. Reframing Perceptions in Restorative Dentistry: Evidence-Based Dentistry and Clinical Decision-Making. Int. J. Dent. 2021, 2021, 4871385. [Google Scholar] [CrossRef]
- Girotto, L.P.S.; Dotto, L.; Pereira, G.K.R.; Bacchi, A.; Sarkis-Onofre, R. Restorative preferences and choices of dentists and students for restoring endodontically treated teeth: A systematic review of survey studies. J. Prosthet. Dent. 2021, 126, 489.e5. [Google Scholar] [CrossRef]
- Pizzolotto, L.; Moraes, R.R. Resin Composites in Posterior Teeth: Clinical Performance and Direct Restorative Techniques. Dent. J. 2022, 10, 222. [Google Scholar] [CrossRef]
- Caussin, E.; Izart, M.; Ceinos, R.; Attal, J.-P.; Beres, F.; François, P. Advanced Material Strategy for Restoring Damaged Endodontically Treated Teeth: A Comprehensive Review. Materials 2024, 17, 3736. [Google Scholar] [CrossRef]
- Murchie, B.; Jiwan, N.; Edwards, D. What are the success rates of anterior restorations used in localised wear cases? Evid. Based Dent. 2025, 26, 54–56. [Google Scholar] [CrossRef]
- Balestra, D.; Lowther, M.; Goracci, C.; Mandurino, M.; Cortili, S.; Paolone, G.; Louca, C.; Vichi, A. 3D Printed Materials for Permanent Restorations in Indirect Restorative and Prosthetic Dentistry: A Critical Review of the Literature. Materials 2024, 17, 1380. [Google Scholar] [CrossRef]
- Mai, H.N.; Lee, K.B.; Lee, D.H. Fit of interim crowns fabricated using photopolymer-jetting 3D printing. J. Prosthet. Dent. 2021, 125, 577–584. [Google Scholar] [CrossRef]
- Shibata, S.; Hoshika, S.; Inokoshi, M.; Minakuchi, S. Effect of post-curing conditions on the mechanical properties of three-dimensional printed provisional restorative material. Dent Mater J. 2021, 40, 715–722. [Google Scholar]
- Ille, C.-E.; Jivănescu, A.; Pop, D.; Stoica, E.T.; Flueras, R.; Talpoş-Niculescu, I.-C.; Cosoroabă, R.M.; Popovici, R.-A.; Olariu, I. Exploring the Properties and Indications of Chairside CAD/CAM Materials in Restorative Dentistry. J. Funct. Biomater. 2025, 16, 46. [Google Scholar] [CrossRef] [PubMed]
- Barakat, B.; Milhem, M.; Naji, G.M.A.; Alzoraiki, M.; Muda, H.B.; Ateeq, A.; Abro, Z. Assessing the Impact of Green Training on Sustainable Business Advantage: Exploring the Mediating Role of Green Supply Chain Practices. Sustainability 2023, 15, 14144. [Google Scholar] [CrossRef]
- Kaurani, P.; Batra, K.; Hooja, H.R.; Chander, N.G.; Bhowmick, A.; Arora, S.; Baba, S.M.; Khateeb, S.U.; Abdulla, A.M.; Grover, V.; et al. Assessing the Compliance of Dental Clinicians towards Regulatory Infection Control Guidelines Using a Newly Developed Survey Tool: A Pilot Cross-Sectional Study in India. Healthcare 2022, 10, 1877. [Google Scholar] [CrossRef] [PubMed]
- Boulding, H.; Hinrichs-Krapels, S. Factors influencing procurement behaviour and decision-making: An exploratory qualitative study in a UK healthcare provider. BMC Health Serv. Res. 2021, 21, 1087. [Google Scholar] [CrossRef]
- Antoniadou, M.; Chrysochoou, G.; Tzanetopoulos, R.; Riza, E. Green Dental Environmentalism among Students and Dentists in Greece. Sustainability 2023, 15, 9508. [Google Scholar] [CrossRef]
- Beske-Janssen, P.; Johnsen, T.; Constant, F.; Wieland, A. New competences enhancing Procurement’s contribution to innovation and sustainability. J. Purch. Supply Manag. 2023, 29, 100847. [Google Scholar] [CrossRef]
- Barnes, E.; Bullock, A.D.; Bailey, S.E.; Cowpe, J.G.; Karaharju-Suvanto, T. A review of continuing professional development for dentists in Europe*. Eur. J. Dent. Edu. 2013, 17 (Suppl. S1), 5–17. [Google Scholar] [CrossRef]
- Țâncu, A.M.C.; Imre, M.; Iosif, L.; Pițuru, S.M.; Pantea, M.; Sfeatcu, R.; Ilinca, R.; Bodnar, D.C.; Didilescu, A.C. Is Sustainability Part of the Drill? Examining Knowledge and Awareness Among Dental Students in Bucharest, Romania. Dent. J. 2025, 13, 114. [Google Scholar] [CrossRef]
- Antoniadou, M.; Intzes, A.; Kladouchas, C.; Christou, I.; Chatzigeorgiou, S.; Plexida, M.; Stefanidakis, V.; Tzoutzas, I. Factors Affecting Water Quality and Sustainability in Dental Practices in Greece. Sustainability 2023, 15, 9115. [Google Scholar] [CrossRef]
- Kichenin, J.; Vallaeys, K.; Arbab Chirani, R.; Duncan, H.F.; Chevalier, V. How does gender influence student learning, stress and career choice in endodontics? Int. Endod. J. 2025. [Google Scholar] [CrossRef]
- Wolbring, G.; Nguyen, A. Equity/Equality, Diversity and Inclusion, and Other EDI Phrases and EDI Policy Frameworks: A Scoping Review. Trends High. Educ. 2023, 2, 168–237. [Google Scholar] [CrossRef]
- Al-Sbei, R.; Ataya, J.; Jamous, I.; Dashash, M. The Impact of a Web-Based Restorative Dentistry Course on the Learning Outcomes of Dental Graduates: Pre-Experimental Study. JMIR Form. Res. 2024, 8, e51141. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.M.; Chang, Y.C. Initiating gender mainstreaming in dentistry. J. Dent. Sci. 2022, 17, 1411–1412. [Google Scholar] [CrossRef] [PubMed]
- Spaveras, A.; Antoniadou, M. Awareness of Students and Dentists on Sustainability Issues, Safety of Use and Disposal of Dental Amalgam. Dent. J. 2023, 11, 21. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, K.; Ferguson, C.; Walczak, A.; Middleton, S.; Levi, C.; Morton, R.L.; Australian Health Research Alliance (AHRA) Health System Improvement and Sustainability Working Group Members. Which strategies support the effective use of clinical practice guidelines and clinical quality registry data to inform health service delivery? A systematic review. Syst. Rev. 2022, 9, 237. [Google Scholar] [CrossRef]
- Mohammadipour, H.S.; Yazdi, S.S.; Mashhad, M.J.M.; Babazadeh, S.; Shahri, A. Color matching and translucency of single-shade resin composites: Effects of restoration thickness, background shade, and aging. BMC Oral Health 2025, 25, 616. [Google Scholar] [CrossRef]
- Gheorghe, A.; Roberts, T.E.; Ives, J.C.; Fletcher, B.R.; Calvert, M. Centre selection for clinical trials and the generalisability of results: A mixed methods study. PLoS ONE 2013, 8, e56560. [Google Scholar] [CrossRef]
- Torgerson, D.J.; Torgerson, C.J. Pilot Randomised Controlled Trials. In Designing Randomised Trials in Health, Education and the Social Sciences: An Introduction; Torgerson, D.J., Torgerson, C.J., Eds.; Palgrave Macmillan: London, UK, 2008; pp. 119–126. [Google Scholar]
- Patino, C.M.; Ferreira, J.C. Inclusion and exclusion criteria in research studies: Definitions and why they matter. J. Bras. Pneumol. Publ. Soc. Bras. Pneumol. Tisilogia 2018, 44, 84. [Google Scholar] [CrossRef]
- Leon, A.C.; Davis, L.L.; Kraemer, H.C. The role and interpretation of pilot studies in clinical research. J. Psychiatr. Res. 2011, 45, 626–629. [Google Scholar] [CrossRef]
- Thabane, L.; Ma, J.; Chu, R.; Cheng, J.; Ismaila, A.; Rios, L.P.; Robson, R.; Thabane, M.; Giangregorio, L.; Goldsmith, C.H. A tutorial on pilot studies: The what, why and how. BMC Med. Res. Methodol. 2010, 10, 1. [Google Scholar] [CrossRef]
- Hallingberg, B.; Turley, R.; Segrott, J.; Wight, D.; Craig, P.; Moore, L.; Murphy, S.; Robling, M.; Simpson, S.A.; Moore, G. Exploratory studies to decide whether and how to proceed with full-scale evaluations of public health interventions: A systematic review of guidance. Pilot Feasibility Stud. 2018, 4, 104. [Google Scholar] [CrossRef]
- Bornstein, M.; Al-Nawas, B.; Kuchler, U.; Tahmaseb, A. Consensus Statements and Recommended Clinical Procedures Regarding Contemporary Surgical and Radiographic Techniques in Implant Dentistry. Int. J. Oral Maxillofac. Implant. 2014, 29, 78–82. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Gender (Female vs. Male Dentists) | Age (over 45 Years vs. Younger) | Dental School (Foreign vs. Domestic) | Postgraduate Studies in Dentistry | Clinical Experience (over 5 Years vs. up to 5 Years) | Employment (Private Clinic vs. Other) | Purchasing Resin Restorations over 2 Times/Year | Not Responsible for Supply of Resin Restorations | Performing over 20 Composite Resin Restorations per Week | |
|---|---|---|---|---|---|---|---|---|---|
| Knowledge about resin materials | −0.152 | 0.236 * | 0.118 | 0.175 | 0.214 * | 0.055 | 0.062 | −0.052 | 0.195 |
| 1. Composition | −0.085 | 0.163 | 0.118 | 0.164 | 0.230 * | −0.044 | 0.061 | −0.153 | 0.206 |
| 2. Biocompatibility | −0.248 * | 0.045 | 0.158 | 0.138 | −0.014 | −0.015 | 0.129 | 0.098 | 0.081 |
| 3. Side effects | −0.084 | 0.135 | −0.052 | 0.072 | 0.033 | −0.041 | 0.072 | 0.179 | 0.041 |
| 4. Shelf life | −0.024 | 0.208 | 0.116 | 0.039 | 0.223 * | 0.170 | 0.110 | −0.145 | 0.149 |
| 5. Method of application | −0.012 | 0.214 * | 0.107 | 0.186 | 0.159 | 0.028 | −0.164 | 0.039 | 0.100 |
| 6. Type of material | −0.165 | 0.137 | 0.072 | 0.161 | 0.177 | 0.097 | −0.099 | −0.115 | 0.141 |
| N | % | ||
|---|---|---|---|
| Familiarity with specifications for dental resin restorative materials | Yes | 55 | 71.4% |
| No | 22 | 28.6% | |
| Importance of resin restorative material compliance with specifications | Very high | 28 | 32.2% |
| High | 47 | 54.0% | |
| Moderate | 12 | 13.8% | |
| Features priority when choosing resin restorative materials | Biocompatibility | 21 | 25.9% |
| Photopolymerization depth | 13 | 16.0% | |
| Bending strength | 28 | 34.6% | |
| Water absorbency, solubility, etc. | 19 | 23.5% | |
| Green practice but falls slightly short of some of the ISO specifications | Certainly yes | 4 | 4.9% |
| It depends on the specifications | 45 | 54.9% | |
| No, for me ISO standards are the most important selection criterion | 33 | 40.2% | |
| Total Sample | Clinical Experience (in Years) | |||||
|---|---|---|---|---|---|---|
| Up to 5 Years | Over 5 Years | |||||
| N | % | N | % | |||
| What are the selection criteria for the resin materials you choose for anterior tooth restorations? | ||||||
| It depends on the anatomical features I want to achieve | 47 | 54.0% | 31 | 70.5% | 16 | 37.2% |
| It depends on the interdental space that exists | 14 | 16.1% | 10 | 22.7% | 4 | 9.3% |
| It depends on the color of the neighboring teeth | 44 | 50.6% | 25 | 56.8% | 19 | 44.2% |
| It depends on the transparency and opacity of the neighboring teeth | 49 | 56.3% | 29 | 65.9% | 20 | 46.5% |
| I do not have a specific criterion, I use what I have in stock | 6 | 6.9% | 4 | 9.1% | 2 | 4.7% |
| I only use special anterior resins | 32 | 36.8% | 10 | 22.7% | 22 | 51.2% |
| What are the selection criteria for the resin materials you choose for posterior tooth restorations? | ||||||
| It depends on the anatomical features I want to achieve | 48 | 55.2% | 29 | 65.9% | 19 | 44.2% |
| It depends on the interdental space that exists | 24 | 27.6% | 15 | 34.1% | 9 | 20.9% |
| It depends on the color of the neighboring teeth | 25 | 28.7% | 14 | 31.8% | 11 | 25.6% |
| I do not have a specific criterion, I use what I have in stock | 24 | 27.6% | 10 | 22.7% | 14 | 32.6% |
| Selection Criteria for the Resin Materials | Gender (Female vs. Male) | Age (over 45 Years) | Dental School (Foreign vs. Domestic) | Postgraduate Studies in Dentistry | Clinical Experience (>5 Years) | Employment (Private Clinic vs. Other) | Purchasing Resin Restorations over 2 Times/Year | Not Responsible for Supply of Resin Restorations | Performing over 20 Restorations/Week |
|---|---|---|---|---|---|---|---|---|---|
| What are the selection criteria for the resin materials you choose for anterior tooth restorations? | |||||||||
| It depends on the anatomical features I want to achieve | −0.043 | −0.204 | 0.055 | −0.134 | −0.334 ** | −0.090 | 0.021 | 0.120 | −0.315 ** |
| It depends on the interdental space that exists | −0.108 | −0.054 | −0.117 | −0.020 | −0.183 | 0.017 | 0.044 | 0.112 | −0.071 |
| It depends on the color of the neighboring teeth | 0.080 | −0.105 | 0.025 | −0.127 | −0.126 | 0.033 | 0.166 | 0.017 | −0.160 |
| It depends on the transparency and opacity of the neighboring teeth | 0.185 | −0.239 * | −0.028 | −0.076 | −0.196 | −0.188 | 0.090 | 0.040 | −0.164 |
| I do not have a specific criterion, I use what I have in stock | −0.028 | −0.007 | −0.124 | 0.068 | −0.088 | 0.154 | −0.085 | 0.014 | 0.126 |
| I only use special anterior resins | 0.017 | 0.199 | 0.030 | 0.337 ** | 0.295 ** | −0.127 | 0.004 | −0.151 | 0.113 |
| What are the selection criteria for the resin materials you choose for posterior tooth restorations? | |||||||||
| It depends on the anatomical features I want to achieve | 0.071 | −0.173 | 0.044 | 0.085 | −0.218 * | −0.162 | 0.105 | 0.055 | −0.133 |
| It depends on the interdental space that exists | 0.091 | −0.123 | −0.077 | −0.058 | −0.147 | −0.012 | 0.142 | −0.025 | −0.037 |
| It depends on the color of the neighboring teeth | −0.041 | 0.020 | −0.021 | 0.132 | −0.069 | 0.164 | 0.178 | −0.097 | −0.057 |
| I do not have a specific criterion; I use what I have in stock | −0.116 | −0.015 | −0.009 | −0.164 | 0.110 | 0.039 | −0.192 | 0.086 | −0.018 |
| I do not know/do not answer | 0.097 | −0.078 | −0.049 | −0.084 | −0.107 | 0.097 | −0.072 | −0.072 | −0.083 |
| Gender (Female vs. Male) | Age (over 45 Years) | Dental School (Foreign vs. Domestic) | Post-Grad Studies in Dentistry | Clinical Experience (over 5 Years) | Employment (Private Clinic vs. Other) | Purchasing Resin Restorations over 2 Times/Year | Not Responsible for Supply of Resin Restorations | Performing over 20 Restorations/Week | |
|---|---|---|---|---|---|---|---|---|---|
| Familiarity with specifications | −0.033 | 0.076 | 0.132 | −0.108 | 0.231 * | −0.041 | 0.254 * | −0.341 ** | 0.163 |
| Specifications importance | 0.109 | 0.150 | 0.094 | 0.038 | 0.195 | −0.025 | 0.052 | −0.092 | 0.095 |
| Features priority when choosing resin restorative materials | |||||||||
| Biocompatibility | 0.232 * | 0.136 | 0.177 | 0.213 | 0.106 | −0.106 | −0.105 | 0.093 | −0.026 |
| Photopolymerization depth | −0.162 | −0.084 | −0.022 | −0.147 | 0.050 | −0.117 | −0.084 | −0.001 | 0.113 |
| Bending strength | −0.204 | −0.111 | 0.011 | −0.056 | −0.233 * | 0.181 | 0.112 | −0.092 | −0.078 |
| Water absorbency, Solubility, etc. | 0.130 | 0.056 | −0.176 | −0.030 | 0.108 | 0.009 | 0.056 | 0.009 | 0.019 |
| Green practice but falls slightly short of some of the ISO specifications | |||||||||
| Certainly yes | 0.092 | 0.181 | 0.066 | 0.057 | 0.113 | −0.028 | 0.211 | −0.021 | 0.182 |
| It depends on the specifications | 0.114 | −0.176 | 0.029 | −0.001 | −0.025 | −0.061 | −0.172 | 0.099 | 0.020 |
| No, for me ISO standards are the most important selection criterion | −0.155 | 0.099 | −0.058 | −0.024 | −0.025 | 0.075 | 0.082 | −0.091 | −0.102 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kontakou Zoniou, A.; Antoniadou, M.; Saridou, S. Selection of Resin-Based Dental Restorative Materials: A Pilot Study on Professional Characteristics, Knowledge, and Selection Criteria. Appl. Sci. 2025, 15, 7987. https://doi.org/10.3390/app15147987
Kontakou Zoniou A, Antoniadou M, Saridou S. Selection of Resin-Based Dental Restorative Materials: A Pilot Study on Professional Characteristics, Knowledge, and Selection Criteria. Applied Sciences. 2025; 15(14):7987. https://doi.org/10.3390/app15147987
Chicago/Turabian StyleKontakou Zoniou, Anna, Maria Antoniadou, and Sofia Saridou. 2025. "Selection of Resin-Based Dental Restorative Materials: A Pilot Study on Professional Characteristics, Knowledge, and Selection Criteria" Applied Sciences 15, no. 14: 7987. https://doi.org/10.3390/app15147987
APA StyleKontakou Zoniou, A., Antoniadou, M., & Saridou, S. (2025). Selection of Resin-Based Dental Restorative Materials: A Pilot Study on Professional Characteristics, Knowledge, and Selection Criteria. Applied Sciences, 15(14), 7987. https://doi.org/10.3390/app15147987