1. Introduction
Aging leads to neuromuscular control difficulties while performing balance and walking needed for daily living [
1]. With decreases in balance comes an increase in risk for falling leading to injury and even death; in the United States, one in four adults over 65 years old falls each year [
2]. Aging is often accompanied by degeneration of nerve and muscle tissues [
3] and of the sensory systems used for balance (i.e., visual, somatosensory, and vestibular), e.g., Ref. [
4]. Moreover, aging is associated with major changes in the neuromotor system. In particular, these include reduction in muscle strength, power, and joint mobility along with an impaired sensorimotor integration [
2]. Within the aging population, strokes are a prominent issue that can lead to disability and even death; over 60% of all strokes occur above the age of 65 years old [
5]. Thus, effective rehabilitation is important towards facilitating balance maintenance in both older individuals that consider themselves healthy and survivors of stroke. Unfortunately, only 60 to 70 percent of survivors of stroke are able to walk again independently after rehabilitation [
6].
In terms of quantifying balance and walking, common clinical measures have focused on qualitative tests, e.g., the commonly known Sit-to-Stand test and Timed Up and Go test (TUG), which can only offer crude, global, and/or descriptive information such as the time it takes to complete sitting and walking tasks, respectively. While kinematic measures (e.g., motion capture) can provide more detailed information in terms of movements, it is difficult to distinguish differences due to neural or musculoskeletal deficits. Further, forceplate methods (e.g., to measure center of pressure (COP)) may have limited applicability tied to movement due to the activation of different neural pathways because the same force and resulting movement can be achieved by many different muscle coordination patterns [
7].
Muscle activation and muscle synergy analysis facilitate the characterization of neuromuscular control strategies for movement. Surface electromyography (sEMG) is a commonly used, non-invasive measure to determine muscle activation. Through post-processing analysis of the raw sEMG signals, muscle synergies then can be determined tied to the activity of the muscles; thus, muscle synergy analysis can facilitate the characterization of neuromuscular control strategies and functional deficits [
1,
8,
9]. Via spatial and temporal activation examined from the recorded muscle activity, muscle synergies offer insight in terms of muscle coordination and activation patterns. Patients with impaired motor functions tend to show an adaptation of muscle synergies to typical characteristics of movement (such as type of movement, speed, compensation of asymmetry due to neurological damage) [
10]. After a stroke, fewer synergies are used during walking and upper-extremity tasks compared with unimpaired adults, possibly reflecting a simplified control strategy [
11,
12]; however, it will be interesting to determine if the same holds true for lower-extremity tasks such as walking. To the best of our knowledge, muscle synergy changes in older adults following several weeks of balance training have not been published, neither for healthy older adults nor survivors of stroke within the aged population.
Previous research regarding muscle synergies in humans has evaluated sEMG responses for walking and during platform perturbations, e.g., Refs. [
1,
12,
13,
14,
15,
16,
17]. The effects of directionality tied to muscle synergy have been examined (e.g., during perturbations for angles between 0 to 270 degrees), e.g., Refs. [
15,
17]. While directional perturbation approaches provide insight into how the central nervous system affects muscle synergies via muscle tuning curves, these stimuli are not a direct comparison and atypical for movement one experiences in daily living. Task-specific muscle synergies have been examined (e.g., by performing straight forward walking, as well as right and left turning) [
9]. However, the above studies have not considered quantifying the effects of balance training on muscle synergies (neither for healthy nor impaired older adults). Further, investigating the effects of more challenging balancing activities (e.g., tandem or backward walking) to evaluate the possibility of muscle synergy ‘improvement’ after training has not been determined. Although older adults could significantly decrease fall risk after balance training, neuromuscular metrics to determine which participants benefit from balance interventions are limited.
Here, by investigating neuromotor control during walking, we sought to understand real-life function and mobilization in the older population, as well as the impacts of balance training on both healthy older adults and older survivors of stroke. By examining whether muscle activation patterns and/or muscle synergies change following balance training (rehabilitation), we hypothesized that we could quantify and validate improvement of lower-limb motor function at the neural level in older adults. More specifically, we would see changes of decreases or increases in the number of synergies that reflect simplification or more complex control, respectively. Thus, we provide a proof of concept that muscle synergy analysis could be useful in comparing different groups of older adults’ balance training and determining if participants have gained motor functions that could generalize to activities of daily living, such as walking.
2. Materials and Methods
All study activities were conducted within the Center for Biomechanical and Rehabilitation Engineering (CBRE) laboratory at the University of the District of Columbia (UDC), the protocol was approved by the UDC Institutional Review Board (protocol no. 979744-1), and all participants gave their informed consent prior to participating in the study.
2.1. Participants
Participants were recruited for the study through flyers posted around the university and word of mouth. The population we were targeting were older individuals that considered themselves healthy and those who have suffered from stroke and were at least 6 months post-stroke. Our results are presented for 5 stroke (66.4 ± 9.48 years old) and 23 healthy participants (69.5 ± 5.7 years old). Participant demographics are shown in
Table 1 (healthy) and
Table 2 (survivors of stroke).
2.2. Training
Participants underwent a 6-week exercise routine which consisted of two 30 min sessions/week. During the sessions, the participants worked with the principal investigator and trainers (research assistants) who also served as spotters to support participants throughout the study as well as the NaviGAITor (multidirectional partial bodyweight support system) to prevent falls. This system did not provide bodyweight support but instead protected the participant in the event of a misstep or fall.
For the balance training sessions, each participant was worked with individually within the CBRE laboratory. Exercises were selected that required both healthy and stroke participants to make use of diverse sensory information to maintain their balance. During weeks one and two, participants performed walking exercises under both eyes-open and eyes-closed conditions, including forward and backward walking with both wide and tandem stepping. Weeks three and four focused on exercises conducted on foam surfaces of varying densities, incorporating standing balance tasks, isolated leg exercises, squats, and walking on hard, dense foam, or thick compliant foam surfaces. In weeks five and six, the training regimen combined walking over obstacles with additional foam-based exercises, further increasing sensory challenges and task complexity. The training consisted of various exercises that challenged visual, somatosensory, and vestibular systems to affect balance; vision was modified to make surroundings more or less challenging (eyes closed/eyes open, respectively), as well as supported surface somatosensory cues (hard or foam surfaces), while vestibular systems were highlighted by limiting combined visual and/or somatosensory cues (e.g., eyes closed while walking or standing on foam) [
18]. Additionally, the base of support (BOS) was modified between large and small (e.g., double-leg, tandem, and single-leg stances) to increase task difficulty. For example, a larger BOS (double-leg stance) allows for increased stability whereas a smaller BOS (tandem and single-leg stances) could lead to decreased stability.
2.3. Assessment
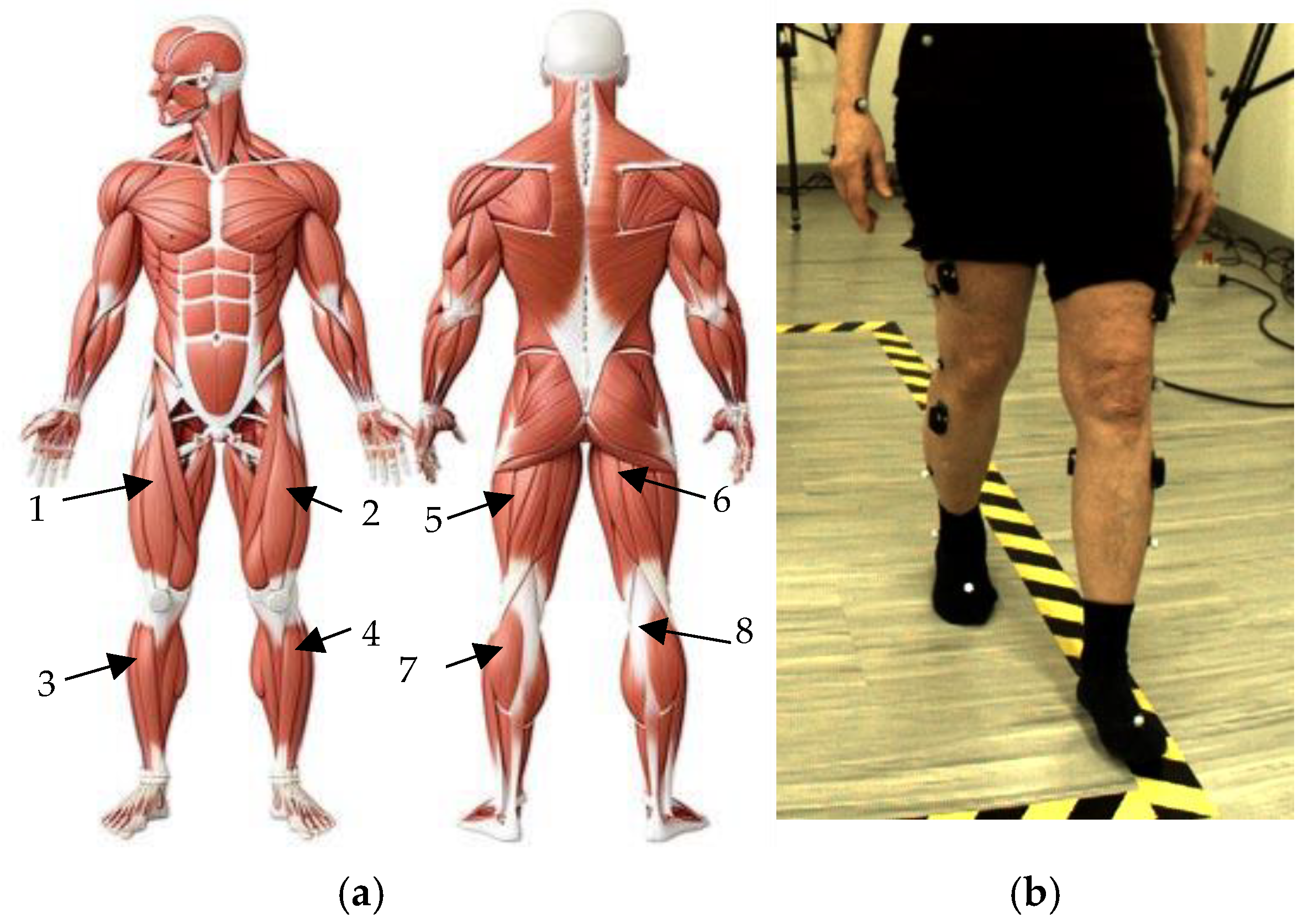
Prior to data collection, a light sponge was used to remove any surface layers of dead skin, then each participant’s skin was cleansed with alcohol wipes prior to attachment of the EMG sensors, and lastly each sensor was affixed with strong double-sided tape (provided by Delsys). Eight wireless Delsys surface electromyography sensors (sEMG) (Trigno, Delsys, Boston, MA, USA) were placed on each muscle: the right and left rectus femoris (RF), right and left tibialis anterior (TA), right and left bicep femoris (BF), and right and left medial gastrocnemius (MG) (
Figure 1). The sEMG data were collected using the Delsys Trigno System at a sampling frequency of 2000 Hz; the sEMG data was recorded, simultaneously with motion capture data, via Vicon Nexus 2.0 software.
Each participant completed a pre-assessment (at 0 weeks) and post-assessment (at 6 weeks) once the training was completed. Each participant performed forward and backward walking trials (FW and BW, respectively), in addition to forward and backward tandem walking trials (FT-W and BT-W, respectively), for a distance of 3 m, two trials per condition, per participant. Tandem walking is described as walking with one foot directly in front of the other, or heel to toe. For all walking trials, there was overground, unassisted walking and the participants were instructed to walk at their own, self-selected moderate pace.
2.4. Data Analysis
2.4.1. Preprocessing and Conditioning Raw sEMG Data
After data acquisition was complete, raw data from the 8 EMG sensors were exported to .csv files for each participant for each walking condition. Each .csv file then displayed the EMG output in terms of microvolts as a function of time. The sEMG data were imported to MATLAB R2024b (MathWorks, Natick, MA, USA) for further processing. The sEMG data underwent analysis and processing using custom MATLAB (version 2024b, Matick, MA, USA) files inspired by analyses performed in previous studies, e.g., Refs. [
1,
20,
21]. The preprocessing phase involved filtering muscle synergies using the raw EMG data. For the notch filter, built in function, “NotchPeakIIR()” with a center frequency of 40 Hz/sampling frequency, was implemented. The filtered output is again passed through a highpass filter using the “highpass()” function followed by a Butterworth lowpass filter, using the “filter()”function, where the 3rd-order Butterworth filter parameters are estimated from the function “butter()” using twice the center frequency as that of the notch filter. After highpass filtering the output undergoes demeaning and rectification. At the final step, the normalized response is interpolated, using the function “interp1()”, to maintain the uniform sampling of signal where 20 subframes for each time frame were recorded in the raw signal.
2.4.2. Determining Muscle Synergies: Non-Negative Matrix Factorization (NNMF)
Muscle synergies were identified using non-negative matrix factorization (NNMF). NNMF motor module analysis of muscle coordination [
17,
21] was implemented here but adapted to suit the specific context of our study. NNMF is a technique that assumes the set of measured data is composed of linear combinations of a smaller number of underlying elements. The NNMF process represents the original sEMG data as a linear combination of vectors called muscle synergies (
W) and activation coefficients (
H) as shown in Equation (1).
The matrix
defines spatial patterns of muscle activation across multiple muscles, or muscle synergies. This matrix is represented as the
matrix, where
is the number of muscle EMGs recorded (in this case 8) represented as rows and
is the number of synergies represented as columns. The values of
are between 0 and 1 as they are coefficients for normalized data. The matrix
describes the activation of the muscle contributions (or coefficients) over time, where
is the number of synergies represented as rows and
is the duration of each trial in samples represented as columns. The resulting (reconstructed) muscle activation,
M, is then predicted. A schematic is shown in
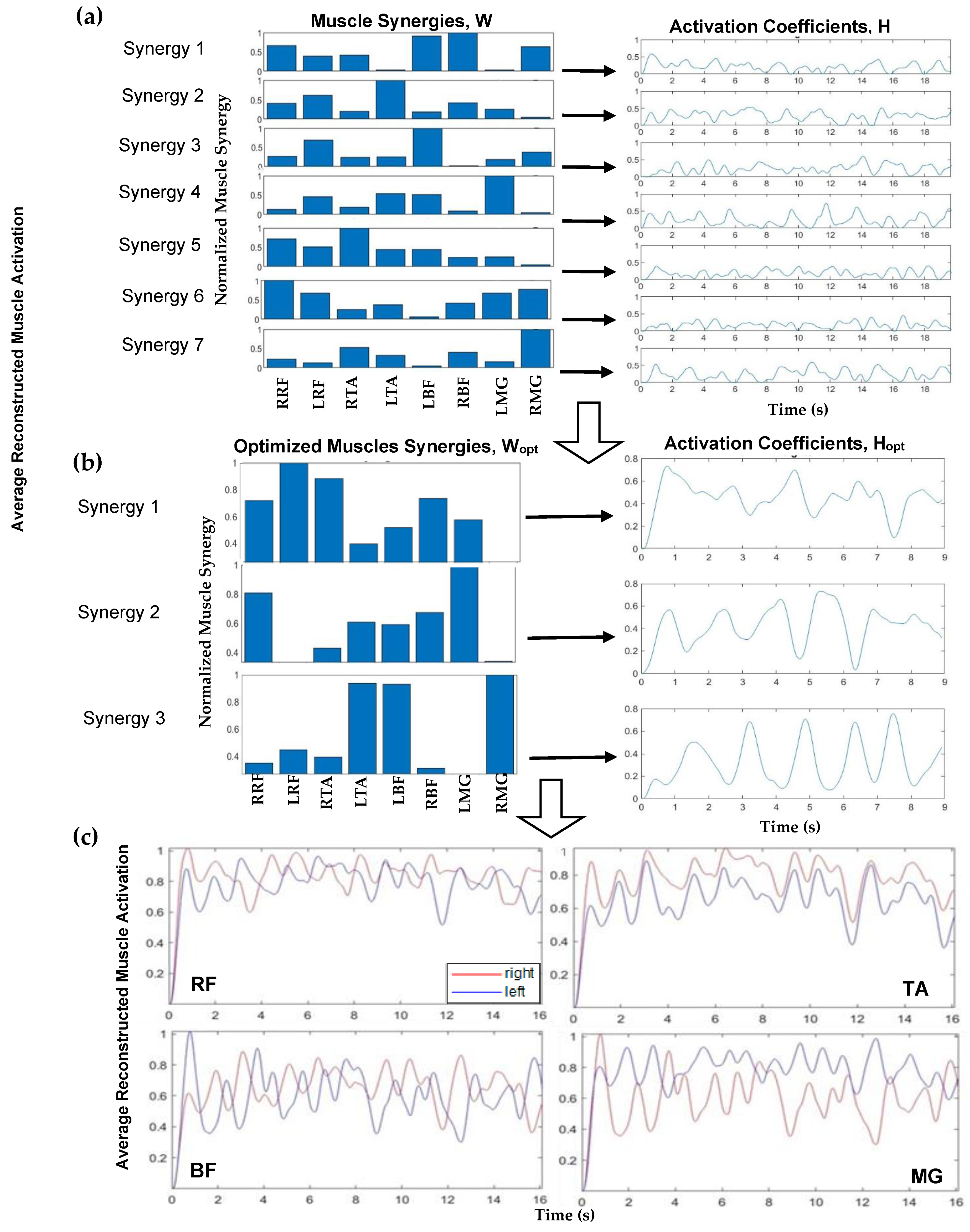
Figure 2.
Implementing NNMF began with using a search algorithm with MATLAB, starting with a set of muscle synergies (where
n is the number of muscle groups, and the max number of muscle synergies is
n − 1). The normalized synergy vectors and the corresponding weight coefficient were estimated using the MATLAB “nnmf()” function. For example, a schematic for one participant, FW pre-training, is shown in
Figure 2.
Figure 2a (left) displays muscle synergies represented for linear combination with the activation coefficients (
Figure 2a, right) corresponding to each muscle, prior to this iterative approach. An iterative approach, varying between 1 and 7 synergies, was used to determine the appropriate number of muscle synergies to reconstruct the EMG data. The >98% variability accounted for the (VAF) threshold with >90% confidence interval (CI) for each muscle data vector guided the computation to yield the number of optimum muscle synergies, W
opt, to represent and reconstruct the muscle activation data (
Figure 2c). Muscle synergy values at this threshold were deemed valid to reconstruct the data. For the 98% benchmark, for example, three components were considered applicable to reconstruct the data as seen (
Figure 2b). In this step, NNMF was further applied to the EMG data and reconstructed with three (optimal) muscle synergies (
Figure 2b, left) and activation coefficients (
Figure 2b, right). The reconstructed muscle responses are the resulting net activation of each muscle by all the muscle synergies recruited during each movement task (
Figure 2c). As an example, a comparison of actual muscle activation and reconstructed muscle activation using 98% VAF is shown in
Figure 3. A MATLAB code was generated to compute and plot the muscle synergy data over the average time it took to complete two gait cycles for each group (healthy or stroke) for each walking condition (FW, FT-W, BW, BT-W). Reconstructed synergies were computed for healthy and stroke participants for two gait cycles. When pooling results, if the participants completed two gait cycles in less or greater than the average time, the
interpol1 function in MATLAB was used to resample the synergies.
2.5. Statistical Analysis
Statistical analysis was performed using MATLAB. To obtain the differences between individual muscle synergies, the outliers and distribution of each synergy across participants of each walking condition were determined. Box plots were generated to examine medians, interquartile ranges, and outliers for each muscle group. Further, significance was determined by implementing the Kruskal–Wallis significance test; this test does not assume data are normally distributed. Optimizing the number of muscle synergies for fixed VAF also helped to identify the synergy with the highest variance. The first synergy for all sensors was utilized for the Kruskal–Wallis significance test function in MATLAB to obtain muscle activation p-values between pre- and post-training. Additionally, the Kruskal–Wallis test was implemented using RStudio software (RStudio Version 2023.12.1, Boston, MA, USA) to test for significant differences between the optimal number of muscle synergies for all groups and walking conditions, and pre vs. post p-values < 0.05 indicated significant differences. Cohen’s d, or the standardized mean difference, was implemented for the stroke participant group due to the small sample size. Cohen’s d specifically measures the effect size of the difference between two means.
4. Discussion
Here, we examined if changes in muscle synergies (e.g., number of synergies and muscle recruitment) could facilitate elucidation of how balance training interventions affect those at high fall risk (i.e., older adults that consider themselves overall healthy and those that have survived stroke). In order to direct goal-focused movements, such as overground walking, the central nervous system must map sensory inputs to motor output. Muscle synergies allow insights into how the muscles work together to execute a specific task. Here, the coordinated recruitment groups of specific leg muscles with specific activation balances and specific activation waveforms were observed. The flexible combination of a number of muscle synergies led to a simplified selection of the appropriate muscle commands for a given behavioral goal (overground walking in older adults).
Our study aimed to determine if muscle synergies could be used to quantify changes in high fall-risk groups (healthy older adults and older adults that had suffered a stroke) post-balance training. Within each group (healthy and stroke), muscle activations and muscle synergies were quantified, and some significant changes were observed. Previous studies have suggested that muscle synergy analysis indicates that changes in muscle activation patterns are due to the recruitment of fewer muscle synergies compared to healthy individuals [
1]; we observed this here in that we saw increases in muscle activation post-training with corresponding decreases (on average) for the number of muscle synergies. The number of muscle synergies lends insight into the complexity of neuromuscular control needed/required while performing a specific task (i.e., a lower number of synergies equates to a more simplified control strategy). Therefore, decreases in muscle synergies used to execute walking could indicate a better ability for the participants to perform a certain task.
There are some limitations that should be acknowledged in our study. Firstly, there was an imbalance in sample size between the healthy versus stroke participant groups, as well as in terms of female versus male participants. This may affect the overall generalizability of our findings. Further, we did not specify a requirement in terms of the type of stroke experienced by participants, just that participants that had suffered a stroke were at least 6 months post-stroke (i.e., in the chronic phase).
In previous research focused on ‘regular’ forward walking, a range of four to eight synergies that accounted for >80% of the variance had been reported by eleven studies [
1]. It had been observed that for undisturbed walking, muscle synergies ranged from 5–8 muscle synergies for roughly 91% VAF [
14]. When examining the whole gait cycle, seven synergies were observed for >80% VAF (the major muscles involved were the external obliques (EOBs)) [
22] and five synergies were observed for >90% VAF; (the major muscles involved were the medial gastrocnemius medialis (MG) and the biceps femoris (BF)) [
23]. In our study, we too observed for the healthy group that the right BF and the right MG showed significant increases in activation for FW and BW, and changes were observed post- compared to pre-training. For the stroke group, the right TA showed significant increases post-training for BT-W. Also, for the stroke group, the right BF (FT-W) and left MG (BW) also showed significant increases. Further, for the healthy group the right RF (quad muscle) showed significant increases post- compared to pre-training. It is important to note that in our study we used a tighter threshold than the aforementioned studies, with VAF set at 98%. This combined with measurements of only four muscles per leg (eight total) may have led to our differences in terms of number of muscle synergies observed. Further, the populations we examined here differed from previous studies in that we researched older adults including those that had suffered a stroke. A previous study was arranged for 6 months and found that the muscle synergy did not change but the muscle definition stability improved [
24]. Our study was for an approximately 6-week training cycle per participant. We were able to observe changes in the numbers of synergies, on average, pre- versus post-training for some of the walking conditions, and we did observe differences in synergies across the two groups. More specifically, we found a significant difference between the number of synergies post-BW and post-BW-T for both the healthy and the stroke groups, which highlights the challenges of completing these tasks as the number of synergies increase post- to pre-training.
Muscle analysis, in particular synergies, may thus offer the clinician a viewpoint of neural structure underlying motor behaviors [
25]. The possibility of diagnosis (i.e., use of synergies to allow quantification of changes in motor deficits and while undergoing rehabilitation) shows promise. Moreover, such information could inform diagnostic tools and evidence-based interventions for the aging population.




{kind=link}
{kind=link}
{kind=link}