
Learning Curve in Robotic-Assisted Total Knee Arthroplasty: A Systematic Review of the Literature

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Search Strategy
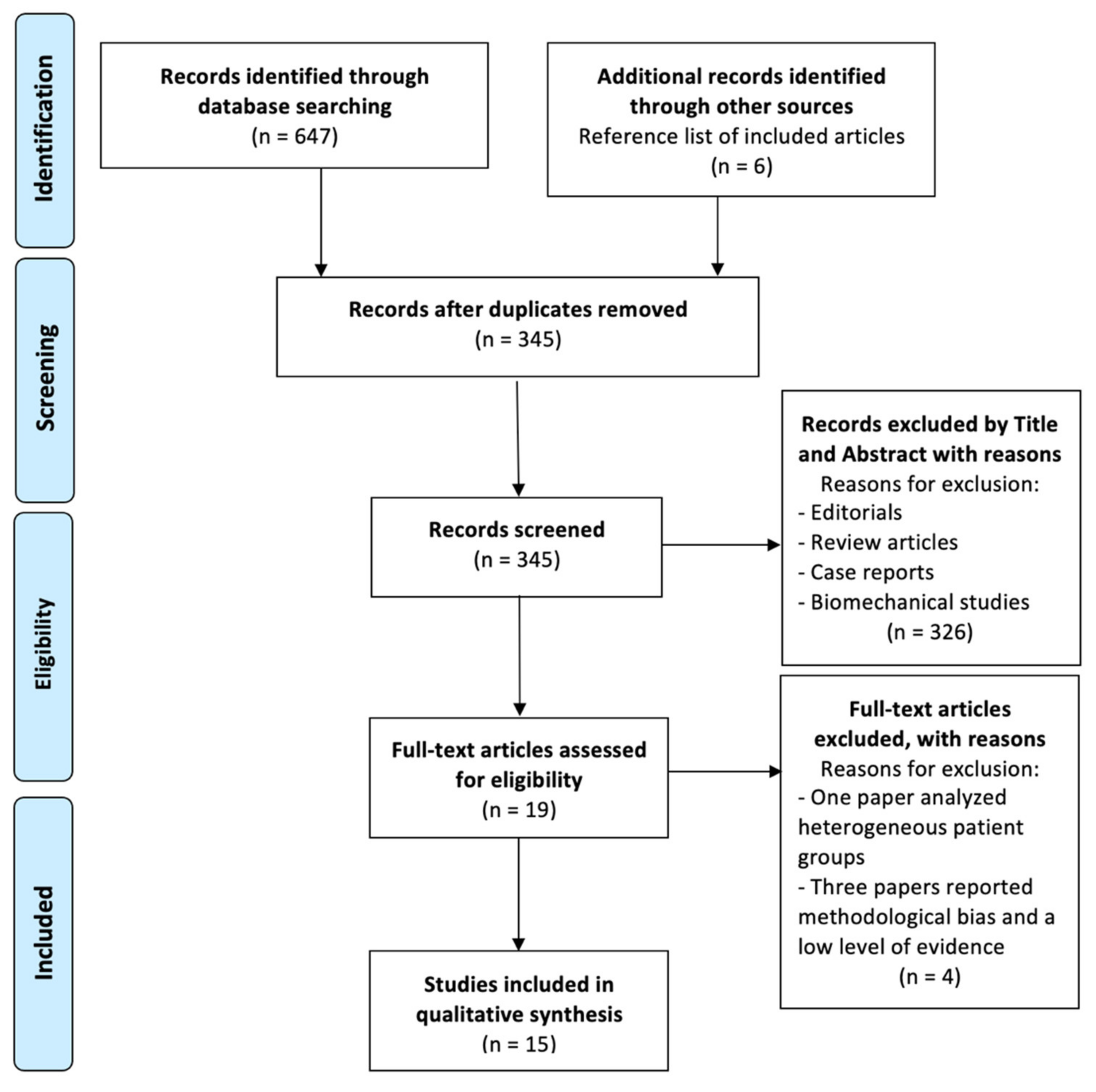
2.2. Study Screening
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction and Collection
2.5. Quality Assessment
3. Results
3.1. Demographic Characteristics and Surgical Data
3.2. Surgical Time
3.3. Lower Limb Alignment
3.4. Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| TKA | total knee arthroplasty |
| raTKA | robotic-assisted TKA |
| n | number |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| PROSPERO | International Prospective Register of Systematic Reviews |
| MINORS | Methodological Index for Non-Randomized Studies |
| LoE | levels of evidence |
| mTKA | manual TKA |
| MPTA | medial proximal tibial angle |
| LDFA | lateral distal femoral angle |
| HKA | hip–knee–ankle angle |
References
- Ayers, D.C.; Yousef, M.; Zheng, H.; Yang, W.; Franklin, P.D. The Prevalence and Predictors of Patient Dissatisfaction 5-years Following Primary Total Knee Arthroplasty. J. Arthroplast. 2022, 37, S121–S128. [Google Scholar] [CrossRef]
- Cacciola, G.; Mancino, F.; De Meo, F.; Di Matteo, V.; Sculco, P.K.; Cavaliere, P.; Maccauro, G.; De Martino, I. Mid-term survivorship and clinical outcomes of the medial stabilized systems in primary total knee arthroplasty: A systematic review. J. Orthop. 2021, 24, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.; Ong, K.; Lau, E.; Mowat, F.; Halpern, M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J. Bone Jt. Surg Am. 2007, 89, 780–785. [Google Scholar] [CrossRef]
- Cacciola, G.; De Martino, I.; De Meo, F. Does the medial pivot knee improve the clinical and radiographic outcome of total knee arthroplasty? A single centre study on two hundred and ninety seven patients. Int. Orthop. 2020, 44, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Quack, V.M.; Kathrein, S.; Rath, B.; Tingart, M.; Lüring, C. Computer-assisted navigation in total knee arthroplasty: A review of literature. Biomed. Tech. 2012, 57, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Risitano, S.; Cacciola, G.; Sabatini, L.; Capella, M.; Bosco, F.; Giustra, F.; Massè, A.; Vaishya, R. Restricted kinematic alignment in primary total knee arthroplasty: A systematic review of radiographic and clinical data. J. Orthop. 2022, 33, 37–43. [Google Scholar] [CrossRef]
- Laverdière, C.; Corban, J.; Khoury, J.; Ge, S.M.; Schupbach, J.; Harvey, E.J.; Reindl, R.; Martineau, P.A. Augmented reality in orthopaedics: A systematic review and a window on future possibilities. Bone Jt. J. 2019, 101-B, 1479–1488. [Google Scholar] [CrossRef]
- Mancino, F.; Rossi, S.; Sangaletti, R.; Lucenti, L.; Terragnoli, F.; Benazzo, F. A new robotically assisted technique can improve outcomes of total knee arthroplasty comparing to an imageless navigation system. Arch. Orthop. Trauma Surg 2022. epub ahead of print. [Google Scholar] [CrossRef]
- Sabatini, L.; Bosco, F.; Barberis, L.; Camazzola, D.; Bistolfi, A.; Risitano, S.; Massè, A.; Indelli, P.F. Kinetic Sensors for Ligament Balance and Kinematic Evaluation in Anatomic Bi-Cruciate Stabilized Total Knee Arthroplasty. Sensors 2021, 21, 5427. [Google Scholar] [CrossRef]
- Bistolfi, A.; Giustra, F.; Bosco, F.; Faccenda, C.; Viotto, M.; Sabatini, L.; Berchialla, P.; Sciannameo, V.; Graziano, E.; Massè, A. Comparable results between crosslinked polyethylene and conventional ultra-high molecular weight polyethylene implanted in total knee arthroplasty: Systematic review and meta-analysis of randomised clinical trials. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 3120–3130. [Google Scholar] [CrossRef]
- Bistolfi, A.; Giustra, F.; Bosco, F.; Sabatini, L.; Aprato, A.; Bracco, P.; Bellare, A. Ultra-high molecular weight polyethylene (UHMWPE) for hip and knee arthroplasty: The present and the future. J. Orthop. 2021, 25, 98–106. [Google Scholar] [CrossRef]
- Fujie, M.G.; Zhang, B. State-of-the-art of intelligent minimally invasive surgical robots. Front. Med. 2020, 14, 404–416. [Google Scholar] [CrossRef]
- Rossi, S.; Sangaletti, R.; Perticarini, L.; Terragnoli, F.; Benazzo, F. High accuracy of a new robotically assisted technique for total knee arthroplasty: An in vivo study. Knee Surg. Sports Traumatol. Arthrosc. 2022, 4, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Mancino, F.; Cacciola, G.; Malahias, M.-A.; De Filippis, R.; De Marco, D.; Di Matteo, V.; Gu, A.; Sculco, P.K.; Maccauro, G.; De Martino, I. What are the benefits of robotic-assisted total knee arthroplasty over conventional manual total knee arthroplasty? A systematic review of comparative studies. Orthop. Rev. 2020, 12, 8657. [Google Scholar] [CrossRef] [PubMed]
- Goyal, T.; Choudhury, A.K.; Paul, S.; Das, L.; Gupta, T. The direct anterior approach without traction table: How does it compare with the posterior approach?—A prospective non-randomised trial. J. Clin. Orthop. Trauma 2022, 31, 101924. [Google Scholar] [CrossRef] [PubMed]
- Hopper, A.N.; Jamison, M.H.; Lewis, W.G. Learning curves in surgical practice. Postgrad Med. J. 2007, 83, 777–779. [Google Scholar] [CrossRef] [PubMed]
- Yotsumoto, F.; Sanui, A.; Ito, T.; Miyahara, D.; Yoshikawa, K.; Shigekawa, K.; Noguchi, Y.; Yasunaga, S.; Miyamoto, S. Cumulative Summation Analysis of Learning Curve for Robotic-assisted Hysterectomy in Patients With Gynecologic Tumors. Anticancer Res. 2022, 42, 4111–4117. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Sideri, S.; Papageorgiou, S.N.; Eliades, T. Registration in the international prospective register of systematic reviews (PROSPERO) of systematic review protocols was associated with increased review quality. J. Clin. Epidemiol. 2018, 100, 103–110. [Google Scholar] [CrossRef]
- Giai Via, R.; Bosco, F.; Giustra, F.; Lavia, A.D.; Artiaco, S.; Risitano, S.; Giachino, M.; Massè, A. Acute Rockwood type III ACJ dislocation: Conservative vs surgical approach. A systematic review and meta-analysis of current concepts in literature. Injury 2022, 53, 3094–3101. [Google Scholar] [CrossRef]
- Schopper, C.; Proier, P.; Luger, M.; Gotterbarm, T.; Klasan, A. The learning curve in robotic assisted knee arthroplasty is flattened by the presence of a surgeon experienced with robotic assisted surgery. Knee Surg. Sports Traumatol. Arthrosc. 2022. epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.; Judd, H.; Harm, R.G.; Nolan, J.R.; Hummel, M.; Spanyer, J. Robotic-assisted total knee arthroplasty: Is there a maximum level of efficiency for the operating surgeon? J Orthop. 2022, 31, 13–16. [Google Scholar] [CrossRef] [PubMed]
- Vanlommel, L.; Neven, E.; Anderson, M.B.; Bruckers, L.; Truijen, J. The initial learning curve for the ROSA® Knee System can be achieved in 6-11 cases for operative time and has similar 90-day complication rates with improved implant alignment compared to manual instrumentation in total knee arthroplasty. J. Exp. Orthop. 2021, 8, 119. [Google Scholar] [CrossRef]
- Thiengwittayaporn, S.; Uthaitas, P.; Senwiruch, C.; Hongku, N.; Tunyasuwanakul, R. Imageless robotic-assisted total knee arthroplasty accurately restores the radiological alignment with a short learning curve: A randomized controlled trial. Int. Orthop. 2021, 45, 2851–2858. [Google Scholar] [CrossRef] [PubMed]
- Savov, P.; Tuecking, L.R.; Windhagen, H.; Ehmig, J.; Ettinger, M. Imageless robotic handpiece-assisted total knee arthroplasty: A learning curve analysis of surgical time and alignment accuracy. Arch. Orthop. Trauma Surg. 2021, 141, 2119–2128. [Google Scholar] [CrossRef]
- Mahure, S.A.; Teo, G.M.; Kissin, Y.D.; Stulberg, B.N.; Kreuzer, S.; Long, W.J. Learning curve for active robotic total knee arthroplasty. Knee Surg Sports Traumatol. Arthrosc. 2022, 30, 2666–2676. [Google Scholar] [CrossRef]
- Bell, C.; Grau, L.; Orozco, F.; Ponzio, D.; Post, Z.; Czymek, M.; Ong, A. The successful implementation of the Navio robotic technology required 29 cases. J. Robot Surg. 2022, 16, 495–499. [Google Scholar] [CrossRef]
- Ali, M.; Phillips, D.; Kamson, A.; Nivar, I.; Dahl, R.; Hallock, R. Learning Curve of Robotic-Assisted Total Knee Arthroplasty for Non-Fellowship-Trained Orthopedic Surgeons. Arthroplast. Today 2022, 13, 194–198. [Google Scholar] [CrossRef]
- Vermue, H.; Luyckx, T.; Winnock de Grave, P.; Ryckaert, A.; Cools, A.S.; Himpe, N.; Victor, J. Robot-assisted total knee arthroplasty is associated with a learning curve for surgical time but not for component alignment, limb alignment and gap balancing. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 593–602. [Google Scholar] [CrossRef]
- King, C.A.; Jordan, M.; Bradley, A.T.; Wlodarski, C.; Tauchen, A.; Puri, L. Transitioning a Practice to Robotic Total Knee Arthroplasty Is Correlated with Favorable Short-Term Clinical Outcomes-A Single Surgeon Experience. J. Knee Surg. 2022, 35, 78–82. [Google Scholar] [CrossRef]
- Collins, K.; Agius, P.A.; Fraval, A.; Petterwood, J. Initial Experience with the NAVIO Robotic-Assisted Total Knee Replacement-Coronal Alignment Accuracy and the Learning Curve. J. Knee Surg. 2021, 35, 1295–1300. [Google Scholar] [CrossRef] [PubMed]
- Naziri, Q.; Cusson, B.C.; Chaudhri, M.; Shah, N.V.; Sastry, A. Making the transition from traditional to robotic-arm assisted TKA: What to expect? A single-surgeon comparative-analysis of the first-40 consecutive cases. J. Orthop. 2019, 16, 364–368. [Google Scholar] [CrossRef] [PubMed]
- Kayani, B.; Konan, S.; Huq, S.S.; Tahmassebi, J.; Haddad, F.S. Robotic-arm assisted total knee arthroplasty has a learning curve of seven cases for integration into the surgical workflow but no learning curve effect for accuracy of implant positioning. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 1132–1141. [Google Scholar] [CrossRef] [PubMed]
- Grau, L.; Lingamfelter, M.; Ponzio, D.; Post, Z.; Ong, A.; Le, D.; Orozco, F. Robotic arm assisted total knee arthroplasty workflow optimization, operative times and learning curve. Arthroplast. Today 2019, 5, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Sodhi, N.; Khlopas, A.; Piuzzi, N.S.; Sultan, A.A.; Marchand, R.C.; Malkani, A.L.; Mont, M.A. The Learning Curve Associated with Robotic Total Knee Arthroplasty. J. Knee Surg. 2018, 31, 17–21. [Google Scholar] [CrossRef]
- Burns, P.B.; Rohrich, R.J.; Chung, K.C. The levels of evidence and their role in evidence-based medicine. Plast Reconstr. Surg. 2011, 128, 305–310. [Google Scholar] [CrossRef]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Lopez, I.B.; Benzakour, A.; Mavrogenis, A.; Benzakour, T.; Ahmad, A.; Lemée, J.M. Robotics in spine surgery: Systematic review of literature. Int. Orthop. 2022. epub ahead of print. [Google Scholar] [CrossRef]
- Mancino, F.; Cacciola, G.; Di Matteo, V.; Perna, A.; Proietti, L.; Greenberg, A.; Ma, M.; Sculco, P.K.; Maccauro, G.; De Martino, I. Surgical implications of the hip-spine relationship in total hip arthroplasty. Orthop. Rev. 2020, 12 (Suppl. S1), 8656. [Google Scholar] [CrossRef]
- Mullaji, A.B.; Khalifa, A.A. Is it prime time for robotic-assisted TKAs? A systematic review of current studies. Journal of orthopaedics. J. Orthop. 2022, 34, 31–39. [Google Scholar] [CrossRef]
- Cacciola, G.; De Meo, F.; Cavaliere, P. Mechanical and elution properties of G3 Low Viscosity bone cement loaded up to three antibiotics. J. Orthop. 2018, 15, 1004–1007. [Google Scholar] [CrossRef] [PubMed]
- Kreuzer, S.; Brar, A.; Campanelli, V. Dimensional accuracy of TKA cut surfaces with an active robotic system. Comput. Assist Surg. 2022, 27, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Ueno, J.; Torii, Y.; Umehra, T.; Iinuma, M.; Yoshida, A.; Tomochika, K.; Niki, H.; Akazawa, T. Robotics is useful for less-experienced surgeons in spinal deformity surgery. Eur. J. Orthop. Surg. Traumatol 2022. epub ahead of print. [Google Scholar] [CrossRef]
- Scott, C.E.; Howie, C.R.; MacDonald, D.; Biant, L.C. Predicting dissatisfaction following total knee replacement: A prospective study of 1217 patients. J. Bone Jt. Surg. Br. 2010, 92, 1253–1258. [Google Scholar] [CrossRef] [PubMed]
- Muertizha, M.; Cai, X.; Ji, B.; Aimaiti, A.; Cao, L. Factors contributing to 1-year dissatisfaction after total knee arthroplasty: A nomogram prediction model. J. Orthop. Surg. Res. 2022, 17, 367. [Google Scholar] [CrossRef] [PubMed]
- Parsley, B.S. Robotics in Orthopedics: A Brave New World. J. Arthroplast. 2018, 33, 2355–2357. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author and Publication Year | LoE | Study Design | raTKA | mTKA | Surgeons N° | Expertise | Age Mean (y.o.) | M/F | BMI Mean (kg/m2) | Minors Score |
|---|---|---|---|---|---|---|---|---|---|---|
| Schopper et al. (2022) [21] | III | Prospective | Mako (Stryker) | Triathlon (Stryker) | 3 | 1 experienced surgeon, 2 non-experienced | 71 | 37/18 | 30.8 | 12 |
| Patel et al. (2022) [22] | IV | Retrospective | Mako (Stryker) | Triathlon (Stryker) | 1 | 1 fellowship-trained surgeon | 64.2 | 353/251 | 33 | 6 |
| Vanlommel et al. (2021) [23] | IV | Retrospective | ROSA (Zimmer) | Persona PS (Zimmer) | 3 | 3 high volume surgeons | 68.7 | 46/44 | 31.3 | 9 |
| Thiengwittayaporn et al. (2021) [24] | III | RCT | Navio (Smith & Nephew) | Legion (Smith & nephew) | 1 | 1 senior surgeon | 69 | giu-69 | 28 | 13 |
| Savov et al. (2021) [25] | III | Prospective | Navio (Smith & Nephew) | Journey II (Smith & Nephew) | 1 | 1 senior surgeon | 64.4 | 22/48 | 28.8 | 14 |
| Mahure et al. (2021) [26] | II | Prospective | Think Surgical | Persona PS (Zimmer), Corin CR, and PS (Unity Knee) | 4 | 4 fellowship-trained recon surgeons | 65.9 | 58/57 | 30.7 | 11 |
| Bell et al. (2021) [27] | III | Prospective | Navio (Smith & Nephew) | Journey II (Smith & Nephew) | 1 | 1 fellowship-trained surgeon | N/A | N/A | N/A | 17 |
| Ali et al. (2021) [28] | IV | Retrospective | Mako (Stryker) | N/A | 2 | 2 non-fellowship surgeons | 66.1 | 50/70 | 33.5 | 13 |
| Vermue et al. (2020) [29] | IV | Retrospective | Mako (Stryker) | Triathlon (Stryker) | 6 | 2 low volume, 1 medium volume, and 3 high volume surgeons | 70.4 | 252/134 | 30 | 18 |
| King et al. (2020) [30] | IV | Retrospective | Mako (Stryker) | Triathlon (Stryker) | 1 | 1 senior surgeon | 68 | 71/131 | N/A | 14 |
| Collins et al. (2020) [31] | IV | Retrospective | Navio (Smith & Nephew) | Legion (Smith & nephew) | 1 | 1 senior surgeon | 67 | 36/36 | N/A | 6 |
| Naziri et al. (2019) [32] | IV | Retrospective | Mako (Stryker) | Triathlon (Stryker) | 1 | 1 fellowship-trained surgeon | 69.5 | 16/24 | 29.1 | 9 |
| Kayani et al. (2018) [33] | II | Prospective | Mako (Stryker) | Triathlon (Stryker) | 1 | N/A | 68.7 | 27/33 | 26.1 | 17 |
| Garau et al. (2019) [34] | III | Prospective | Mako (Stryker) | N/A | 1 | 1 senior surgeon | N/A | N/A | N/A | 12 |
| Sodhi et al. (2018) [35] | III | Retrospective | Mako (Stryker) | N/A | 2 | 2 lower limb certified surgeons | N/A | N/A | N/A | 6 |
| Author and Publication Year | raTKA N° | Inflection Point | Learning Phase Mean Surgical Time (min) | Proficiency Phase Mean Surgical Time (min) | p-Value | Improvement in Surgical Time between the First and Last Cases of raTKA | Improvement in Surgical Time of raTKA Compared to mTKA |
|---|---|---|---|---|---|---|---|
| Schopper et al. (2022) [21] | 55 | No inflection for two surgeons; after 5 cases for the third surgeon | N/A | N/A | N/A | N/A | N/A |
| Patel et al. (2022) [22] | 604 | Reached within the first 200 cases | N/A | N/A | N/A | Significant improvement (p < 0.05) between the first and last cases (84.9 min vs. 62 min) | N/A |
| Vanlommel et al. (2021) [23] | 90 | After 10, 6, and 11 cases, respectively, for the three surgeons | 102.4 | 86.5 | <0.05 | The average surgical time of the first cases was significantly higher than the last cases | N/A |
| Thiengwittayaporn et al. (2021) [24] | 75 | After 7 cases | 100.7 | 67.4 | <0.05 | Significant decrease in mean surgical time between the first and last cases (49.1 min vs. 36.5 min) | The mean surgical time of all raTKA was significantly longer than that of mTKA |
| Savov et al. (2021) [25] | 59 | After 11 cases | No difference in average surgical time before and after the inflection point | N/A | N/A | N/A | |
| Mahure et al. (2021) [26] | 107 | No inflection points for one surgeon. After 12, 16, and 19, respectively, for the remaining 3 surgeons | N/A | N/A | N/A | N/A | N/A |
| Bell et al. (2021) [27] | 58 | After 29 cases | N/A | N/A | N/A | Significant decrease in mean surgical time between the first and last cases (41.8 min vs. 31.1 min). | N/A |
| Ali et al. (2021) [28] | 120 | N/A | N/A | N/A | N/A | A significant decrease between the first and last cases was reported for one surgeon, but no difference for the second surgeon | N/A |
| Vermue et al. (2020) [29] | 386 | After 11, 22, and 43 cases for high-volume surgeons. No inflection points for medium and low-volume surgeons. | Statistically significant lower time for high-volume surgeons during the proficiency phase compared to the learning phase | N/A | N/A | The mean surgical time in raTKA compared to mTKA was longer for the first 10 cases. No differences were reported between the last cases of raTKA and mTKA | |
| Kayani et al. (2018) [33] | 60 | After 7 cases | 89.2 | N/A | <0.05 | N/A | N/A |
| Garau et al. (2019) [34] | 132 | Reached within the first 40 cases | N/A | N/A | N/A | The average surgical time in the first cases was higher than in the last cases | For one surgeon, all patients treated with raTKA showed higher mean surgical times than mTKA. For the second surgeon, the mean surgical time was significantly higher for the first 20 cases only |
| Sodhi et al. (2018) [35] | 240 | N/A | N/A | N/A | N/A | The average surgical time for both surgeons was higher in the first group of patients than in the later groups | The average surgical time for the first cases was higher than for mTKA, but no difference was noted for the last cases |
| Naziri et al. (2019) [32] | 40 | N/A | N/A | N/A | N/A | N/A | The mean surgical time for all raTKA was significantly higher (p < 0.05) than for mTKA. No difference in mean surgical time was reported from the last 20 cases of raTKA and mTKA |
| Author and Publication Year | raTKA N° | Implant Position | Intraoperative and Postoperative Measurements | Coronal and Sagittal Alignment | Outliers > 3° |
|---|---|---|---|---|---|
| Schopper et al. (2022) [21] | 55 | High percentage of outliers in mTKA compared to raTKA after reaching the inflection point | No difference between intraoperative and postoperative measurements | N/A | No outliers >3° (mean angles analyzed within 1°) |
| Thiengwittayaporn et al. (2021) [24] | 75 | N/A | N/A | raTKA improved the postoperative mechanical axis accuracy, sagittal alignment of the femur, and coronal alignment of the tibia | Fewer outliers for HKA, coronal femoral angle, coronal tibial angle, sagittal femoral angle, and sagittal tibial angle in raTKA compared to mTKA |
| Savov et al. (2021) [25] | 59 | The learning curve was not associated with implant position after reaching the inflection point | Significant differences between intraoperative and postoperative measurements (MPTA accurate to 1°, LDFA to 1.6°, and HKA to 2°). | N/A | 5.5% outliers with raTKA on coronal alignment |
| Mahure et al. (2021) [26] | 107 | The learning curve was not associated with implant position after reaching the inflection point | N/A | N/A | Higher outliers for raTKA (43%) than for mTKA (32%) |
| Vermue et al. (2020) [29] | 386 | The learning curve was not associated with implant position after reaching the inflection point | The mean postoperative HKA was 1.2° more valgus than that measured intraoperatively | N/A | N/A |
| Kayani et al. (2018) [33] | 60 | The learning curve was not associated with implant position after reaching the inflection point | N/A | raTKA improved postoperative mechanical axis accuracy, posterior tibial slope, coronal and sagittal alignment of the femur, and coronal and sagittal alignment of the tibia. | N/A |
| Naziri et al. (2019) [32] | 40 | N/A | N/A | No difference in lower limb alignment between raTKA and mTKA | No outliers in both groups |
| Collins et al. (2020) [31] | 72 | N/A | N/A | N/A | 6.9% outliers in coronal plane alignment |
| Author and Publication Year | raTKA N° | Learning/Proficiency Phase N° | Complications Related to raTKA N° | Complications Not Related to raTKA N° |
|---|---|---|---|---|
| Schopper et al. (2022) [21] | 55 | N/A | N/A | 1 open patellar tendon rupture, 1 post-traumatic wound dehiscence |
| Mahure et al. (2022) [26] | 107 | N/A | 1 Metallic tack left to the distal femur | N/A |
| Vermue et al. (2022) [29] | 386 | N/A | 1 Diaphyseal femoral stress fracture at pin insertion | N/A |
| Kayani et al. (2019) [33] | 60 | N/A | 1 wound dehiscence at pin insertion | N/A |
| Vanlommel et al. (2021) [23] | 90 | One complication during the learning phase (1 arthrofibrosis). Three complications after reaching the proficiency phase (1 arthrofibrosis, 1 surgical site infection, 1 deep vein thrombosis). | 0 | 2 arthrofibrosis, 1 surgical site infection, 1 deep vein thrombosis |
| Patel et al. (2022) [22] | 604 | N/A | N/A | N/A |
| Bell et al. (2022) [27] | 58 | N/A | 0 | N/A |
| Naziri et al. [32] | 40 | N/A | 0 | N/A |
| King et al. [30] | 202 | N/A | 0 | N/A |
| Ali et al. [28] | 120 | N/A | N/A | 2 arthrofibrosis, 1 cellulitis, 1 acute kidney injury, 1 congestive heart failure |
| Collins et al. [31] | 72 | N/A | N/A | 2 arthrofibrosis, 1 intraoperative tibial periprosthetic fracture, 1 fatal pulmonary embolism |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cacciola, G.; Bosco, F.; Giustra, F.; Risitano, S.; Capella, M.; Bistolfi, A.; Massè, A.; Sabatini, L. Learning Curve in Robotic-Assisted Total Knee Arthroplasty: A Systematic Review of the Literature. Appl. Sci. 2022, 12, 11085. https://doi.org/10.3390/app122111085
Cacciola G, Bosco F, Giustra F, Risitano S, Capella M, Bistolfi A, Massè A, Sabatini L. Learning Curve in Robotic-Assisted Total Knee Arthroplasty: A Systematic Review of the Literature. Applied Sciences. 2022; 12(21):11085. https://doi.org/10.3390/app122111085
Chicago/Turabian StyleCacciola, Giorgio, Francesco Bosco, Fortunato Giustra, Salvatore Risitano, Marcello Capella, Alessandro Bistolfi, Alessandro Massè, and Luigi Sabatini. 2022. "Learning Curve in Robotic-Assisted Total Knee Arthroplasty: A Systematic Review of the Literature" Applied Sciences 12, no. 21: 11085. https://doi.org/10.3390/app122111085
APA StyleCacciola, G., Bosco, F., Giustra, F., Risitano, S., Capella, M., Bistolfi, A., Massè, A., & Sabatini, L. (2022). Learning Curve in Robotic-Assisted Total Knee Arthroplasty: A Systematic Review of the Literature. Applied Sciences, 12(21), 11085. https://doi.org/10.3390/app122111085