Different Resorptive Patterns of Two Avulsed and Replanted Upper Central Incisors Based on Scanning Electron Microscopy and Stereomicroscopic Analysis: A Case Report


 ,
,  , and
, and 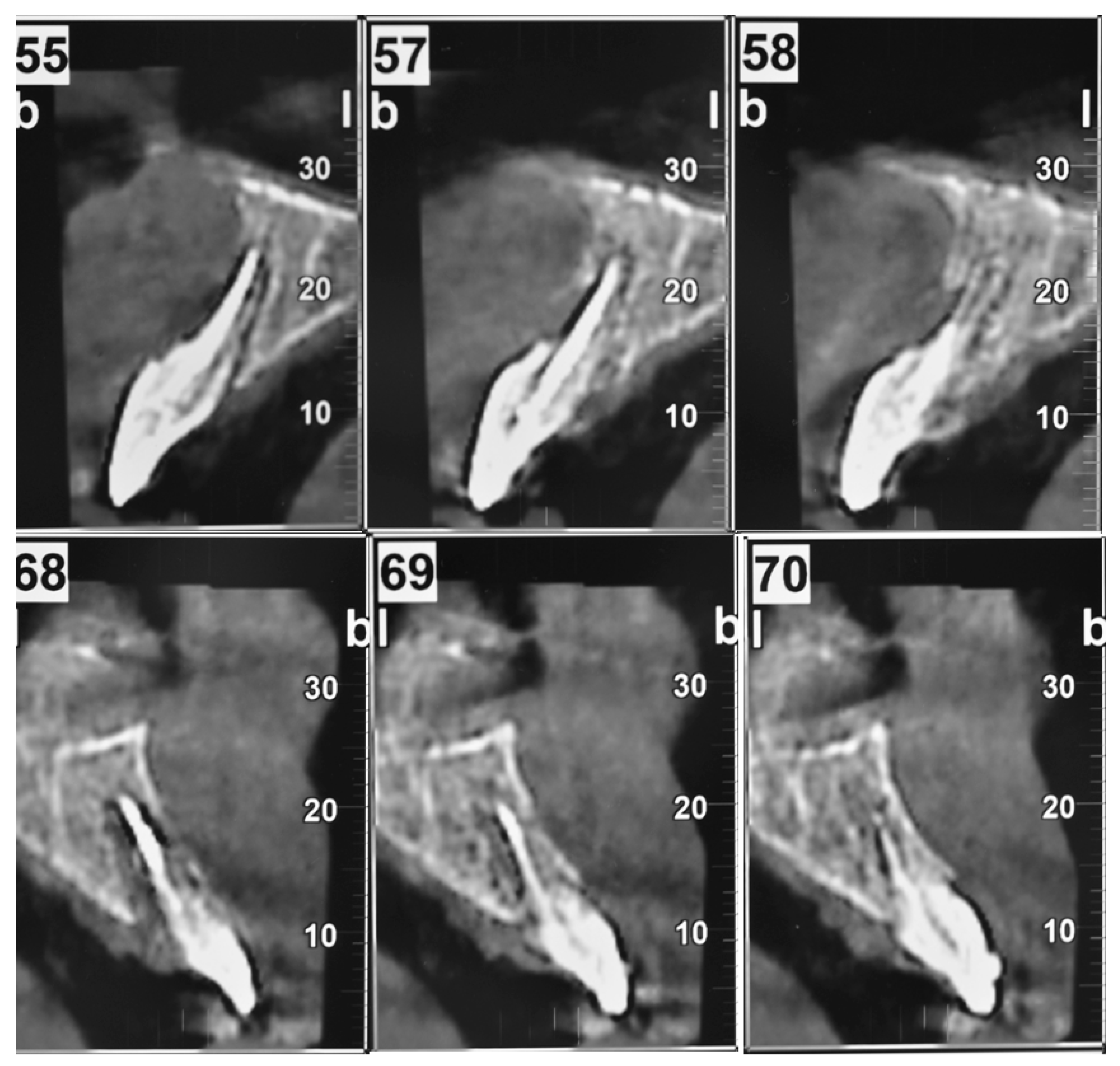{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Case Presentation
Stereomicroscopy and SEM Images
- i.
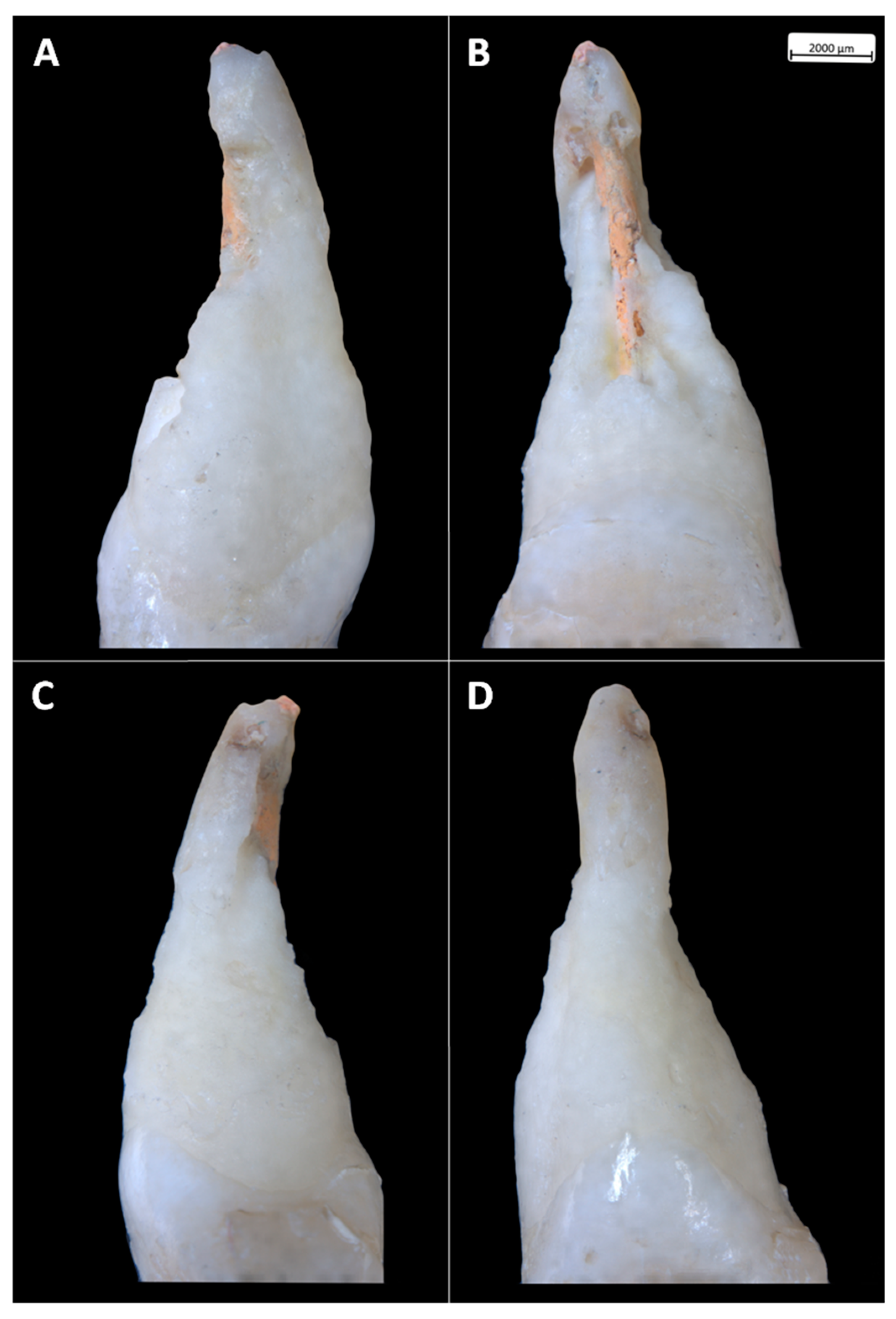
- Tooth 21 experienced a heterogeneous root resorption, with the dentine lacunae extending more mesially and distally when compared to tooth 11 (Figure 3A,C);
- ii.
- The most apical portion of the root is almost preserved in tooth 11, while it is missing in tooth 21 as a consequence of the dentine resorption and the breakage of the gutta-percha filling;
- iii.
- iv.
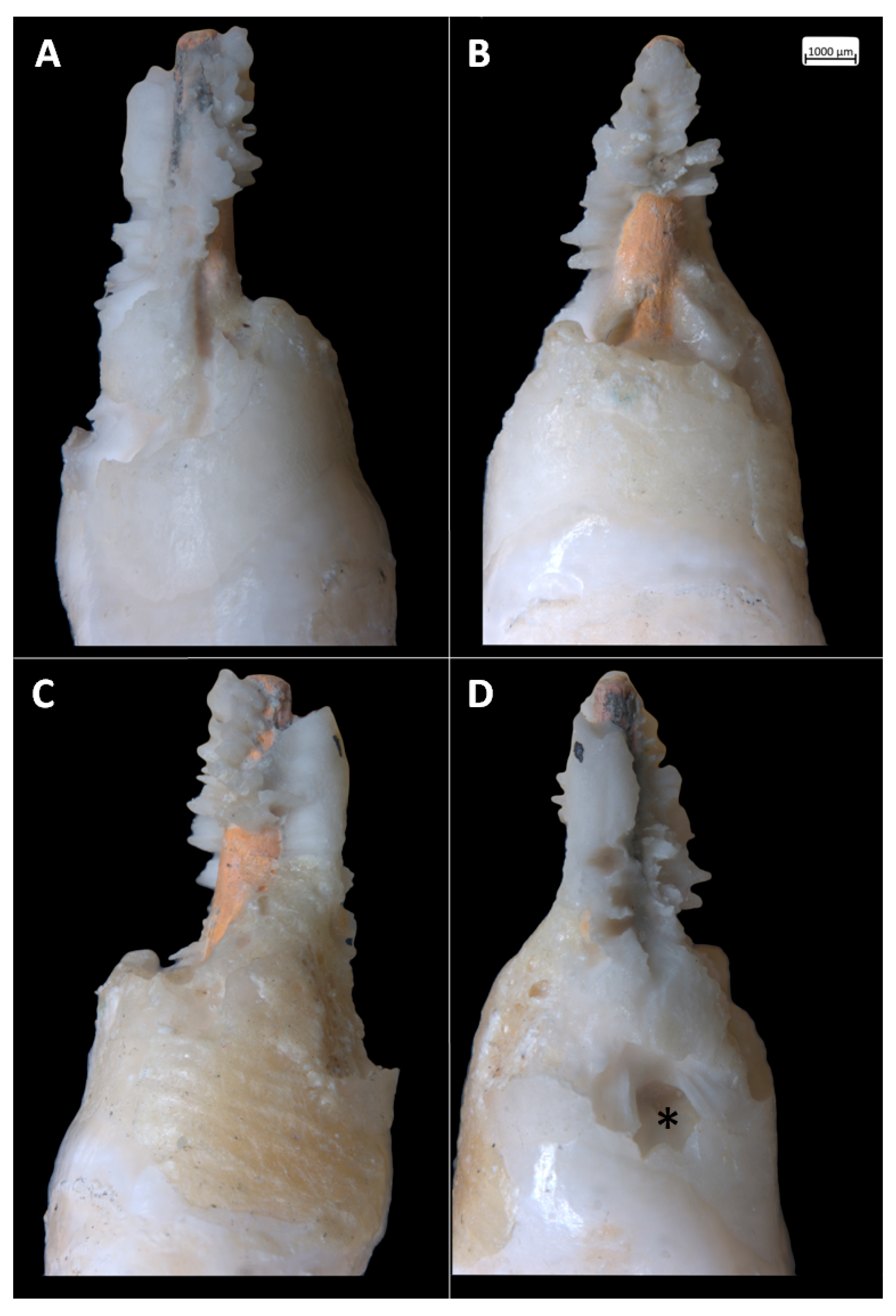
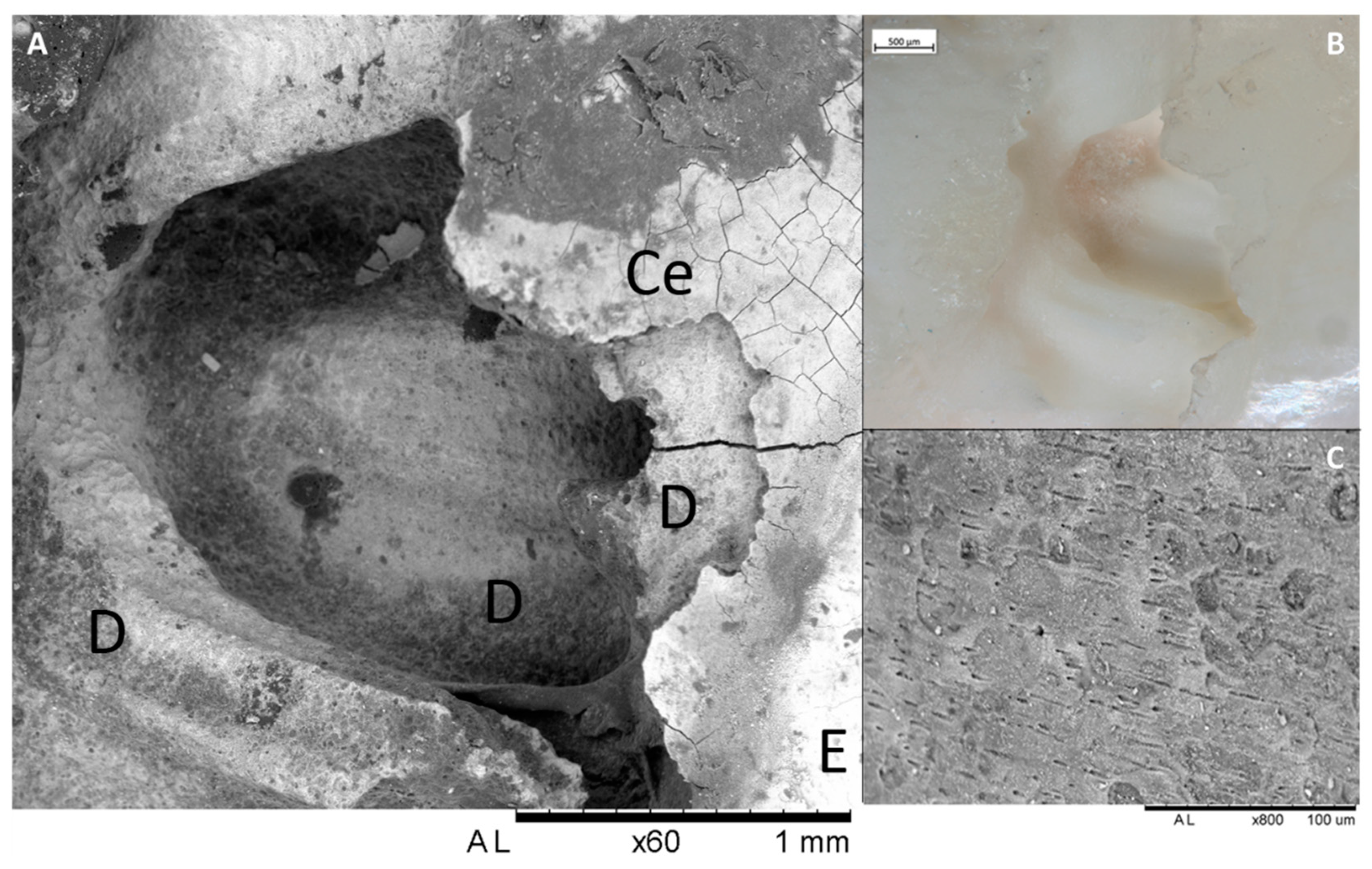
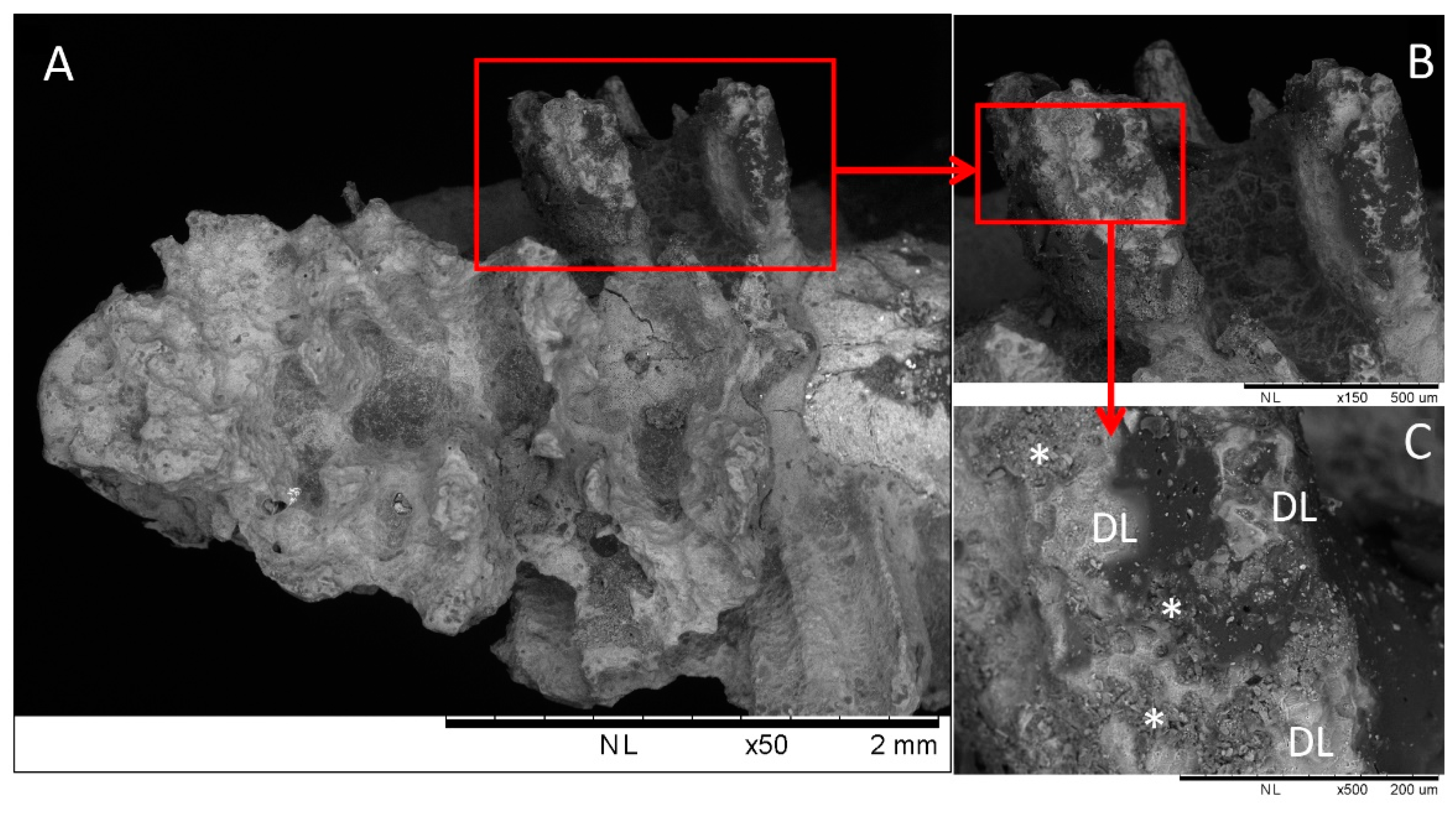
- The resorptive pattern characterizing the root of the tooth 21 shows high heterogeneity (Figure 5). In this tooth, the external replacement resorption invaded the root by resorbing all the cementum and, irregularly, the dentine, that assumed a spurs appearance (Figure 5A,B). At higher magnifications (Figure 5C), these spurs are characterized by the presence of resorptive dentine lacunae and by the presence of treatment agents used by the dental practitioner before replantation. The dentine at the base of the spurs and at higher magnification (Figure 6) shows the same resorptive lacunae with dentine tubules surrounded by a hypermineralized collar of peritubular dentine;
- v.
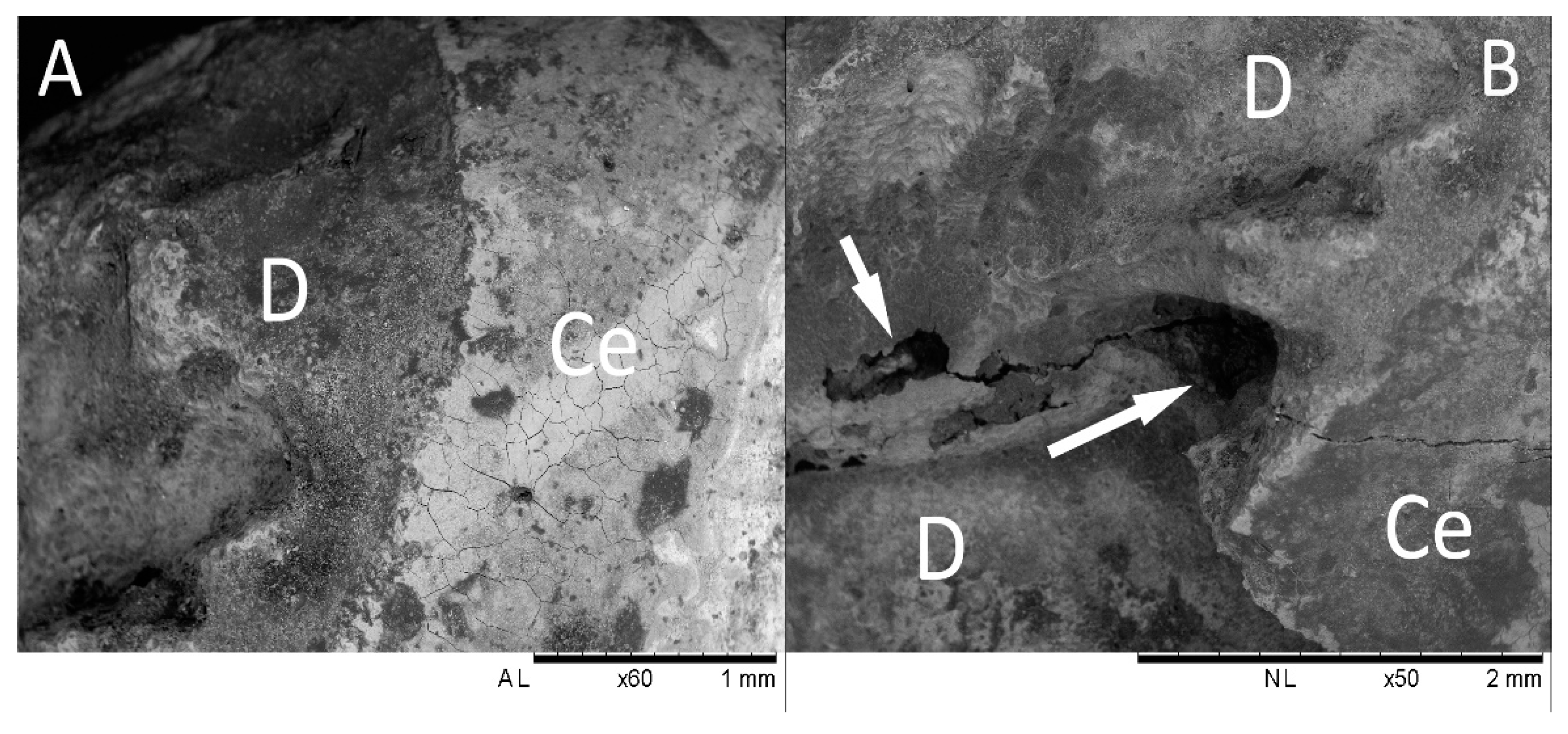
- The microscopic structure of tooth 11 (Figure 7) is characterized by the same pattern of resorptive dentine lacunae as tooth 21 and by the same appearance of the dentine tubules (i.e., surrounded by a hypermineralized collar of peritubular dentine). Differently from tooth 21, here the cement preserves in some areas, preventing the resorptive reaction.
3. Discussion and Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethical approval
Informed consent
References
- Azami-Aghdash, S.; Azar, F.E.; Azar, F.P.; Rezapour, A.; Moradi-Joo, M.; Moosavi, A.; Oskouei, S.G. Prevalence, etiology, and types of dental trauma in children and adolescents: Systematic review and meta-analysis. Med. J. Islam Repub Iran. 2015, 29, 234. [Google Scholar] [PubMed]
- Lam, R. Epidemiology and outcomes of traumatic dental injuries: A review of the literature. Aust. Dent. J. 2016, 61, 4–20. [Google Scholar] [CrossRef] [PubMed]
- Andersson, L.; Andreasen, J.O.; Day, P.; Heithersay, G.; Trope, M.; DiAngelis, A.J.; Kenny, D.J.; Sigurdsson, A.; Bourguignon, C.; Flores, M.T. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 2. Avulsion of permanent teeth. Dent. Traumatol. 2012, 2, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Panzarini, S.R.; Gulinelli, J.L.; Poi, W.R.; Sonoda, C.K.; Pedrini, D.; Brandini, D.A. Treatment of root surface in delayed tooth replantation: A review of literature. Dent. Traumatol. 2008, 24, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, M.; Kinirons, M. Factors affecting the time of onset of resorption in avulsed and replanted incisor teeth in children. Dent. Traumatol. 2001, 17, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Petrovic, B.; Marković, D.; Peric, T.; Blagojevic, D. Factors related to treatment and outcomes of avulsed teeth. Dent. Traumatol. 2010, 26, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Souza, B.D.M.; Dutra, K.L.; Kuntze, M.M.; Bortoluzzi, E.A.; Flores-Mir, C.; Reyes-Carmona, J.; Felippe, W.T.; Porporatti, A.L.; De Luca Canto, G. Incidence of Root Resorption after the Replantation of Avulsed Teeth: A Meta-analysis. J. Endod. 2018, 44, 1216–1227. [Google Scholar] [CrossRef] [PubMed]
- Brignardello-Petersen, R. There is probably high variability in the incidence of root resorption after replantation of avulsed teeth across and within types of teeth and resorption. J. Am. Dent. Assoc 2019, 150, e15. [Google Scholar] [CrossRef] [PubMed]
- Bastos, J.V.; de SouzaCôrtes, M.I.; Goulart, E.M.A.; Colosimo, E.A.; Gomez, R.S.; Dutra, W.O. Age and timing of pulp extirpation as major factors associated with inflammatory root resorption in replanted permanent teeth. J. Endod. 2014, 40, 366–371. [Google Scholar] [CrossRef] [PubMed]
- Trope, M. Clinical management of the avulsed tooth: Present strategies and future directions. Dent. Traumatol. 2002, 18, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Blomlöf, L.; Lindskog, S.; Andersson, L.; Hedström, K.G.; Hammarström, L. Storage of experimentally avulsed teeth in milk prior to replantation. J. Dent. Res. 1983, 62, 912–916. [Google Scholar]
- Andersson, L.; Bodin, I.; Sorensen, S. Progression of root resorption following replantation of human teeth after extended extraoral storage. Dent. Traumatol. 1989, 5, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Mavridou, A.M.; Hauben, E.; Wevers, M.; Schepers, E.; Bergmans, L.; Lambrechts, P. Understanding external cervical resorption patterns in endodontically treated teeth. Int. Endod. J. 2017, 50, 1116–1133. [Google Scholar] [CrossRef] [PubMed]
- Tsukiboshi, M.; Tsukiboshi, T. Bone morphology after delayed tooth replantation—Case series. Dent. Traumatol. 2014, 30, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Roskamp, L.; Westphalen, V.D.; Carneiro, E.; Fariniuk, L.F.; Silva Neto, U.X.; Westphalen, F.H. Relationship between extra-alveolar time and atopy in the prognosis of the replantation of avulsed teeth. J. Trauma 2010, 69, 79–81. [Google Scholar] [CrossRef] [PubMed]
- Roskamp, L.; Westphalen, V.P.; Carneiro, E.; Fariniuk, L.F.; Silva Neto, U.X. The positive influence of atopy on the prognosis of avulsed and replanted teeth despite differences in post-trauma management. J. Endod. 2011, 37, 463–465. [Google Scholar] [CrossRef] [PubMed]
- Roskamp, L.; Silva Neto, U.X.; Carneiro, E.; Fariniuk, L.F.; Westphalen, V.P. Influence of Atopy in the Outcome of Avulsed and Replanted Teeth during 5 Years of Follow-up. J. Trauma 2017, 43, 25–28. [Google Scholar] [CrossRef] [PubMed]
- He, D.; Kou, X.; Luo, Q.; Yang, R.; Liu, D.; Wang, X.; Song, Y.; Cao, H.; Zeng, M.; Gan, Y.; et al. Enhanced M1/M2 macrophage ratio promotes orthodontic root resorption. J. Dent. Res. 2015, 94, 129–139. [Google Scholar] [CrossRef] [PubMed]







© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazur, M.; Marasca, R.; Ottolenghi, L.; Vozza, I.; Covello, F.; Zupancich, A.; Cristiani, E.; Nava, A. Different Resorptive Patterns of Two Avulsed and Replanted Upper Central Incisors Based on Scanning Electron Microscopy and Stereomicroscopic Analysis: A Case Report. Appl. Sci. 2020, 10, 3551. https://doi.org/10.3390/app10103551
Mazur M, Marasca R, Ottolenghi L, Vozza I, Covello F, Zupancich A, Cristiani E, Nava A. Different Resorptive Patterns of Two Avulsed and Replanted Upper Central Incisors Based on Scanning Electron Microscopy and Stereomicroscopic Analysis: A Case Report. Applied Sciences. 2020; 10(10):3551. https://doi.org/10.3390/app10103551
Chicago/Turabian StyleMazur, Marta, Roberto Marasca, Livia Ottolenghi, Iole Vozza, Francesco Covello, Andrea Zupancich, Emanuela Cristiani, and Alessia Nava. 2020. "Different Resorptive Patterns of Two Avulsed and Replanted Upper Central Incisors Based on Scanning Electron Microscopy and Stereomicroscopic Analysis: A Case Report" Applied Sciences 10, no. 10: 3551. https://doi.org/10.3390/app10103551
APA StyleMazur, M., Marasca, R., Ottolenghi, L., Vozza, I., Covello, F., Zupancich, A., Cristiani, E., & Nava, A. (2020). Different Resorptive Patterns of Two Avulsed and Replanted Upper Central Incisors Based on Scanning Electron Microscopy and Stereomicroscopic Analysis: A Case Report. Applied Sciences, 10(10), 3551. https://doi.org/10.3390/app10103551