
Relationship Between Cardiac Troponin I Concentration and Myocardial Function in Hypertrophic Cardiomyopathy Cats With or Without Left Ventricular Outflow Tract Obstruction

 , , , and
, , , and
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Standard Echocardiography
2.3. Two-Dimensional Speckle Tracking Echocardiography
2.4. cTnI Measurement
2.5. Statistical Analysis
3. Results
3.1. Clinical Prifiles and Standard Echocardiography
3.2. 2D-STE Variables
3.3. Correlation Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferasin, L.; Sturgess, C.P.; Cannon, M.J.; Caney, S.M.A.; Gruffydd-Jones, T.J.; Wotton, P.R. Feline Idiopathic Cardiomyopathy: A Retrospective Study of 106 Cats (1994–2001). J. Feline Med. Surg. 2003, 5, 151–159. [Google Scholar] [CrossRef]
- Fox, P.R.; Keene, B.W.; Lamb, K.; Schober, K.A.; Chetboul, V.; Luis Fuentes, V.; Wess, G.; Payne, J.R.; Hogan, D.F.; Motsinger-Reif, A.; et al. International Collaborative Study to Assess Cardiovascular Risk and Evaluate Long-Term Health in Cats with Preclinical Hypertrophic Cardiomyopathy and Apparently Healthy Cats: The REVEAL Study. J. Vet. Intern Med. 2018, 32, 930–943. [Google Scholar] [CrossRef] [PubMed]
- Saito, T.; Suzuki, R.; Yuchi, Y.; Fukuoka, H.; Satomi, S.; Teshima, T.; Matsumoto, H. Comparative Study of Myocardial Function in Cases of Feline Hypertrophic Cardiomyopathy with and without Dynamic Left-Ventricular Outflow-Tract Obstruction. Front. Vet. Sci. 2023, 10, 1191211. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, R.; Saito, T.; Yuchi, Y.; Kanno, H.; Teshima, T.; Matsumoto, H.; Koyama, H. Detection of Congestive Heart Failure and Myocardial Dysfunction in Cats With Cardiomyopathy by Using Two-Dimensional Speckle-Tracking Echocardiography. Front. Vet. Sci. 2021, 8, 771244. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, R.; Mochizuki, Y.; Yoshimatsu, H.; Niina, A.; Teshima, T.; Matsumoto, H.; Koyama, H. Layer-Specific Myocardial Function in Asymptomatic Cats with Obstructive Hypertrophic Cardiomyopathy Assessed Using 2-Dimensional Speckle-Tracking Echocardiography. J. Vet. Intern. Med. 2019, 33, 37–45. [Google Scholar] [CrossRef]
- Suzuki, R.; Mochizuki, Y.; Yuchi, Y.; Yasumura, Y.; Saito, T.; Teshima, T.; Matsumoto, H.; Koyama, H. Assessment of Myocardial Function in Obstructive Hypertrophic Cardiomyopathy Cats with and without Response to Medical Treatment by Carvedilol. BMC Vet. Res. 2019, 15, 1–8. [Google Scholar] [CrossRef]
- Yang, H.; Carasso, S.; Woo, A.; Jamorski, M.; Nikonova, A.; Wigle, E.D.; Rakowski, H. Hypertrophy Pattern and Regional Myocardial Mechanics Are Related in Septal and Apical Hypertrophic Cardiomyopathy. J. Am. Soc. Echocardiogr. 2010, 23, 1081–1089. [Google Scholar] [CrossRef]
- Carasso, S.; Yang, H.; Woo, A.; Vannan, M.A.; Jamorski, M.; Wigle, E.D.; Rakowski, H. Systolic Myocardial Mechanics in Hypertrophic Cardiomyopathy: Novel Concepts and Implications for Clinical Status. J. Am. Soc. Echocardiogr. 2008, 21, 675–683. [Google Scholar] [CrossRef]
- Suzuki, R.; Mochizuki, Y.; Yoshimatsu, H.; Niina, A.; Teshima, T.; Matsumoto, H.; Koyama, H. Early Detection of Myocardial Dysfunction Using Two-Dimensional Speckle Tracking Echocardiography in a Young Cat with Hypertrophic Cardiomyopathy. JFMS Open Rep. 2018, 4, 2055116918756219. [Google Scholar] [CrossRef]
- Adams, J.E.; Bodor, G.S.; Dávila-Román, V.G.; Delmez, J.A.; Apple, F.S.; Ladenson, J.H.; Jaffe, A.S. Cardiac Troponin I. A Marker with High Specificity for Cardiac Injury. Circulation 1993, 88, 101–106. [Google Scholar] [CrossRef]
- Chapelle, J.P. Cardiac Troponin I and Troponin T: Recent Players in the Field of Myocardial Markers. Clin. Chem. Lab. Med. 1999, 37, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Lipshultz, S.E.; Rifai, N.; Sallan, S.E.; Lipsitz, S.R.; Dalton, V.; Sacks, D.B.; Ottlinger, M.E. Predictive Value of Cardiac Troponin T in Pediatric Patients at Risk for Myocardial Injury. Circulation 1997, 96, 2641–2648. [Google Scholar] [CrossRef] [PubMed]
- Coats, C.J.; Masri, A.; Barriales-Villa, R.; Abraham, T.P.; Brinkley, D.M.; Claggett, B.L.; Hagege, A.; Hegde, S.M.; Ho, C.Y.; Kulac, I.J.; et al. Cardiac Biomarkers and Effects of Aficamten in Obstructive Hypertrophic Cardiomyopathy: The SEQUOIA-HCM Trial. Eur. Heart. J. 2024, 45, 4464–4478. [Google Scholar] [CrossRef]
- Hori, Y.; Iguchi, M.; Heishima, Y.; Yamashita, Y.; Nakamura, K.; Hirakawa, A.; Kitade, A.; Ibaragi, T.; Katagi, M.; Sawada, T.; et al. Diagnostic Utility of Cardiac Troponin I in Cats with Hypertrophic Cardiomyopathy. J. Vet. Intern. Med. 2018, 32, 922–929. [Google Scholar] [CrossRef]
- Borgeat, K.; Sherwood, K.; Payne, J.R.; Luis Fuentes, V.; Connolly, D.J. Plasma Cardiac Troponin I Concentration and Cardiac Death in Cats with Hypertrophic Cardiomyopathy. J. Vet. Intern. Med. 2014, 28, 1731–1737. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.; Payne, J.R.; Novo Matos, J.; Fong, W.W.; Connolly, D.J.; Luis Fuentes, V. Biomarker Changes with Systolic Anterior Motion of the Mitral Valve in Cats with Hypertrophic Cardiomyopathy. J. Vet. Intern. Med. 2020, 34, 1718–1727. [Google Scholar] [CrossRef]
- Williams, L.K.; Chan, R.H.; Carasso, S.; Durand, M.; Misurka, J.; Crean, A.M.; Ralph-Edwards, A.; Gruner, C.; Woo, A.; Lesser, J.R.; et al. Effect of Left Ventricular Outflow Tract Obstruction on Left Atrial Mechanics in Hypertrophic Cardiomyopathy. Biomed. Res. Int. 2015, 2015, 1–10. [Google Scholar] [CrossRef]
- Novo Matos, J.; Sargent, J.; Silva, J.; Payne, J.R.; Seo, J.; Spalla, I.; Borgeat, K.; Loureiro, J.; Pereira, N.; Simcock, I.C.; et al. Thin and Hypokinetic Myocardial Segments in Cats with Cardiomyopathy. J. Vet. Cardiol. 2023, 46, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Luis Fuentes, V.; Abbott, J.; Chetboul, V.; Côté, E.; Fox, P.R.; Häggström, J.; Kittleson, M.D.; Schober, K.; Stern, J.A. ACVIM Consensus Statement Guidelines for the Classification, Diagnosis, and Management of Cardiomyopathies in Cats. J. Vet. Intern. Med. 2020, 34, 1062–1077. [Google Scholar] [CrossRef]
- Fox, P.R.; Liu, S.K.; Maron, B.J. Echocardiographic Assessment of Spontaneously Occurring Feline Hypertrophic Cardiomyopathy. An Animal Model of Human Disease. Circulation 1995, 92, 2645–2651. [Google Scholar] [CrossRef]
- Jackson, B.L.; Adin, D.B.; Lehmkuhl, L.B. Effect of Atenolol on Heart Rate, Arrhythmias, Blood Pressure, and Dynamic Left Ventricular Outflow Tract Obstruction in Cats with Subclinical Hypertrophic Cardiomyopathy. J. Vet. Cardiol. 2015, 17 (Suppl. 1), S296–S305. [Google Scholar] [CrossRef]
- Dini, F.L.; Capozza, P.; Donati, F.; Simioniuc, A.; Corciu, A.I.; Fontanive, P.; Pieroni, A.; Di Bello, V.; Marzilli, M. Patterns of Left Ventricular Remodeling in Chronic Heart Failure: Prevalence and Prognostic Implications. Am. Heart J. 2011, 161, 1088–1095. [Google Scholar] [CrossRef] [PubMed]
- Okada, K.; Yamada, S.; Iwano, H.; Nishino, H.; Nakabachi, M.; Yokoyama, S.; Abe, A.; Ichikawa, A.; Kaga, S.; Nishida, M.; et al. Myocardial Shortening in 3 Orthogonal Directions and Its Transmural Variation in Patients with Nonobstructive Hypertrophic Cardiomyopathy. Circ. J. 2015, 79, 2471–2479. [Google Scholar] [CrossRef] [PubMed]
- Ozawa, K.; Funabashi, N.; Takaoka, H.; Kamata, T.; Kanaeda, A.; Saito, M.; Nomura, F.; Kobayashi, Y. Characteristic Myocardial Strain Identified in Hypertrophic Cardiomyopathy Subjects with Preserved Left Ventricular Ejection Fraction Using a Novel Multi-Layer Transthoracic Echocardiography Technique. Int. J. Cardiol. 2015, 184, 237–243. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the Freely Available Easy-to-Use Software “EZR” for Medical Statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, R.A.; Holmes, D.R. Clinical Practice. Hypertrophic Obstructive Cardiomyopathy. N. Engl. J. Med. 2004, 350, 1320–1327. [Google Scholar] [CrossRef]
- Ferasin, L.; Kilkenny, E.; Ferasin, H. Evaluation of N-Terminal Prohormone of Brain Natriuretic Peptide and Cardiac Troponin-I Levels in Cats with Systolic Anterior Motion of the Mitral Valve in the Absence of Left Ventricular Hypertrophy. J. Vet. Cardiol. 2020, 30, 23–31. [Google Scholar] [CrossRef]
- Chang, S.A.; Lee, S.C.; Choe, Y.H.; Hahn, H.J.; Jang, S.Y.; Park, S.J.; Choi, J.O.; Park, S.W.; Oh, J.K. Effects of Hypertrophy and Fibrosis on Regional and Global Functional Heterogeneity in Hypertrophic Cardiomyopathy. Int. J. Cardiovasc. Imaging 2012, 28 (Suppl. 2), 133–140. [Google Scholar] [CrossRef]
- Katrukha, A.G.; Bereznikova, A.V.; Esakova, T.V.; Pettersson, K.; Lövgren, T.; Severina, M.E.; Pulkki, K.; Vuopio-Pulkki, L.M.; Gusev, N.B. Troponin I Is Released in Bloodstream of Patients with Acute Myocardial Infarction Not in Free Form but as Complex. Clin. Chem. 1997, 43, 1379–1385. [Google Scholar] [CrossRef]
- Dunn, M.E.; Coluccio, D.; Hirkaler, G.; Mikaelian, I.; Nicklaus, R.; Lipshultz, S.E.; Doessegger, L.; Reddy, M.; Singer, T.; Geng, W. The Complete Pharmacokinetic Profile of Serum Cardiac Troponin I in the Rat and the Dog. Toxicol. Sci. 2011, 123, 368–373. [Google Scholar] [CrossRef]
- Dybro, A.M.; Rasmussen, T.B.; Nielsen, R.R.; Andersen, M.J.; Jensen, M.K.; Poulsen, S.H. Randomized Trial of Metoprolol in Patients With Obstructive Hypertrophic Cardiomyopathy. J. Am. Coll. Cardiol. 2021, 78, 2505–2517. [Google Scholar] [CrossRef] [PubMed]
- Maron, B.J.; Maron, M.S.; Wigle, E.D.; Braunwald, E. The 50-Year History, Controversy, and Clinical Implications of Left Ventricular Outflow Tract Obstruction in Hypertrophic Cardiomyopathy from Idiopathic Hypertrophic Subaortic Stenosis to Hypertrophic Cardiomyopathy: From Idiopathic Hypertrophic Subaortic Stenosis to Hypertrophic Cardiomyopathy. J. Am. Coll. Cardiol. 2009, 54, 191–200. [Google Scholar] [CrossRef]
- Coppini, R.; Ferrantini, C.; Pioner, J.M.; Santini, L.; Wang, Z.J.; Palandri, C.; Scardigli, M.; Vitale, G.; Sacconi, L.; Stefàno, P.; et al. Electrophysiological and Contractile Effects of Disopyramide in Patients with Obstructive Hypertrophic Cardiomyopathy: A Translational Study. JACC Basic Transl. Sci. 2019, 4, 795–813. [Google Scholar] [CrossRef] [PubMed]
- Teichman, S. The Anticholinergic Side Effects of Disopyramide and Controlled-Release Disopyramide. Angiology 1985, 36, 767–771. [Google Scholar] [CrossRef] [PubMed]
- Masri, A.; Choudhury, L.; Barriales-Villa, R.; Elliott, P.; Maron, M.S.; Nassif, M.E.; Oreziak, A.; Owens, A.T.; Saberi, S.; Tower-Rader, A.; et al. Standard-of-Care Medication Withdrawal in Patients with Obstructive Hypertrophic Cardiomyopathy Receiving Aficamten in FOREST-HCM. J. Am. Coll. Cardiol. 2024, 84, 1839–1849. [Google Scholar] [CrossRef] [PubMed]
- Dong, Z.; Wang, S.; Liu, Z.; Han, E.; Wu, C.; Luo, C.; Chen, W.; Mei, F.; Lu, X.; Yan, M.; et al. An Innovative Minimally Invasive Approach for Hypertrophic Obstructive Cardiomyopathy: Transaortic Septal Myectomy via Right Infra-Axillary Incision. JTCVS Tech. 2024, 28, 50–58. [Google Scholar] [CrossRef]
- Ommen, S.R.; Ho, C.Y.; Asif, I.M.; Balaji, S.; Burke, M.A.; Day, S.M.; Dearani, J.A.; Epps, K.C.; Evanovich, L.; Ferrari, V.A.; et al. 2024 AHA/ACC/AMSSM/HRS/PACES/SCMR Guideline for the Management of Hypertrophic Cardiomyopathy: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation 2024, 149, e1239–e1311. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables | HNCM (n = 13) | HOCM (n = 33) | p-Value |
|---|---|---|---|
| Sex (male, female) | 6, 7 | 23, 10 | 0.18 |
| Age (year) | 3.4 (1.7, 7.1) | 2.7 (1.4, 5.7) | 0.45 |
| Body weight (kg) | 4.2 (3.6, 4.9) | 4.3 (3.8, 5.4) | 0.35 |
| ACVIM (B1, B2, C/D) | 12, 1, 0 | 30, 3, 0 | 0.99 |
| Heart rate (bpm) | 180 (132, 202) | 192 (166, 229) | 0.79 |
| Systolic blood pressure (mmHg) | 131 (125, 140) | 135 (121, 142) | 0.26 |
| LVOTVrest (m/s) | 1.1 (0.9, 1.3) | 3.7 (2.8, 4.5) * | <0.01 |
| LVOTVexcited (m/s) | 1.4 (1.2, 1.9) | 4.3 (4.0, 4.9) * | <0.01 |
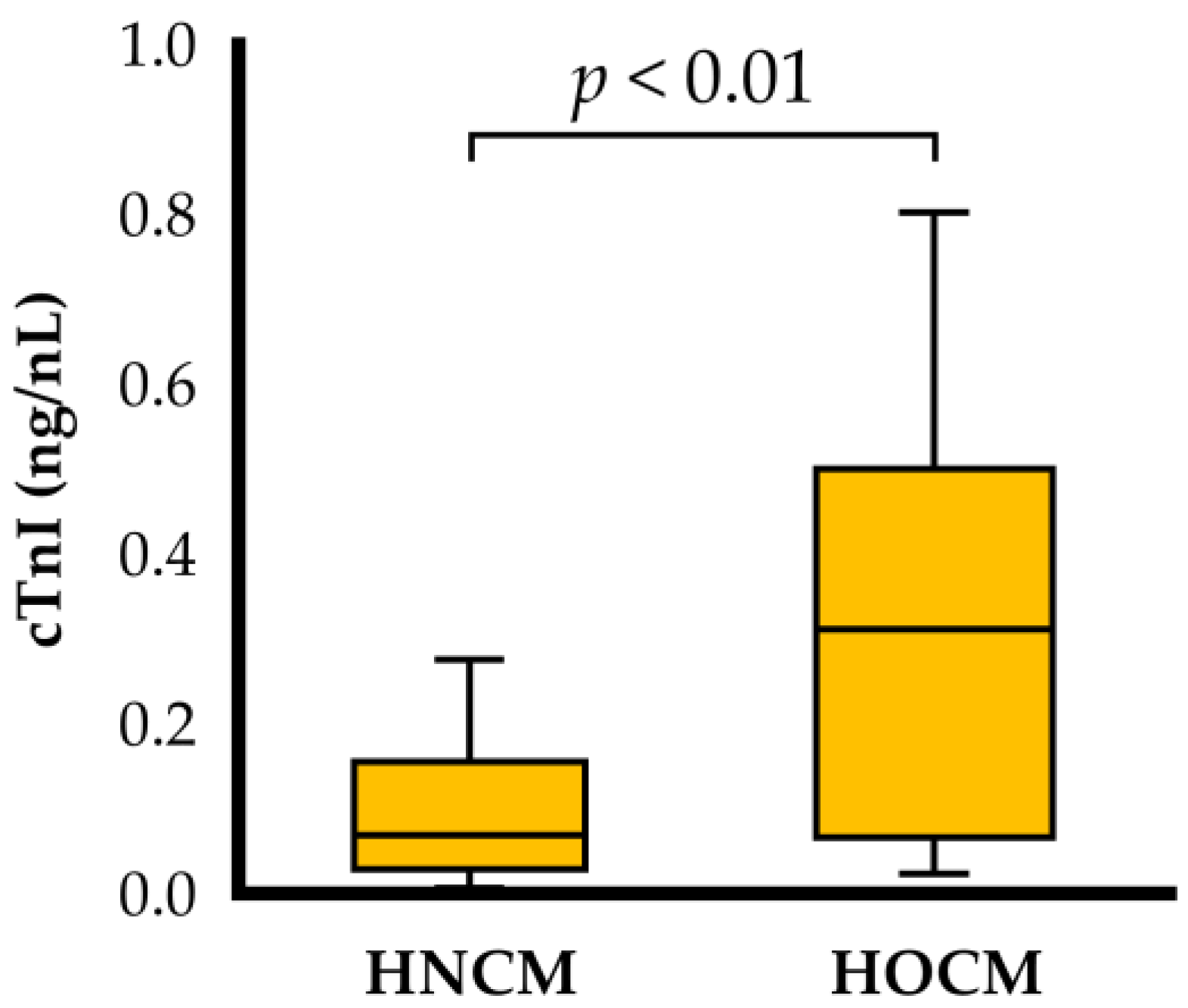
| cTnI (ng/mL) | 0.069 (0.029, 0.156) | 0.311 (0.066, 0.500) * | <0.01 |
| Number of cases with high cTnI levels (n) | 4 | 24 | 0.02 |
| Medication (yes, no) | 9, 4 | 13, 20 | 0.10 |
| Medical Drugs | HNCM (n = 13) | HOCM (n = 33) | p-Value |
|---|---|---|---|
| Beta blocker (n) | 7 | 10 | 0.18 |
| Angiotensin converting enzyme inhibitor (n) | 1 | 2 | 0.99 |
| Pimobendan (n) | 1 | 1 | 0.99 |
| Clopidogrel (n) | 2 | 0 | 0.36 |
| No medication (n) | 4 | 20 | 0.10 |
| Variables | HNCM | HOCM | p-Value |
|---|---|---|---|
| LA/Ao | 1.2 (1.1, 1.2) | 1.3 (1.2, 1.4) * | 0.049 |
| IVSd (mm) | 6.0 (5.0, 7.1) | 6.3 (5.3, 7.0) | 0.52 |
| LVPWd (mm) | 5.2 (4.6, 6.6) | 5.8 (5.4, 6.9) | 0.053 |
| LVIDd (mm) | 13.3 (11.4, 15.5) | 12.8 (11.9, 15.3) | 0.85 |
| RWT | 0.90 (0.81, 0.93) | 0.94 (0.76, 1.08) | 0.28 |
| FS (%) | 42.2 (37.4, 54.9) | 43.0 (37.9, 48.4) | 0.92 |
| E vel (m/s) | 0.6 (0.5, 0.7) | 0.8 (0.7, 0.9) * | 0.01 |
| E/A | 0.8 (0.8, 1.1) | 0.9 (0.8, 1.3) | 0.45 |
| E/A fusion | 1.0 (0.8, 1.0) (n = 5) | 1.0 (0.9, 1.1) (n = 9) | 0.62 |
| HNCM | HOCM | p-Value | |
|---|---|---|---|
| Longitudinal strain (%) | |||
| Whole layer | 13.1 (10.9, 14.2) | 13.0 (9.2, 16.9) | 0.89 |
| Endocardium | 15.0 (12.6, 16.2) | 14.0 (10.8, 20.1) | 0.94 |
| Epicardium | 11.6 (9.4, 12.9) | 10.7 (8.0, 13.9) * | 0.52 |
| End/Epi | 1.3 (1.2, 1.4) | 1.3 (1.2, 1.6) | 0.70 |
| Circumferential strains (%) | |||
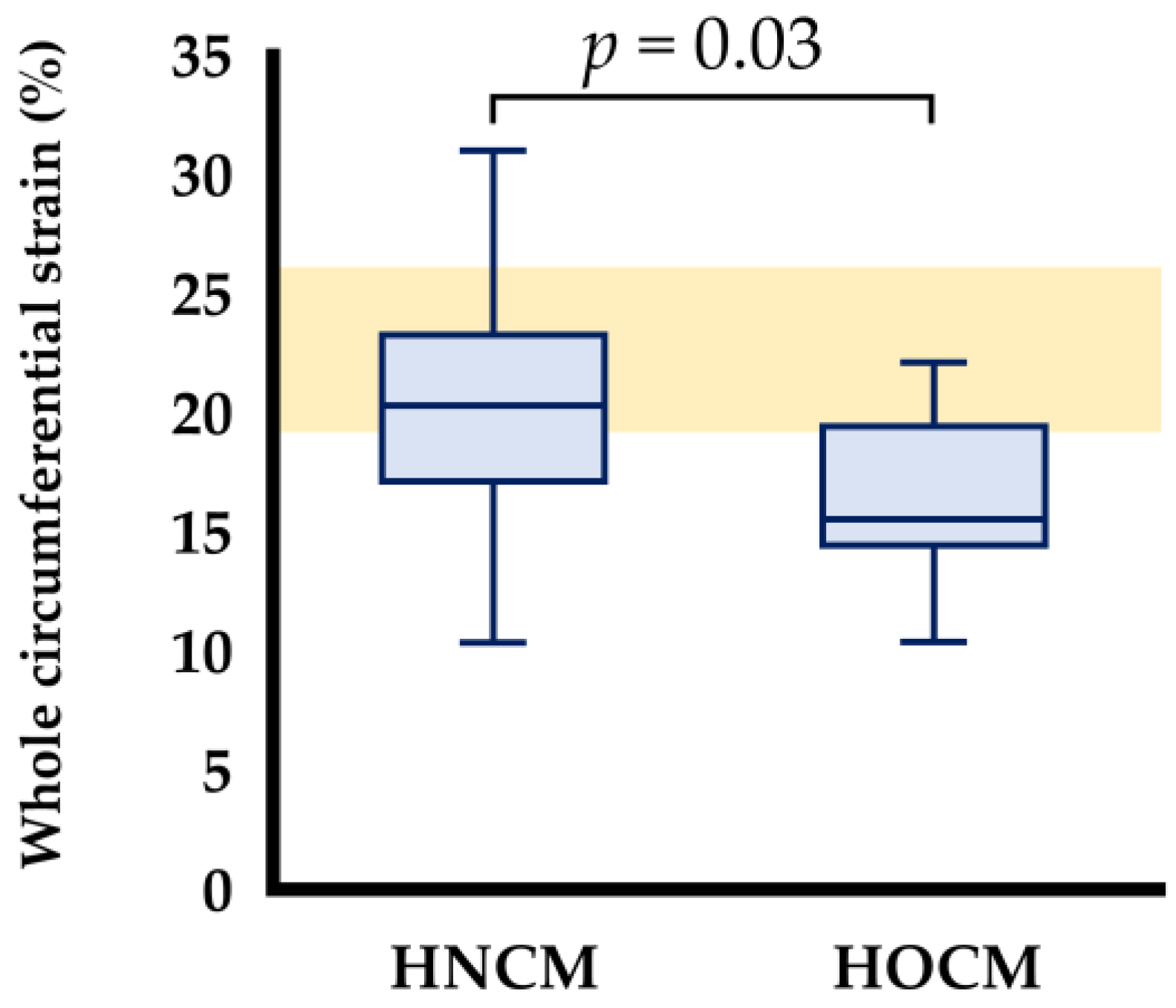
| Whole layer | 20.3 (16.0, 23.5) | 15.5 (14.3, 19.7) * | 0.028 |
| Endocardium | 37.2 (31.8, 41.1) | 31.8 (28.6, 35.6) | 0.07 |
| Epicardium | 8.9 (7.3, 12.0) | 6.6 (5.0, 8.8) * | 0.011 |
| End/Epi | 4.2 (3.2, 5.3) | 4.7 (3.8, 5.8) | 0.23 |
| cTnI | LVOTVexcited | LVOTVrest | ||||
|---|---|---|---|---|---|---|
| r | p | r | p | r | p | |
| cTnI | ― | ― | 0.51 | <0.01 | 0.50 | <0.01 |
| LVOTVexcited | ― | ― | 0.72 | <0.01 | ||
| LVOTVrest | ― | ― | ||||
| Longitudinal strain (%) | ||||||
| Whole layer | −0.27 | 0.13 | −0.02 | 0.90 | −0.01 | 0.98 |
| Endocardium | −0.19 | 0.28 | −0.09 | 0.64 | −0.03 | 0.87 |
| Epicardium | −0.29 | 0.10 | −0.15 | 0.39 | −0.15 | 0.26 |
| Circumferential strains (%) | ||||||
| Whole layer | −0.20 | 0.26 | −0.08 | 0.67 | −0.18 | 0.30 |
| Endocardium | −0.13 | 0.46 | −0.12 | 0.51 | −0.07 | 0.71 |
| Epicardium | −0.12 | 0.10 | −0.03 | 0.85 | −0.20 | 0.26 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Satomi, S.; Suzuki, R.; Yuchi, Y.; Yoshii, Y.; Kanno, H.; Teshima, T.; Matsumoto, H. Relationship Between Cardiac Troponin I Concentration and Myocardial Function in Hypertrophic Cardiomyopathy Cats With or Without Left Ventricular Outflow Tract Obstruction. Animals 2025, 15, 1313. https://doi.org/10.3390/ani15091313
Satomi S, Suzuki R, Yuchi Y, Yoshii Y, Kanno H, Teshima T, Matsumoto H. Relationship Between Cardiac Troponin I Concentration and Myocardial Function in Hypertrophic Cardiomyopathy Cats With or Without Left Ventricular Outflow Tract Obstruction. Animals. 2025; 15(9):1313. https://doi.org/10.3390/ani15091313
Chicago/Turabian StyleSatomi, Shuji, Ryohei Suzuki, Yunosuke Yuchi, Yayoi Yoshii, Haruka Kanno, Takahiro Teshima, and Hirotaka Matsumoto. 2025. "Relationship Between Cardiac Troponin I Concentration and Myocardial Function in Hypertrophic Cardiomyopathy Cats With or Without Left Ventricular Outflow Tract Obstruction" Animals 15, no. 9: 1313. https://doi.org/10.3390/ani15091313
APA StyleSatomi, S., Suzuki, R., Yuchi, Y., Yoshii, Y., Kanno, H., Teshima, T., & Matsumoto, H. (2025). Relationship Between Cardiac Troponin I Concentration and Myocardial Function in Hypertrophic Cardiomyopathy Cats With or Without Left Ventricular Outflow Tract Obstruction. Animals, 15(9), 1313. https://doi.org/10.3390/ani15091313