
Knowledge, Attitudes and Behaviors regarding Tick-Borne Encephalitis Vaccination and Prevention of Tick-Borne Diseases among Primary Care Physicians in Bavaria and Baden-Wuerttemberg, Germany, May–September 2022
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Procedures
2.3. Questionnaire Content
- -
- Demographic characteristics (i.e., gender, age, TBE and influenza vaccination status);
- -
- General practice data (i.e., type of practice, license plate area code of practice, medical specialty). We used the license plate area code to determine the work state and classify urban–rural level according to the nomenclature of territorial units for statistics (NUTS) 2021 level 3 [27];
- -
- Awareness of TBE guidelines and experience with TBE and other TBDs (i.e., awareness of STIKO recommendations, STIKO vaccination app and TBE risk area status, experience with treating TBDs, self-perceived adequacy of knowledge about risks and benefits of TBE vaccination);
- -
- General vaccination and TBE vaccination practices (i.e., provision of vaccination to clients, method of conducting vaccination consultations, checking client’s vaccination status, reminding clients of due vaccinations);
- -
- Reasons for not providing vaccinations (i.e., logistical difficulties, high effort for clarification, patient non-compliance, concerns about TBE vaccine safety, low perceived health risk of TBE, doubts about TBE vaccine effectiveness);
- -
- Self-perception of adequate knowledge about risk and benefits of TBE vaccination;
- -
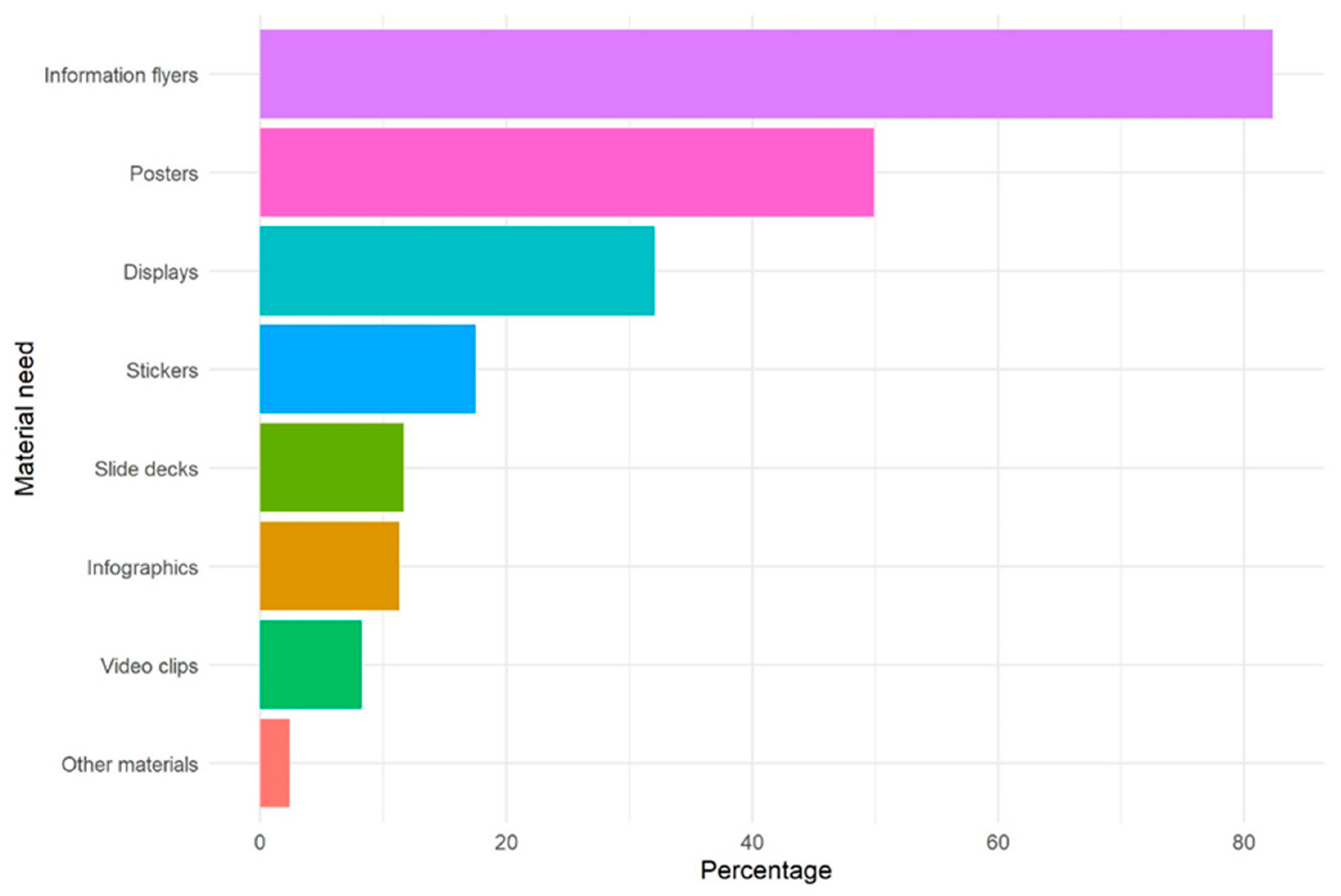
- Specific knowledge needs and need for information materials (i.e., posters, information flyers, stickers, display stands, video clips, slide sets, infographs, others) on TBE vaccination, TBDs in general and tick prevention;
- -
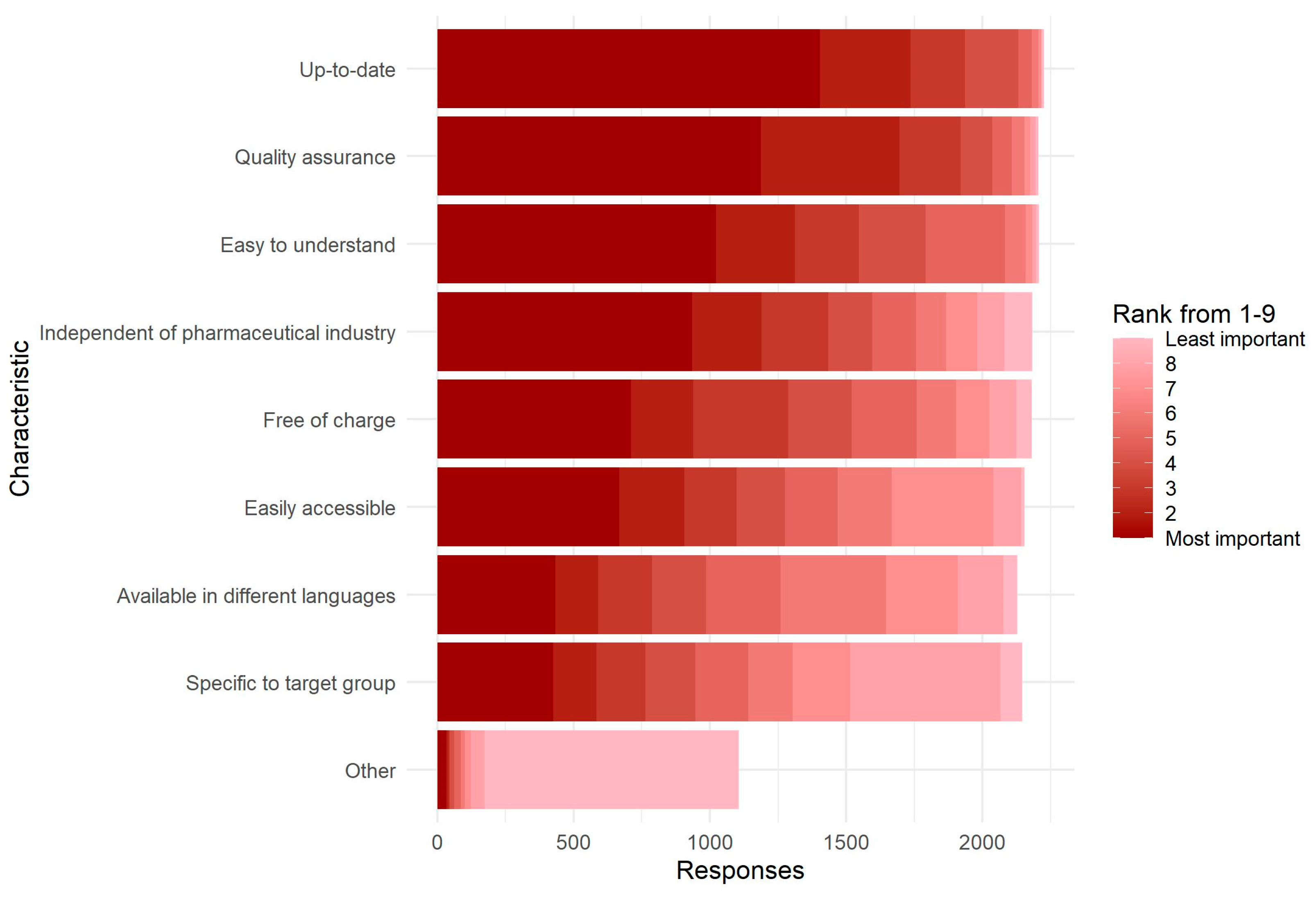
- Relative importance of different characteristics of information materials (i.e., independence of pharmaceutical companies, quality assurance, free-of-charge, up-to-date, easy to understand, specific to target group, accessibility, availability in different languages, others).
2.4. Statistical Analysis
3. Results
3.1. Study Population
3.2. Awareness of TBE Guidelines and Experience with Tick-Borne Diseases including TBE
3.3. Vaccination Practices
3.4. Information Material Needs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Piesman, J.; Gern, L. Lyme borreliosis in Europe and North America. Parasitology 2004, 129, S191–S220. [Google Scholar] [CrossRef]
- Enkelmann, J.; Böhmer, M.; Fingerle, V.; Siffczyk, C.; Werber, D.; Littmann, M.; Merbecks, S.-S.; Helmeke, C.; Schroeder, S.; Hell, S.; et al. Incidence of notified Lyme borreliosis in Germany, 2013–2017. Sci. Rep. 2018, 8, 14976. [Google Scholar] [CrossRef]
- Böhmer, M.M.; Böhm, S.; Heinzinger, S.; Fingerle, V. Epidemiological Surveillance of Lyme Borreliosis in Bavaria, Germany, 2013–2020. Microorganisms 2021, 3, 1872. [Google Scholar] [CrossRef] [PubMed]
- Stanek, G.; Strl, F. Lyme borreliosis–from tick bite to diagnosis and treatment. FEMS Microbiol. Rev. 2018, 42, 233–258. [Google Scholar] [CrossRef] [PubMed]
- Dumpis, U.; Crook, D.; Oksi, J. Tick-Borne Encephalitis. Clin. Infect. Dis. 1999, 28, 882–890. [Google Scholar] [CrossRef] [PubMed]
- Lindquist, L.; Vapalahti, O. Tick-borne encephalitis. Lancet 2008, 371, 1861–1871. [Google Scholar] [CrossRef] [PubMed]
- Kohl, I.; Kozuch, O.; Elecková, E.; Labuda, M.; Zaludko, J. Family outbreak of alimentary tick-borne encephalitis in Slovakia associated with a natural focus of infection. Eur. J. Epidemiol. 1996, 12, 373–375. [Google Scholar] [CrossRef]
- Holzmann, H. Diagnosis of tick-borne encephalitis. Vaccine 2003, 21 (Suppl. 1), S36–S40. [Google Scholar] [CrossRef]
- Kaiser, R. The clinical and epidemiological profile of tick-borne encephalitis in southern Germany 1994-98: A prospective study of 656 patients. Brain 1999, 122 Pt 11, 2067–2078. [Google Scholar] [CrossRef]
- Mickiene, A.; Laiskonis, A.; Günther, G.; Vene, S.; Lundkvistz, A.; Lindquist, L. Tickborne encephalitis in an area of high endemicity in lithuania: Disease severity and long-term prognosis. Clin. Infect. Dis. 2002, 35, 650–658. [Google Scholar] [CrossRef]
- Robert Koch Institute. SurvStat@RKI 2.0. Web-Basierte Abfrage der Meldedaten gemäß Infektionsschutzgesetz (IfSG) 2023 (updated 15 January 2023). Available online: https://survstat.rki.de/ (accessed on 9 February 2023).
- Robert Koch Institute. Meldepflichtige Krankheiten und Krankheitserreger (updated 16 November 2020). Available online: https://www.rki.de/DE/Content/Infekt/IfSG/Meldepflichtige_Krankheiten/Meldepflichtige_Krankheiten_node.html (accessed on 26 January 2023).
- Robert Koch Institute (RKI). FSME: Risikogebiete in Deutschland (Stand: Januar 2023). Epidemiologisches Bulletin 2023, 9, 3–22. [Google Scholar]
- Hellenbrand, W.; Kreusch, T.; Böhmer, M.M.; Wagner-Wiening, C.; Dobler, G.; Wichmann, O.; Altmann, D. Epidemiology of Tick-Borne Encephalitis (TBE) in Germany, 2001–2018. Pathogens 2019, 8, 42. [Google Scholar] [CrossRef]
- Borde, J.P.; Kaier, K.; Hehn, P.; Böhmer, M.M.; Kreusch, T.M.; Dobler, G. Tick-borne encephalitis virus infections in Germany. Seasonality and in-year patterns. A retrospective analysis from 2001–2018. PLoS ONE 2019, 14, e0224044. [Google Scholar] [CrossRef]
- Robert Koch Institute. SurvStat@RKI 2.0. Web-Basierte Abfrage der Meldedaten gemäß Infektionsschutzgesetz (IfSG) 2023 (updated 16 March 2023). Available online: https://survstat.rki.de/ (accessed on 16 March 2023).
- World Health Organization. WHO Guidelines on Tularaemia. 2007. Available online: https://apps.who.int/iris/handle/10665/43793 (accessed on 3 April 2023).
- Heinz, F.X.; Stiasny, K.; Holzmann, H.; Grgic-Vitek, M.; Kriz, B.; Essl, A.; Kundi, M. Vaccination and tick-borne encephalitis, central Europe. Emerg. Infect. Dis. 2013, 19, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Demicheli, V.; Debalini, M.G.; Rivetti, A. Vaccines for preventing tick-borne encephalitis. Cochrane Database Syst. Rev. 2009, 2009, Cd000977. [Google Scholar] [CrossRef] [PubMed]
- Nygren, T.M.; Pilic, A.; Böhmer, M.M.; Wagner-Wiening, C.; Wichmann, O.; Harder, T.; Hellenbrand, W. Tick-borne encephalitis vaccine effectiveness and barriers to vaccination in Germany. Sci. Rep. 2022, 12, 11706. [Google Scholar] [CrossRef] [PubMed]
- Robert Koch Institute. Epidemiologisches Bulletin. Empfehlungen der Ständigen Impfkommission beim Robert Koch-Institut, 2021; Robert Koch Institute: Berlin, Germany, 2021. [Google Scholar]
- Schley, K.; Malerczyk, C.; Beier, D.; Schiffner-Rohe, J.; von Eiff, C.; Häckl, D.; Süß, J. Vaccination rate and adherence of tick-borne encephalitis vaccination in Germany. Vaccine 2021, 39, 830–838. [Google Scholar] [CrossRef] [PubMed]
- Böhmer, M.M.; Walter, D.; Krause, G.; Müters, S.; Gösswald, A.; Wichmann, O. Determinants of tetanus and seasonal influenza vaccine uptake in adults living in Germany. Hum. Vaccin. 2011, 7, 1317–1325. [Google Scholar] [CrossRef]
- Gargano, L.M.; Herbert, N.L.; Painter, J.E.; Sales, J.M.; Morfaw, C.; Rask, K.; Murray, D.; DiClemente, R.J.; Hughes, J.M. Impact of a physician recommendation and parental immunization attitudes on receipt or intention to receive adolescent vaccines. Hum. Vaccines Immunother. 2013, 9, 2627–2633. [Google Scholar] [CrossRef]
- Hagemann, C.; Streng, A.; Kraemer, A.; Liese, J.G. Heterogeneity in coverage for measles and varicella vaccination in toddlers—Analysis of factors influencing parental acceptance. BMC Public Health 2017, 17, 724. [Google Scholar] [CrossRef]
- LamaPoll. Available online: https://www.lamapoll.de/ (accessed on 14 February 2023).
- NUTS—Nomenclature of Territorial Units for Statistics. 2021. Available online: https://ec.europa.eu/eurostat/web/nuts/background (accessed on 4 April 2023).
- Wilson, K.; Atkinson, K.M.; Westeinde, J. Apps for immunization: Leveraging mobile devices to place the individual at the center of care. Hum. Vaccines Immunother. 2015, 11, 2395–2399. [Google Scholar] [CrossRef] [PubMed]
- Bednarczyk, R.A.; Frew, P.M.; Salmon, D.A.; Whitney, E.; Omer, S.B. ReadyVax: A new mobile vaccine information app. Hum. Vaccines Immunother. 2017, 13, 1149–1154. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. CDC Vaccine Schedules App for Healthcare Providers. Available online: https://www.cdc.gov/vaccines/schedules/hcp/schedule-app.html (accessed on 4 April 2023).
- Ricco, M.; Gualerzi, G.; Ranzieri, S.; Ferraro, P.; Bragazzi, N.L. Knowledge, Attitudes, Practices (KAP) of Italian Occupational Physicians towards Tick Borne Encephalitis. Trop. Med. Infect. Dis. 2020, 5, 117. [Google Scholar] [CrossRef] [PubMed]
- Vasić, A.; Bjekić, J.; Veinović, G.; Mihaljica, D.; Sukara, R.; Poluga, J.; Filipović, S.R.; Tomanović, S. Knowledge, Attitudes, and Practices on Tick-Borne Encephalitis Virus and Tick-Borne Diseases within Professionally Tick-Exposed Persons, Health Care Workers, and General Population in Serbia: A Questionnaire-Based Study. Int. J. Environ. Res. Public Health 2022, 19, 867. [Google Scholar] [CrossRef] [PubMed]
- Vandererven, C.; Bellanger, A.-P.; Faucher, J.-F.; Marguet, P. Primary care physician management of tick bites in the Franche-Comté region (Eastern France, 2013). Médecine Mal. Infect. 2017, 47, 261–265. [Google Scholar] [CrossRef]
- Dollat, M.; Bellanger, A.-P.; Millon, L.; Chirouze, C.; Lepiller, Q.; Marguet, P. Knowledge and vaccination practices among family physicians in northeastern France regarding tick-borne encephalitis virus. Ticks Tick-Borne Dis. 2021, 12, 101774. [Google Scholar] [CrossRef]
- Pilz, A.; Erber, W.; Schmitt, H.-J. Vaccine uptake in 20 countries in Europe 2020: Focus on tick-borne encephalitis (TBE). Ticks Tick-Borne Dis. 2023, 14, 102059. [Google Scholar] [CrossRef]
- ImpfDocNE: Evidenzbasiertes Impf management für die Praxis. Available online: https://www.impfdocne.de/ (accessed on 9 February 2023).
- Kunze, M.; Banović, P.; Bogovič, P.; Briciu, V.; Čivljak, R.; Dobler, G.; Hristea, A.; Kerlik, J.; Kuivanen, S.; Kynčl, J.; et al. Recommendations to Improve Tick-Borne Encephalitis Surveillance and Vaccine Uptake in Europe. Microorganisms 2022, 10, 1283. [Google Scholar] [CrossRef]
- Schuler, U. Vergleichende Studie über Steigende Quoten der Influenza-und Pneumokokken-Impfung unter Patienten mit chronischen Erkrankungen und Patienten ab 60 Jahren nach Einführung der Praxissoftware Impf-doc; Ludwig-Maximilians-Universität: Munich, Germany, 2016. [Google Scholar]
- Cataldi, J.R.; Kerns, M.E.; O’Leary, S.T. Evidence-based strategies to increase vaccination uptake: A review. Curr. Opin. Pediatr. 2020, 32, 151–159. [Google Scholar] [CrossRef]
- Akmatov, M.K.; Rübsamen, N.; Deyneko, I.V.; Karch, A.; Mikolajczyk, R.T. Poor knowledge of vaccination recommendations and negative attitudes towards vaccinations are independently associated with poor vaccination uptake among adults—Findings of a population-based panel study in Lower Saxony, Germany. Vaccine 2018, 36, 2417–2426. [Google Scholar] [CrossRef]
- Slunge, D. The Willingness to Pay for Vaccination against Tick-Borne Encephalitis and Implications for Public Health Policy: Evidence from Sweden. PLoS ONE 2015, 10, e0143875. [Google Scholar] [CrossRef] [PubMed]
- Betsch, C.; Schmid, P.; Korn, L.; Steinmeyer, L.; Heinemeier, D.; Eitze, S.; Küpke, N.K.; Böhm, R. Psychological antecedents of vaccination: Definitions, measurement, and interventions. Bundesgesundheitsblatt Gesundh. Gesundh. 2019, 62, 400–409. [Google Scholar] [CrossRef]
- Erber, W.; Schmitt, H.-J. Self-reported tick-borne encephalitis (TBE) vaccination coverage in Europe: Results from a cross-sectional study. Ticks Tick-Borne Dis. 2018, 9, 768–777. [Google Scholar] [CrossRef] [PubMed]
- Kunze, M.; Erber, W.; Haditsch, M. Chapter 13: TBE as a matter of public health. In The TBE Book, 4th ed.; Dobler, G., Erber, W., Bröker, M., Schmitt, H.J., Eds.; Global Health Press Pte Ltd.: Singapore, 2021; pp. 359–366. [Google Scholar]
- Faber, M.; Heuner, K.; Jacob, D.; Grunow, R. Tularemia in Germany-A Re-emerging Zoonosis. Front. Cell. Infect. Microbiol. 2018, 8, 40. [Google Scholar] [CrossRef]
- Böhmer, M.M.; Walter, D.; Ehrhardt, J.; Reiter, S.; Krause, G.; Wichmann, O. Saisonale und pandemische Influenzaimpfung: Impfquoten und Einstellung niedergelassener Ärzte in Deutschland. Das Gesundh. 2014, 76, 44–47. [Google Scholar] [CrossRef]
- Stöcker, A.; Hoffmann, J.; Mause, L.; Neufeind, J.; Ohnhaüser, T.; Scholten, N. What impact does the attitude toward COVID-19 vaccination have on physicians as vaccine providers? A cross-sectional study from the German outpatient sector. Vaccine 2023, 41, 263–273. [Google Scholar] [CrossRef] [PubMed]
- Hadigal, S.; Cook, J. Knowledge and perception regarding effectiveness in influenza vaccines among General Practitioners in Germany: A national survey. Vaccine X 2022, 12, 100236. [Google Scholar] [CrossRef]
- Tillmann, J.; Weckbecker, K.; Wiesheu, P.; Bleckwenn, M.; Deutsch, T.; Münster, E. Hausärtzliche Versorgung ukrainischer Geflüchteter. Z. Für Allg. 2023, 99, 28–33. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| State | ||||
|---|---|---|---|---|
| Characteristic | Overall N = 2321 | Baden-Wuerttemberg n = 1222 | Bavaria n = 1067 | Not Coded n = 32 |
| Online or paper questionnaire | ||||
| Online | 797 (34%) | 431 (35%) | 359 (34%) | 7 (22%) |
| Paper | 1524 (66%) | 791 (65%) | 708 (66%) | 25 (78%) |
| Gender | ||||
| Female | 1009 (44%) | 510 (42%) | 489 (46%) | 10 (50%) |
| Male | 1278 (56%) | 700 (58%) | 568 (53%) | 10 (50%) |
| Not specified | 15 (0.7%) | 7 (0.6%) | 8 (0.8%) | 0 (0%) |
| Age in years | ||||
| ≤30 | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| 31–40 | 169 (7.4%) | 81 (6.7%) | 87 (8.2%) | 1 (5.3%) |
| 41–50 | 504 (22%) | 260 (21%) | 238 (22%) | 6 (32%) |
| 51–60 | 864 (38%) | 477 (39%) | 382 (36%) | 5 (26%) |
| >60 | 753 (33%) | 393 (32%) | 353 (33%) | 7 (37%) |
| Type of practice | ||||
| Individual practice | 1165 (51%) | 606 (50%) | 548 (53%) | 11 (58%) |
| Joint or group practice | 1075 (47%) | 587 (49%) | 480 (46%) | 8 (42%) |
| Medical care center | 11 (0.5%) | 5 (0.4%) | 6 (0.6%) | 0 (0%) |
| Other | 15 (0.7%) | 7 (0.6%) | 8 (0.8%) | 0 (0%) |
| Urban–rural level of practice (NUTS level 3) | ||||
| Predominantly rural | 494 (22%) | 127 (10%) | 367 (34%) | Missing |
| Intermediate | 1030 (45%) | 588 (48%) | 442 (41%) | Missing |
| Predominantly urban | 760 (33%) | 503 (41%) | 257 (24%) | Missing |
| Medical speciality | ||||
| General medicine/practitioner | 1533 (66%) | 746 (61%) | 774 (73%) | 13 (65%) |
| Internal medicine (primary care, without further specialisation) | 339 (15%) | 297 (24%) | 38 (3.6%) | 4 (20%) |
| Pediatrics | 334 (14%) | 127 (10%) | 206 (19%) | 1 (5.0%) |
| Other | 100 (4.3%) | 49 (4.0%) | 49 (4.6%) | 2 (10%) |
| Offers travel medicine advice | 1863 (81%) | 963 (80%) | 884 (83%) | 16 (80%) |
| Regularly gets vaccinated against influenza | 1949 (85%) | 1035 (85%) | 890 (84%) | 24 (80%) |
| Vaccinated against TBE | 1937 (84%) | 1026 (85%) | 888 (84%) | 23 (77%) |
| State | ||||
|---|---|---|---|---|
| Characteristic | Overall N = 2321 | Baden-Wuerttemberg n = 1222 | Bavaria n = 1067 | Not Coded n = 32 |
| Is aware of: | ||||
| Current STIKO recommendations | 2088 (91%) | 1114 (92%) | 955 (90%) | 19 (100%) |
| STIKO@RKI vaccination app | 776 (34%) | 432 (36%) | 340 (32%) | 4 (21%) |
| TBE risk areas | 2065 (90%) | 1105 (92%) | 944 (89%) | 16 (84%) |
| Practice located in a TBE risk area | 2255 (99%) | 1199 (99%) | 1037 (98%) | 19 (100%) |
| Has experience with: | ||||
| Treating TBE | 1110 (48%) | 612 (50%) | 488 (46%) | 10 (53%) |
| Treating Lyme borreliosis | 2203 (96%) | 1162 (96%) | 1023 (97%) | 18 (95%) |
| Treating tularemia | 55 (2.4%) | 27 (2.2%) | 28 (2.6%) | 0 (0%) |
| Treating other TBDs | 197 (8.6%) | 96 (7.9%) | 100 (9.4%) | 1 (5.3%) |
| No experience with treating TBDs | 60 (2.6%) | 34 (2.8%) | 26 (2.5%) | 0 (0%) |
| Perceives knowledge about risks and benefits of vaccination in general as adequate | 2260 (98%) | 1198 (99%) | 1033 (97%) | 29 (94%) |
| State | ||||
|---|---|---|---|---|
| Characteristic | Overall N = 2321 | Baden-Wuerttemberg n = 1222 | Bavaria n = 1067 | Not Coded n = 32 |
| Provides vaccinations | 2226 (97%) | 1189 (98%) | 1019 (96%) | 18 (95%) |
| Provides TBE vaccinations | 2230 (97%) | 1184 (97%) | 1018 (96%) | 28 (93%) |
| Method(s) of offering vaccination consultations: | ||||
| During initial consultation for new patients | 1541 (67%) | 829 (68%) | 700 (66%) | 12 (40%) |
| Regularly for all patients by actively approaching them | 1469 (64%) | 766 (63%) | 683 (64%) | 20 (67%) |
| At the active request of patients | 1846 (80%) | 964 (79%) | 861 (81%) | 21 (70%) |
| In the context of preventive medical check-ups | 2049 (89%) | 1082 (89%) | 947 (89%) | 20 (67%) |
| Through providing information materials | 1351 (59%) | 704 (58%) | 633 (60%) | 14 (47%) |
| Does not offer vaccination consultations | 34 (1.5%) | 14 (1.2%) | 20 (1.9%) | 0 (0%) |
| Regularly checks vaccination status of patients | 2030 (89%) | 1075 (89%) | 930 (88%) | 25 (81%) |
| Reminds patients of due vaccinations | 1934 (84%) | 1022 (84%) | 888 (84%) | 24 (80%) |
| Among those who remind patients (N = 1934), uses reminder system | 538 (28%) | 278 (28%) | 254 (29%) | 6 (26%) |
| Reminds patients of due TBE vaccinations | 1817 (79%) | 958 (79%) | 837 (79%) | 22 (73%) |
| Among those who remind patients (N = 1817), method of reminding patients: | ||||
| Card/sheet of paper with next vaccination | 1240 (69%) | 642 (68%) | 585 (70%) | 13 (59%) |
| Letter or postcard | 77 (4.3%) | 39 (4.1%) | 36 (4.3%) | 2 (9.1%) |
| 88 (4.9%) | 34 (3.6%) | 53 (6.4%) | 1 (4.5%) | |
| Telephone call | 264 (15%) | 117 (12%) | 145 (17%) | 2 (9.1%) |
| SMS (or WhatsApp, etc.) | 36 (2.0%) | 12 (1.3%) | 24 (2.9%) | 0 (0%) |
| Other methods | 738 (41%) | 384 (41%) | 344 (41%) | 10 (45%) |
| Advises against TBE vaccination for: | ||||
| Children | 46 (2.2%) | 23 (2.1%) | 22 (2.3%) | 1 (3.7%) |
| Persons with a medical contraindication | 1841 (88%) | 965 (88%) | 855 (88%) | 21 (78%) |
| Persons who are not exposed to ticks | 453 (22%) | 244 (22%) | 201 (21%) | 8 (30%) |
| Persons who do not live in a TBE risk area | 371 (18%) | 208 (19%) | 156 (16%) | 7 (26%) |
| Other persons | 98 (4.7%) | 49 (4.5%) | 48 (5.0%) | 1 (3.7%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coyer, L.; Sogan-Ekinci, A.; Greutélaers, B.; Kuhn, J.; Saller, F.S.; Hailer, J.; Böhm, S.; Brosch, R.; Wagner-Wiening, C.; Böhmer, M.M. Knowledge, Attitudes and Behaviors regarding Tick-Borne Encephalitis Vaccination and Prevention of Tick-Borne Diseases among Primary Care Physicians in Bavaria and Baden-Wuerttemberg, Germany, May–September 2022. Microorganisms 2023, 11, 961. https://doi.org/10.3390/microorganisms11040961
Coyer L, Sogan-Ekinci A, Greutélaers B, Kuhn J, Saller FS, Hailer J, Böhm S, Brosch R, Wagner-Wiening C, Böhmer MM. Knowledge, Attitudes and Behaviors regarding Tick-Borne Encephalitis Vaccination and Prevention of Tick-Borne Diseases among Primary Care Physicians in Bavaria and Baden-Wuerttemberg, Germany, May–September 2022. Microorganisms. 2023; 11(4):961. https://doi.org/10.3390/microorganisms11040961
Chicago/Turabian StyleCoyer, Liza, Aylin Sogan-Ekinci, Benedikt Greutélaers, Julia Kuhn, Franziska S. Saller, Jana Hailer, Stefanie Böhm, Rainer Brosch, Christiane Wagner-Wiening, and Merle M. Böhmer. 2023. "Knowledge, Attitudes and Behaviors regarding Tick-Borne Encephalitis Vaccination and Prevention of Tick-Borne Diseases among Primary Care Physicians in Bavaria and Baden-Wuerttemberg, Germany, May–September 2022" Microorganisms 11, no. 4: 961. https://doi.org/10.3390/microorganisms11040961
APA StyleCoyer, L., Sogan-Ekinci, A., Greutélaers, B., Kuhn, J., Saller, F. S., Hailer, J., Böhm, S., Brosch, R., Wagner-Wiening, C., & Böhmer, M. M. (2023). Knowledge, Attitudes and Behaviors regarding Tick-Borne Encephalitis Vaccination and Prevention of Tick-Borne Diseases among Primary Care Physicians in Bavaria and Baden-Wuerttemberg, Germany, May–September 2022. Microorganisms, 11(4), 961. https://doi.org/10.3390/microorganisms11040961