
Respiratory Syncytial Virus-Load Kinetics and Clinical Course of Acute Bronchiolitis in Hospitalized Infants: Interim Results and Review of the Literature
 , , ,
, , ,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Analysis of Study Patients’ Demographic and Clinical Characteristics
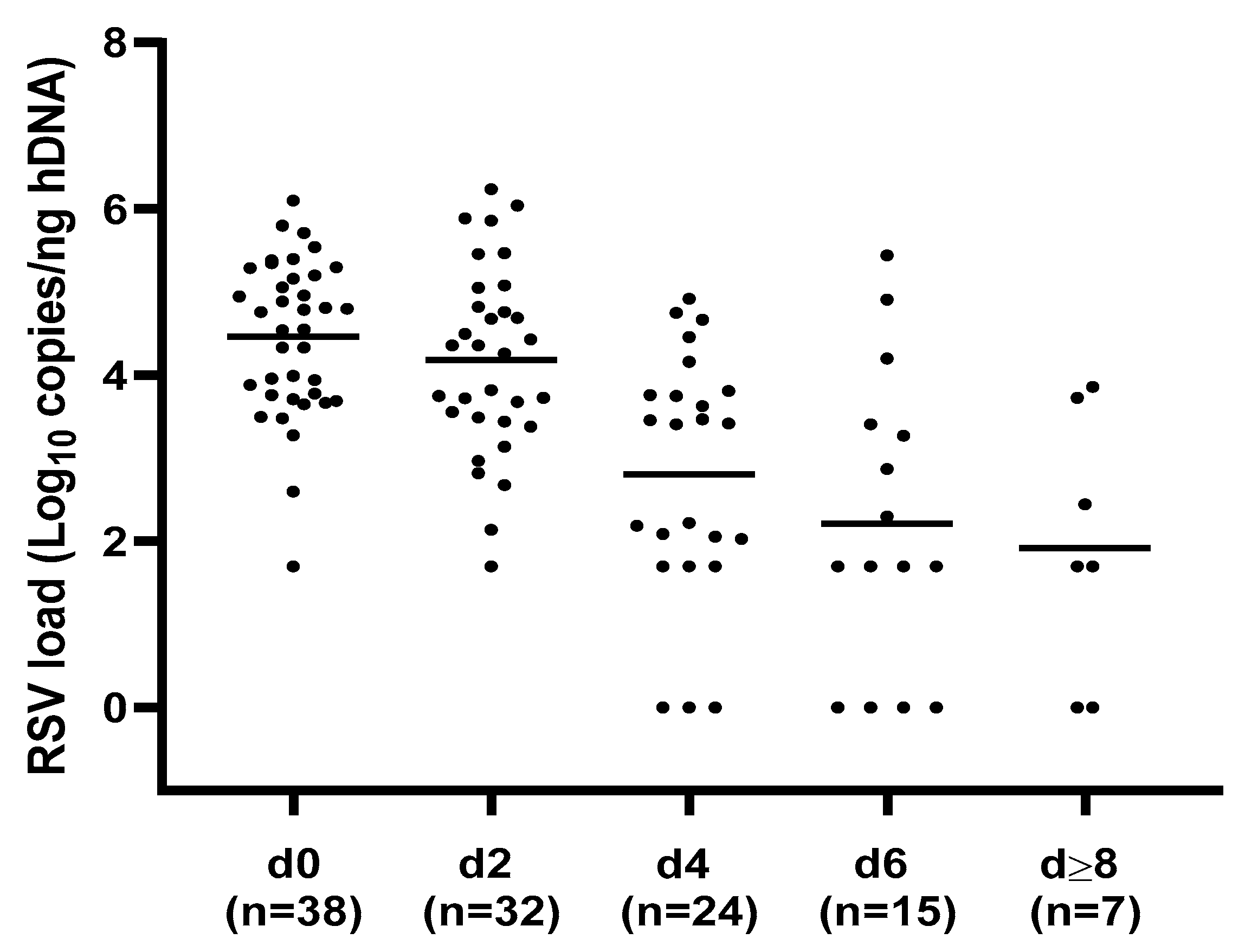
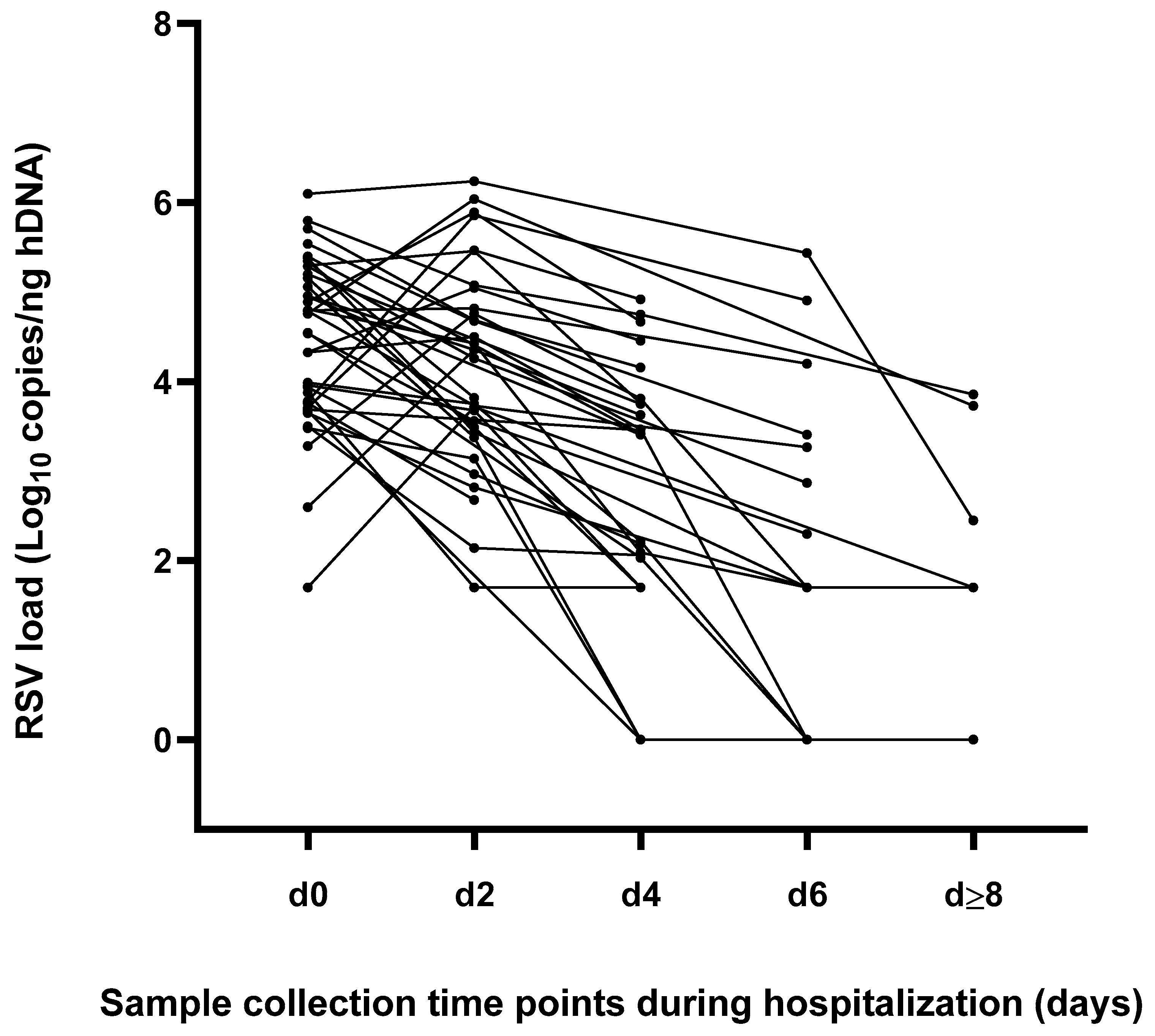
3.2. Analysis of RSV Load and Kinetics of Viral Replication during Hospitalization Independently by Bronchiolitis Clinical Course
3.3. Impact of RSV Load and Non-Viral Risk Factors (Patients’ Characteristics and Laboratory Findings) on the Disease Severity
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rima, B.; Collins, P. ICTV Virus Taxonomy Profile: Pneumoviridae. J. Gen. Virol. 2017, 98, 2912–2913. [Google Scholar] [CrossRef]
- Nair, H.; Nokes, D.J. Global burden of acute lower respiratory infections due to respiratory syncytial virus in young children: A systematic review and meta-analysis. Lancet 2010, 375, 1545–1555. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence: Bronchiolitis in Children. NG9. London: National Institute for Health and Clinical Excellence. 2021. Available online: https://www.nice.org.uk/guidance/ng9 (accessed on 22 January 2023).
- Manti, S.; Staiano, A. UPDATE—2022 Italian guidelines on the management of bronchiolitis in infants. Italy J. Pediatr. 2023, 49, 19. [Google Scholar] [CrossRef]
- Keam, S.J. Nirsevimab: First Approval. Drugs 2023, 83, 181–187. [Google Scholar] [CrossRef]
- Baraldi, E.; Lanari, M. Inter-society consensus document on treatment and prevention of bronchiolitis in newborns and infants. Italy J. Pediatr. 2014, 40, 65. [Google Scholar] [CrossRef]
- Garcia-Mauriño, C.; Moore-Clingenpeel, M. Viral Load Dynamics and Clinical Disease Severity in Infants with Respiratory Syncytial Virus Infection. J. Infect. Dis. 2019, 219, 1207–1215. [Google Scholar] [CrossRef]
- Hall, C.B.; Douglas, R.G. Respiratory syncytial virus infections in infants: Quantitation and duration of shedding. J. Pediatr. 1976, 89, 11–15. [Google Scholar] [CrossRef]
- Buckingham, S.C.; Bush, A.J. Nasal quantity of respiratory syncytial virus correlates with disease severity in hospitalized infants. Pediatr. Infect. Dis. J. 2000, 19, 113–117. [Google Scholar] [CrossRef]
- Wright, P.F.; Gruber, W.C. Illness severity, viral shedding, and antibody responses in infants hospitalized with bronchiolitis caused by respiratory syncytial virus. J. Infect. Dis. 2002, 185, 1011–1018. [Google Scholar] [CrossRef]
- DeVincenzo, J.P.; El Saleeby, C.M. Respiratory syncytial virus load predicts disease severity in previously healthy infants. J. Infect. Dis. 2005, 191, 1861–1868. [Google Scholar] [CrossRef]
- Fodha, I.; Vabret, A. Respiratory syncytial virus infections in hospitalized infants: Association between viral load, virus subgroup, and disease severity. J. Med. Virol. 2007, 79, 1951–1958. [Google Scholar] [CrossRef] [PubMed]
- Houben, M.L.; Coenjaerts, F.E. Disease severity and viral load are correlated in infants with primary respiratory syncytial virus infection in the community. J. Med. Virol. 2010, 82, 1266–1271. [Google Scholar] [CrossRef] [PubMed]
- El Saleeby, C.M.; Bush, A.J. Respiratory syncytial virus load, viral dynamics, and disease severity in previously healthy naturally infected children. J. Infect. Dis. 2011, 204, 996–1002. [Google Scholar] [CrossRef] [PubMed]
- Van Leeuwen, J.C.; Goossens, L.K. Equal virulence of rhinovirus and respiratory syncytial virus in infants hospitalized for lower respiratory tract infection. Pediatr. Infect. Dis. J. 2012, 31, 84–86. [Google Scholar] [CrossRef] [PubMed]
- Scagnolari, C.; Midulla, F. Evaluation of viral load in infants hospitalized with bronchiolitis caused by respiratory syncytial virus. Med. Microbiol. Immunol. 2012, 201, 311–317. [Google Scholar] [CrossRef]
- Zhou, L.; Xiao, Q. The impact of viral dynamics on the clinical severity of infants with respiratory syncytial virus bronchiolitis. J. Med. Virol. 2015, 87, 1276–1284. [Google Scholar] [CrossRef]
- Hasegawa, K.; Jartti, T. Respiratory syncytial virus genomic load and disease severity among children hospitalized with bronchiolitis: Multicenter cohort studies in the United States and Finland. J. Infect. Dis. 2015, 211, 1550–1559. [Google Scholar] [CrossRef]
- Skjerven, H.O.; Megremis, S. Virus Type and Genomic Load in Acute Bronchiolitis: Severity and Treatment Response with Inhaled Adrenaline. J. Infect. Dis. 2016, 213, 915–921. [Google Scholar] [CrossRef]
- Souza, A.P.; Leitão, L.A. Lack of association between viral load and severity of acute bronchiolitis in infants. J. Bras. Pneumol. 2016, 42, 261–265. [Google Scholar] [CrossRef]
- Yan, X.L.; Li, Y.N. Clinical characteristics and viral load of respiratory syncytial virus and human metapneumovirus in children hospitalized for acute lower respiratory tract infection. J. Med. Virol. 2017, 89, 589–597. [Google Scholar] [CrossRef]
- Espinosa, Y.; San Martín, C. Genomic Loads and Genotypes of Respiratory Syncytial Virus: Viral Factors during Lower Respiratory Tract Infection in Chilean Hospitalized Infants. Int. J. Mol. Sci. 2017, 18, 654. [Google Scholar] [CrossRef]
- Piedra, F.A.; Mei, M. The interdependencies of viral load, the innate immune response, and clinical outcome in children presenting to the emergency department with respiratory syncytial virus-associated bronchiolitis. PLoS ONE 2017, 12, e0172953. [Google Scholar] [CrossRef] [PubMed]
- Thwaites, R.S.; Coates, M. Reduced Nasal Viral Load and IFN Responses in Infants with Respiratory Syncytial Virus Bronchiolitis and Respiratory Failure. Am. J. Respir. Crit. Care Med. 2018, 198, 1074–1084. [Google Scholar] [CrossRef] [PubMed]
- De Paulis, M.; Oliveira, D.B.L. The importance of viral load in the severity of acute bronchiolitis in hospitalized infants. Clinics 2021, 76, e3192. [Google Scholar] [PubMed]
- Watanabe, R.A.S.; Cruz, J.S. Respiratory syncytial virus: Viral load, viral decay, and disease progression in children with bronchiolitis. Braz. J. Microbiol. 2022, 53, 1241–1247. [Google Scholar] [CrossRef] [PubMed]
- Basile, V.; Di Mauro, A. Lung ultrasound: A useful tool in diagnosis and management of bronchiolitis. BMC Pediatr. 2015, 15, 63. [Google Scholar] [CrossRef] [PubMed]
- Pierangeli, A.; Piralla, A. Multicenter epidemiological investigation and genetic characterization of respiratory syncytial virus and metapneumovirus infections in the pre-pandemic 2018–2019 season in northern and central Italy. Clin. Exp. Med. 2022, 15, 1–13. [Google Scholar] [CrossRef]
- Vandini, S.; Bottau, P. Immunological, Viral, Environmental, and Individual Factors Modulating Lung Immune Response to Respiratory Syncytial Virus. Biomed. Res. Int. 2015, 2015, 875723. [Google Scholar] [CrossRef]
- Moreel, L.; Proesmans, M. High flow nasal cannula as respiratory support in treating infant bronchiolitis: A systematic review. Eur. J. Pediatr. 2020, 179, 711–718. [Google Scholar] [CrossRef]
- Eden, J.S.; Sikazwe, C. Off-season RSV epidemics in Australia after easing of COVID-19 restrictions. Nat. Commun. 2022, 13, 2884. [Google Scholar] [CrossRef]
- Nenna, R.; Matera, L. An Italian Multicenter Study on the Epidemiology of Respiratory Syncytial Virus During SARS-CoV-2 Pandemic in Hospitalized Children. Front. Pediatr. 2022, 10, 930281. [Google Scholar] [CrossRef] [PubMed]
- Pruccoli, G.; Castagno, E. The Importance of RSV Epidemiological Surveillance: A Multicenter Observational Study of RSV Infection during the COVID-19 Pandemic. Viruses 2023, 15, 280. [Google Scholar] [CrossRef] [PubMed]
- Stera, G.; Pierantoni, L. Impact of SARS-CoV-2 Pandemic on Bronchiolitis Hospitalizations: The Experience of an Italian Tertiary Center. Children 2021, 8, 556. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Need of Oxygen Therapy | Type of Oxygen Therapy | Duration of Oxygen Therapy (hours) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Yes (n = 24) | No (n = 14) | p Value | HFNC (n = 5) | Low-Flow (n = 19) | p Value | ≤72 h (n = 13) | >72 h (n = 11) | p Value | |
| RSV load | |||||||||
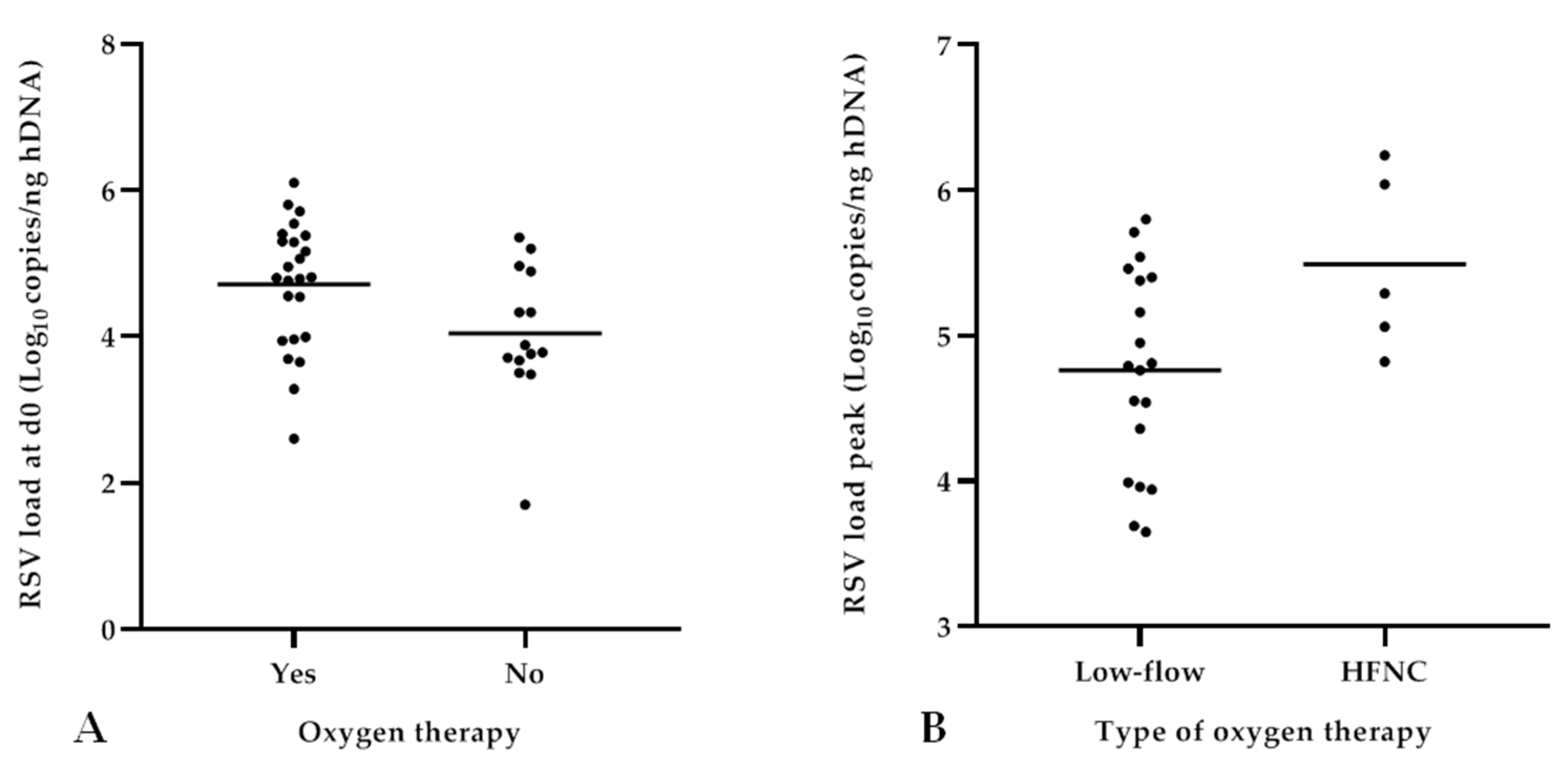
| d0 | 4.71 ± 0.87 | 4.04 ± 0.93 | 0.03 | 5.20 ± 0.55 | 4.58 ± 0.90 | 0.16 | 4.51 ± 0.93 | 4.95 ± 0.75 | 0.22 |
| d2 | 4.28 ± 0.95 | 4.03 ± 1.41 | 0.55 | 4.95 ± 1.20 | 4.06 ± 0.78 | 0.07 | 4.09 ± 1.22 | 4.47 ± 1.17 | 0.39 |
| d4 | 2.82 ± 1.24 | 2.78 ± 1.92 | 0.95 | n.e.$ | n.e.$ | n.e.$ | 3.01 ± 0.88 | 2.54 ± 1.71 | 0.49 |
| d6 | 2.36 ± 1.59 | 2.46 ± 3.47 | 0.95 | n.e.$ | n.e.$ | n.e.$ | 2.06 ± 1.25 | 2.27 ± 2.04 | 0.83 |
| Peak | 4.91 ± 0.73 | 4.59 ± 0.90 | 0.24 | 5.49 ± 0.62 | 4.76 ± 0.69 | 0.04 | 4.77 ± 0.62 | 5.08 ± 0.84 | 0.30 |
| ∆ d0–d2 | 0.44 ± 1.02 | −0.06 ± 1.46 | 0.26 | 0.25 ± 1.14 | 0.51 ± 1.01 | 0.64 | 0.37 ± 1.22 | 0.52 ± 0.83 | 0.75 |
| ∆ d0–d4 | 1.73 ± 1.50 | 1.33 ± 1.62 | 0.55 | n.e.$ | n.e.$ | n.e.$ | n.e.$ | n.e.$ | n.e.$ |
| Demographic characteristics | |||||||||
| Age (month) | 3.4 ± 2.9 | 4.8 ± 2.9 | 0.18 | 3.7 ± 2.9 | 3.4 ± 3.0 | 0.83 | 4.1 ± 3.4 | 2.7 ± 2.2 | 0.27 |
| Sex (male) | 12 | 7 | 1.00 | 3 | 9 | 1.00 | 8 | 4 | 0.41 |
| Ethnicity (total available n *) | (n * = 22) | (n = 14) | 0.04 | (n = 5) | (n * = 17) | n.e.§ | (n * = 11) | (n = 11) | n.e.§ |
| Caucasian | 20 | 8 | 5 | 15 | 10 | 10 | |||
| Asian | 1 | 1 | 0 | 1 | 0 | 1 | |||
| African-American | 1 | 5 | 0 | 1 | 1 | 0 | |||
| Clinical characteristics | |||||||||
| Premature birth (<37 WG) | 3 | 3 | 0.53 | 1 | 2 | 0.32 | 1 | 2 | 0.59 |
| Weight on admission (kg) | 5.6 ± 1.7 | 6.5 ± 1.8 | 0.17 | 6.0 ± 1.6 | 5.4 ± 1.8 | 0.52 | 5.9 ± 2.0 | 5.1 ± 1.4 | 0.29 |
| Breastfeeding | 19 | 13 | 0.26 | 3 | 16 | 0.27 | 12 | 7 | 0.14 |
| Duration of symptoms prior to d0 (days) | 3.5 ± 2.2 | 3.8 ± 2.0 | 0.75 | 2.8 ± 1.9 | 3.7 ± 2.3 | 0.45 | 4.2 ± 2.7 | 2.6 ± 1.3 | 0.08 |
| Laboratory findings at d0 | |||||||||
| White blood cells (×109 cell/L) | 10,787 ± 4,029 | 10,738 ± 4,003 | 0.97 | 12,868 ± 4,819 | 10,209 ± 3,731 | 0.2 | 9,499 ± 3,208 | 12,193 ± 4,498 | 0.11 |
| Neutrophils (×109 cell/L) | 4,792 [2,393–4,712] | 3,587 [2,659–5,966] | 0.26 | 6,419 [4,928–6,926] | 3,510 [2,245–5,272] | 0.06 | 3,728 [2,045–5,184] | 4,928 [3,144–6,713] | 0.21 |
| Basophils (×109 cell/L) | 29 [28–43] | 31 [22–54] | 0.87 | 32 [29–55] | 29 [20–51] | 0.53 | 29 [21–45] | 32 [27–58] | 0.65 |
| Eosinophils (×109 cell/L) | 39 [15–239] | 83 [22–126] | 0.47 | 96 [40–143] | 32 [12–97] | 0.22 | 28 [10–120] | 40 [31–120] | 0.37 |
| Lymphocytes (×109 cell/L) | 4,963 ± 2,402 | 5,483 ± 3,959 | 0.62 | 4,799 ± 2,480 | 5,008 ± 2,451 | 0.87 | 4,585 ± 2,050 | 5,375 ± 2,776 | 0.44 |
| Monocytes (×109 cell/L) | 1,040 ± 459 | 841 ± 239 | 0.15 | 1,303 ± 351 | 967 ± 466 | 0.15 | 913 ± 455 | 1,179 ± 4,441 | 0.17 |
| C-reactive protein (mg/dL) | 0.9 [0.04–9.7] | 0.9 [0.04–12.6] | 0.96 | 0.6 [0.2–1.6] | 1.0 [0–9.7] | 0.85 | 1.14 [0.04–4.11] | 0.59 [0.08–9.70] | 0.78 |
| LOS in Hospital (days) | BCS at Admission | |||||
|---|---|---|---|---|---|---|
| ≤5 (n = 23) | >5 (n = 15) | p Value | Mild BCS (n = 30) | Moderate BCS (n = 8) | p Value | |
| RSV load | ||||||
| d0 | 4.46 ± 0.89 | 4.47 ± 1.04 | 0.97 | 4.47 ± 1.01 | 4.45 ± 0.63 | 0.96 |
| d2 | 4.10 ± 1.04 | 4.29 ± 1.27 | 0.63 | 4.19 ± 1.01 | 4.17 ± 1.84 | 0.97 |
| d4 | 3.01 ± 1.49 | 2.32 ± 1.48 | 0.32 | 2.79 ± 1.63 | 2.87 ± 0.94 | 0.92 |
| d6 | 2.52 ± 094 | 2.10 ± 2.05 | 0.71 | 2.27 ± 1.81 | 1.97 ± 2.11 | 0.80 |
| Peak | 0.32 ± 1.20 | 0.17 ± 1.26 | 0.72 | 4.84 ± 0.79 | 4.63 ± 0.86 | 0.52 |
| ∆ d0–d2 | 4.76 ± 0.78 | 4.85 ± 0.85 | 0.73 | 0.25 ± 1.22 | 0.31 ± 1.29 | 0.91 |
| ∆ d0–d4 | n.e.$ | n.e.$ | n.e.$ | n.e.$ | n.e.$ | n.e.$ |
| Demographic characteristics | ||||||
| Age (month) | 4.8 ± 3.2 | 2.6 ± 2.1 | 0.03 | 3.8 ± 2.8 | 4.6 ± 3.6 | 0.5 |
| Sex (male) | 10 | 9 | 0.5 | 14 | 5 | 0.7 |
| Ethnicity (total available n *) | (n * = 21) | (n = 15) | n.e.§ | (n * = 29) | (n * = 7) | n.e.§ |
| Caucasian | 17 | 11 | 23 | 5 | ||
| Asian | 0 | 2 | 1 | 1 | ||
| African-American | 4 | 2 | 5 | 1 | ||
| Clinical characteristics | ||||||
| Premature birth (<37 WG) | 5 | 1 | 0.22 | 6 | 0 | n.e.$ |
| Weight on admission (kg) | 6.2 ± 2.0 | 5.4 ± 1.4 | 0.2 | 6.0 ± 1.8 | 5.6 ± 1.8 | 0.6 |
| Breastfeeding | 20 | 12 | 0.7 | 24 | 8 | 0.3 |
| Duration of symptoms prior to d0 (days) | 3.3 ± 1.9 | 3.9 ± 2.5 | 0.4 | 3.8 ± 2.3 | 2.9 ± 1.6 | 0.2 |
| Laboratory findings | ||||||
| White blood cells (×109 cell/L) | 10,438 ± 3,851 | 11,356 ± 4,245 | 0.5 | 10,366 ± 3,523 | 12,441 ± 5,441 | 0.2 |
| Neutrophils (×109 cell/L) | 3,874 [2,659–4,952] | 4,852 [1,898–6,499] | 0.6 | 3,874 [2,626–4,928] | 6,499 [2,850–8,400] | 0.2 |
| Basophils (×109 cell/L) | 29 [22–43] | 34 [29–61] | 0.9 | 29 [22–43] | 52 [38–58] | 0.04 |
| Eosinophils (×109 cell/L) | 37 [15–116] | 46 [29–232] | 0.3 | 40 [18–143] | 30 [15–126] | 0.7 |
| Lymphocytes (×109 cell/L) | 5,199 ± 3,515 | 5,066 ± 1,944 | 0.9 | 5,129 ± 3,194 | 5,239 ± 2,293 | 0.9 |
| Monocytes (×109 cell/L) | 836 ± 322 | 1,203 ± 432 | 0.01 | 965 ± 346 | 981 ± 618 | 0.9 |
| C-reactive protein (mg/dL) | 0.90 [0.21–1.44] | 0.80 [0.28–1.75] | 0.6 | 0.85 [0.16–1.43] | 2.06 [0.46–5.70] | 0.2 |
| RSV Load d0 | Peak | |||
|---|---|---|---|---|
| r * | p Value | r * | p Value | |
| Demographic characteristics | ||||
| Age (months) | −0.12 | 0.46 | 0.08 | 0.64 |
| Clinical characteristics | ||||
| Weight (kg) | −0.26 | 0.12 | −0.02 | 0.91 |
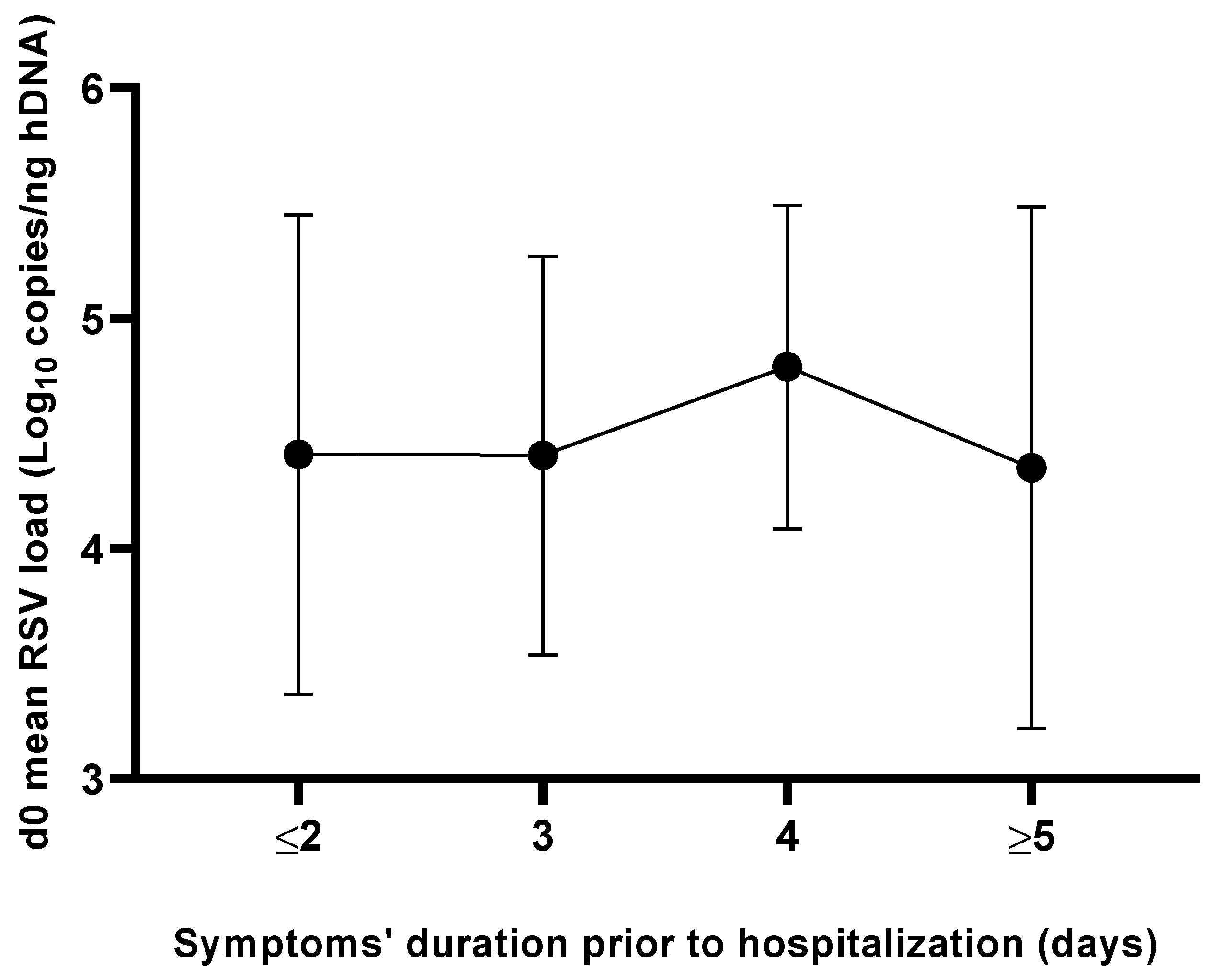
| Duration of symptoms prior to d0 (days) | −0.003 | 0.98 | 0.002 | 0.99 |
| Laboratory findings | ||||
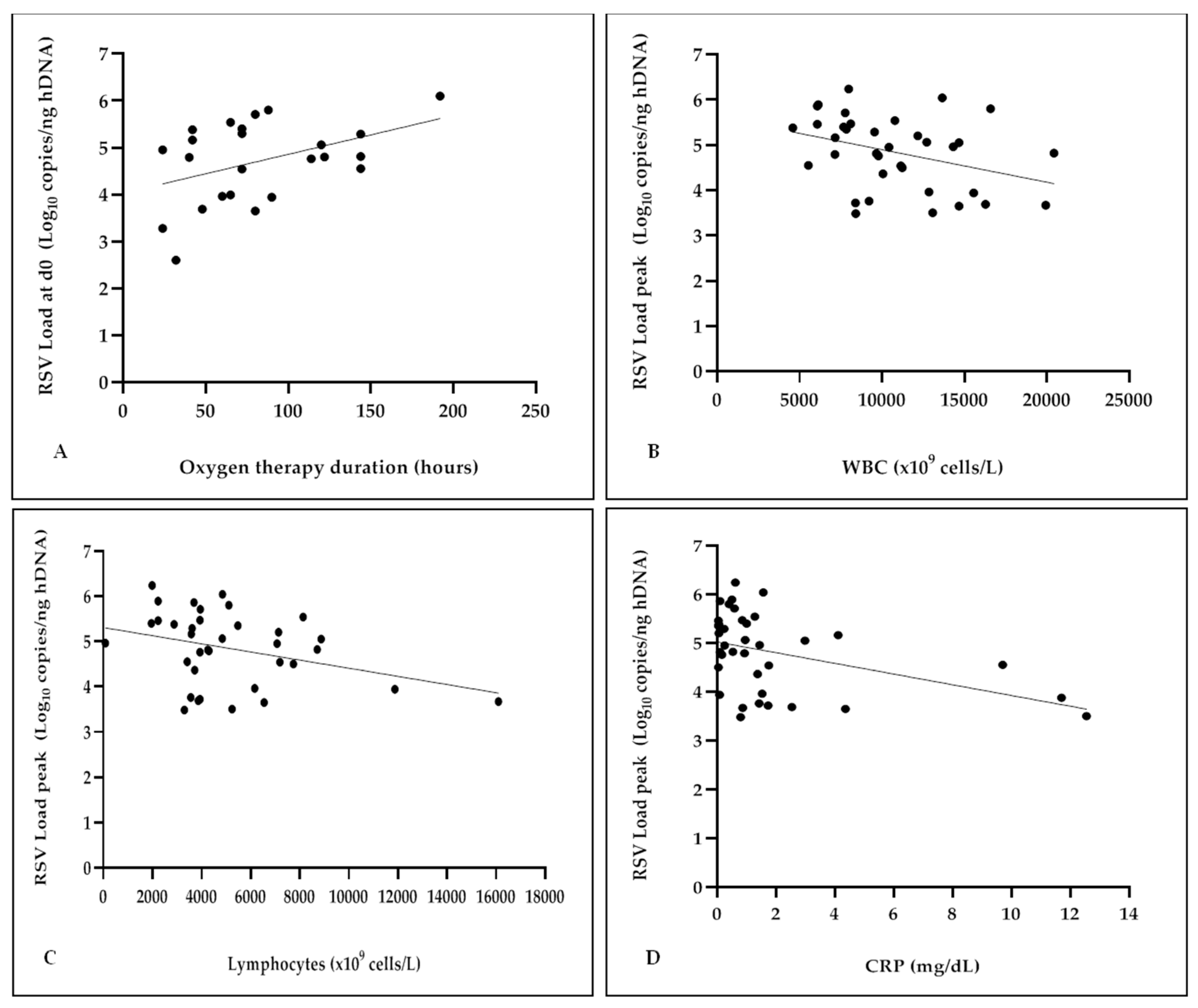
| White blood cells (×109 cell/L) | 0.14 | 0.41 | −0.35 | 0.03 |
| Neutrophils (×109 cell/L) | −0.06 | 0.72 | −0.14 | 0.43 |
| Basophils (×109 cell/L) | −0.1 | 0.57 | −0.23 | 0.17 |
| Eosinophils (×109 cell/L) | 0.09 | 0.59 | 0.08 | 0.62 |
| Lymphocytes (×109 cell/L) | −0.16 | 0.37 | −0.34 | 0.04 |
| Monocytes (×109 cell/L) | 0.09 | 0.59 | −0.02 | 0.91 |
| C-reactive protein (mg/dL) | −0.25 | 0.14 | −0.4 | 0.01 |
| Clinical outcomes | ||||
| Duration of oxygen therapy | 0.42 | 0.04 | 0.34 | 0.11 |
| LOS in the hospital | 0.11 | 0.49 | 0.09 | 0.61 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piccirilli, G.; Rocca, A.; Borgatti, E.C.; Gabrielli, L.; Zama, D.; Pierantoni, L.; Leone, M.; Totaro, C.; Pavoni, M.; Lazzarotto, T.; et al. Respiratory Syncytial Virus-Load Kinetics and Clinical Course of Acute Bronchiolitis in Hospitalized Infants: Interim Results and Review of the Literature. Pathogens 2023, 12, 645. https://doi.org/10.3390/pathogens12050645
Piccirilli G, Rocca A, Borgatti EC, Gabrielli L, Zama D, Pierantoni L, Leone M, Totaro C, Pavoni M, Lazzarotto T, et al. Respiratory Syncytial Virus-Load Kinetics and Clinical Course of Acute Bronchiolitis in Hospitalized Infants: Interim Results and Review of the Literature. Pathogens. 2023; 12(5):645. https://doi.org/10.3390/pathogens12050645
Chicago/Turabian StylePiccirilli, Giulia, Alessandro Rocca, Eva Caterina Borgatti, Liliana Gabrielli, Daniele Zama, Luca Pierantoni, Marta Leone, Camilla Totaro, Matteo Pavoni, Tiziana Lazzarotto, and et al. 2023. "Respiratory Syncytial Virus-Load Kinetics and Clinical Course of Acute Bronchiolitis in Hospitalized Infants: Interim Results and Review of the Literature" Pathogens 12, no. 5: 645. https://doi.org/10.3390/pathogens12050645
APA StylePiccirilli, G., Rocca, A., Borgatti, E. C., Gabrielli, L., Zama, D., Pierantoni, L., Leone, M., Totaro, C., Pavoni, M., Lazzarotto, T., & Lanari, M. (2023). Respiratory Syncytial Virus-Load Kinetics and Clinical Course of Acute Bronchiolitis in Hospitalized Infants: Interim Results and Review of the Literature. Pathogens, 12(5), 645. https://doi.org/10.3390/pathogens12050645