Exploring Children’s Physical Activity Behaviours According to Location: A Mixed-Methods Case Study



Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Data Processing and Statistical Analysis
3. Results
3.1. Children’s PA Levels
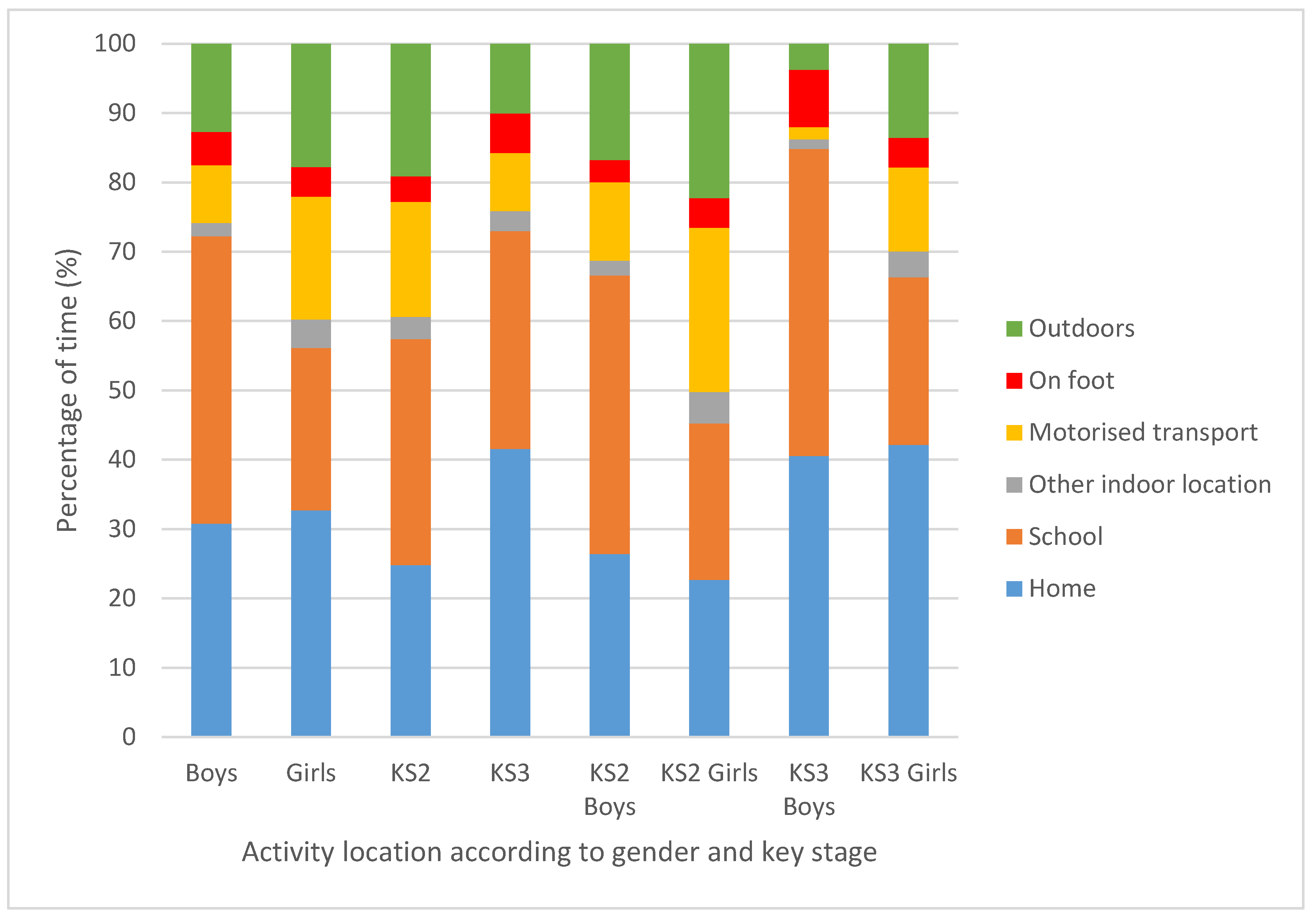
3.2. Time Spent in the Surrounding Environment.
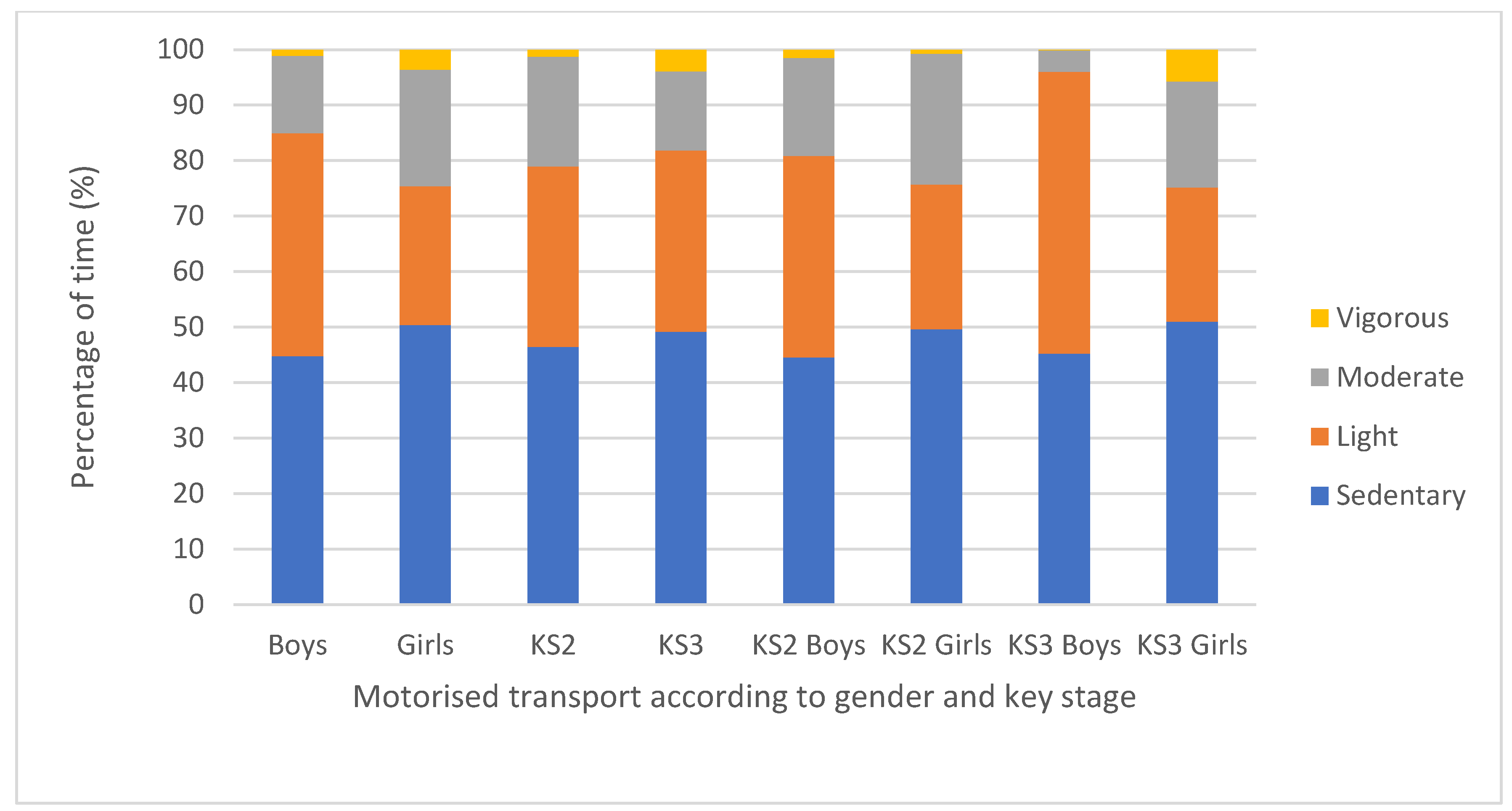
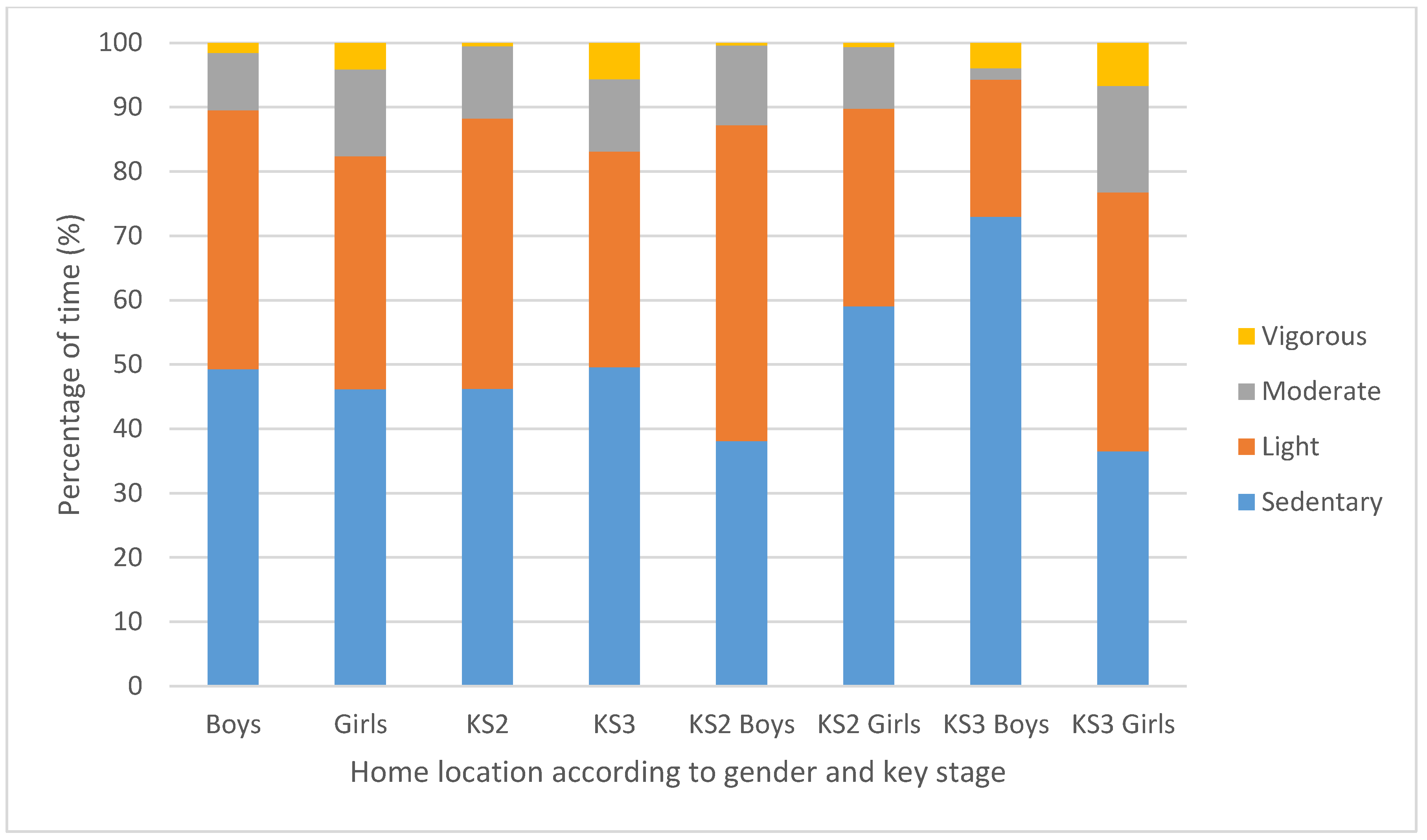
3.3. PA Intensities According to Location
3.4. PA Barriers and Facilitators
3.4.1. Barriers to PA (Categorised According to Relevant Social–Ecological Component)
‘Individual’ Component
‘Social Environment’ Component
‘Other’ Component
3.4.2. Facilitators for PA (Categorised According to Relevant Social–Ecological Component)
‘Individual’ Component
‘Physical Environment’ Component
‘Policy’ Component
‘Other’ Component
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Biddle, S.J.; Asare, M. Physical activity and mental health in children and adolescents: A review of reviews. Br. J. Sports Med. 2011, 45, 886–895. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; Leblanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2010, 7. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P. Interventions for Human Frailty: Physical Activity as a Model. Cold Spring Harb. Perspect. Med. 2016, 6. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.B.; Bugge, A.; Dencker, M.; Eiberg, S.; El-Naaman, B. The association between physical activity, physical fitness and development of metabolic disorders. Int. J. Pediatr. Obes. 2011, 6 (Suppl. 1), 29–34. [Google Scholar] [CrossRef]
- Hills, A.P.; Andersen, L.B.; Byrne, N.M. Physical activity and obesity in children. Br. J. Sports Med. 2011, 45, 866–870. [Google Scholar] [CrossRef]
- World Health Organisation. Global Recommendations on Physical Activity for Health; World Health Organisation: Geneva, Switzerland, 2011. [Google Scholar]
- Chief Medical Officers. UK Chief Medical Officers’ Physical Activity Guidelines; Department of Health: London, UK, 2019.
- Warburton, D.E.R.; Bredin, S.S.D. Reflections on Physical Activity and Health: What Should We Recommend? Can. J. Cardiol. 2016, 32, 495–504. [Google Scholar] [CrossRef]
- Smedegaard, S.; Christiansen, L.B.; Lund-Cramer, P.; Bredahl, T.; Skovgaard, T. Improving the well-being of children and youths: A randomized multicomponent, school-based, physical activity intervention. BMC Public Health 2016, 16, 1127. [Google Scholar] [CrossRef]
- Loprinzi, P.D.; Cardinal, B.J.; Loprinzi, K.L.; Lee, H. Benefits and environmental determinants of physical activity in children and adolescents. Obes. Facts 2012, 5, 597–610. [Google Scholar] [CrossRef]
- Telama, R. Tracking of physical activity from childhood to adulthood: A review. Obes. Facts 2009, 2, 187–195. [Google Scholar] [CrossRef]
- Schoeppe, S.; Duncan, M.J.; Badland, H.M.; Oliver, M.; Browne, M. Associations between children’s independent mobility and physical activity. BMC Public Health. 2014, 14. [Google Scholar] [CrossRef]
- Ekelund, U.; Luan, J.; Sherar, L.B.; Esliger, D.W.; Griew, P.; Cooper, A. Moderate to vigorous physical activity and sedentary time and cardiometabolic risk factors in children and adolescents. J. Am. Med. Assoc. 2012, 307. [Google Scholar] [CrossRef] [PubMed]
- Burkhalter, T.M.; Hillman, C.H. A narrative review of physical activity, nutrition, and obesity to cognition and scholastic performance across the human lifespan. Adv. Nutr. 2011, 2, 201S–206S. [Google Scholar] [CrossRef] [PubMed]
- Health and Social Care Information Centre. Health Survey for England 2016 Children’s Health; Health and Social Care Information Centre: Leeds, UK, 2017.
- British Heart Foundation. Active Lives Survey 2015-16: Year 1 Report; British Heart Foundation: London, UK, 2017. [Google Scholar]
- Telama, R.; Yang, X.; Viikari, J.; Valimaki, I.; Wanne, O.; Raitakari, O. Physical activity from childhood to adulthood: A 21-year tracking study. Am. J. Prev. Med. 2005, 28, 267–273. [Google Scholar] [CrossRef]
- Nader, P.R.; Bradley, R.H.; Houts, R.M.; McRitchie, S.L.; O’Brien, M. Moderate-to-vigorous physical activity from ages 9 to 15 years. JAMA 2008, 300, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Gray, C.; Gibbons, R.; Larouche, R.; Sandseter, E.B.; Bienenstock, A.; Brussoni, M.; Chabot, G.; Herrington, S.; Janssen, I.; Pickett, W.; et al. What Is the Relationship between Outdoor Time and Physical Activity, Sedentary Behaviour, and Physical Fitness in Children? A Systematic Review. Int. J. Environ. Res. Public Health 2015, 12, 6455–6474. [Google Scholar] [CrossRef] [PubMed]
- McMinn, A.M.; Griffin, S.J.; Jones, A.P.; van Sluijs, E.M. Family and home influences on children’s after-school and weekend physical activity. Eur. J. Public Health 2013, 23, 805–810. [Google Scholar] [CrossRef] [PubMed]
- Atkin, A.J.; Corder, K.; Ekelund, U.; Wijndaele, K.; Griffin, S.J.; van Sluijs, E.M. Determinants of change in children’s sedentary time. PLoS ONE 2013, 8, e67627. [Google Scholar] [CrossRef]
- Collings, P.J.; Wijndaele, K.; Corder, K.; Westgate, K.; Ridgway, C.L.; Dunn, V.; Goodyer, I.; Ekelund, U.; Brage, S. Levels and patterns of objectively-measured physical activity volume and intensity distribution in UK adolescents: The ROOTS study. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 23. [Google Scholar] [CrossRef]
- Collins, P.; Al-Nakeeb, Y.; Nevill, A.; Lyons, M. The impact of the built environment on young people’s physical activity patterns: A suburban-rural comparison using GPS. Int. J. Environ. Res. Public Health 2012, 9, 3030–3050. [Google Scholar] [CrossRef]
- Cooper, A.R.; Page, A.S.; Wheeler, B.W.; Hillsdon, M.; Griew, P.; Jago, R. Patterns of GPS measured time outdoors after school and objective physical activity in English children: The PEACH project. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 31. [Google Scholar] [CrossRef]
- Maddison, R.; Ni Mhurchu, C. Global positioning system: A new opportunity in physical activity measurement. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 73. [Google Scholar] [CrossRef] [PubMed]
- Moore, H.J.; Nixon, C.A.; Lake, A.A.; Douthwaite, W.; O’Malley, C.L.; Pedley, C.L.; Summerbell, C.D.; Routen, A.C. The environment can explain differences in adolescents’ daily physical activity levels living in a deprived urban area: Cross-sectional study using accelerometry, GPS, and focus groups. J. Phys. Act. Health 2014, 11, 1517–1524. [Google Scholar] [CrossRef] [PubMed]
- Oreskovic, N.M.; Blossom, J.; Field, A.E.; Chiang, S.R.; Winickoff, J.P.; Kleinman, R.E. Combining global positioning system and accelerometer data to determine the locations of physical activity in children. Geospat. Health 2012, 6, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Van Remoortel, H.; Giavedoni, S.; Raste, Y.; Burtin, C.; Louvaris, Z.; Gimeno-Santos, E.; Langer, D.; Glendenning, A.; Hopkinson, N.S.; Vogiatzis, I.; et al. Validity of activity monitors in health and chronic disease: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 84. [Google Scholar] [CrossRef] [PubMed]
- Åstrand, P.O. Textbook of Work Physiology: Physiological Bases of Exercise; Human Kinetics: Champaign, IL, USA, 2003. [Google Scholar]
- Troped, P.J.; Wilson, J.S.; Matthews, C.E.; Cromley, E.K.; Melly, S.J. The built environment and location-based physical activity. Am. J. Prev. Med. 2010, 38, 429–438. [Google Scholar] [CrossRef]
- Vu, M.B.; Murrie, D.; Gonzalez, V.; Jobe, J.B. Listening to girls and boys talk about girls’ physical activity behaviors. Health Educ. Behav. 2006, 33, 81–96. [Google Scholar] [CrossRef]
- Derrett, S.; Colhoun, S. Being a quantitative interviewer: Qualitatively exploring interviewers’ experiences in a longitudinal cohort study. BMC Med. Res. Methodol 2011, 11, 165. [Google Scholar] [CrossRef]
- Carlsen, B.; Glenton, C. What about N? A methodological study of sample-size reporting in focus group studies. BMC Med. Res. Methodol 2011, 11, 26. [Google Scholar] [CrossRef]
- Gibson, F. Conducting focus groups with children and young people: Strategies for success. J. Res. Nurs. 2007, 12, 473–483. [Google Scholar] [CrossRef]
- Department for Education. Schools, Pupils and Their Characteristics: January 2018; Department for Education: London, UK, 2018.
- Heyward, V.H. Advanced Fitness Assessment and Exercise Prescription, 6th ed.; Human Kinetics: Champaign, IL, USA, 2010. [Google Scholar]
- Maddison, R.; Jiang, Y.; Vander Hoorn, S.; Exeter, D.; Mhurchu, C.N.; Dorey, E. Describing patterns of physical activity in adolescents using global positioning systems and accelerometry. Pediatr. Exerc. Sci. 2010, 22, 392–407. [Google Scholar] [CrossRef]
- Bryman, A. Social Research Methods, 4th ed.; Oxford University Press: New York, NY, USA, 2012. [Google Scholar]
- McLeroy, K.R.; Bibeau, D.; Steckler, A.; Glanz, K. An ecological perspective on health promotion programs. Health Educ. Q. 1988, 15, 351–377. [Google Scholar] [CrossRef] [PubMed]
- Kenney, W.L.; Wilmore, J.; Costill, D. Physiology of Sport and Exercise, 6th ed.; Human Kinetics: Champaign, IL, USA, 2015. [Google Scholar]
- Kent, M. The Oxford Dictionary of Sports Science & Medicine; Oxford University Press: Oxford, UK, 2006. [Google Scholar]
- Jones, I.B.L.H.I. Qualitative Research in Sport and Physical Activity; Sage Publications: Thousand Oaks, CA, USA, 2012. [Google Scholar]
- Flick, U. An. Introduction to Qualitative Research; SAGE Publications: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Bull, F.C.; the Expert Working Group. Physical Activity Guidelines in the U.K.: Review and Recommendations; Loughborough University: Loughborough, UK, 2011. [Google Scholar]
- Ridgers, N.D.; Salmon, J.; Parrish, A.M.; Stanley, R.M.; Okely, A.D. Physical activity during school recess: A systematic review. Am. J. Prev. Med. 2012, 43. [Google Scholar] [CrossRef] [PubMed]
- Owen, C.G.; Nightingale, C.M.; Rudnicka, A.R.; Cook, D.G.; Ekelund, U.; Whincup, P.H. Ethnic and gender differences in physical activity levels among 9-10-year-old children of white European, South Asian and African-Caribbean origin: The Child Heart Health Study in England (CHASE Study). Int. J. Epidemiol. 2009, 38, 1082–1093. [Google Scholar] [CrossRef] [PubMed]
- Tudor-Locke, C.; Craig, C.L.; Beets, M.W.; Belton, S.; Cardon, G.M.; Duncan, S.; Hatano, Y.; Lubans, D.R.; Olds, T.S.; Raustorp, A.; et al. How many steps/day are enough? for children and adolescents. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 78. [Google Scholar] [CrossRef]
- Van Sluijs, E.M.; Skidmore, P.M.L.; Mwanza, K.; Jones, A.P.; Callaghan, A.M.; Ekelund, U.; Harrison, F.; Harvey, I.; Panter, J.; Wareham, N.J.; et al. Physical activity and dietary behaviour in a population based sample of British 10 year old children: The SPEEDY study. BMC Public Health 2008, 8, 388. [Google Scholar] [CrossRef]
- Mitchell, J.A.; Pate, R.R.; Beets, M.W.; Nader, P.R. Time spent in sedentary behavior and changes in childhood BMI: A longitudinal study from ages 9 to 15 years. Int. J. Obes. (Lond) 2013, 37. [Google Scholar] [CrossRef]
- Dumith, S.C.; Gigante, D.P.; Domingues, M.R.; Kohl, H.W., 3rd. Physical activity change during adolescence: A systematic review and a pooled analysis. Int. J. Epidemiol. 2011, 40, 685–698. [Google Scholar] [CrossRef]
- Trost, S.G.; Pate, R.R.; Sallis, J.F.; Freedson, P.S.; Taylor, W.C.; Dowda, M.; Sirard, J. Age and gender differences in objectively measured physical activity in youth. Med. Sci. Sports Exerc. 2002, 34, 350–355. [Google Scholar] [CrossRef]
- Smith, J.J.; Eather, N.; Morgan, P.J.; Plotnikoff, R.C.; Faigenbaum, A.D.; Lubans, D.R. The health benefits of muscular fitness for children and adolescents: A systematic review and meta-analysis. Sports Med. 2014, 44, 1209–1223. [Google Scholar] [CrossRef]
- Dishman, R.K.; Motl, R.W.; Saunders, R.; Felton, G.; Ward, D.S.; Dowda, M.; Pate, R.R. Enjoyment mediates effects of a school-based physical-activity intervention. Med. Sci. Sports Exerc. 2005, 37, 478–487. [Google Scholar] [CrossRef]
- Domville, M.; Watson, P.M.; Richardson, D.; Graves, L.E.F. Children’s perceptions of factors that influence PE enjoyment: A qualitative investigation. Phys. Educ. Sport Pedagog. 2019, 24, 207–219. [Google Scholar] [CrossRef]
- Pearce, M.; Saunders, D.H.; Allison, P.; Turner, A.P. Indoor and Outdoor Context-Specific Contributions to Early Adolescent Moderate to Vigorous Physical Activity as Measured by Combined Diary, Accelerometer, and GPS. J. Phys. Act. Health 2018, 15, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Haddad, J.; Ullah, S.; Bell, L.; Leslie, E.; Magarey, A. The Influence of Home and School Environments on Children’s Diet and Physical Activity, and Body Mass Index: A Structural Equation Modelling Approach. Matern. Child Health J. 2018, 22, 364–375. [Google Scholar] [CrossRef] [PubMed]
- Engelen, L.; Wyver, S.; Perry, G.; Bundy, A.; Chan, T.K.Y.; Ragen, J.; Bauman, A.; Naughton, G. Spying on children during a school playground intervention using a novel method for direct observation of activities during outdoor play. J. Adventure Educ. Outdoor Learn. 2018, 18, 86–95. [Google Scholar] [CrossRef]
- Fairclough, S.J.; McGrane, B.; Sanders, G.; Taylor, S.; Owen, M.; Curry, W. A non-equivalent group pilot trial of a school-based physical activity and fitness intervention for 10-11 year old english children: Born to move. BMC Public Health 2016, 16, 861. [Google Scholar] [CrossRef]
- Humpel, N.; Owen, N.; Leslie, E. Environmental factors associated with adults’ participation in physical activity: A review. Am. J. Prev. Med. 2002, 22, 188–199. [Google Scholar] [CrossRef]
- Evenson, K.R.; Wen, F.; Hillier, A.; Cohen, D.A. Assessing the contribution of parks to physical activity using global positioning system and accelerometry. Med. Sci. Sports Exerc. 2013, 45, 1981–1987. [Google Scholar] [CrossRef]
- Dunton, G.F.; Liao, Y.; Almanza, E.; Jerrett, M.; Spruijt-Metz, D.; Pentz, M.A. Locations of joint physical activity in parent-child pairs based on accelerometer and GPS monitoring. Ann. Behav. Med. 2013, 45 (Suppl. 1), S162–S172. [Google Scholar] [CrossRef]
- Chaix, B.; Kestens, Y.; Duncan, S.; Merrien, C.; Thierry, B.; Pannier, B.; Brondeel, R.; Lewin, A.; Karusisi, N.; Perchoux, C.; et al. Active transportation and public transportation use to achieve physical activity recommendations? A combined GPS, accelerometer, and mobility survey study. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 124. [Google Scholar] [CrossRef]
- Thierry, B.; Chaix, B.; Kestens, Y. Detecting activity locations from raw GPS data: A novel kernel-based algorithm. Int. J. Health Geogr. 2013, 12, 14. [Google Scholar] [CrossRef]
- Chaix, B.; Meline, J.; Duncan, S.; Merrien, C.; Karusisi, N.; Perchoux, C.; Lewin, A.; Labadi, K.; Kestens, Y. GPS tracking in neighborhood and health studies: A step forward for environmental exposure assessment, a step backward for causal inference? Health Place 2013, 21, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Ridgers, N.D.; Saint-Maurice, P.F.; Welk, G.J.; Siahpush, M.; Huberty, J. Differences in physical activity during school recess. J. Sch. Health 2011, 81. [Google Scholar] [CrossRef] [PubMed]
- Wan, N.; Wen, M.; Fan, J.X.; Tavake-Pasi, O.F.; McCormick, S.; Elliott, K.; Nicolosi, E. Physical Activity Barriers and Facilitators Among US Pacific Islanders and the Feasibility of Using Mobile Technologies for Intervention: A Focus Group Study With Tongan Americans. J. Phys. Act. Health 2017, 15, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Krops, L.A.; Hols, D.H.J.; Folkertsma, N.; Dijkstra, P.U.; Geertzen, J.H.B.; Dekker, R. Requirements on a community-based intervention for stimulating physical activity in physically disabled people: A focus group study amongst experts. Disabil. Rehabil. 2018, 40, 1–8. [Google Scholar] [CrossRef]
- Noonan, R.J.; Boddy, L.M.; Fairclough, S.J.; Knowles, Z.R. Write, draw, show, and tell: A child-centred dual methodology to explore perceptions of out-of-school physical activity. BMC Public Health 2016, 16, 326. [Google Scholar] [CrossRef]
- Carlin, A.; Murphy, M.H.; Gallagher, A.M. Current influences and approaches to promote future physical activity in 11-13 year olds: A focus group study. BMC Public Health 2015, 15, 1270. [Google Scholar] [CrossRef]
- Beighle, A.; Erwin, H.; Morgan, C.F.; Alderman, B. Children’s in-school and out-of-school physical activity during two seasons. Res. Q Exerc. Sport 2012, 83, 103–107. [Google Scholar] [CrossRef]
- Belanger, M.; Gray-Donald, K.; O’Loughlin, J.; Paradis, G.; Hanley, J. Influence of weather conditions and season on physical activity in adolescents. Ann. Epidemiol. 2009, 19, 180–186. [Google Scholar] [CrossRef]
- Krenn, P.J.; Titze, S.; Oja, P.; Jones, A.; Ogilvie, D. Use of global positioning systems to study physical activity and the environment: A systematic review. Am. J. Prev. Med. 2011, 41. [Google Scholar] [CrossRef]
- Biddle, S.J.; Gorely, T.; Pearson, N.; Bull, F.C. An assessment of self-reported physical activity instruments in young people for population surveillance: Project ALPHA. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 1. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Key Stage (and Age Range) | Boys | Girls | Total |
|---|---|---|---|
| 2 (School Years 5–6, 9–11 years of age) | 42 | 32 | 74 |
| 3 (School Years 7–8, 11–13 years of age) | 15 | 30 | 45 |
| Total | 57 | 62 | 119 |
| Variable | SB (min) Percentage SB Time (%) | LPA (min) Percentage LPA Time (%) | MPA (min) Percentage MPA Time (%) | VPA (min) Percentage VPA Time (%) | MVPA (min) Percentage MVPA Time (%) | Meeting PA Guidelines | |
|---|---|---|---|---|---|---|---|
| No. Children | Percent of Children (%) | ||||||
| Boys | 207.6 (±122.4) | 200.9 (±146) | 53.9 (±52.9) | 14.6 (±24) | 68.6 (±63.8) | 16 | 52 |
| 45.7% (±25.4%) | 39.6% (±19.8%) | 11.7% (±10.2%) | 2.8% (±3.5%) | 13.8% (±11.2%) | |||
| Girls | 204.4 (±138.8) | 172.9 (±143.1) | 91.9 (±103.6) | 15 (±30.3) | 106.9 (±117.5) | 15 | 48 |
| 45.3% (±28.9%) | 33.6% (±23%) | 17.9% (±19.5%) | 3.1% (±6.4%) | 20.9% (±22%) | |||
| KS2 (9–11 years) | 216 (±143) | 183.1 (±145.4) | 64 (±62.4) | 13.2 (±18.2) | 77.2 (±72.7) | 18 | 58 |
| 46.2% (±27.3%) | 36.5% (±23%) | 14% (±12.5%) | 2.9% (±4.5%) | 16.5% (±14.6%) | |||
| KS3 (11–13 years) | 191.8 (±110.6) | 191 (±144.7) | 87 (±108.4) | 17.1 (±36.6) | 104 (±122.5) | 13 | 42 |
| 44.4% (±27.2%) | 36.4% (±20%) | 16.2% (±20%) | 3% (±6) | 18.8% (±21.9%) | |||
| KS2 Boys | 183.6 (±119.6) | 204.1 (±143.3) | 59.3 (±53.8) | 13.3 (±14.2) | 72.6 (±63.5) | 11 | 35 |
| 40.5 (±24.1) | 42.6 (±20.1) | 13.6 (±10.9) | 2.8 (±2.8) | 15.7% (±12.1%) | |||
| KS2 Girls | 259.2 (±163.6) | 155.2 (±148.3) | 70.1 (±73.8) | 13.1 (±23) | 83.3 (±85.5) | 7 | 23 |
| 53.9 (±30.1) | 28.4 (±24.4) | 14.4 (±14.7) | 3.1 (±6.2) | 17.6% (±17.8%) | |||
| KS3 Boys | 260.9 (±117.5) * | 193.7 (±160.3) | 41.9 (±51.6) | 17.6 (±39) | 59.5 (±67.3) | 5 | 16 |
| 57.1 (±25.6) | 32.9 (±18.2) | 7.3 (±7.4) | 2.7 (±4.8) | 9.6% (±8.5%) | |||
| KS3 Girls | 153 (±87.9) * | 189.5 (±140.7) | 112.3 (±124.4) | 16.8 (±36.5) | 129 (±140.5) | 8 | 26 |
| 37.2 (±26) | 38.4 (±21.3) | 21.2 (±23.1) | 3.2 (±6.8) | 24% (±25.6%) | |||
| Overall | 205.9 (±130) | 186.4 (±143.9) | 73.5 (±84.6) | 14.8 (±27.2) | 88.4 (±96.6) | 31 | 100 |
| 45.5% (±27%) | 36.5% (±21.6%) | 14.9% (±15.9%) | 2.9% (±5.2%) | 17.5% (±17.9%) | |||
| Variable | Home | School | Other Indoor Location | Motorised Transport | On Foot | Outdoors (Not Including ‘On Foot’) | Outside (Combining ‘On Foot’ and ‘Outdoors’) |
|---|---|---|---|---|---|---|---|
| Boys | 30.8 (±23.1) | 41.4 (±22.7) ** | 1.9 (±3.8) | 8.3 (±12.4) * | 4.8 (5.8) | 12.7 (±11.8) | 15.5 (±10.8) |
| Girls | 32.7 (±7.5) | 23.4 (±26.4) ** | 4.1 (±8.9) | 17.7 (±17.6) * | 4.3 (5.8) | 17.8 (±14.8) | 17.4 (±13.2) |
| KS2 (9–11 years) | 24.8 (±21.2) * | 32.6 (±25) | 3.2 (±8.4) | 16.6 (±18.4) * | 3.7 (±4.9) | 19.1 (±12.7) ** | 19.4 (±13.2) * |
| KS3 (11–13 years) | 41.6 (±27.7) * | 31.4 (±28) | 2.9 (±4.4) | 8.4 (±10) * | 5.7 (±6.8) | 10 (±13) ** | 12.4 (±8.8) * |
| KS2 Boys | 26.4 (±21.9) | 40.2 (±23.8) * | 2.1 (±4.2) | 11.3 (±13.9) * | 3.2 (±3.8) | 16.8 (±10.9) | 17.3 (±11.3) |
| KS2 Girls | 22.7 (±20.9) | 22.5 (±23.8) * | 4.6 (±12) | 23.7 (±21.6) * | 4.3 (±6) | 22.2 (±14.6) | 22.3 (±15.4) |
| KS3 Boys | 40.5 (±24) | 44.3 (±21.2) | 1.4 (±2.7) | 1.7 (±2.4) * | 8.3 (±8.1) | 3.7 (±8.5) | 11.5 (±9) |
| KS3 Girls | 42.2 (±30.3) | 24.2 (±29.4) | 3.7 (±4.9) | 12 (±10.8) * | 4.3 (±5.7) | 13.6 (±14.1) | 12.8 (±8.9) |
| Overall | 31.8 (±25.3) | 32.1 (±26.1) | 3.1 (±7) | 13.2 (±15.9) | 4.5 (±5.8) | 15.3 (±13.5) | 16.5 (±12) |
| Themes | Selected Quotes From Children | |
|---|---|---|
| Barriers to PA | Facilitators for PA | |
| Individual | ||
| Time | “If I have too much homework, exams and stuff.” | “… however long you do on a physical activity, you get half that time on technologyor something like that” |
| Fitness/Health | “If you’re ill” | “I don’t want to be all weaker when I’m older, I want to stay healthy” |
| Fun and enjoyment | “They might not like it, so they might not want to do it.” | “I do it because I like dancing and it just makes me happy” |
| Equipment cost | “… if they don’t have like the right equipment to do it.” | “Maybe lower the price a little bit so that people don’t have to wait loads to save up” |
| Social Environment | ||
| Friends and family | “Might have to look after their family and it might stops [sic]you having their social time with their friends and going out” | “I do runs with my dad, I go on my bike” |
| Socialise | “… sometimes some of the people might have other plans” | “It’s a chance to meet up with friends” |
| Physical Environment | ||
| Location/Environment | “Not exercising and getting outside.” | “I go up to the college car park because it’s big and loads of my friends just play there.” |
| Club | “… have to be good at it to go there and stay there” | “… because that’s where the club [is], it’s what I do and I’m a part of that team” |
| Facilities | “That’s where you play, that’s the home ground or your home team. You have to go there.” | “There’s trampolining at, I can’t remember the school now but it’s a high school.” |
| Policy | ||
| Rewards | “…make it into like a fun game and whoever did the most exercise in that period of time would get a prize or something like that.” | “… in periods of time when who does the most exercise you win a prize, so you’re kind of pushing the students to work for the prize.” |
| Promotion | - | “… put a word on Facebook and tell people what’s happening and let everyone know happening and try and bring some people down to it.” |
| Child Voice | “People might not like what the variety is” | “You can ask what they like the most, and start clubs and get them to come.” |
| Awareness | - | “Like do a survey to see what they would want to do instead of like saying we’re going to do hockey today because some people might not like it.” |
| Other | ||
| Weather | “… if it’s in the winter, some people don’t have motivation because it’s quite cold and dark, and if it’s muddy.” | “… you need the activity, the exercise and the nice fresh air, instead of being stuck indoors, stuff like that.” |
| Technology | “When you’ve got a phone or like a console, you don’t think as much about getting active, you just want to play on them.” | “You could reduce your time down on a tablet or computer so that you’re not always on it.” |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khawaja, I.; Woodfield, L.; Collins, P.; Benkwitz, A.; Nevill, A. Exploring Children’s Physical Activity Behaviours According to Location: A Mixed-Methods Case Study. Sports 2019, 7, 240. https://doi.org/10.3390/sports7110240
Khawaja I, Woodfield L, Collins P, Benkwitz A, Nevill A. Exploring Children’s Physical Activity Behaviours According to Location: A Mixed-Methods Case Study. Sports. 2019; 7(11):240. https://doi.org/10.3390/sports7110240
Chicago/Turabian StyleKhawaja, Irfan, Lorayne Woodfield, Peter Collins, Adam Benkwitz, and Alan Nevill. 2019. "Exploring Children’s Physical Activity Behaviours According to Location: A Mixed-Methods Case Study" Sports 7, no. 11: 240. https://doi.org/10.3390/sports7110240
APA StyleKhawaja, I., Woodfield, L., Collins, P., Benkwitz, A., & Nevill, A. (2019). Exploring Children’s Physical Activity Behaviours According to Location: A Mixed-Methods Case Study. Sports, 7(11), 240. https://doi.org/10.3390/sports7110240