
Multicomponent Exercise and Functional Fitness: Strategies for Fall Prevention in Aging Women

 ,
,  ,
, 
 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
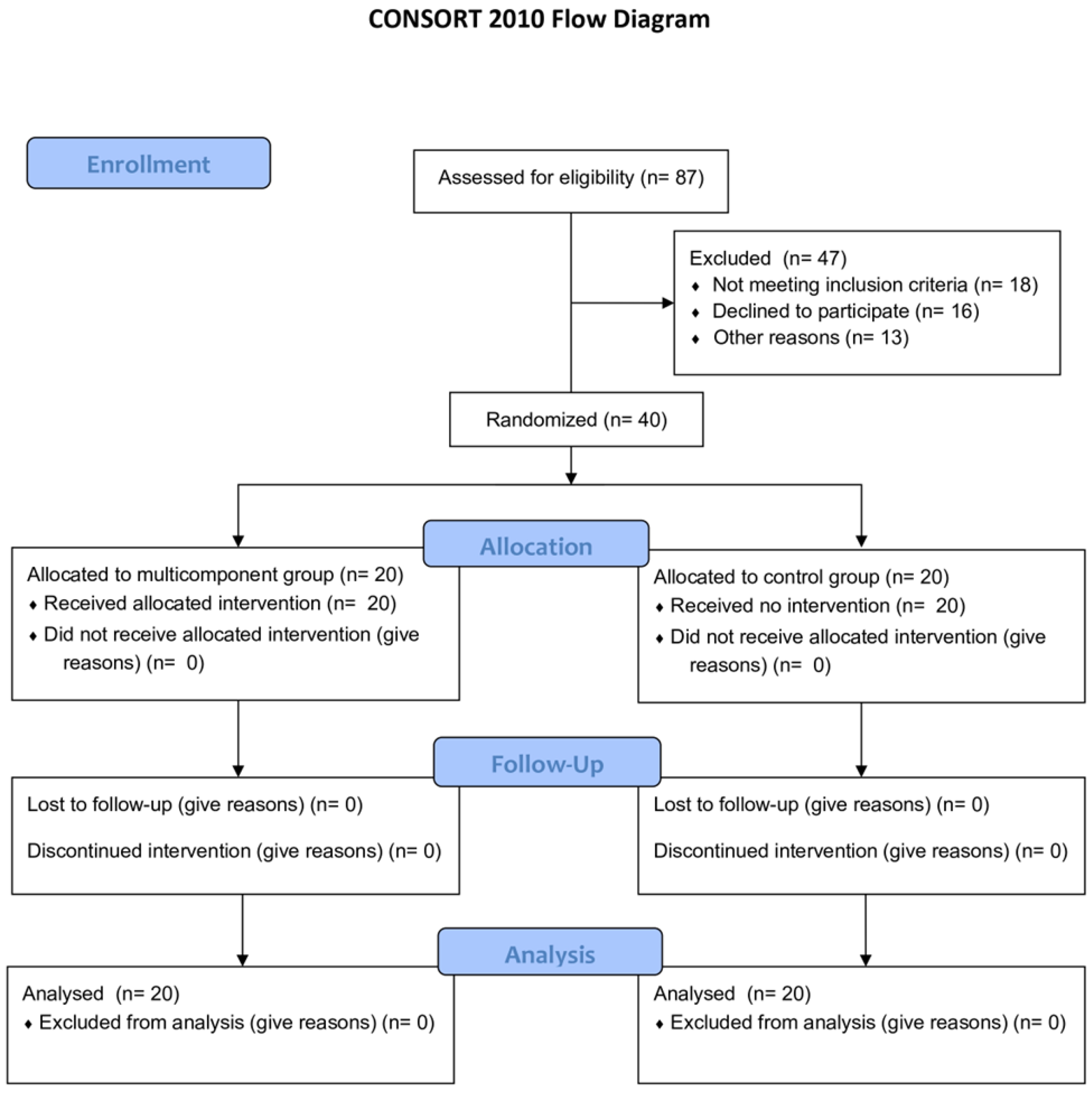
2.1. Study Design
2.2. Sample
2.3. Procedures
2.3.1. Anthropometry and Body Composition
2.3.2. Assessment of Functional Fitness
- Lower limb strength: 30 s chair stand test, measuring the number of full stands from a seated position.
- Upper limb strength: arm curl test using a 2 kg dumbbell, counting the number of repetitions performed in 30 s.
- Lower body flexibility: chair sit-and-reach test, with the distance (in centimeters) measured between the extended fingertips and the toes.
- Upper body flexibility: back scratch test, measuring the distance (in centimeters) between the middle fingers of each hand.
- Agility: Timed Up and Go (TUG) test, which records the time (in seconds) required to stand up from a chair, walk 3 m, turn around, return, and sit down.
- Aerobic endurance: 2 min step test, counting the number of steps completed while raising the knees to hip level.
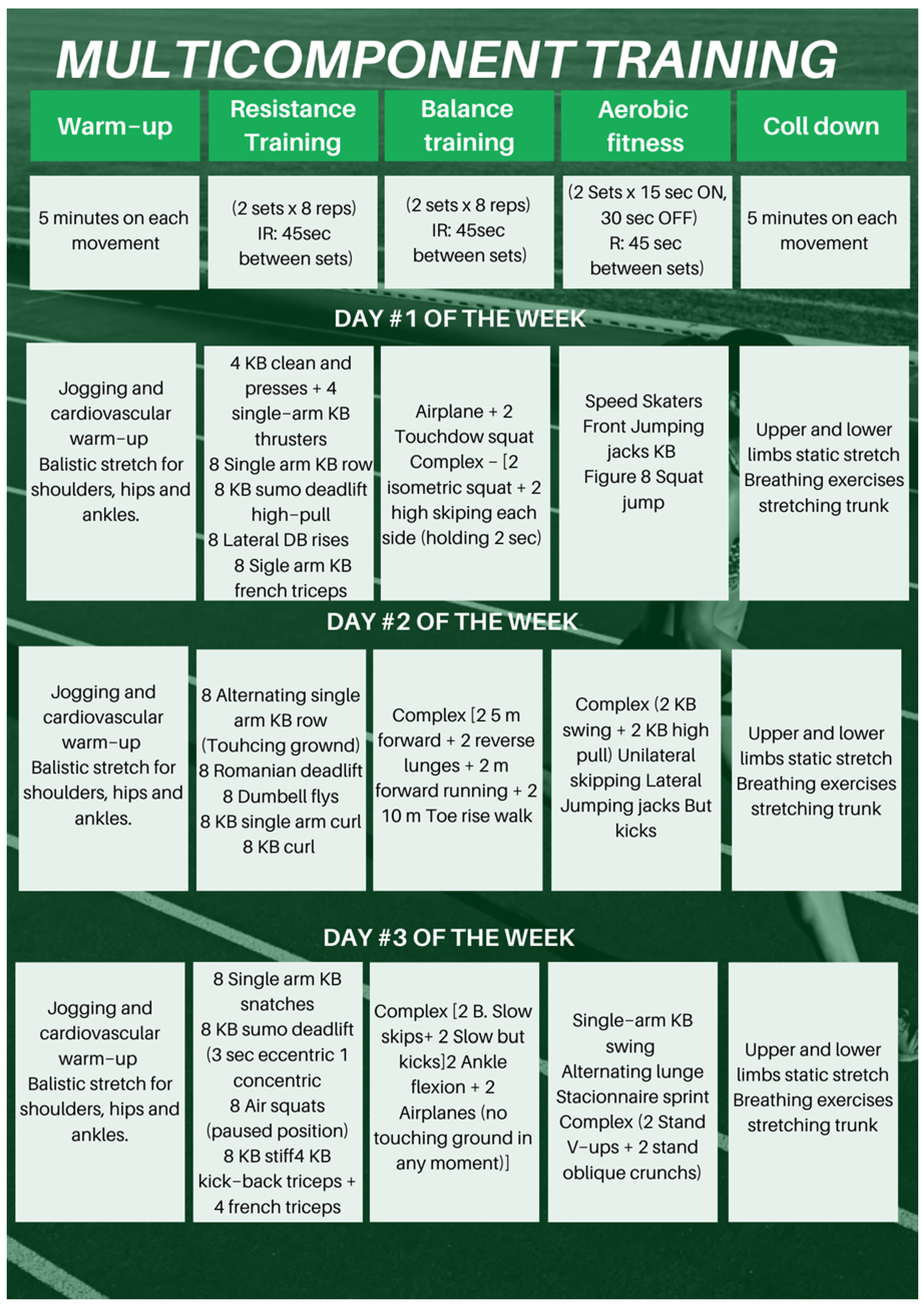
2.3.3. Multicomponent Training Program
- Warm-up (10 min): dynamic stretches, mobility exercises, and light jogging.
- Strength training (20 min): exercises using free weights, dumbbells, and kettlebells, targeting major muscle groups including upper limbs, lower limbs, and core.
- Balance and coordination training (10 min): activities such as single-leg exercises, plyometric movements, and tasks involving unstable surfaces.
- Aerobic training (15 min): dynamic and rhythmic movements like lateral jumps, jumping jacks, running in place, and heel raises.
- Cool-down (5 min): static stretches for upper and lower limbs and trunk, plus guided breathing exercises.
2.3.4. Pre-Test and Post-Test Evaluations
2.3.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ismail, Z.; Ahmad, W.I.W.; Hamjah, S.H.; Astina, I.K. The Impact of Population Ageing: A Review. Iran. J. Public Health 2021, 50, 2451–2460. [Google Scholar] [CrossRef] [PubMed]
- Ageing and Health [Internet]. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 20 December 2024).
- Bárrios, M.J.; Marques, R.; Fernandes, A.A. Aging with health: Aging in place strategies of a Portuguese population aged 65 years or older. Rev. Saude Publica 2020, 54, 129. [Google Scholar] [CrossRef]
- Ageing Europe—Statistics on Population Developments [Internet]. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Ageing_Europe_-_statistics_on_population_developments (accessed on 14 March 2025).
- Rony, M.K.K.; Parvin, M.R.; Wahiduzzaman, M.d.; Akter, K.; Ullah, M. Challenges and Advancements in the Health-Related Quality of Life of Older People. Adv. Public Health 2024, 2024, 8839631. [Google Scholar] [CrossRef]
- Dharmarajan, T.S. Physiology of Aging. In Geriatr Gastroenterol; Pitchumoni, C.S., Dharmarajan, T.S., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 1–54. Available online: https://doi.org/10.1007/978-3-319-90761-1_5-1 (accessed on 14 March 2025).
- Larsson, L.; Degens, H.; Li, M.; Salviati, L.; Lee, Y.I.; Thompson, W.; Kirkland, J.L.; Sandri, M. Sarcopenia: Aging-Related Loss of Muscle Mass and Function. Physiol. Rev. 2019, 99, 427–511. [Google Scholar] [CrossRef] [PubMed]
- Mi, B.; Xiong, Y.; Knoedler, S.; Alfertshofer, M.; Panayi, A.C.; Wang, H.; Lin, S.; Li, G.; Liu, G. Ageing-related bone and immunity changes: Insights into the complex interplay between the skeleton and the immune system. Bone Res. 2024, 12, 42. [Google Scholar] [CrossRef]
- Völter, C.; Thomas, J.P.; Maetzler, W.; Guthoff, R.; Grunwald, M.; Hummel, T. Sensory Dysfunction in Old Age. Dtsch. Ärzteblatt Int. 2021, 118, 512–520. [Google Scholar] [CrossRef]
- Seidler, R.D.; Bernard, J.A.; Burutolu, T.B.; Fling, B.W.; Gordon, M.T.; Gwin, J.T.; Kwak, Y.; Lipps, D.B. Motor Control and Aging: Links to Age-Related Brain Structural, Functional, and Biochemical Effects. Neurosci. Biobehav. Rev. 2010, 34, 721–733. [Google Scholar] [CrossRef] [PubMed]
- Kohler, R.; Rorato, P.; Braga, A.L.F.; Velho, R.B.; Krause, M.P. Effects of Aging and Exercise on the Cardiorespiratory Fitness of Older Women. Rev. Bras. Geriatr. Gerontol. 2016, 19, 603–612. [Google Scholar] [CrossRef]
- Ferrucci, L.; Cooper, R.; Shardell, M.; Simonsick, E.M.; Schrack, J.A.; Kuh, D. Age-Related Change in Mobility: Perspectives from Life Course Epidemiology and Geroscience. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2016, 71, 1184–1194. [Google Scholar] [CrossRef]
- Oduro, J.K.; Okyere, J.; Nyador, J.K.M.T. Risky health behaviours and chronic conditions among aged persons: Analysis of SAGE selected countries. BMC Geriatr. 2023, 23, 145. [Google Scholar] [CrossRef]
- Montero-Odasso, M.; Van Der Velde, N.; Martin, F.C.; Petrovic, M.; Tan, M.P.; Ryg, J.; Aguilar-Navarro, S.; Alexander, N.B.; Becker, C.; Blain, H.; et al. World guidelines for falls prevention and management for older adults: A global initiative. Age Ageing 2022, 51, afac205. [Google Scholar] [CrossRef] [PubMed]
- Dionyssiotis, Y. Analyzing the problem of falls among older people. Int. J. Gen. Med. 2012, 5, 805–813. [Google Scholar] [CrossRef]
- Cunningham, C.; O’Sullivan, R.; Caserotti, P.; Tully, M.A. Consequences of physical inactivity in older adults: A systematic review of reviews and meta-analyses. Scand. J. Med. Sci. Sports 2020, 30, 816–827. [Google Scholar] [CrossRef] [PubMed]
- Langhammer, B.; Bergland, A.; Rydwik, E. The Importance of Physical Activity Exercise Among Older People. BioMed Res. Int. 2018, 2018, 7856823. [Google Scholar] [CrossRef] [PubMed]
- Vaishya, R.; Vaish, A. Falls in Older Adults are Serious. Indian J. Orthop. 2020, 54, 69–74. [Google Scholar] [CrossRef]
- Berg, R.L.; Cassells, J.S. Falls in Older Persons: Risk Factors and Prevention. In The Second Fifty Years: Promoting Health and Preventing Disability; National Academies Press (US): Washington, DC, USA, 1992. Available online: https://www.ncbi.nlm.nih.gov/books/NBK235613/ (accessed on 14 March 2025).
- Giovannini, S.; Brau, F.; Galluzzo, V.; Santagada, D.A.; Loreti, C.; Biscotti, L.; Laudisio, A.; Zuccala, G.; Bernabei, R. Falls Among Older Adults: Screening, Identification, Rehabilitation, and Management. Appl. Sci. 2022, 12, 7934. [Google Scholar] [CrossRef]
- Lee, D.; Tak, S.H. A concept analysis of fear of falling in older adults: Insights from qualitative research studies. BMC Geriatr. 2023, 23, 651. [Google Scholar] [CrossRef]
- Ferreira, C.R.; Mascarenhas-Melo, F.; Rodrigues, A.R.; Lima, M.J.R.; Pinheiro, J.P.; Chaves, C.; Teixeira-Lemos, E.; Bell, V. Characterisation of institutionalised Portuguese older adult fallers: Is there a place for pharmacist intervention? A preliminary study. Pharm. Pract. 2022, 20, 2717. [Google Scholar] [CrossRef]
- Fuller, G.F. Falls in the elderly. Am. Fam. Physician 2000, 61, 2159–2168. [Google Scholar]
- Tropeções, Quedas e Trambolhões [Internet]. Available online: https://www.sns.gov.pt/noticias/2017/12/19/tropecoes-quedas-e-trambolhoes/ (accessed on 14 March 2025).
- Chidume, T. Promoting older adult fall prevention education and awareness in a community setting: A nurse-led intervention. Appl. Nurs. Res. 2021, 57, 151392. [Google Scholar] [CrossRef]
- Garatachea, N.; Pareja-Galeano, H.; Sanchis-Gomar, F.; Santos-Lozano, A.; Fiuza-Luces, C.; Morán, M.; Emanuele, E.; Joyner, M.J.; Lucia, A. Exercise attenuates the major hallmarks of aging. Rejuvenation Res. 2015, 18, 57–89. [Google Scholar] [CrossRef]
- Sun, M.; Min, L.; Xu, N.; Huang, L.; Li, X. The Effect of Exercise Intervention on Reducing the Fall Risk in Older Adults: A Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2021, 18, 12562. [Google Scholar] [CrossRef]
- Sherrington, C.; Fairhall, N.; Kwok, W.; Wallbank, G.; Tiedemann, A.; Michaleff, Z.A.; Ng, C.A.; Bauman, A. Evidence on physical activity and falls prevention for people aged 65+ years: Systematic review to inform the WHO guidelines on physical activity and sedentary behaviour. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 144. [Google Scholar] [CrossRef]
- Sadaqa, M.; Németh, Z.; Makai, A.; Prémusz, V.; Hock, M. Effectiveness of exercise interventions on fall prevention in ambulatory community-dwelling older adults: A systematic review with narrative synthesis. Front. Public Health 2023, 11, 1209319. [Google Scholar] [CrossRef]
- Sherrington, C.; Michaleff, Z.A.; Fairhall, N.; Paul, S.S.; Tiedemann, A.; Whitney, J.; Cumming, R.G.; Herbert, R.D.; Close, J.C.; Lord, S.R. Exercise to Prevent Falls in Older Adults: An Updated Systematic Review and Meta-Analysis. 2017. Available online: https://bjsm.bmj.com/content/51/24/1750 (accessed on 14 March 2025).
- Sherrington, C.; Fairhall, N.J.; Wallbank, G.K.; Tiedemann, A.; Michaleff, Z.A.; Howard, K.; Clemson, L.; Hopewell, S.; Lamb, S.E. Exercise for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2019, 1, CD012424. [Google Scholar] [CrossRef]
- Dyer, S.M.; Suen, J.; Kwok, W.S.; Dawson, R.; McLennan, C.; Cameron, I.D.; Hill, K.D.; Sherrington, C. Exercise for falls prevention in aged care: Systematic review and trial endpoint meta-analyses. Age Ageing 2023, 52, afad217. [Google Scholar] [CrossRef]
- Murray, K.O.; Mahoney, S.A.; Venkatasubramanian, R.; Seals, D.R.; Clayton, Z.S. Aging, aerobic exercise, and cardiovascular health: Barriers, alternative strategies and future directions. Exp. Gerontol. 2023, 173, 112105. [Google Scholar] [CrossRef]
- Chapman, S.B.; Aslan, S.; Spence, J.S.; DeFina, L.F.; Keebler, M.W.; Didehbani, N.; Lu, H. Shorter term aerobic exercise improves brain, cognition, and cardiovascular fitness in aging. Front. Aging Neurosci. 2013, 5, 75. [Google Scholar] [CrossRef]
- Lavin, K.M.; Roberts, B.M.; Fry, C.S.; Moro, T.; Rasmussen, B.B.; Bamman, M.M. The Importance of Resistance Exercise Training to Combat Neuromuscular Aging. Physiology 2019, 34, 112–122. [Google Scholar] [CrossRef]
- Cannataro, R.; Cione, E.; Bonilla, D.A.; Cerullo, G.; Angelini, F.; D’Antona, G. Strength training in elderly: An useful tool against sarcopenia. Front. Sports Act. Living 2022, 4, 950949. [Google Scholar] [CrossRef]
- Dunsky, A. The Effect of Balance and Coordination Exercises on Quality of Life in Older Adults: A Mini-Review. Front. Aging Neurosci. 2019, 11, 318. [Google Scholar] [CrossRef] [PubMed]
- Dunsky, A.; Unger, L.; Carasso, R.; Fox, O. The Effect of a Single Session of Balance and Coordination Training on Cognitive Function in Older Adults. Appl. Sci. 2023, 13, 3598. [Google Scholar] [CrossRef]
- Labata-Lezaun, N.; Gonzalez-Rueda, V.; Llurda-Almuzara, L.; Lopez-de-Celis, C.; Rodriguez-Sanz, J.; Bosch, J.; Vicente-Rodriguez, G.; Gorczakowska, D.; Araluze-Arizti, P.; Perez-Bellmunt, A. Effectiveness of multicomponent training on physical performance in older adults: A systematic review and meta-analysis. Arch. Gerontol. Geriatr. 2023, 104, 104838. [Google Scholar] [CrossRef]
- Rodrigues, F.; Matos, R.; Jacinto, M.; Antunes, R.; Monteiro, D.; Amaro, N. A Comparison of Multicomponent and Concurrent Exercise Protocols on Muscle Strength in Older Adults. Motricidade 2024, 20. [Google Scholar] [CrossRef]
- Casas-Herrero, Á.; Saez de Asteasu, M.L.; Antón-Rodrigo, I.; Sánchez-Sánchez, J.L.; Montero-Odasso, M.; Marín-Epelde, I.; Ramón-Espinoza, F.; Zambom-Ferraresi, F.; Petidier-Torregrosa, R.; Elexpuru-Estomba, J.; et al. Effects of Vivifrail multicomponent intervention on functional capacity: A multicentre, randomized controlled trial. J. Cachexia Sarcopenia Muscle 2022, 13, 884–893. [Google Scholar] [CrossRef]
- Kruse, A.; Cordes, T.; Schulz, S.; Wollesen, B. Feasibility of Multicomponent Training for People with Moderate to Severe Dementia Living in a Long-Term Care Home: A Social Ethical Approach. Int. J. Environ. Res. Public Health 2021, 18, 7631. [Google Scholar] [CrossRef]
- Philippe, A.G.; Goncalves, A.; Martinez, C.; Deshayes, M.; Charbonnier, E. Can an Eight-Session Multicomponent Physical Exercise Program Reduce Fall Risk and Fear of Falling among the Elderly? Int. J. Environ. Res. Public Health 2022, 19, 8262. [Google Scholar] [CrossRef]
- Sadaqa, M.; Debes, W.A.; Németh, Z.; Bera-Baka, Z.; Vachtler-Szepesi, M.; Nácziné Földes, L.; Prémusz, V.; Hock, M. Multicomponent Exercise Intervention for Preventing Falls and Improving Physical Functioning in Older Nursing Home Residents: A Single-Blinded Pilot Randomised Controlled Trial. J. Clin. Med. 2024, 13, 1577. [Google Scholar] [CrossRef]
- Dolenc, M.; Knific, T.; Tomažin, K. A multicomponent exercise programme to prevent falls and frailty in community-dwelling older adults. Eur. J. Public Health 2023, 33, ckad133.174. [Google Scholar] [CrossRef]
- Sánchez-Sánchez, J.L.; Udina, C.; Medina-Rincón, A.; Esbrí-Victor, M.; Bartolomé-Martín, I.; Moral-Cuesta, D.; Marín-Epelde, I.; Ramon-Espinoza, F.; Latorre, M.S.; Idoate, F.; et al. Effect of a multicomponent exercise program and cognitive stimulation (VIVIFRAIL-COGN) on falls in frail community older persons with high risk of falls: Study protocol for a randomized multicenter control trial. BMC Geriatr. 2022, 22, 612. [Google Scholar] [CrossRef]
- Osuka, Y.; Nofuji, Y.; Seino, S.; Maruo, K.; Oka, H.; Shinkai, S.; Fujiwara, Y.; Sasai, H. The effect of a multicomponent intervention on occupational fall-related factors in older workers: A pilot randomized controlled trial. J. Occup. Health 2022, 64, e12374. [Google Scholar] [CrossRef] [PubMed]
- Sedaghati, P.; Goudarzian, M.; Ahmadabadi, S.; Tabatabai-Asl, S. The impact of a multicomponent-functional training with postural correction on functional balance in the elderly with a history of falling. J. Exp. Orthop. 2022, 9, 23. [Google Scholar] [CrossRef]
- Linhares, D.G.; Borba-Pinheiro, C.J.; de Castro, J.B.P.; dos Santos, A.O.B.; dos Santos, L.L.; Cordeiro, L.D.S.; Drigo, A.J.; Nunes, R.D.A.M.; Vale, R.G.D.S. Effects of Multicomponent Exercise Training on the Health of Older Women with Osteoporosis: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 14195. [Google Scholar] [CrossRef]
- Rodrigues, K.; Prado, L.; de Almeida, M.; Yamada, A.; Finzeto, L.; Bueno Junior, C. Effects of Combined Versus Multicomponent Training in Physically Active Women Aged 50–75 Years. Res. Q. Exerc. Sport 2022, 93, 710–717. [Google Scholar] [CrossRef]
- Cancela Carral, J.; Rodrigues, L.; Bezerra, P. The Long-Term Benefits of a Multicomponent Physical Activity Program to Body Composition, Muscle Strength, Cardiorespiratory Capacity, and Bone Mineral Density in a Group of Nonagenarians. Rejuvenation Res. 2019, 23, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Healthy Ageing and Functional Ability [Internet]. Available online: https://www.who.int/news-room/questions-and-answers/item/healthy-ageing-and-functional-ability (accessed on 14 March 2025).
- Talaulikar, V. Menopause transition: Physiology and symptoms. Best Pract. Res. Clin. Obstet. Gynaecol. 2022, 81, 3–7. [Google Scholar] [CrossRef]
- Gale, C.R.; Cooper, C.; Aihie Sayer, A. Prevalence and risk factors for falls in older men and women: The English Longitudinal Study of Ageing. Age Ageing. 2016, 45, 789–794. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Fu, H. Relationship between proprioception and balance control among Chinese senior older adults. Front. Physiol. 2022, 13, 1078087. [Google Scholar] [CrossRef]
- Sobrinho, A.; Almeida, M.; Rodrigues, G.; Bertani, R.; Lima, J.; Bueno Junior, C. Stretching and Multicomponent Training to Functional Capacities of Older Women: A Randomized Study. Int. J. Environ. Res. Public Health 2021, 19, 27. [Google Scholar] [CrossRef]
- Monteiro, A.; Rodrigues, S.; Matos, S.; Teixeira, J.; Barbosa, T.; Forte, P. The Effects of 32 Weeks of Multicomponent Training with Different Exercises Order in Elderly Women’s Functional Fitness and Body Composition. Medicina 2022, 58, 628. [Google Scholar] [CrossRef]
- Chan, A.-W.; Tetzlaff, J.M.; Altman, D.G.; Laupacis, A.; Gøtzsche, P.C.; Krleža-Jerić, K.; Hróbjartsson, A.; Mann, H.; Dickersin, K.; Berlin, J.A.; et al. SPIRIT 2013 statement: Defining standard protocol items for clinical trials. Ann. Intern. Med. 2013, 158, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Eldridge, S.M.; Chan, C.L.; Campbell, M.J.; Bond, C.M.; Hopewell, S.; Thabane, L.; Lancaster, G.A. CONSORT 2010 statement: Extension to randomised pilot and feasibility trials. BMJ 2016, 355, i5239. [Google Scholar] [CrossRef] [PubMed]
- Body Mass Index: Obesity, BMI, and Health: A Critical Review—PMC. Available online: https://pmc.ncbi.nlm.nih.gov/articles/PMC4890841/ (accessed on 14 March 2025).
- A Healthy Lifestyle—WHO Recommendations [Internet]. Available online: https://www.who.int/europe/news-room/fact-sheets/item/a-healthy-lifestyle---who-recommendations (accessed on 14 March 2025).
- Rikli, R.E.; Jones, C.J. Development and Validation of a Functional Fitness Test for Community-Residing Older Adults. J. Aging Phys. Act. 1999, 7, 129–161. [Google Scholar] [CrossRef]
- Carvalho, M.; Marques, E.; Mota, J. Training and detraining effects on functional fitness after a multicomponent training in older women. Gerontology 2009, 55, 41–48. [Google Scholar] [CrossRef]
- Izquierdo, M.; Merchant, R.A.; Morley, J.E.; Anker, S.D.; Aprahamian, I.; Arai, H.; Aubertin-Leheudre, M.; Bernabei, R.; Cadore, E.L.; Cesari, M.; et al. International Exercise Recommendations in Older Adults (ICFSR): Expert Consensus Guidelines. J. Nutr. Health Aging 2021, 25, 824–853. [Google Scholar] [CrossRef]
- Hanusz, Z.; Tarasinska, J.; Zieliński, W. Shapiro–Wilk Test with Known Mean. REVSTAT-Stat. J. 2016, 14, 89–100. [Google Scholar]
- Gastwirth, J.; Gel, Y.; Miao, W. The Impact of Levene’s Test of Equality of Variances on Statistical Theory and Practice. Stat. Sci. 2010, 24, 343–360. [Google Scholar] [CrossRef]
- Sawyer, S. Analysis of Variance: The Fundamental Concepts. J. Man. Manip. Ther. 2009, 17, 27E–38E. [Google Scholar] [CrossRef]
- Andrade, C. The P Value and Statistical Significance: Misunderstandings, Explanations, Challenges, and Alternatives. Indian J. Psychol. Med. 2019, 41, 210–215. [Google Scholar] [CrossRef]
- Rodrigues, F.; Teixeira, J.E.; Forte, P. The Reliability of the Timed Up and Go Test Among Portuguese Elderly. Healthcare 2023, 11, 928. [Google Scholar] [CrossRef]
- Barry, E.; Galvin, R.; Keogh, C.; Horgan, F.; Fahey, T. Is the Timed Up and Go Test a Useful Predictor of Risk of Falls in Community Dwelling Older Adults: A Systematic Review and Meta- Analysis. BMC Geriatr. 2014, 14, 14. [Google Scholar] [CrossRef] [PubMed]
- Timed Up and Go Test—An Overview|ScienceDirect Topics [Internet]. Available online: https://www.sciencedirect.com/topics/medicine-and-dentistry/timed-up-and-go-test (accessed on 14 May 2025).
- Halma, M.; Marik, P.; Varon, J.; Tuszynski, J. Reversing Decline in Aging Muscles: Expected Trends, Impacts and Remedies. J. Funct. Morphol. Kinesiol. 2025, 10, 29. [Google Scholar] [CrossRef]
- Cho, K.H.; Bok, S.K.; Kim, Y.-J.; Hwang, S.L. Effect of Lower Limb Strength on Falls and Balance of the Elderly. Ann. Rehabil. Med. 2012, 36, 386–393. [Google Scholar] [CrossRef]
- de Almeida Nagata, C.; Hamu, T.C.D.D.S.; Pelicioni, P.H.S.; Durigan, J.L.Q.; Garcia, P.A. Influence of lower limb isokinetic muscle strength and power on the occurrence of falls in community-dwelling older adults: A longitudinal study. PLoS ONE 2024, 19, e0300818. [Google Scholar] [CrossRef]
- Porto, J.M.; Cangussu-Oliveira, L.M.; Freire Junior, R.C.; Vieira, F.T.; Capato, L.L.; de Oliveira, B.G.M.; de Abreu, D.C.C. Relationship Between Lower Limb Muscle Strength and Future Falls Among Community-Dwelling Older Adults with No History of Falls: A Prospective 1-Year Study. J. Appl. Gerontol. 2021, 40, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Zhu, R.T.L.; Zuo, J.J.J.; Li, K.J.; Lam, F.M.H.; Wong, A.Y.L.; Yang, L.; Bai, X.; Wong, M.S.; Kwok, T.; Zheng, Y.P.; et al. Association of lower-limb strength with different fall histories or prospective falls in community-dwelling older people: A systematic review and meta-analysis. BMC Geriatr. 2025, 25, 83. [Google Scholar] [CrossRef] [PubMed]
- Arrieta, H.; Rezola-Pardo, C.; Gil, S.M.; Virgala, J.; Iturburu, M.; Antón, I.; González-Templado, V.; Irazusta, J.; Rodriguez-Larrad, A. Effects of Multicomponent Exercise on Frailty in Long-Term Nursing Homes: A Randomized Controlled Trial. J. Am. Geriatr. Soc. 2019, 67, 1145–1151. [Google Scholar] [CrossRef]
- de Souto Barreto, P.; Cesari, M.; Denormandie, P.; Armaingaud, D.; Vellas, B.; Rolland, Y. Exercise or Social Intervention for Nursing Home Residents with Dementia: A Pilot Randomized, Controlled Trial. J. Am. Geriatr. Soc. 2017, 65, E123–E129. [Google Scholar] [CrossRef]
- Sousa, N.; Mendes, R.; Silva, A.; Oliveira, J. Combined exercise is more effective than aerobic exercise in the improvement of fall risk factors: A randomized controlled trial in community-dwelling older men. Clin. Rehabil. 2017, 31, 478–486. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Group (n) | Age (Mean ± SD) | Median | Min./Max. Age | BMI (Mean ± SD) | Median | Min./Max. BMI | p-Value |
|---|---|---|---|---|---|---|---|
| Control (20) | 68.5 ± 5.24 | 67 | 61/82 | 31.25 kg/m2 ± 5.97 | 30.34 | 23.47/47.58 | 0.89 |
| Multicomponent Training (20) | 68.8 ± 6.35 | 68.5 | 60/86 | 29.67 kg/m2 ± 5.98 | 28.01 | 20.10/40.78 | 0.40 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schneider, A.; Leite, L.B.; Teixeira, J.; Forte, P.; Barbosa, T.M.; Monteiro, A.M. Multicomponent Exercise and Functional Fitness: Strategies for Fall Prevention in Aging Women. Sports 2025, 13, 159. https://doi.org/10.3390/sports13060159
Schneider A, Leite LB, Teixeira J, Forte P, Barbosa TM, Monteiro AM. Multicomponent Exercise and Functional Fitness: Strategies for Fall Prevention in Aging Women. Sports. 2025; 13(6):159. https://doi.org/10.3390/sports13060159
Chicago/Turabian StyleSchneider, André, Luciano Bernardes Leite, José Teixeira, Pedro Forte, Tiago M. Barbosa, and António M. Monteiro. 2025. "Multicomponent Exercise and Functional Fitness: Strategies for Fall Prevention in Aging Women" Sports 13, no. 6: 159. https://doi.org/10.3390/sports13060159
APA StyleSchneider, A., Leite, L. B., Teixeira, J., Forte, P., Barbosa, T. M., & Monteiro, A. M. (2025). Multicomponent Exercise and Functional Fitness: Strategies for Fall Prevention in Aging Women. Sports, 13(6), 159. https://doi.org/10.3390/sports13060159