Old Habits Die Hard: Kinematic Carryover Between Low- and High-Impact Tasks in Active Females

 , , , , , and
, , , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Considerations
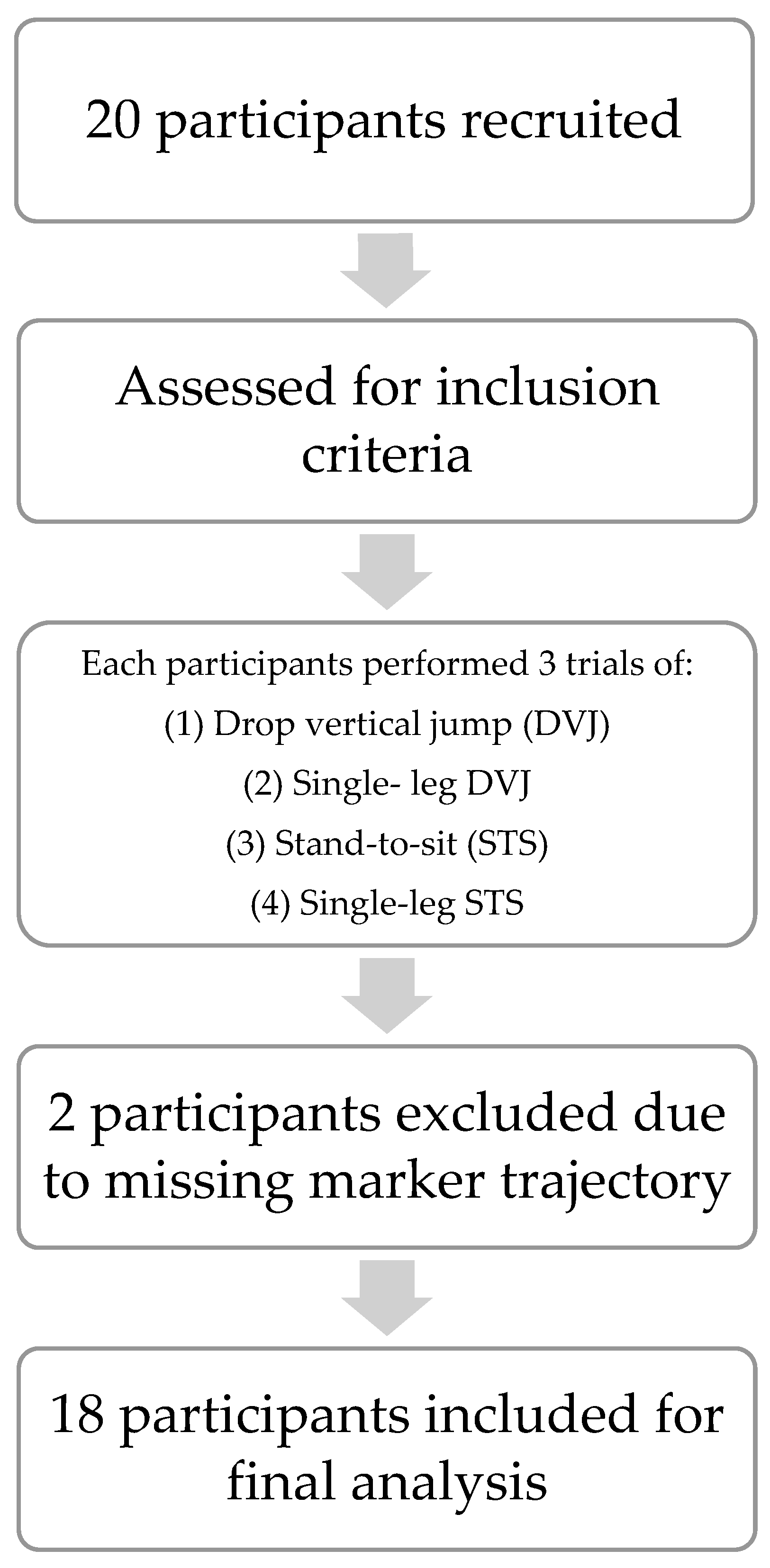
2.2. Sample Size
2.3. Inclusion and Exclusion Criteria
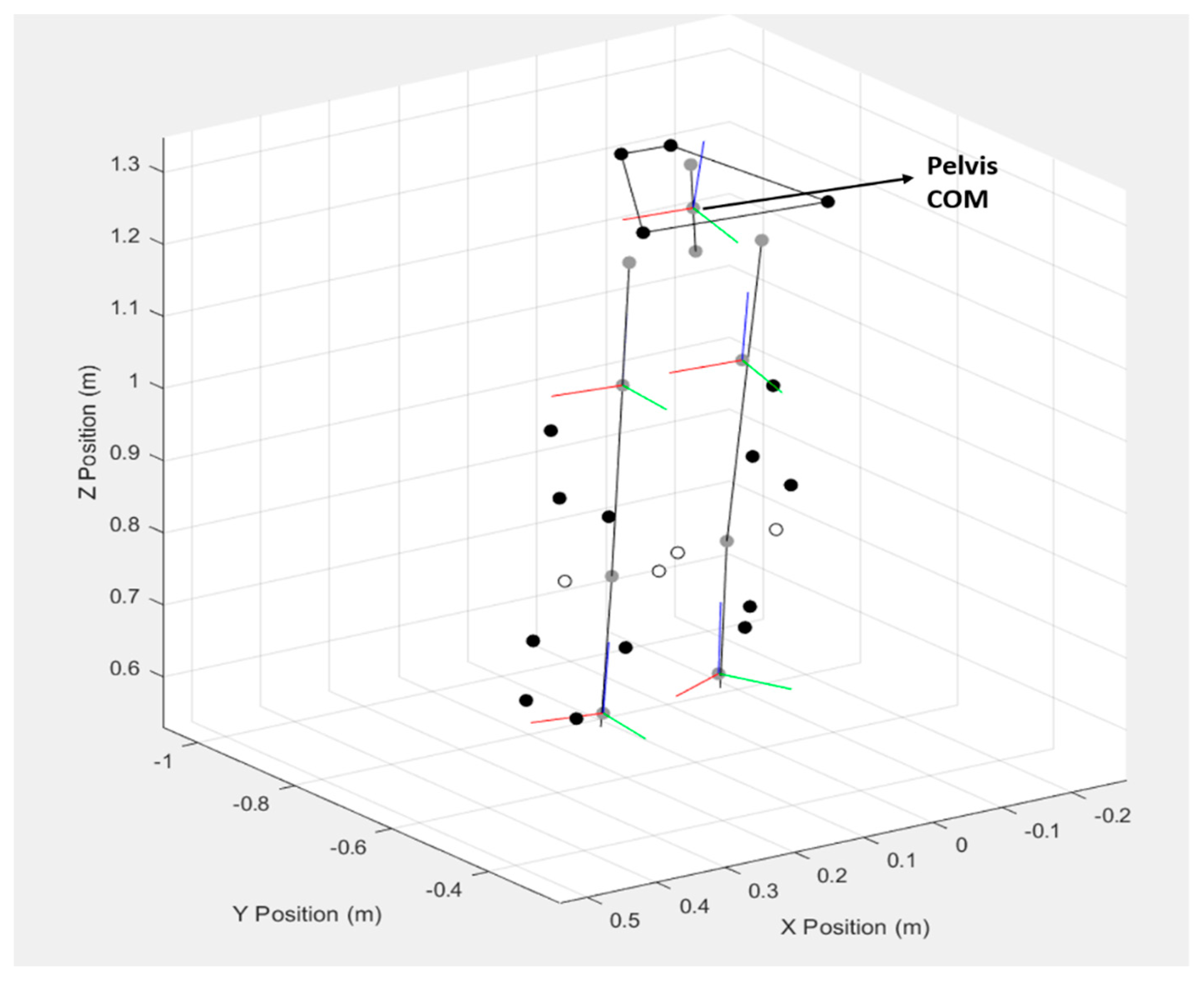
2.4. Instrumentation and Materials
2.5. Data Collection
2.6. Data Reduction
2.7. Statistical Analysis
3. Results
3.1. Participants
3.2. Kinematic Descriptive Data Results
3.3. Correlation Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Majewski, M.; Susanne, H.; Klaus, S. Epidemiology of Athletic Knee Injuries: A 10-Year Study. Knee 2006, 13, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Montalvo, A.M.; Schneider, D.K.; Yut, L.; Webster, K.E.; Beynnon, B.; Kocher, M.S.; Myer, G.D. “What’s My Risk of Sustaining an ACL Injury While Playing Sports?” A Systematic Review with Meta-Analysis. Br. J. Sports Med. 2019, 53, 1003–1012. [Google Scholar] [CrossRef]
- Padua, D.A.; Marshall, S.W.; Boling, M.C.; Thigpen, C.A.; Garrett Jr, W.E.; Beutler, A.I. The Landing Error Scoring System (LESS) Is a Valid and Reliable Clinical Assessment Tool of Jump-Landing Biomechanics: The JUMP-ACL Study. Am. J. Sports Med. 2009, 37, 1996–2002. [Google Scholar] [CrossRef]
- Fox, A.S.; Bonacci, J.; McLean, S.G.; Spittle, M.; Saunders, N. A Systematic Evaluation of Field-Based Screening Methods for the Assessment of Anterior Cruciate Ligament (ACL) Injury Risk. Sports Med. 2016, 46, 715–735. [Google Scholar] [CrossRef]
- Schweizer, N.; Strutzenberger, G.; Franchi, M.V.; Farshad, M.; Scherr, J.; Spörri, J. Screening Tests for Assessing Athletes at Risk of Acl Injury or Reinjury—A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 2864. [Google Scholar] [CrossRef] [PubMed]
- Asgari, M.; Alizadeh, S.; Sendt, A.; Jaitner, T. Evaluation of the Functional Movement Screen (FMS) in Identifying Active Females Who Are Prone to Injury. A Systematic Review. Sports Med.-Open 2021, 7, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Landis, S.E.; Baker, R.T.; Seegmiller, J.G. Non-Contact Anterior Cruciate Ligament and Lower Extremity Injury Risk Prediction Using Functional Movement Screen and Knee Abduction Moment: An Epidemiological Observation of Female Intercollegiate Athletes. Int. J. Sports Phys. Ther. 2018, 13, 973. [Google Scholar] [CrossRef]
- Jones, H. Overcoming Barriers Faced by Practitioners in Assessing ACL Injury Risk. Doctoral Dissertation, Cardiff Metropolitan University, Cardiff, UK, 2023. [Google Scholar]
- Gokeler, A.; Benjaminse, A.; Della Villa, F.; Tosarelli, F.; Verhagen, E.; Baumeister, J. Anterior Cruciate Ligament Injury Mechanisms through a Neurocognition Lens: Implications for Injury Screening. BMJ Open Sport Exerc. Med. 2021, 7, e001091. [Google Scholar] [CrossRef]
- King, M.G.; Heerey, J.J.; Schache, A.G.; Semciw, A.I.; Middleton, K.J.; Sritharan, P.; Lawrenson, P.R.; Crossley, K.M. Lower Limb Biomechanics during Low-and High-Impact Functional Tasks Differ between Men and Women with Hip-Related Groin Pain. Clin. Biomech. 2019, 68, 96–103. [Google Scholar] [CrossRef]
- Guild, P.; Lininger, M.R.; Warren, M. The Association between the Single Leg Hop Test and Lower-Extremity Injuries in Female Athletes: A Critically Appraised Topic. J. Sport Rehabil. 2020, 30, 320–326. [Google Scholar] [CrossRef]
- General Assembly of the World Medical Association World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. J. Am. Coll. Dent. 2014, 81, 14–18.
- Pappas, E.; Carpes, F.P. Lower Extremity Kinematic Asymmetry in Male and Female Athletes Performing Jump-Landing Tasks. J. Sci. Med. Sport 2012, 15, 87–92. [Google Scholar] [CrossRef]
- Portney, L.G. Foundations of Clinical Research: Applications to Evidence-Based Practice; FA Davis: Philadelphia, PA, USA, 2020; ISBN 0-8036-6116-9. [Google Scholar]
- Mall, N.A.; Chalmers, P.N.; Moric, M.; Tanaka, M.J.; Cole, B.J.; Bach Jr, B.R.; Paletta, G.A., Jr. Incidence and Trends of Anterior Cruciate Ligament Reconstruction in the United States. Am. J. Sports Med. 2014, 42, 2363–2370. [Google Scholar] [CrossRef] [PubMed]
- Thein, R.; Hershkovich, O.; Gordon, B.; Burstein, G.; Tenenbaum, S.; Derazne, E.; Tzur, D.; Shamis, A.; Afek, A.; Kreiss, Y. The Prevalence of Cruciate Ligament and Meniscus Knee Injury in Young Adults and Associations with Gender, Body Mass Index, and Height a Large Cross-Sectional Study. J. Knee Surg. 2017, 30, 565–570. [Google Scholar] [CrossRef]
- James, C.R. Gait Analysis Program (GaitAP) Ver. 0.4 (Delta). In Biomechanical Modeling Software for Gait and Posture; Center for Rehabilitation Research, Texas Tech University Health Sciences Center: Lubbock, TX, USA, 2022. [Google Scholar]
- Fukano, M.; Fukubayashi, T. Changes in Talocrural and Subtalar Joint Kinematics of Barefoot versus Shod Forefoot Landing. J. Foot Ankle Res. 2014, 7, 42. [Google Scholar] [CrossRef]
- Koyama, K.; Yamauchi, J. Comparison of Lower Limb Kinetics, Kinematics and Muscle Activation during Drop Jumping under Shod and Barefoot Conditions. J. Biomech. 2018, 69, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Yeow, C.; Lee, P.; Goh, J. Shod Landing Provides Enhanced Energy Dissipation at the Knee Joint Relative to Barefoot Landing from Different Heights. Knee 2011, 18, 407–411. [Google Scholar] [CrossRef]
- Tully, E.A.; Fotoohabadi, M.R.; Galea, M.P. Sagittal Spine and Lower Limb Movement during Sit-to-Stand in Healthy Young Subjects. Gait Posture 2005, 22, 338–345. [Google Scholar] [CrossRef]
- Decker, M.J.; Torry, M.R.; Wyland, D.J.; Sterett, W.I.; Steadman, J.R. Gender Differences in Lower Extremity Kinematics, Kinetics and Energy Absorption during Landing. Clin. Biomech. 2003, 18, 662–669. [Google Scholar] [CrossRef]
- Hughes, G.; Watkins, J. Lower Limb Coordination and Stiffness during Landing from Volleyball Block Jumps. Res. Sports Med. 2008, 16, 138–154. [Google Scholar] [CrossRef]
- Martinez, A.F.; Lessi, G.C.; Carvalho, C.; Serrao, F.V. Association of Hip and Trunk Strength with Three-Dimensional Trunk, Hip, and Knee Kinematics during a Single-Leg Drop Vertical Jump. J. Strength Cond. Res. 2018, 32, 1902–1908. [Google Scholar] [CrossRef] [PubMed]
- Lewis, C.L.; Foch, E.; Luko, M.M.; Loverro, K.L.; Khuu, A. Differences in Lower Extremity and Trunk Kinematics between Single Leg Squat and Step down Tasks. PLoS ONE 2015, 10, e0126258. [Google Scholar] [CrossRef] [PubMed]
- Winter, D.A. Biomechanics and Motor Control of Human Movement; John Wiley & Sons: Hoboken, NJ, USA, 2009; ISBN 0-470-39818-3. [Google Scholar]
- Zatsiorsky, V. Kinematics of Human Motion; Human Kinetics: Champaign, IL, USA, 1998. [Google Scholar]
- Harrington, M.; Zavatsky, A.; Lawson, S.; Yuan, Z.; Theologis, T. Prediction of the Hip Joint Centre in Adults, Children, and Patients with Cerebral Palsy Based on Magnetic Resonance Imaging. J. Biomech. 2007, 40, 595–602. [Google Scholar] [CrossRef]
- Reynold, H.M.; Snow, C.C.; Young, J.W. Spatial Geometry of the Human Pelvis; Civil Aerospace Medical Institute: Oklahoma City, OH, USA, 1982. [Google Scholar]
- Nissan, M.; Gilad, I. Dimensions of Human Lumbar Vertebrae in the Sagittal Plane. J. Biomech. 1986, 19, 753–758. [Google Scholar] [CrossRef]
- Earl, J.E.; Monteiro, S.K.; Snyder, K.R. Differences in Lower Extremity Kinematics between a Bilateral Drop-Vertical Jump and a Single-Leg Step-Down. J. Orthop. Sports Phys. Ther. 2007, 37, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Kerr, K.; White, J.; Barr, D.; Mollan, R. Analysis of the Sit-Stand-Sit Movement Cycle in Normal Subjects. Clin. Biomech. 1997, 12, 236–245. [Google Scholar] [CrossRef]
- Parkinson, S.; Campbell, A.; Dankaerts, W.; Burnett, A.; O’Sullivan, P. Upper and Lower Lumbar Segments Move Differently during Sit-to-Stand. Man. Ther. 2013, 18, 390–394. [Google Scholar] [CrossRef]
- Blackburn, J.T.; Padua, D.A. Sagittal-Plane Trunk Position, Landing Forces, and Quadriceps Electromyographic Activity. J. Athl. Train. 2009, 44, 174–179. [Google Scholar] [CrossRef]
- Scholtes, S.A.; Salsich, G.B. Consistency of Dynamic Knee Valgus Kinematics and Pain Across Functional Tasks in Females With Patellofemoral Pain: A Cross-Sectional Study. Int. J. Sports Phys. Ther. 2020, 15, 985. [Google Scholar] [CrossRef]
- Hajouj, E.; Hadian, M.R.; Mir, S.M.; Talebian, S.; Ghazi, S. Motor Control Changes after Innovative Aquatic Proprioceptive Training in Athletes with Anterior Cruciate Ligament Reconstruction: Voluntary Response Index Analysis. Arch. Neurosci. 2021, 8, e112185. [Google Scholar] [CrossRef]
- Laudani, L.; Giombini, A.; Mariani, P.P.; Pigozzi, F.; Macaluso, A. Application of the Sit-to-Stand Movement for the Early Assessment of Functional Deficits in Patients Who Underwent Anterior Cruciate Ligament Reconstruction. Am. J. Phys. Med. Rehabil. 2014, 93, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Micheo, W.; Hernández, L.; Seda, C. Evaluation, Management, Rehabilitation, and Prevention of Anterior Cruciate Ligament Injury: Current Concepts. PM&R 2010, 2, 935–944. [Google Scholar]
- Taylor, W.R.; Schütz, P.; Bergmann, G.; List, R.; Postolka, B.; Hitz, M.; Dymke, J.; Damm, P.; Duda, G.; Gerber, H. A Comprehensive Assessment of the Musculoskeletal System: The CAMS-Knee Data Set. J. Biomech. 2017, 65, 32–39. [Google Scholar] [CrossRef]
- Lindbeck, L.; Kjellberg, K. Gender Differences in Lifting Technique. Ergonomics 2001, 44, 202–214. [Google Scholar] [CrossRef] [PubMed]
- Hong, Y.N.G.; Shin, C.S. Gender Differences of Sagittal Knee and Ankle Biomechanics during Stair-to-Ground Descent Transition. Clin. Biomech. 2015, 30, 1210–1217. [Google Scholar] [CrossRef] [PubMed]
- Graci, V.; Van Dillen, L.R.; Salsich, G.B. Gender Differences in Trunk, Pelvis and Lower Limb Kinematics during a Single Leg Squat. Gait Posture 2012, 36, 461–466. [Google Scholar] [CrossRef]
- Bates, N.A.; Ford, K.R.; Myer, G.D.; Hewett, T.E. Impact Differences in Ground Reaction Force and Center of Mass between the First and Second Landing Phases of a Drop Vertical Jump and Their Implications for Injury Risk Assessment. J. Biomech. 2013, 46, 1237–1241. [Google Scholar] [CrossRef]
- Sahabuddin, F.N.A.; Jamaludin, N.I.; Bahari, M.L.H.S.; Najib, R.K.M.R.A.; Shaharudin, S. Lower Limb Biomechanics during Drop Vertical Jump at Different Heights among University Athletes. J. Phys. Educ. Sport 2021, 21, 1829–1835. [Google Scholar]
- Kwon, Y.; Heo, J.-H.; Jeon, H.-M.; Min, S.D.; Jun, J.-H.; Tack, G.-R.; Park, B.K.; Kim, J.-W.; Eom, G.-M. Age–Gender Difference in the Biomechanical Features of Sit-to-Stand Movement. J. Mech. Med. Biol. 2016, 16, 1640027. [Google Scholar] [CrossRef]
- Ferreira, V.; Machado, L.; Vilaça, A.; Xará-Leite, F.; Roriz, P. Effects of Tailored Lateral Wedge Insoles on Medial Knee Osteoarthritis Based on Biomechanical Analysis: 12-Week Randomized Controlled Trial. Clin. Rehabil. 2021, 35, 1235–1246. [Google Scholar] [CrossRef]
- Petrella, J.K.; Kim, J.; Tuggle, S.C.; Hall, S.R.; Bamman, M.M. Age Differences in Knee Extension Power, Contractile Velocity, and Fatigability. J. Appl. Physiol. 2005, 98, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Arundale, A.J.; Silvers-Granelli, H.J.; Myklebust, G. ACL Injury Prevention: Where Have We Come from and Where Are We Going? J. Orthop. Res. 2022, 40, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Tassignon, B.; Verschueren, J.; Baeyens, J.-P.; Benjaminse, A.; Gokeler, A.; Serrien, B.; Clijsen, R. An Exploratory Meta-Analytic Review on the Empirical Evidence of Differential Learning as an Enhanced Motor Learning Method. Front. Psychol. 2021, 12, 533033. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Activity | Joint | Plane | Mean | SD |
|---|---|---|---|---|
| bilateral DVJ | dominant hip | sagittal | 99.77 | 14.86 |
| frontal | −5.27 | 7.35 | ||
| transverse | −5.84 | 6.80 | ||
| dominant knee | sagittal | 99.99 | 12.57 | |
| frontal | −6.89 | 7.08 | ||
| transverse | −12.19 | 8.73 | ||
| non-dominant hip | sagittal | 102.27 | 14.55 | |
| frontal | 9.60 | 5.91 | ||
| transverse | 5.57 | 7.55 | ||
| non-dominant knee | sagittal | 101.38 | 14.34 | |
| frontal | 10.34 | 7.12 | ||
| transverse | 6.45 | 8.93 | ||
| bilateral STS | dominant hip | sagittal | 69.07 | 14.63 |
| frontal | −2.75 | 6.00 | ||
| transverse | −2.93 | 6.94 | ||
| dominant knee | sagittal | 85.89 | 8.03 | |
| frontal | −3.22 | 8.72 | ||
| transverse | −15.03 | 7.66 | ||
| non-dominant hip | sagittal | 69.75 | 13.56 | |
| frontal | 6.50 | 3.66 | ||
| transverse | 3.68 | 6.54 | ||
| non-dominant knee | sagittal | 84.62 | 9.78 | |
| frontal | 5.01 | 7.03 | ||
| transverse | 6.67 | 7.26 |
| Activity | Joint | Plane | Mean | SD |
|---|---|---|---|---|
| Single-leg DVJ | dominant hip | sagittal | 68.89 | 13.31 |
| frontal | 6.06 | 6.90 | ||
| transverse | −5.98 | 6.71 | ||
| dominant knee | sagittal | 74.70 | 10.40 | |
| frontal | −4.67 | 6.31 | ||
| transverse | −12.58 | 8.15 | ||
| non-dominant hip | sagittal | 68.81 | 15.84 | |
| frontal | −2.37 | 6.47 | ||
| transverse | 9.78 | 6.32 | ||
| non-dominant knee | sagittal | 72.8 | 10.06 | |
| frontal | 7.48 | 6.07 | ||
| transverse | 2.84 | 9.31 | ||
| Single-leg STS | dominant hip | sagittal | 55.75 | 10.81 |
| frontal | −1.65 | 6.89 | ||
| transverse | −7.84 | 6.43 | ||
| dominant knee | sagittal | 88.29 | 7.49 | |
| frontal | 1.09 | 6.80 | ||
| transverse | −13.01 | 8.10 | ||
| non-dominant hip | sagittal | 57.62 | 11.98 | |
| frontal | 5.17 | 3.34 | ||
| transverse | 10.04 | 5.45 | ||
| non-dominant knee | sagittal | 88.59 | 9.87 | |
| frontal | 1.72 | 6.55 | ||
| transverse | 6.06 | 8.20 |
| LIT | HIT | Joint | Kinematics LIT | Kinematics HIT | Relationship, p-Value | Consistency in the Kinematic Direction |
|---|---|---|---|---|---|---|
| STS | DVJ | Dominant Hip | Abduction | Abduction | r = 0.84, p < 0.01 ** | Consistent |
| SL-STS | DVJ | Dominant Hip | Abduction | Abduction | r = 0.83, p < 0.01 ** | Consistent |
| STS | DVJ | Dominant Knee | Abduction | Abduction | r = 0.81, p < 0.01 ** | Consistent |
| STS | SL-DVJ | Non-dominant Knee | Adduction | Adduction | r = 0.71, p < 0.01 ** | Consistent |
| SL-STS | DVJ | Dominant Knee | Adduction | Abduction | r = 0.80, p < 0.01 ** | Not consistent |
| SL-STS | SL-DVJ | Dominant Knee | Adduction | Abduction | r = 0.86, p < 0.01 ** | Not consistent |
| SL-STS | SL-DVJ | Non-dominant Knee | Adduction | Adduction | r = 0.85, p < 0.01 ** | Consistent |
| LIT | HIT | Joint | Kinematics LIT | Kinematics HIT | Relationship, p-Value | Consistency in the Kinematic Direction |
|---|---|---|---|---|---|---|
| STS | SL-DVJ | Non-dominant hip | Internal rotation | Internal rotation | r = 0.77, p < 0.01 ** | Consistent |
| STS | SL-DVJ | Non-dominant knee | Internal rotation | Internal rotation | r = 0.76, p < 0.01 ** | Consistent |
| STS | DVJ | Dominant knee | External rotation | External rotation | r = 0.77, p < 0.01 ** | Consistent |
| SL-STS | SL-DVJ | Dominant knee | External rotation | External rotation | r = 0.82, p < 0.01 ** | Consistent |
| SL-STS | SL-DVJ | Non-dominant knee | Internal rotation | Internal rotation | r = 0.69, p < 0.05 * | Consistent |
| SL-STS | DVJ | Non-dominant knee | Internal rotation | Internal rotation | r = 0.64, p < 0.05 * | Consistent |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiddarwar, V.V.; Wilford, K.F.; Hooper, T.L.; James, C.R.; Natesan, K.; Likness, A.; Seeber, G.H.; Sizer, P.S. Old Habits Die Hard: Kinematic Carryover Between Low- and High-Impact Tasks in Active Females. Sports 2025, 13, 160. https://doi.org/10.3390/sports13060160
Chiddarwar VV, Wilford KF, Hooper TL, James CR, Natesan K, Likness A, Seeber GH, Sizer PS. Old Habits Die Hard: Kinematic Carryover Between Low- and High-Impact Tasks in Active Females. Sports. 2025; 13(6):160. https://doi.org/10.3390/sports13060160
Chicago/Turabian StyleChiddarwar, Vaishnavi Vivek, Katherine F. Wilford, Troy L. Hooper, C. Roger James, Karthick Natesan, Aaron Likness, Gesine H. Seeber, and Phillip S. Sizer. 2025. "Old Habits Die Hard: Kinematic Carryover Between Low- and High-Impact Tasks in Active Females" Sports 13, no. 6: 160. https://doi.org/10.3390/sports13060160
APA StyleChiddarwar, V. V., Wilford, K. F., Hooper, T. L., James, C. R., Natesan, K., Likness, A., Seeber, G. H., & Sizer, P. S. (2025). Old Habits Die Hard: Kinematic Carryover Between Low- and High-Impact Tasks in Active Females. Sports, 13(6), 160. https://doi.org/10.3390/sports13060160