
Obesity: Friend or Foe in Sjögren’s Syndrome Patients?


Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Cardiovascular Diseases
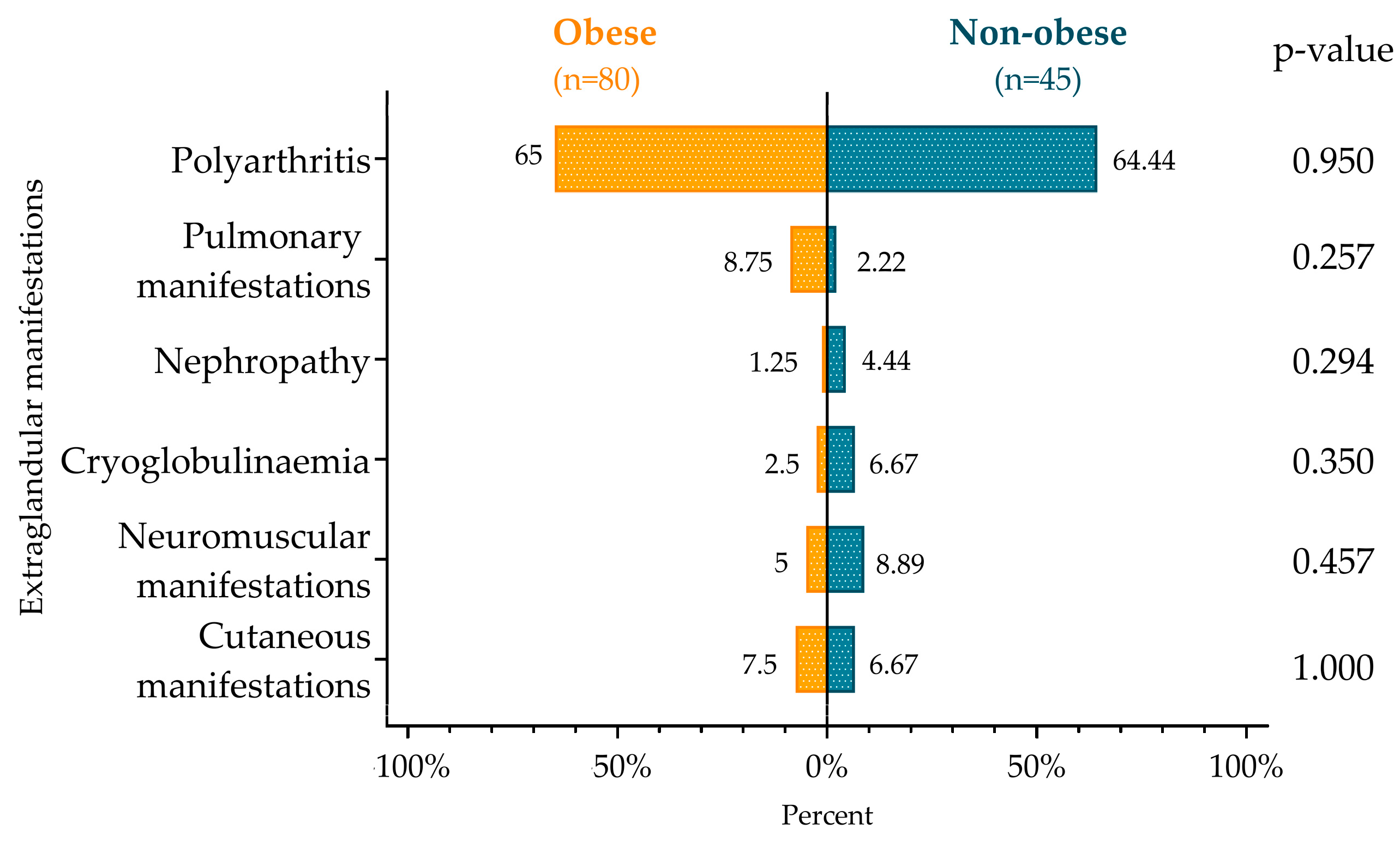
3.2. Autoimmune Disorders and Extraglandular Manifestations
3.3. Laboratory Parameters and Immune Serological Results
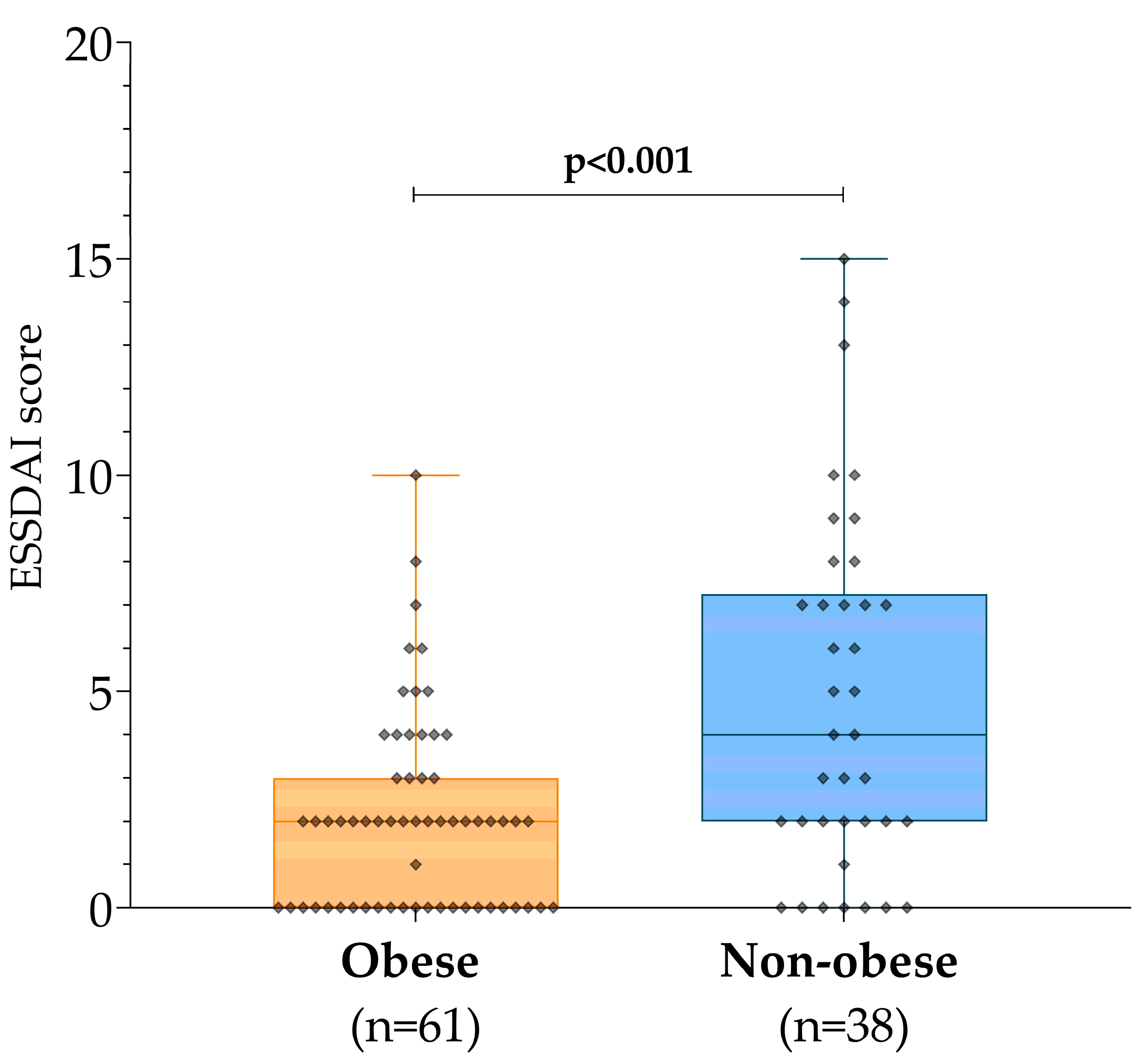
3.4. Disease Management and Disease Activity
3.5. Multiple Linear Regression Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stefanski, A.L.; Tomiak, C.; Pleyer, U.; Dietrich, T.; Burmester, G.R.; Dörner, T. The Diagnosis and Treatment of Sjögren’s Syndrome. Dtsch. Arztebl. Int. 2017, 114, 354–361. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- André, F.; Böckle, B.C. Sjögren’s syndrome. J. Dtsch. Dermatol. Ges. 2022, 20, 980–1002. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Vecchié, A.; Dallegri, F.; Carbone, F.; Bonaventura, A.; Liberale, L.; Portincasa, P.; Frühbeck, G.; Montecucco, F. Obesity phenotypes and their paradoxical association with cardiovascular diseases. Eur. J. Intern. Med. 2018, 48, 6–17. [Google Scholar] [CrossRef] [PubMed]
- Shoenfeld, Y.; Gerli, R.; Doria, A.; Matsuura, E.; Cerinic, M.M.; Ronda, N.; Jara, L.J.; Abu-Shakra, M.; Meroni, P.L.; Sherer, Y. Accelerated atherosclerosis in autoimmune rheumatic diseases. Circulation 2005, 112, 3337–3347. [Google Scholar] [CrossRef] [PubMed]
- Nelson, R.H. Hyperlipidemia as a risk factor for cardiovascular disease. Prim. Care Clin. Off. Pract. 2013, 40, 195–211. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Shiboski, C.H.; Shiboski, S.C.; Seror, R.; Criswell, L.A.; Labetoulle, M.; Lietman, T.M.; Rasmussen, A.; Scofield, H.; Vitali, C.; Bowman, S.J.; et al. 2016 American College of Rheumatology/European League Against Rheumatism Classification Criteria for Primary Sjögren’s Syndrome: A Consensus and Data-Driven Methodology Involving Three International Patient Cohorts. Arthritis Rheumatol. 2017, 69, 35–45. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Both, T.; Dalm, V.A.; van Hagen, P.M.; van Daele, P.L. Reviewing primary Sjögren’s syndrome: Beyond the dryness—From pathophysiology to diagnosis and treatment. Int. J. Med. Sci. 2017, 14, 191–200. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ramos-Casals, M.; Font, J.; García-Carrasco, M.; Brito, M.-P.; Rosas, J.; Calvo-Alen, J.; Pallarés, L.; Cervera, R.; Ingelmo, M. Primary Sjögren syndrome: Hematologic patterns of disease expression. Medicine 2002, 81, 281–292. [Google Scholar] [CrossRef] [PubMed]
- Fox, R.I.; Fox, C.M.; Gottenberg, J.E.; Dörner, T. Treatment of Sjögren’s syndrome: Current therapy and future directions. Rheumatology 2021, 60, 2066–2074. [Google Scholar] [CrossRef] [PubMed]
- Vivino, F.B.; Carsons, S.E.; Foulks, G.; Daniels, T.E.; Parke, A.; Brennan, M.T.; Forstot, S.L.; Scofield, R.H.; Hammitt, K.M. New Treatment Guidelines for Sjögren’s Disease. Rheum. Dis. Clin. N. Am. 2016, 42, 531–551. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chaturvedi, S.; McCrae, K.R. Diagnosis and management of the antiphospholipid syndrome. Blood Rev. 2017, 31, 406–417. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pinal-Fernandez, I.; Casal-Dominguez, M.; Mammen, A.L. Statins: Pros and cons. Med. Clin. 2018, 150, 398–402. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dehnavi, S.; Sohrabi, N.; Sadeghi, M.; Lansberg, P.; Banach, M.; Al-Rasadi, K.; Johnston, T.P.; Sahebkar, A. Statins and autoimmunity: State-of-the-art. Pharmacol. Ther. 2020, 214, 107614. [Google Scholar] [CrossRef] [PubMed]
- Zeiser, R. Immune modulatory effects of statins. Immunology 2018, 154, 69–75. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lundbye, J.B.; Thompson, P.D. Statin use in the metabolic syndrome. Curr. Atheroscler. Rep. 2005, 7, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Tonstad, S.; Després, J.P. Treatment of lipid disorders in obesity. Expert Rev. Cardiovasc. Ther. 2011, 9, 1069–1080. [Google Scholar] [CrossRef] [PubMed]
- Costenbader, K.H.; Coblyn, J.S. Statin therapy in rheumatoid arthritis. South. Med. J. 2005, 98, 534–540; quiz 541, 572. [Google Scholar] [CrossRef] [PubMed]
- Sheng, X.; Murphy, M.J.; Macdonald, T.M.; Wei, L. Effectiveness of statins on total cholesterol and cardiovascular disease and all-cause mortality in osteoarthritis and rheumatoid arthritis. J. Rheumatol. 2012, 39, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Chhibber, A.; Hansen, S.; Biskupiak, J. Statin use and mortality in rheumatoid arthritis: An incident user cohort study. J. Manag. Care Spec. Pharm. 2021, 27, 296–305. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Paraskevas, K.I. Statin treatment for rheumatoid arthritis: A promising novel indication. Clin. Rheumatol. 2008, 27, 281–287. [Google Scholar] [CrossRef] [PubMed]
- De Vera, M.A.; Choi, H.; Abrahamowicz, M.; Kopec, J.; Lacaille, D. Impact of statin discontinuation on mortality in patients with rheumatoid arthritis: A population-based study. Arthritis Care Res. 2012, 64, 809–816. [Google Scholar] [CrossRef] [PubMed]
- Sahebkar, A.; Rathouska, J.; Derosa, G.; Maffioli, P.; Nachtigal, P. Statin impact on disease activity and C-reactive protein concentrations in systemic lupus erythematosus patients: A systematic review and meta-analysis of controlled trials. Autoimmun. Rev. 2016, 15, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Jorge, A.; Lu, N.; Keller, S.; Rai, S.K.; Zhang, Y.; Choi, H.K. The impact of statin use on mortality in systemic autoimmune rheumatic diseases. J. Rheumatol. 2018, 45, 1689–1695. [Google Scholar] [CrossRef] [PubMed]
- Simati, S.; Kokkinos, A.; Dalamaga, M.; Argyrakopoulou, G. Obesity Paradox: Fact or Fiction? Curr. Obes. Rep. 2023, 12, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Won, K.B.; Hur, S.H.; Nam, C.W.; Ann, S.H.; Park, G.M.; Lee, S.G.; Kim, H.E.; Cho, Y.K.; Yoon, H.J.; Park, H.S.; et al. Evaluation of the impact of statin therapy on the obesity paradox in patients with acute myocardial infarction: A propensity score matching analysis from the Korea Acute Myocardial Infarction Registry. Medicine 2017, 96, e7180. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Asenjo-Lobos, C.; González, L.; Bulnes, J.F.; Roque, M.; Muñoz Venturelli, P.; Rodríguez, G.M. Cardiovascular events risk in patients with systemic autoimmune diseases: A prognostic systematic review and meta-analysis. Clin. Res. Cardiol. 2024, 113, 246–259. [Google Scholar] [CrossRef] [PubMed]
- Beltai, A.; Barnetche, T.; Daien, C.; Lukas, C.; Gaujoux-Viala, C.; Combe, B.; Morel, J. Cardiovascular morbidity and mortality in primary Sjögren’s syndrome: A systematic review and meta-analysis. Arthritis Care Res. 2020, 72, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.F.; Huang, J.Y.; Chiou, J.Y.; Chen, H.H.; Wei, J.C.; Dong, L.L. Increased risk of coronary heart disease among patients with primary Sjögren’s syndrome: A nationwide population-based cohort study. Sci. Rep. 2018, 8, 2209. [Google Scholar] [CrossRef] [PubMed]
- Yong, W.C.; Sanguankeo, A.; Upala, S. Association between primary Sjögren’s syndrome, cardiovascular and cerebrovascular disease: A systematic review and meta-analysis. Clin. Exp. Rheumatol. 2018, 36 (Suppl. S112), 190–197. [Google Scholar] [PubMed]
- Bartoloni, E.; Baldini, C.; Schillaci, G.; Quartuccio, L.; Priori, R.; Carubbi, F.; Bini, V.; Alunno, A.; Bombardieri, S.; De Vita, S.; et al. Cardiovascular disease risk burden in primary Sjögren’s syndrome: Results of a population-based multicenter cohort study. J. Intern. Med. 2015, 278, 185–192. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Obese n (% of Total 80) | Non-Obese, n (% of Total 45) | p-Value | Effect-Size (w) | |
|---|---|---|---|---|
| Hypertension | 55 (68.75) | 21 (46.67) | 0.015 | 0.217 |
| Type 2 Diabetes | 14 (17.5) | 1 (2.22) | 0.012 | 0.226 |
| Stroke | 4 (5) | 1 (2.22) | 0.653 | 0.040 |
| Ischemic heart disease | 23 (28.75) | 9 (20) | 0.282 | 0.096 |
| Carotid artery stenosis | 5 (6.25) | 2 (4.44) | 1.000 | 0.000 |
| Obese n (% of Total 80) | Non-Obese, n (% of Total 45) | p-Value | Effect-Size (w) | |
|---|---|---|---|---|
| Rheumatoid Arthritis | 15 (18.75) | 7 (15.56) | 0.653 | 0.040 |
| Systemic Lupus Erythematosus | 4 (5) | 4 (8.89) | 0.457 | 0.067 |
| Antiphospholipid Syndrome | 3 (3.75) | 3 (6.67) | 0.666 | 0.039 |
| Associated Sjögren’s syndrome | 18 (22.5) | 12 (26.6) | 0.601 | 0.047 |
| Hashimoto Thyreoiditis | 11 (13.75) | 6 (13.33) | 0.948 | 0.006 |
| Raynaud’s phenomenon | 20 (25) | 18 (40) | 0.080 | 0.157 |
| Obese | Non-Obese | p-Value | Effect-Size | |||
|---|---|---|---|---|---|---|
| Valid n | Median (IQR) or Mean ± SD or n (%) | Valid n | Median (IQR) or Mean ± SD or n (%) | |||
| GFR (mL/p/1.73 m2) | 79 | 80 (68–90) | 45 | 79 (67–90) | 0.989 | d = 0.002 |
| Urea (mmol/l) | 79 | 5.1 (4.05–6.4) | 45 | 4.9 (4.4–5.8) | 0.419 | d = 0.146 |
| Creatinine (μmol/l) | 79 | 69 (60.5–78) | 45 | 71 (62–81) | 0.582 | d = 0.099 |
| AST (U/L) | 80 | 21 (17–26) | 44 | 20.5 (16–25) | 0.364 | d = 0.164 |
| ALT (U/L) | 80 | 71.5 (58.5–91.25) | 45 | 64 (56–73) | 0.093 | d = 0.305 |
| GGT (U/L) | 80 | 24 (17.75–47.5) | 45 | 19 (15–25) | 0.005 | d = 0.523 |
| AP (U/L) | 80 | 21 (15–29.5) | 45 | 16 (13–22) | 0.010 | d = 0.477 |
| CRP (mg/l) | 80 | 2.8 (1.5–6.6) | 44 | 2.28 (1–7.1) | 0.522 | d = 0.115 |
| LDH (U/L) | 79 | 211 (188–244.5) | 44 | 205.5 (178.75–233.75) | 0.348 | d = 0.169 |
| Cholesterol (mmol/L) | 79 | 5.02 ± 1.21 | 45 | 4.75 ± 1.15 | 0.231 | d = 0.225 |
| Triglyceride (mmol/L) | 79 | 1.4 (1.05–1.95) | 45 | 1.1 (0.7–1.4) | <0.001 | d = 0.699 |
| Leukocyte (G/L) | 79 | 6.47 (5.3–7.84) | 45 | 6.51 (5.42–8.72) | 0.647 | d = 0.082 |
| Hemoglobin (g/l) | 79 | 133.42 ± 12.57 | 45 | 125.71 ± 14.32 | 0.002 | d = 0.583 |
| Platelet (/mL) | 79 | 229 (197.5–291) | 45 | 243 (202–285) | 0.682 | d = 0.074 |
| Neutrophil (%) | 79 | 59.95 ± 11.51 | 45 | 65.46 ± 12.84 | 0.015 | d = 0.459 |
| Lymphocyte (%) | 79 | 28.52 ± 10.35 | 45 | 23.47 ± 10.81 | 0.011 | d = 0.48 |
| Erythrocyte sedimentation rate (mm/h) | 79 | 20 (14–38) | 45 | 28 (12–52) | 0.260 | d = 0.203 |
| IgA (g/L) | 80 | 1.95 (1.5–2.7) | 45 | 2.1 (1.6–2.8) | 0.088 | d = 0.31 |
| IgG (g/L) | 80 | 10.2 (7.98–11.6) | 45 | 10.6 (8.5–16.5) | 0.089 | d = 0.309 |
| IgM (g/L) | 78 | 1.13 (0.66–1.84) | 45 | 1.1 (0.71–1.65) | 0.983 | d = 0.004 |
| c3 (g/L) | 80 | 1.4 (1.25–1.53) | 45 | 1.21 (1.07–1.36) | <0.001 | d = 0.877 |
| c4 (g/L) | 80 | 0.27 (0.23–0.31) | 45 | 0.22 (0.17–0.27) | 0.003 | d = 0.549 |
| CH50 (CH50/mL) | 79 | 73 (59.5–83) | 44 | 76.5 (63.5–82) | 0.969 | d = 0.007 |
| anti-Ro/SS-A+ | 80 | 40 (50) | 45 | 25 (55.56) | 0.551 | w = 0.053 |
| anti-La/SS-B+ | 80 | 26 (32.5) | 45 | 16 (35.56) | 0.728 | w = 0.031 |
| Rheumatoid factor + | 80 | 38 (47.5) | 45 | 30 (66.67) | 0.039 | w = 0.185 |
| Obese, n (%) | Non-Obese, (n%) | p-Value | Effect-Size (w) | |
|---|---|---|---|---|
| DMARD | 47 (58.75) | 32 (71.11) | 0.169 | 0.123 |
| Steroid | 31 (38.75) | 26 (57.78) | 0.040 | 0.183 |
| Statin | 35 (43.75) | 10 (22.22) | 0.016 | 0.215 |
| Unstandardized | Standardized | t | p-Value | 95% Confidence Interval for B | |||
|---|---|---|---|---|---|---|---|
| B | Standard Error | β | Lower Bound | Upper Bound | |||
| (Constant) | −1.388 | 2.587 | −0.537 | 0.593 | −6.527 | 3.751 | |
| Obesity | −1.618 | 0.971 | −0.172 | −1.666 | 0.099 | −3.548 | 0.311 |
| Steroid | 3.513 | 0.979 | 0.376 | 3.588 | 0.001 | 1.568 | 5.457 |
| Statin | −0.018 | 0.955 | −0.002 | −0.018 | 0.985 | −1.915 | 1.880 |
| anti-Ro/SS-A+ | 0.436 | 1.019 | 0.048 | 0.428 | 0.670 | −1.588 | 2.460 |
| anti-La/SS-B+ | 0.348 | 1.166 | 0.036 | 0.298 | 0.766 | −1.969 | 2.665 |
| Rheumatoid factor + | 0.072 | 0.985 | 0.008 | 0.073 | 0.942 | −1.885 | 2.029 |
| CRP (mg/L) | −0.054 | 0.058 | −0.086 | −0.932 | 0.354 | −0.168 | 0.061 |
| LDH (U/L) | 0.022 | 0.009 | 0.235 | 2.528 | 0.013 | 0.005 | 0.038 |
| Triglyceride (mmol/L) | −0.177 | 0.774 | −0.024 | −0.229 | 0.819 | −1.714 | 1.359 |
| Cholesterol (mmol/L) | 0.061 | 0.369 | 0.017 | 0.166 | 0.869 | −0.672 | 0.795 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mezei, K.; Nagy, L.; Orosz, V.; Aradi, Z.; Bói, B.; Szántó, A. Obesity: Friend or Foe in Sjögren’s Syndrome Patients? Diagnostics 2024, 14, 2725. https://doi.org/10.3390/diagnostics14232725
Mezei K, Nagy L, Orosz V, Aradi Z, Bói B, Szántó A. Obesity: Friend or Foe in Sjögren’s Syndrome Patients? Diagnostics. 2024; 14(23):2725. https://doi.org/10.3390/diagnostics14232725
Chicago/Turabian StyleMezei, Kincső, Laura Nagy, Viktória Orosz, Zsófia Aradi, Bernadett Bói, and Antónia Szántó. 2024. "Obesity: Friend or Foe in Sjögren’s Syndrome Patients?" Diagnostics 14, no. 23: 2725. https://doi.org/10.3390/diagnostics14232725
APA StyleMezei, K., Nagy, L., Orosz, V., Aradi, Z., Bói, B., & Szántó, A. (2024). Obesity: Friend or Foe in Sjögren’s Syndrome Patients? Diagnostics, 14(23), 2725. https://doi.org/10.3390/diagnostics14232725