

Inequalities in PM2.5 and SO2 Exposure Health Risks in Terms of Emissions in China, 2013–2017
 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Data and Methods
2.1. Data Sources and Pre-Processing
2.1.1. Data Sources
2.1.2. Data Pre-Processing
2.2. Methods
2.2.1. Inequality Analysis
2.2.2. Health Risk Evaluation
3. Results
3.1. Health Risk Assessment
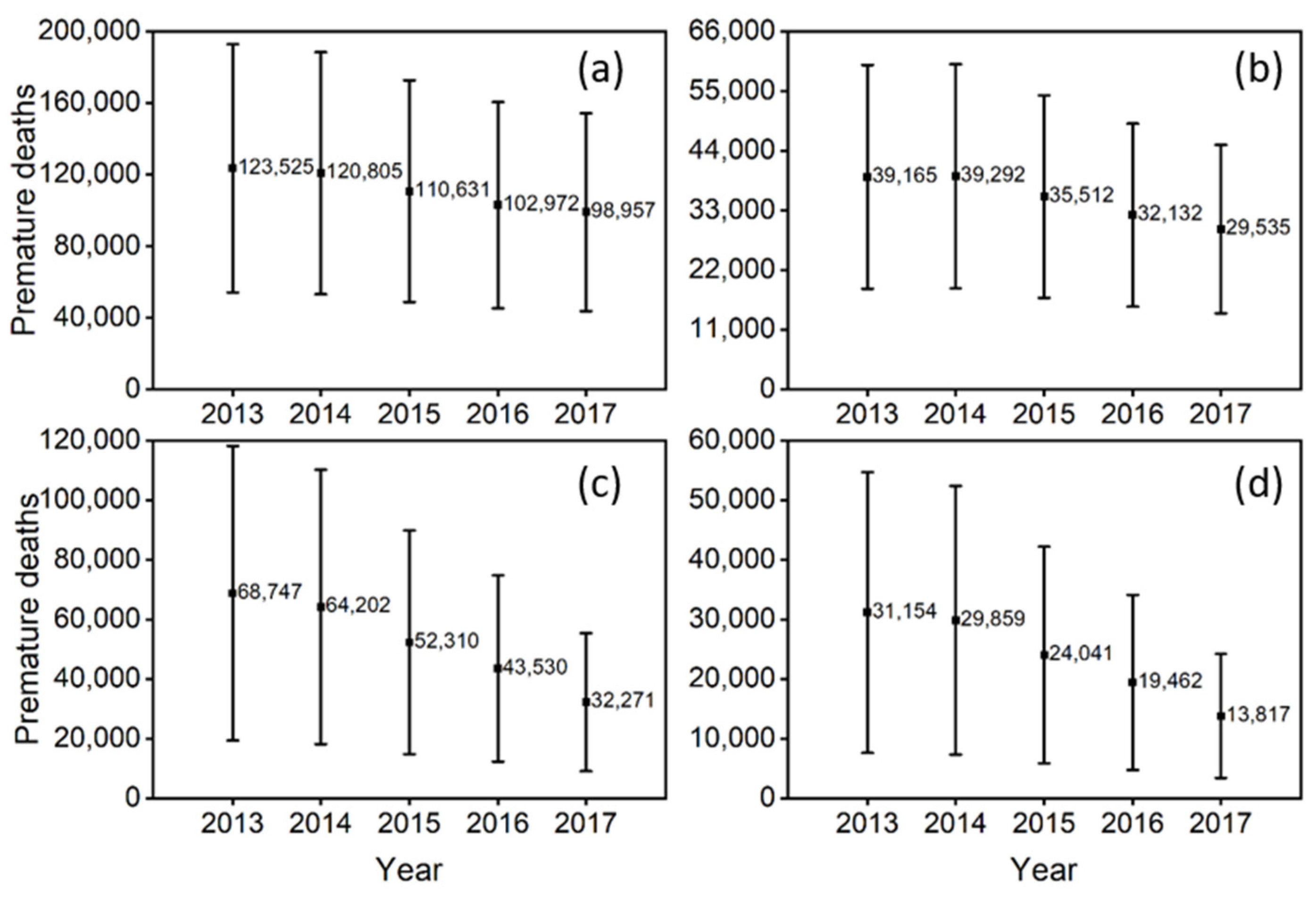
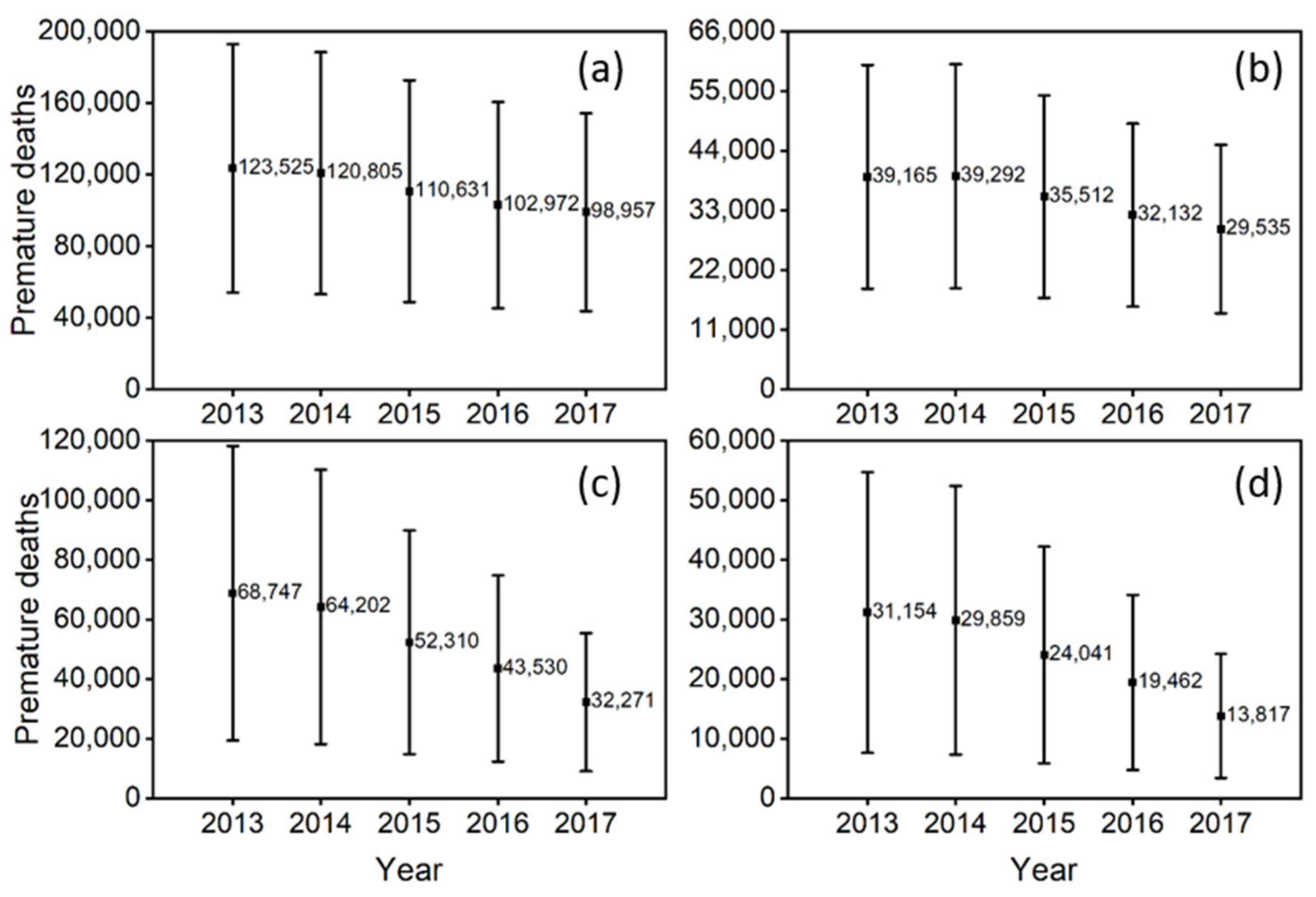
3.1.1. Characteristics of the Health Risk Variation with Time in National Scale
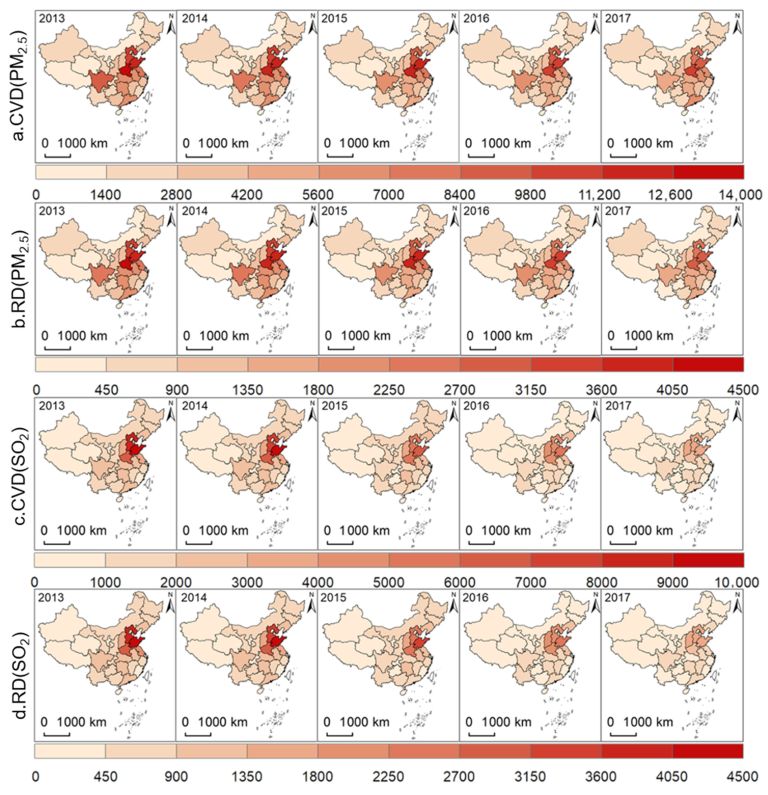
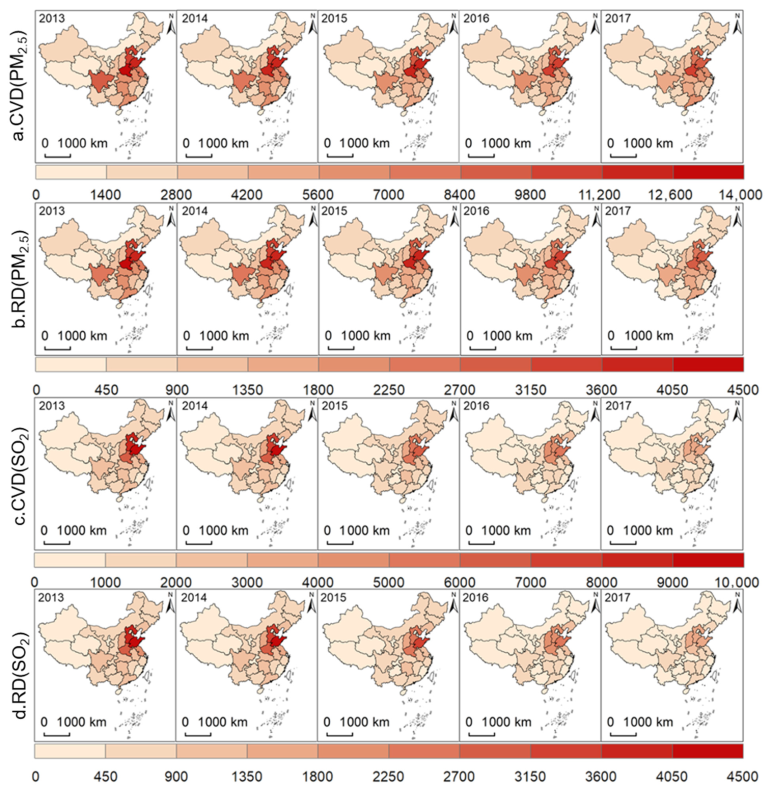
3.1.2. Characteristics of Temporal and Spatial Distribution of Health Risk in Provincial Scale
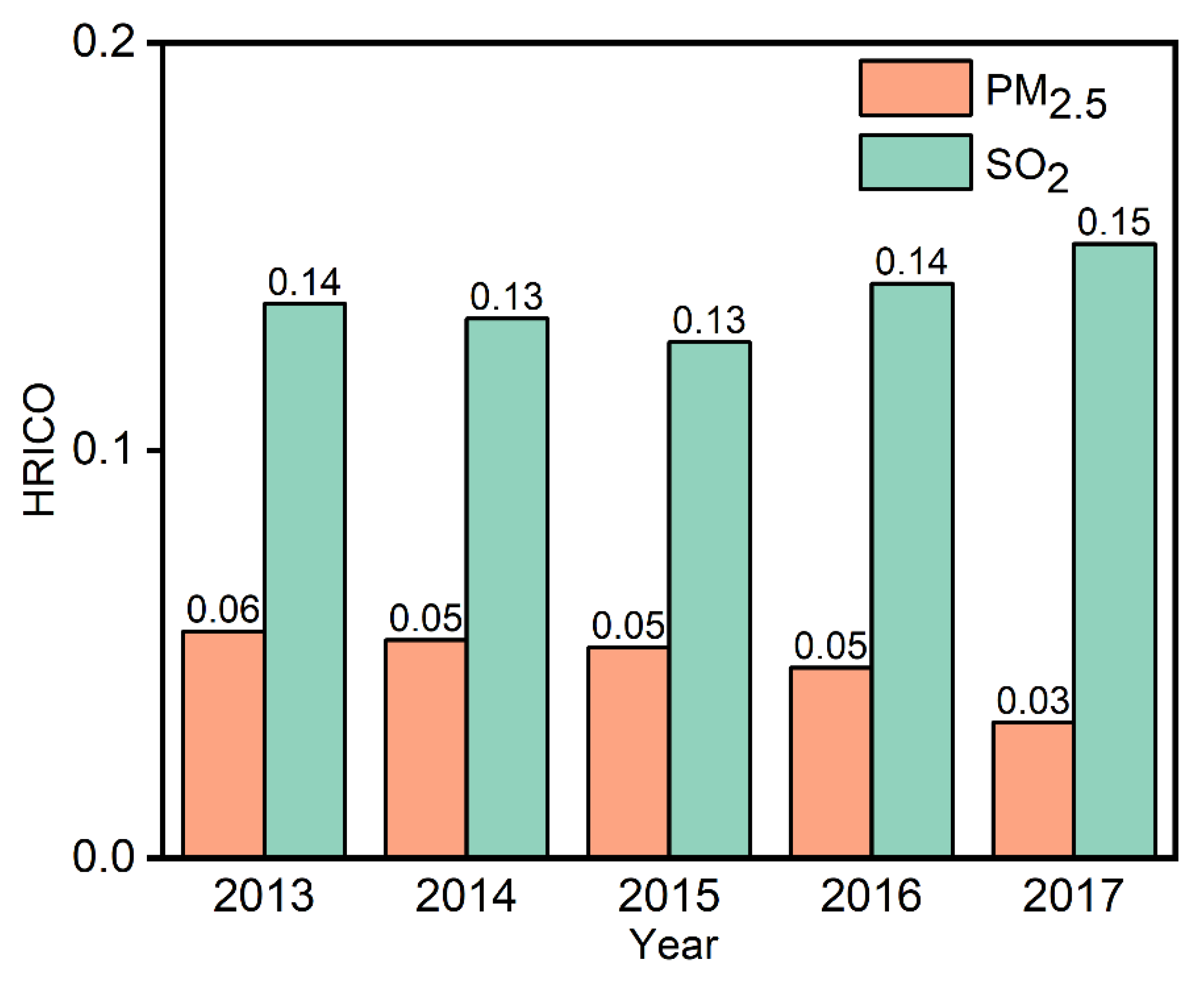
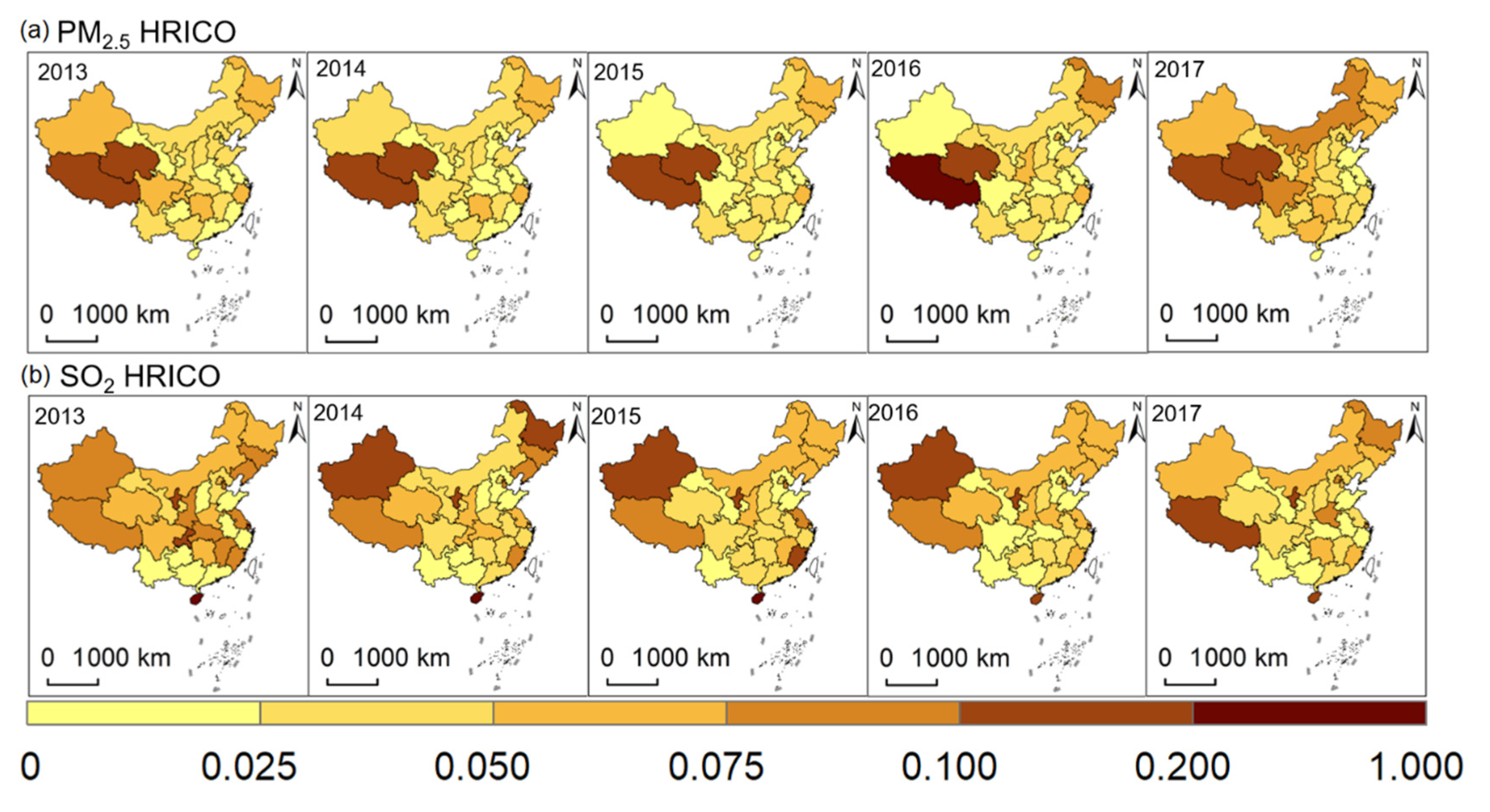
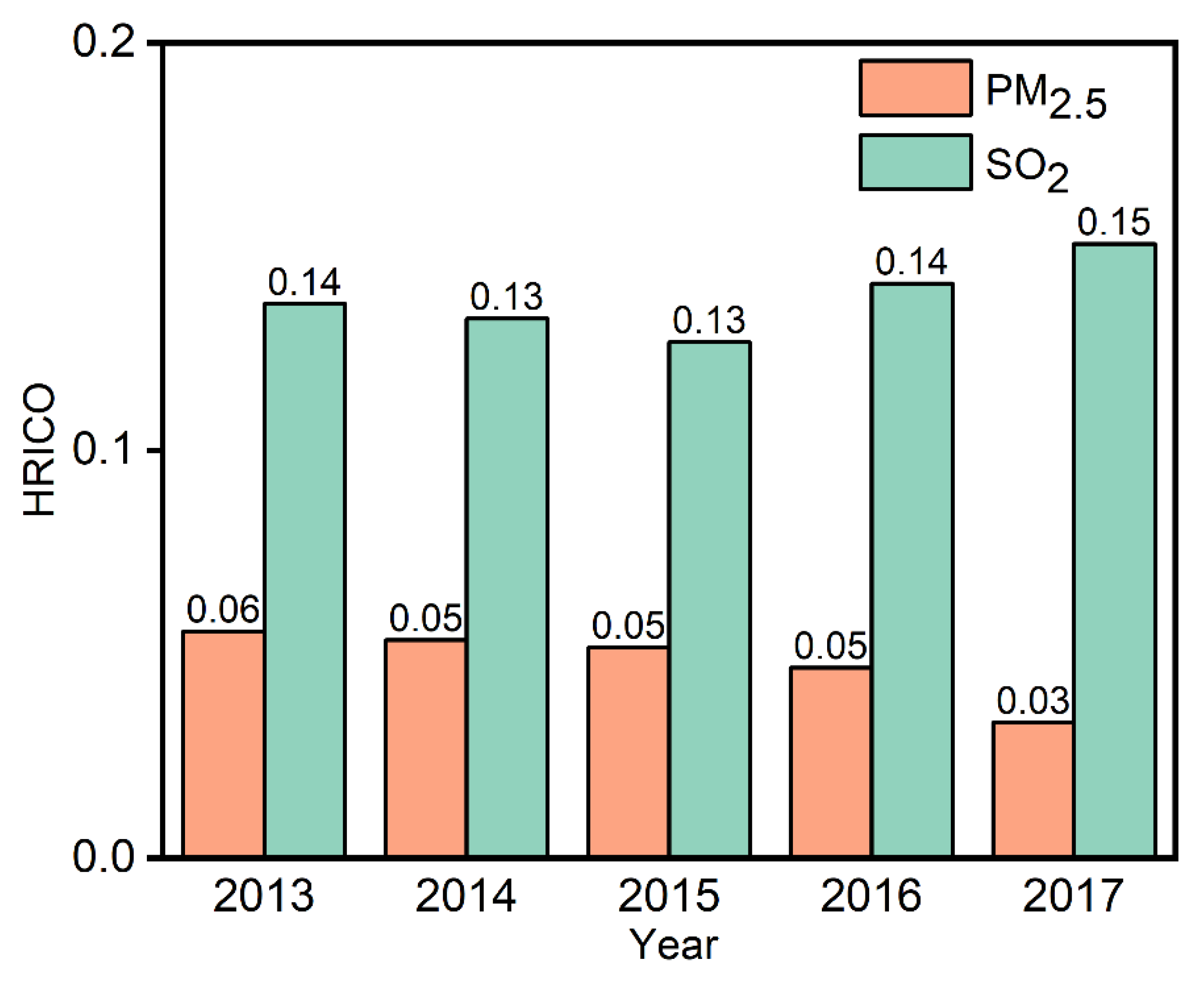
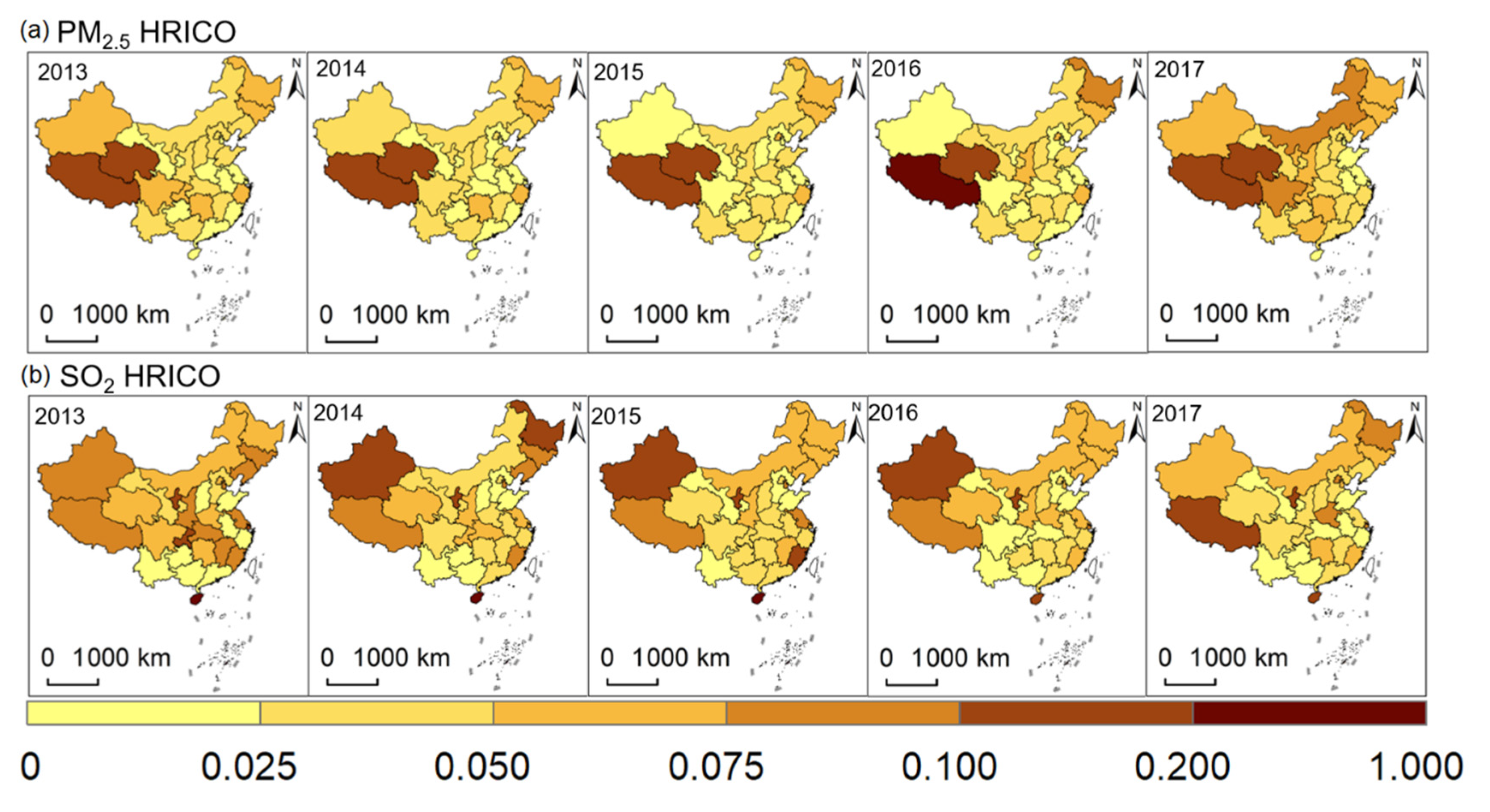
3.2. Inequality Analysis
4. Discussion
4.1. Health Risk Analysis
4.2. Analysis of Inequality
4.3. Uncertainties
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Qi, H.; Wang, R.; Han, J.; Wei, G.; Wang, J.; Liu, J. Theoretical Model of Environmental Justice and Environmental Inequality in China’s Four Major Economic Zones. Sustainability 2019, 11, 5923. [Google Scholar] [CrossRef]
- Heffron, R.J.; McCauley, D.; Sovacool, B.K. Resolving Society’s Energy Trilemma through the Energy Justice Metric. Energy Policy 2015, 87, 168–176. [Google Scholar] [CrossRef]
- Liu, M.; Saari, R.K.; Zhou, G.; Li, J.; Han, L.; Liu, X. Recent Trends in Premature Mortality and Health Disparities Attributable to Ambient PM2.5 Exposure in China: 2005–2017. Environ. Pollut. 2021, 279, 116882. [Google Scholar] [CrossRef] [PubMed]
- Pun, V.C.; Kazemiparkouhi, F.; Manjourides, J.; Suh, H.H. Long-Term PM2.5 Exposure and Respiratory, Cancer, and Cardiovascular Mortality in Older US Adults. Am. J. Epidemiol. 2017, 186, 961–969. [Google Scholar] [CrossRef]
- Requia, W.J.; Adams, M.D.; Arain, A.; Papatheodorou, S.; Koutrakis, P.; Mahmoud, M. Global Association of Air Pollution and Cardiorespiratory Diseases: A Systematic Review, Meta-Analysis, and Investigation of Modifier Variables. Am. J. Public Health 2018, 108, S123–S130. [Google Scholar] [CrossRef]
- Bell, M.L.; Ebisu, K. Environmental Inequality in Exposures to Airborne Particulate Matter Components in the United States. Environ. Health Perspect. 2012, 120, 1699–1704. [Google Scholar] [CrossRef]
- Kazakos, V.; Taylor, J.; Luo, Z. Impact of COVID-19 Lockdown on NO2 and PM2.5 Exposure Inequalities in London, UK. Environ. Res. 2021, 198, 111236. [Google Scholar] [CrossRef]
- Kihal-Talantikite, W.; Legendre, P.; Le Nouveau, P.; Deguen, S. Premature Adult Death and Equity Impact of a Reduction of NO2, PM10, and PM2.5 Levels in Paris—A Health Impact Assessment Study Conducted at the Census Block Level. Int. J. Environ. Res. Public Health 2019, 16, 38. [Google Scholar] [CrossRef]
- Rosofsky, A.; Levy, J.I.; Zanobetti, A.; Janulewicz, P.; Fabian, M.P. Temporal Trends in Air Pollution Exposure Inequality in Massachusetts. Environ. Res. 2018, 161, 76–86. [Google Scholar] [CrossRef]
- Son, J.-Y.; Lane, K.J.; Miranda, M.L.; Bell, M.L. Health Disparities Attributable to Air Pollutant Exposure in North Carolina: Influence of Residential Environmental and Social Factors. Health Place 2020, 62, 102287. [Google Scholar] [CrossRef]
- Boulanger, G.; Bayeux, T.; Mandin, C.; Kirchner, S.; Vergriette, B.; Pernelet-Joly, V.; Kopp, P. Socio-Economic Costs of Indoor Air Pollution: A Tentative Estimation for Some Pollutants of Health Interest in France. Environ. Int. 2017, 104, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Azimi, M.; Feng, F.; Zhou, C. Air Pollution Inequality and Health Inequality in China: An Empirical Study. Environ. Sci. Pollut. Res. 2019, 26, 11962–11974. [Google Scholar] [CrossRef]
- Yuan, Q.; McIntyre, N.; Wu, Y.; Liu, Y.; Liu, Y. Towards Greater Socio-Economic Equality in Allocation of Wastewater Discharge Permits in China Based on the Weighted Gini Coefficient. Resour. Conserv. Recycl. 2017, 127, 196–205. [Google Scholar] [CrossRef]
- Li, Y.; Zhong, R.; Wang, Z.; Yu, M.; Wu, Y.; Irfan, M.; Hao, Y. Would the Inequality of Environmental Quality Affect Labor Productivity and the Income Gap? Evidence from China. J. Environ. Plan. Manag. 2022, 1–34. [Google Scholar] [CrossRef]
- Bosi, S.; Seegmuller, T. Optimal Cycles and Social Inequality: What Do We Learn from the Gini Index? Res. Econ. 2006, 60, 35–46. [Google Scholar] [CrossRef]
- Duan, C.; Chen, B. Analysis of Global Energy Consumption Inequality by Using Lorenz Curve. Energy Procedia 2018, 152, 750–755. [Google Scholar] [CrossRef]
- Soares, T.C.; Fernandes, E.A.; Toyoshima, S.H. The CO2 Emission Gini Index and the Environmental Efficiency: An Analysis for 60 Leading World Economies. EconomiA 2018, 19, 266–277. [Google Scholar] [CrossRef]
- Zaręba, M.; Danek, T. Analysis of Air Pollution Migration during COVID-19 Lockdown in Krakow, Poland. Aerosol Air Qual. Res. 2022, 22, 210275. [Google Scholar] [CrossRef]
- Khan, S.; Dahu, B.M.; Scott, G.J. A Spatio-Temporal Study of Changes in Air Quality from Pre-COVID Era to Post-COVID Era in Chicago, USA. Aerosol Air Qual. Res. 2022, 22, 220053. [Google Scholar] [CrossRef]
- Nie, W.; Liu, C.; Zhang, H.; Wang, H.; Jin, H.; Yan, J.; Liu, Q. The Preparation of a Novel Hydrogel Based on Crosslinked Polymers for Suppressing Coal Dusts. J. Clean. Prod. 2020, 249, 119343. [Google Scholar]
- Wang, J. Life Cycle Assessment and Environmental Cost Accounting of Coal-Fired Power Generation in China. Energy Policy 2018, 115, 374–384. [Google Scholar] [CrossRef]
- Xu, B. Regional Differences of Pollution Emissions in China: Contributing Factors and Mitigation Strategies. J. Clean. Prod. 2016, 112, 1454–1463. [Google Scholar] [CrossRef]
- Xu, C. Pollution Haven or Halo? The Role of the Energy Transition in the Impact of FDI on SO2 Emissions. Sci. Total Environ. 2021, 763, 143002. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Ning, M.; Lei, Y.; Sun, Y.; Liu, W.; Wang, J. Defending Blue Sky in China: Effectiveness of the “Air Pollution Prevention and Control Action Plan” on Air Quality Improvements from 2013 to 2017. J. Environ. Manag. 2019, 252, 109603. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zang, L.; Du, W.; Xu, D.; Shen, G.; Zhang, Q.; Zou, Q.; Chen, J.; Zhao, M.; Yao, D. Ambient Air Pollution of Particles and Gas Pollutants, and the Predicted Health Risks from Long-Term Exposure to PM2.5 in Zhejiang Province, China. Environ. Sci. Pollut. Res. 2018, 25, 23833–23844. [Google Scholar] [CrossRef] [PubMed]
- Liang, F.; Liu, F.; Huang, K.; Yang, X.; Li, J.; Xiao, Q.; Chen, J.; Liu, X.; Cao, J.; Shen, C.; et al. Long-Term Exposure to Fine Particulate Matter and Cardiovascular Disease in China. J. Am. Coll. Cardiol. 2020, 75, 707–717. [Google Scholar] [CrossRef]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Hammer, M.S.; van Donkelaar, A.; Li, C.; Lyapustin, A.; Sayer, A.M.; Hsu, N.C.; Levy, R.C.; Garay, M.J.; Kalashnikova, O.V.; Kahn, R.A.; et al. Global Estimates and Long-Term Trends of Fine Particulate Matter Concentrations (1998–2018). Environ. Sci. Technol. 2020, 54, 7879–7890. [Google Scholar] [CrossRef]
- He, Y. Analysis on the Spatial and Temporal Pattern of PM2.5 and Its Influencing Factors in Shaanxi Province. Master’s Thesis, Northwest Normal University, Lanzhou, China, 2021. [Google Scholar]
- Weiguang, F.; Pingyu, Z.; Lianjun, T.; Chenggu, L.; Xin, L.; Jing, L.; Zuopeng, M. Green Development for Supporting Sustainability of Northeast China: Performance Quantification, Spatio-Temporal Dynamics and Implica- Tions. Chin. Geogr. Sci. 2022, 32, 13. [Google Scholar]
- Zheng, B.; Tong, D.; Li, M.; Liu, F.; Hong, C.; Geng, G.; Li, H.; Li, X.; Peng, L.; Qi, J.; et al. Trends in China’s Anthropogenic Emissions since 2010 as the Consequence of Clean Air Actions. Atmos. Chem. Phys. 2018, 18, 14095–14111. [Google Scholar] [CrossRef]
- Lloyd, C.T.; Chamberlain, H.; Kerr, D.; Yetman, G.; Pistolesi, L.; Stevens, F.R.; Gaughan, A.E.; Nieves, J.J.; Hornby, G.; MacManus, K.; et al. Global Spatio-Temporally Harmonised Datasets for Producing High-Resolution Gridded Population Distribution Datasets. Big Earth Data 2019, 3, 108–139. [Google Scholar] [CrossRef]
- Wang, Q.-Y.; Zheng, K.-D.; Han, X.-S.; He, F.; Zhao, X.; Fan, P.-F.; Zhang, L. Site-Specific and Seasonal Variation in Habitat Use of Eurasian Otters (Lutra lutra) in Western China: Implications for Conservation. Zool. Res. 2021, 42, 824–832. [Google Scholar] [CrossRef]
- Environmental Systems Research Institute (ESRI). ArcGISDesktop; Environmental Systems Research Institute (ESRI): Redlands, CA, USA, 2018. [Google Scholar]
- Chuai, X.; Lu, Y.; Xie, F.; Yang, F.; Zhao, R.; Pang, B. A New Approach to Evaluate Regional Inequity Determined by PM2.5 Emissions and Concentrations. J. Environ. Manag. 2021, 277, 111335. [Google Scholar] [CrossRef]
- Zhu, F.; Chen, L.; Qian, Z.; Liao, Y.; Zhang, Z.; McMillin, S.E.; Wang, X.; Lin, H. Acute Effects of Particulate Matter with Different Sizes on Respiratory Mortality in Shenzhen, China. Environ. Sci. Pollut. Res. 2021, 28, 37195–37203. [Google Scholar] [CrossRef]
- Lu, X.; Lin, C.; Li, W.; Chen, Y.; Huang, Y.; Fung, J.C.H.; Lau, A.K.H. Analysis of the Adverse Health Effects of PM2.5 from 2001 to 2017 in China and the Role of Urbanization in Aggravating the Health Burden. Sci. Total Environ. 2019, 652, 683–695. [Google Scholar] [CrossRef]
- Chen, L.; Shi, M.; Gao, S.; Li, S.; Mao, J.; Zhang, H.; Sun, Y.; Bai, Z.; Wang, Z. Assessment of Population Exposure to PM2.5 for Mortality in China and Its Public Health Benefit Based on BenMAP. Environ. Pollut. 2017, 221, 311–317. [Google Scholar] [CrossRef]
- Cai, J.; Peng, C.; Yu, S.; Pei, Y.; Liu, N.; Wu, Y.; Fu, Y.; Cheng, J. Association between PM2.5 Exposure and All-Cause, Non-Accidental, Accidental, Different Respiratory Diseases, Sex and Age Mortality in Shenzhen, China. Int. J. Environ. Res. Public Health 2019, 16, 401. [Google Scholar] [CrossRef]
- Kim, H.; Byun, G.; Choi, Y.; Kim, S.; Kim, S.-Y.; Lee, J.-T. Effects of Long-Term Exposure to Air Pollution on All-Cause Mortality and Cause-Specific Mortality in Seven Major Cities of South Korea: Korean National Health and Nutritional Examination Surveys with Mortality Follow-Up. Environ. Res. 2021, 192, 110290. [Google Scholar] [CrossRef]
- Lu, F.; Xu, D.; Cheng, Y.; Dong, S.; Guo, C.; Jiang, X.; Zheng, X. Systematic Review and Meta-Analysis of the Adverse Health Effects of Ambient PM2.5 and PM10 Pollution in the Chinese Population. Environ. Res. 2015, 136, 196–204. [Google Scholar] [CrossRef]
- Zhao, H.; Chen, K.; Liu, Z.; Zhang, Y.; Shao, T.; Zhang, H. Coordinated Control of PM2.5 and O3 Is Urgently Needed in China after Implementation of the “Air Pollution Prevention and Control Action Plan”. Chemosphere 2021, 270, 129441. [Google Scholar] [CrossRef]
- Zhao, B.; Zheng, H.; Wang, S.; Smith, K.R.; Lu, X.; Aunan, K.; Gu, Y.; Wang, Y.; Ding, D.; Xing, J.; et al. Change in Household Fuels Dominates the Decrease in PM2.5 Exposure and Premature Mortality in China in 2005–2015. Proc. Natl. Acad. Sci. USA 2018, 115, 12401–12406. [Google Scholar] [CrossRef] [PubMed]
- Xue, T.; Liu, J.; Zhang, Q.; Geng, G.; Zheng, Y.; Tong, D.; Liu, Z.; Guan, D.; Bo, Y.; Zhu, T.; et al. Rapid Improvement of PM2.5 Pollution and Associated Health Benefits in China during 2013–2017. Sci. China Earth Sci. 2019, 62, 1847–1856. [Google Scholar] [CrossRef]
- Liu, H.; Liu, S.; Xue, B.; Lv, Z.; Meng, Z.; Yang, X.; Xue, T.; Yu, Q.; He, K. Ground-Level Ozone Pollution and Its Health Impacts in China. Atmos. Environ. 2018, 173, 223–230. [Google Scholar] [CrossRef]
- Kuerban, M.; Waili, Y.; Fan, F.; Liu, Y.; Qin, W.; Dore, A.J.; Peng, J.; Xu, W.; Zhang, F. Spatio-Temporal Patterns of Air Pollution in China from 2015 to 2018 and Implications for Health Risks. Environ. Pollut. 2020, 258, 113659. [Google Scholar] [CrossRef]
- Zeng, J.; Liu, T.; Feiock, R.; Li, F. The Impacts of China’s Provincial Energy Policies on Major Air Pollutants: A Spatial Econometric Analysis. Energy Policy 2019, 132, 392–403. [Google Scholar] [CrossRef]
- Bai, X.; Tian, H.; Liu, X.; Wu, B.; Liu, S.; Hao, Y.; Luo, L.; Liu, W.; Zhao, S.; Lin, S.; et al. Spatial-Temporal Variation Characteristics of Air Pollution and Apportionment of Contributions by Different Sources in Shanxi Province of China. Atmos. Environ. 2021, 244, 117926. [Google Scholar] [CrossRef]
- Liu, Q.; Zhang, Z.; Shao, C.; Zhao, R.; Guan, Y.; Chen, C. Spatio-Temporal Variation and Driving Factors Analysis of PM2.5 Health Risks in Chinese Cities. Ecol. Indic. 2021, 129, 107937. [Google Scholar] [CrossRef]
- Cao, L.; Wu, Y. Inequality of Pollutant Discharge in an Urban Agglomeration and Nonurban Agglomeration—Evidence from a New Theil-DEA Model. Environ. Sci. Pollut. Res. 2022, 29, 21876–21890. [Google Scholar] [CrossRef]
- Zhang, L. Exploration and Analysis on the Proportionality of Green Development Capability in Yangtze River Delta Region Based on Geordie Coefficient Method. Environ. Sustain. Dev. 2021, 46, 102–108. [Google Scholar]
- Tessum, C.W.; Paolella, D.A.; Chambliss, S.E.; Apte, J.S.; Hill, J.D.; Marshall, J.D. PM2.5 Polluters Disproportionately and Systemically Affect People of Color in the United States. Sci. Adv. 2021, 7, eabf4491. [Google Scholar] [CrossRef]
- Chen, L.; Lin, J.; Martin, R.; Du, M.; Weng, H.; Kong, H.; Ni, R.; Meng, J.; Zhang, Y.; Zhang, L.; et al. Inequality in Historical Transboundary Anthropogenic PM2.5 Health Impacts. Sci. Bull. 2022, 67, 437–444. [Google Scholar] [CrossRef]
- Guo, S.; Zheng, S.; Hu, Y.; Hong, J.; Wu, X.; Tang, M. Embodied Energy Use in the Global Construction Industry. Appl. Energy 2019, 256, 113838. [Google Scholar] [CrossRef]
- Zhong, Q.; Ma, J.; Shen, G.; Shen, H.; Zhu, X.; Yun, X.; Meng, W.; Cheng, H.; Liu, J.; Li, B.; et al. Distinguishing Emission-Associated Ambient Air PM2.5 Concentrations and Meteorological Factor-Induced Fluctuations. Environ. Sci. Technol. 2018, 52, 10416–10425. [Google Scholar] [CrossRef] [Green Version]
- Guan, Y.; Huang, G.; Liu, L.; Zhai, M.; Xu, X. Measurement of Air-Pollution Inequality through a Three-Perspective Accounting Model. Sci. Total Environ. 2019, 696, 133937. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Liu, P.; Song, H.; Miao, C.; Wang, F.; Xing, Y.; Wang, W.; Liu, X.; Zhao, M. Effects of Anthropogenic Emissions from Different Sectors on PM2.5 Concentrations in Chinese Cities. Int. J. Environ. Res. Public Health 2021, 18, 10869. [Google Scholar] [CrossRef]
- Cooper, N.; Green, D.; Knibbs, L.D. Inequalities in Exposure to the Air Pollutants PM2.5 and NO2 in Australia. Environ. Res. Lett. 2019, 14, 115005. [Google Scholar] [CrossRef]
- Qian, Y.; Behrens, P.; Tukker, A.; Rodrigues, J.F.D.; Li, P.; Scherer, L. Environmental Responsibility for Sulfur Dioxide Emissions and Associated Biodiversity Loss across Chinese Provinces. Environ. Pollut. 2019, 245, 898–908. [Google Scholar] [CrossRef]
- Liang, H.; Dong, L.; Luo, X.; Ren, J.; Zhang, N.; Gao, Z.; Dou, Y. Balancing Regional Industrial Development: Analysis on Regional Disparity of China’s Industrial Emissions and Policy Implications. J. Clean. Prod. 2016, 126, 223–235. [Google Scholar] [CrossRef]
- Yang, X.; Feng, K.; Su, B.; Zhang, W.; Huang, S. Environmental Efficiency and Equality Embodied in China’s Inter-Regional Trade. Sci. Total Environ. 2019, 672, 150–161. [Google Scholar] [CrossRef]
- Qin, Q.; Li, X.; Li, L.; Zhen, W.; Wei, Y.-M. Air Emissions Perspective on Energy Efficiency: An Empirical Analysis of China’s Coastal Areas. Appl. Energy 2017, 185, 604–614. [Google Scholar] [CrossRef]
- Yao, M.; Wu, G.; Zhao, X.; Zhang, J. Estimating Health Burden and Economic Loss Attributable to Short-Term Exposure to Multiple Air Pollutants in China. Environ. Res. 2020, 183, 109184. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cui, T.; Ye, Z.; Wang, Z.; Zhou, J.; He, C.; Hong, S.; Yang, L.; Niu, X.; Wu, Q. Inequalities in PM2.5 and SO2 Exposure Health Risks in Terms of Emissions in China, 2013–2017. Atmosphere 2022, 13, 1422. https://doi.org/10.3390/atmos13091422
Cui T, Ye Z, Wang Z, Zhou J, He C, Hong S, Yang L, Niu X, Wu Q. Inequalities in PM2.5 and SO2 Exposure Health Risks in Terms of Emissions in China, 2013–2017. Atmosphere. 2022; 13(9):1422. https://doi.org/10.3390/atmos13091422
Chicago/Turabian StyleCui, Tingting, Zhixiang Ye, Zongyu Wang, Jingcheng Zhou, Chao He, Song Hong, Lu Yang, Xiaoxiao Niu, and Qian Wu. 2022. "Inequalities in PM2.5 and SO2 Exposure Health Risks in Terms of Emissions in China, 2013–2017" Atmosphere 13, no. 9: 1422. https://doi.org/10.3390/atmos13091422
APA StyleCui, T., Ye, Z., Wang, Z., Zhou, J., He, C., Hong, S., Yang, L., Niu, X., & Wu, Q. (2022). Inequalities in PM2.5 and SO2 Exposure Health Risks in Terms of Emissions in China, 2013–2017. Atmosphere, 13(9), 1422. https://doi.org/10.3390/atmos13091422