
A Protocol for Organoids from the Urine of Bladder Cancer Patients

 , ,
, ,  ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Isolation of Cells from the Urine of Bladder Cancer Patients and Expansion of Cells in Organoid Cultures
2.2. Isolation of Cells from Urothelial Carcinoma Tissue from Bladder Cancer Patients and Expansion of Cells in Organoid Cultures
2.3. Immunohistochemistry and Immunofluorescence of Organoids
2.4. Software and Statistics
3. Results
3.1. Patient Characteristics
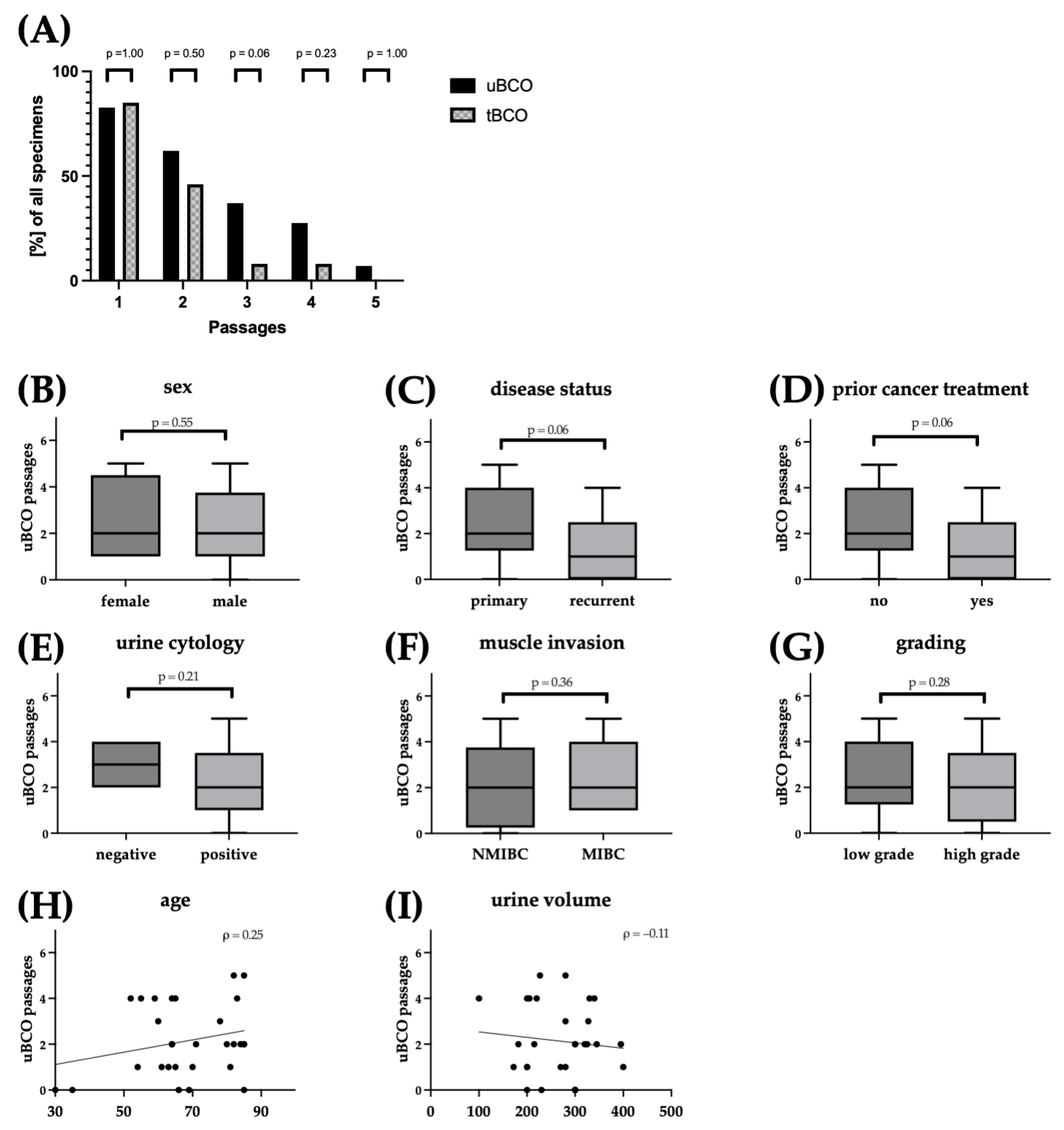
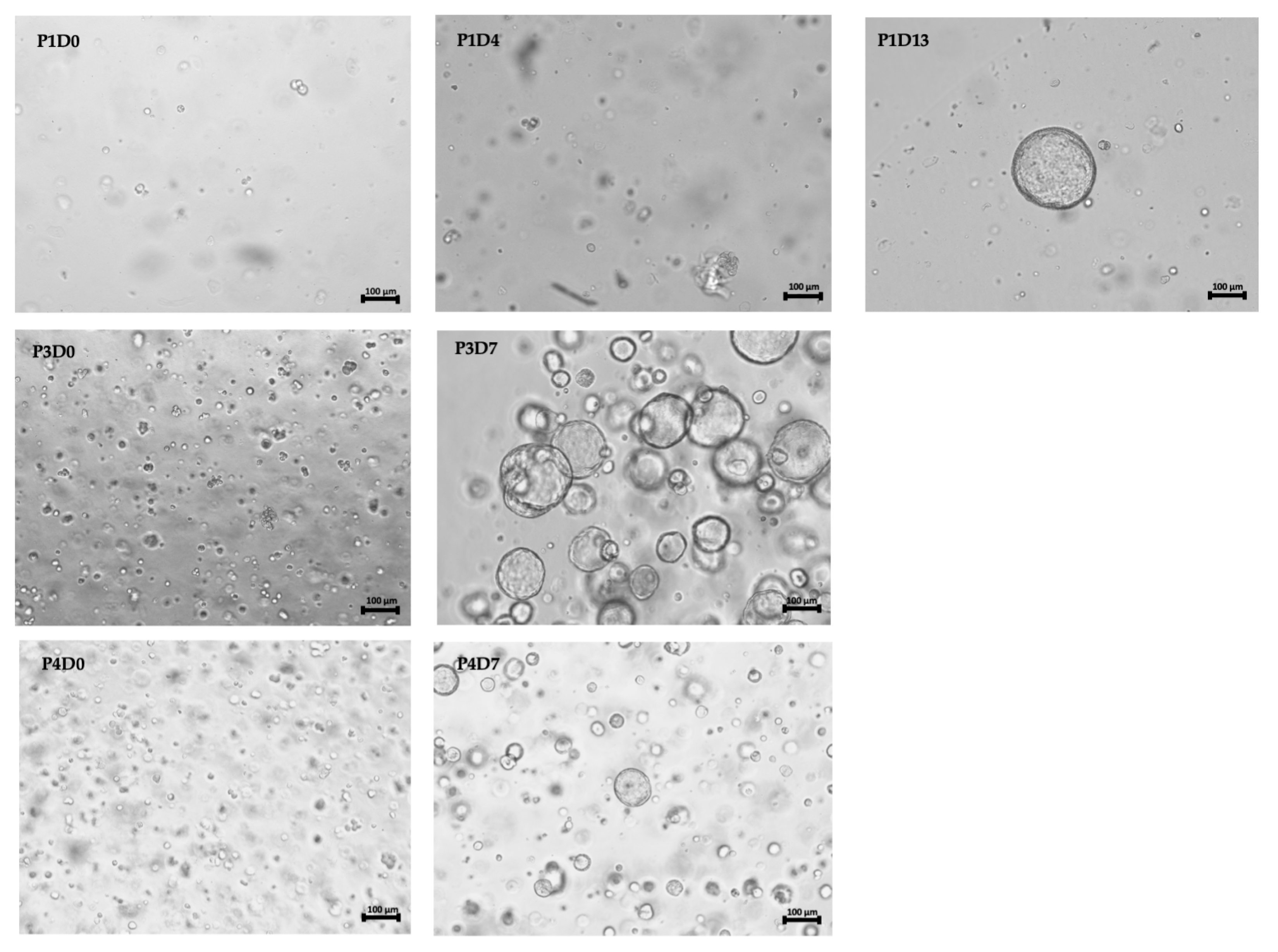
3.2. Efficient Culturing of Urine-Derived Bladder Cancer Organoids
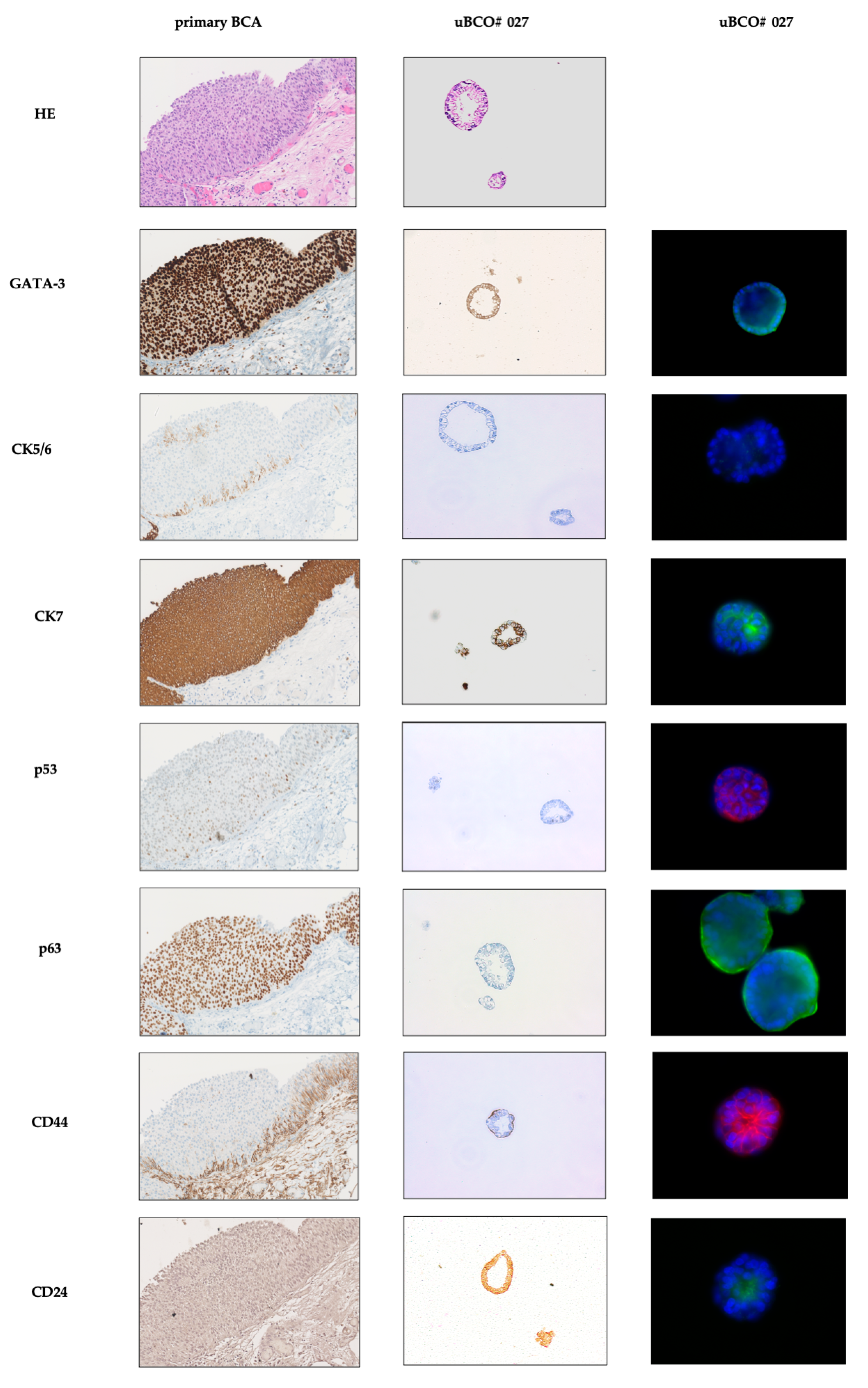
3.3. Urine-Derived Bladder Cancer Organoids Show Classical Features of Organoids and Mimic Primary Bladder Cancer
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [PubMed]
- Walz, S.; Aslani, V.; Sawodny, O.; Stenzl, A. Robotic radical cystectomy–more precision needed? Curr. Opin. Urol. 2023, 33, 157–162. [Google Scholar] [PubMed]
- Soukup, V.; Capoun, O.; Cohen, D.; Hernandez, V.; Babjuk, M.; Burger, M.; Comperat, E.; Gontero, P.; Lam, T.; MacLennan, S.; et al. Prognostic Performance and Reproducibility of the 1973 and 2004/2016 World Health Organization Grading Classification Systems in Non-muscle-invasive Bladder Cancer: A European Association of Urology Non-muscle Invasive Bladder Cancer Guidelines Panel Systematic Review. Eur. Urol. 2017, 72, 801–813. [Google Scholar] [PubMed]
- Huguet, J. Follow-up after radical cystectomy based on patterns of tumour recurrence and its risk factors. Actas Urol. Esp. 2013, 37, 376–382. [Google Scholar]
- Ghoneim, M.A.; Abdel-Latif, M.; el-Mekresh, M.; Abol-Enein, H.; Mosbah, A.; Ashamallah, A.; el-Baz, M.A. Radical cystectomy for carcinoma of the bladder: 2720 consecutive cases 5 years later. J. Urol. 2008, 180, 121–127. [Google Scholar]
- Sjodahl, G.; Abrahamsson, J.; Holmsten, K.; Bernardo, C.; Chebil, G.; Eriksson, P.; Johansson, I.; Kollberg, P.; Lindh, C.; Lovgren, K.; et al. Different Responses to Neoadjuvant Chemotherapy in Urothelial Carcinoma Molecular Subtypes. Eur. Urol. 2022, 81, 523–532. [Google Scholar]
- von der Maase, H.; Hansen, S.W.; Roberts, J.T.; Dogliotti, L.; Oliver, T.; Moore, M.J.; Bodrogi, I.; Albers, P.; Knuth, A.; Lippert, C.M.; et al. Gemcitabine and cisplatin versus methotrexate, vinblastine, doxorubicin, and cisplatin in advanced or metastatic bladder cancer: Results of a large, randomized, multinational, multicenter, phase III study. J. Clin. Oncol. 2000, 18, 3068–3077. [Google Scholar]
- Lancaster, M.A.; Knoblich, J.A. Organogenesis in a dish: Modeling development and disease using organoid technologies. Science 2014, 345, 1247125. [Google Scholar]
- Sato, T.; Stange, D.E.; Ferrante, M.; Vries, R.G.; Van Es, J.H.; Van den Brink, S.; Van Houdt, W.J.; Pronk, A.; Van Gorp, J.; Siersema, P.D.; et al. Long-term expansion of epithelial organoids from human colon, adenoma, adenocarcinoma, and Barrett’s epithelium. Gastroenterology 2011, 141, 1762–1772. [Google Scholar]
- Wei, Y.; Amend, B.; Todenhöfer, T.; Lipke, N.; Aicher, W.K.; Fend, F.; Stenzl, A.; Harland, N. Urinary Tract Tumor Organoids Reveal Eminent Differences in Drug Sensitivities When Compared to 2-Dimensional Culture Systems. Int. J. Mol. Sci. 2022, 23, 6305. [Google Scholar]
- Clevers, H. Modeling Development and Disease with Organoids. Cell 2016, 165, 1586–1597. [Google Scholar]
- Kim, E.; Choi, S.; Kang, B.; Kong, J.; Kim, Y.; Yoon, W.H.; Lee, H.R.; Kim, S.; Kim, H.M.; Lee, H.; et al. Creation of bladder assembloids mimicking tissue regeneration and cancer. Nature 2020, 588, 664–669. [Google Scholar]
- Lee, S.H.; Hu, W.; Matulay, J.T.; Silva, M.V.; Owczarek, T.B.; Kim, K.; Chua, C.W.; Barlow, L.J.; Kandoth, C.; Williams, A.B.; et al. Tumor Evolution and Drug Response in Patient-Derived Organoid Models of Bladder Cancer. Cell 2018, 173, 515–528 e17. [Google Scholar]
- Drost, J.; Clevers, H. Organoids in cancer research. Nat. Rev. Cancer 2018, 18, 407–418. [Google Scholar]
- Pasch, C.A.; Favreau, P.F.; Yueh, A.E.; Babiarz, C.P.; Gillette, A.A.; Sharick, J.T.; Karim, M.R.; Nickel, K.P.; DeZeeuw, A.K.; Sprackling, C.M.; et al. Patient-Derived Cancer Organoid Cultures to Predict Sensitivity to Chemotherapy and Radiation. Clin. Cancer Res. 2019, 25, 5376–5387. [Google Scholar]
- Hill, S.J.; Decker, B.; Roberts, E.A.; Horowitz, N.S.; Muto, M.G.; Worley, M.J., Jr.; Feltmate, C.M.; Nucci, M.R.; Swisher, E.M.; Nguyen, H. Prediction of DNA repair inhibitor response in short-term patient-derived ovarian cancer organoids. Cancer Discov. 2018, 8, 1404–1421. [Google Scholar]
- Minoli, M.; Cantore, T.; Hanhart, D.; Kiener, M.; Fedrizzi, T.; La Manna, F.; Karkampouna, S.; Chouvardas, P.; Genitsch, V.; Rodriguez-Calero, A. Bladder cancer organoids as a functional system to model different disease stages and therapy response. Nat. Commun. 2023, 14, 2214. [Google Scholar]
- Yao, Y.; Xu, X.; Yang, L.; Zhu, J.; Wan, J.; Shen, L.; Xia, F.; Fu, G.; Deng, Y.; Pan, M. Patient-derived organoids predict chemoradiation responses of locally advanced rectal cancer. Cell Stem Cell 2020, 26, 17–26.e6. [Google Scholar]
- Pauli, C.; Hopkins, B.D.; Prandi, D.; Shaw, R.; Fedrizzi, T.; Sboner, A.; Sailer, V.; Augello, M.; Puca, L.; Rosati, R. Personalized In Vitro and In Vivo Cancer Models to Guide Precision MedicinePersonalized Cancer Models to Guide Precision Medicine. Cancer Discov. 2017, 7, 462–477. [Google Scholar]
- Medle, B.; Sjödahl, G.; Eriksson, P.; Liedberg, F.; Höglund, M.; Bernardo, C. Patient-derived bladder cancer organoid models in tumor biology and drug testing: A systematic review. Cancers 2022, 14, 2062. [Google Scholar]
- Grossman, H.B.; Soloway, M.; Messing, E.; Katz, G.; Stein, B.; Kassabian, V.; Shen, Y. Surveillance for recurrent bladder cancer using a point-of-care proteomic assay. JAMA 2006, 295, 299–305. [Google Scholar] [CrossRef]
- Veeramachaneni, R.; Nordberg, M.L.; Shi, R.; Herrera, G.A.; Turbat-Herrera, E.A. Evaluation of fluorescence in situ hybridization as an ancillary tool to urine cytology in diagnosing urothelial carcinoma. Diagn. Cytopathol. 2003, 28, 301–307. [Google Scholar] [CrossRef]
- Farrow, G.M. Urine cytology in the detection of bladder cancer: A critical approach. J. Occup. Med. 1990, 32, 817–821. [Google Scholar] [CrossRef]
- Elbadawy, M.; Usui, T.; Mori, T.; Tsunedomi, R.; Hazama, S.; Nabeta, R.; Uchide, T.; Fukushima, R.; Yoshida, T.; Shibutani, M. Establishment of a novel experimental model for muscle-invasive bladder cancer using a dog bladder cancer organoid culture. Cancer Sci. 2019, 110, 2806–2821. [Google Scholar] [CrossRef]
- Geng, R.; Harland, N.; Montes-Mojarro, I.A.; Fend, F.; Aicher, W.K.; Stenzl, A.; Amend, B. CD24: A Marker for an Extended Expansion Potential of Urothelial Cancer Cell Organoids In Vitro? Int. J. Mol. Sci. 2022, 23, 5453. [Google Scholar] [CrossRef]
- Mullenders, J.; de Jongh, E.; Brousali, A.; Roosen, M.; Blom, J.P.A.; Begthel, H.; Korving, J.; Jonges, T.; Kranenburg, O.; Meijer, R.; et al. Mouse and human urothelial cancer organoids: A tool for bladder cancer research. Proc. Natl. Acad. Sci. USA 2019, 116, 4567–4574. [Google Scholar] [CrossRef]
- Yu, L.; Li, Z.; Mei, H.; Li, W.; Chen, D.; Liu, L.; Zhang, Z.; Sun, Y.; Song, F.; Chen, W.; et al. Patient-derived organoids of bladder cancer recapitulate antigen expression profiles and serve as a personal evaluation model for CAR-T cells in vitro. Clin. Transl. Immunol. 2021, 10, e1248. [Google Scholar] [CrossRef]
- Jiang, J.; Ulbright, T.M.; Younger, C.; Sanchez, K.; Bostwick, D.G.; Koch, M.O.; Eble, J.N.; Cheng, L. Cytokeratin 7 and cytokeratin 20 in primary urinary bladder carcinoma and matched lymph node metastasis. Arch. Pathol. Lab. Med. 2001, 125, 921–923. [Google Scholar] [CrossRef]
- Ravanini, J.N.; Assato, A.K.; Wakamatsu, A.; Alves, V.A.F. Combined use of immunohistochemical markers of basal and luminal subtypes in urothelial carcinoma of the bladder: Association with clinicopathological features and outcomes. Clinics 2021, 76, e2587. [Google Scholar] [CrossRef]
- Agarwal, H.; Babu, S.; Rana, C.; Kumar, M.; Singhai, A.; Shankhwar, S.N.; Singh, V.; Sinha, R.J. Diagnostic utility of GATA3 immunohistochemical expression in urothelial carcinoma. Indian J. Pathol. Microbiol. 2019, 62, 244–250. [Google Scholar]
- Abugomaa, A.; Elbadawy, M.; Yamawaki, H.; Usui, T.; Sasaki, K. Emerging Roles of Cancer Stem Cells in Bladder Cancer Progression, Tumorigenesis, and Resistance to Chemotherapy: A Potential Therapeutic Target for Bladder Cancer. Cells 2020, 9, 235. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex (n) | |
| female | 5 |
| male | 24 |
| Age (years) | |
| Median | 66 |
| Range | (30–85) |
| Urine volume (mL) | |
| Median | 280 |
| Range | (172–400) |
| Tissue acquisition | |
| TURBT | 28 |
| Cystectomy | 1 |
| Disease status | |
| Primary diagnosis | 16 |
| Relapse | 13 |
| Pathological features | |
| CIS * | 3 |
| pTa | 16 |
| pT1 | 4 |
| pT2 | 8 |
| pT3 | 0 |
| pT4 | 1 |
| low grade | 12 |
| high grade | 17 |
| Urine cytology | |
| negative | 4 |
| positive | 21 |
| unkown | 4 |
| Prior cancer treatment | |
| non | 16 |
| TURBT | 10 |
| Mitomycin instillation | 1 |
| BCG instillation | 1 |
| neoadj. chemotherapy | 1 |
| Primary Culture (Wells) | 1. Passage (Wells) | Δ (%) | |
|---|---|---|---|
| uBCO #001 | 7 | 8 | +14 |
| tBCO #001 | 6 | 0 | −100 |
| uBCO #002 | 7 | 7 | 0 |
| tBCO #002 | 6 | 7 | +17 |
| uBCO #003 | 7 | 7 | 0 |
| tBCO #003 | 7 | 8 | +14 |
| uBCO #004 | 6 | 7 | +17 |
| tBCO #004 | 6 | 8 | +33 |
| uBCO #005 | 6 | 10 | +66 |
| tBCO #005 | 6 | 6 | +17 |
| uBCO #006 | 6 | 11 | +83 |
| tBCO #006 | 6 | 7 | +17 |
| uBCO #007 | 7 | 6 | −14 |
| tBCO #007 | 6 | 6 | 0 |
| uBCO #008 | 26 | 0 | −100 |
| tBCO #008 | 3 | 0 | −100 |
| uBCO #009 | 5 | 7 | +40 |
| tBCO #009 | 7 | 3 | −57 |
| uBCO #010 | 29 | 7 | −76 |
| tBCO #010 | 6 | 21 | +250 |
| uBCO #011 | 28 | 21 | −25 |
| tBCO #011 | 6 | 9 | +50 |
| uBCO #013 | uBCO #015 | uBCO #019 | uBCO #022 | uBCO #027 | uBCO #028 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SS in ms | SS in ms | SS in ms | SS in ms | SS in ms | SS in ms | |||||||
| GATA-3 | + | 1638–2636 | +/− | 1000 | + | 1179–5000 | + | 1629–5083 | + | 668–1160 | − | 1000 |
| AE1/AE3 | + | 363–524 | + | 108–1000 | + | 129–519 | + | 124–511 | + | 422–575 | + | 252–978 |
| CK7 | + | 398–804 | + | 147–1000 | + | 177–217 | + | 150–199 | +/− | 210–859 | + | 258–1000 |
| p53 | +/− | 3000 | +/− | 1000 | + | 3000 | + | 3489–4038 | +/− | 569–2000 | +/− | 1000 |
| TP63 | + | 1792–3000 | − | 1000 | + | 308–3000 | − | 5000 | + | 2000 | +/− | 1000 |
| Vimentin | + | 1378–3000 | +/− | 1000 | − | 3000 | − | 5000 | + | 1589–2000 | − | 1000 |
| S100P | − | 3000 | +/− | 521–1000 | + | 114–423 | + | 571–1452 | + | 1624–2000 | + | 233–729 |
| CK5 | + | 2076–3000 | − | 1000 | − | 3000 | − | 5000 | + | 2000 | − | 1000 |
| CK20 | − | 3000 | +/− | 1000 | + | 302–1493 | − | 5000 | − | 2000 | + | 1000 |
| CD276 | − | 3000 | +/− | 1000 | + | 981–3000 | + | 266–4714 | + | 747–859 | − | 1000 |
| CD24 | − | 3000 | − | 1000 | − | 3000 | +/− | 579–5000 | +/− | 2000 | − | 1000 |
| CD44 | − | 3000 | +/− | 1000 | +/− | 3000 | − | 3892–5000 | + | 179–500 | +/− | 386–402 |
| Ki67 | n.a. | + | 1000 | + | 240–545 | + | 400–1000 | + | 353–911 | n.a. | ||
| FGFR3 | − | 3000 | − | 1000 | − | 3000 | n.a. | − | 2000 | n.a. | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Walz, S.; Pollehne, P.; Geng, R.; Schneider, J.; Maas, M.; Aicher, W.K.; Stenzl, A.; Amend, B.; Harland, N. A Protocol for Organoids from the Urine of Bladder Cancer Patients. Cells 2023, 12, 2188. https://doi.org/10.3390/cells12172188
Walz S, Pollehne P, Geng R, Schneider J, Maas M, Aicher WK, Stenzl A, Amend B, Harland N. A Protocol for Organoids from the Urine of Bladder Cancer Patients. Cells. 2023; 12(17):2188. https://doi.org/10.3390/cells12172188
Chicago/Turabian StyleWalz, Simon, Paul Pollehne, Ruizhi Geng, Johannes Schneider, Moritz Maas, Wilhelm K. Aicher, Arnulf Stenzl, Bastian Amend, and Niklas Harland. 2023. "A Protocol for Organoids from the Urine of Bladder Cancer Patients" Cells 12, no. 17: 2188. https://doi.org/10.3390/cells12172188
APA StyleWalz, S., Pollehne, P., Geng, R., Schneider, J., Maas, M., Aicher, W. K., Stenzl, A., Amend, B., & Harland, N. (2023). A Protocol for Organoids from the Urine of Bladder Cancer Patients. Cells, 12(17), 2188. https://doi.org/10.3390/cells12172188