BRCA Detection Rate in an Italian Cohort of Luminal Early-Onset and Triple-Negative Breast Cancer Patients without Family History: When Biology Overcomes Genealogy

 , , ,
, , ,  , , ,
, , ,  ,
,
Abstract
1. Introduction
2. Results
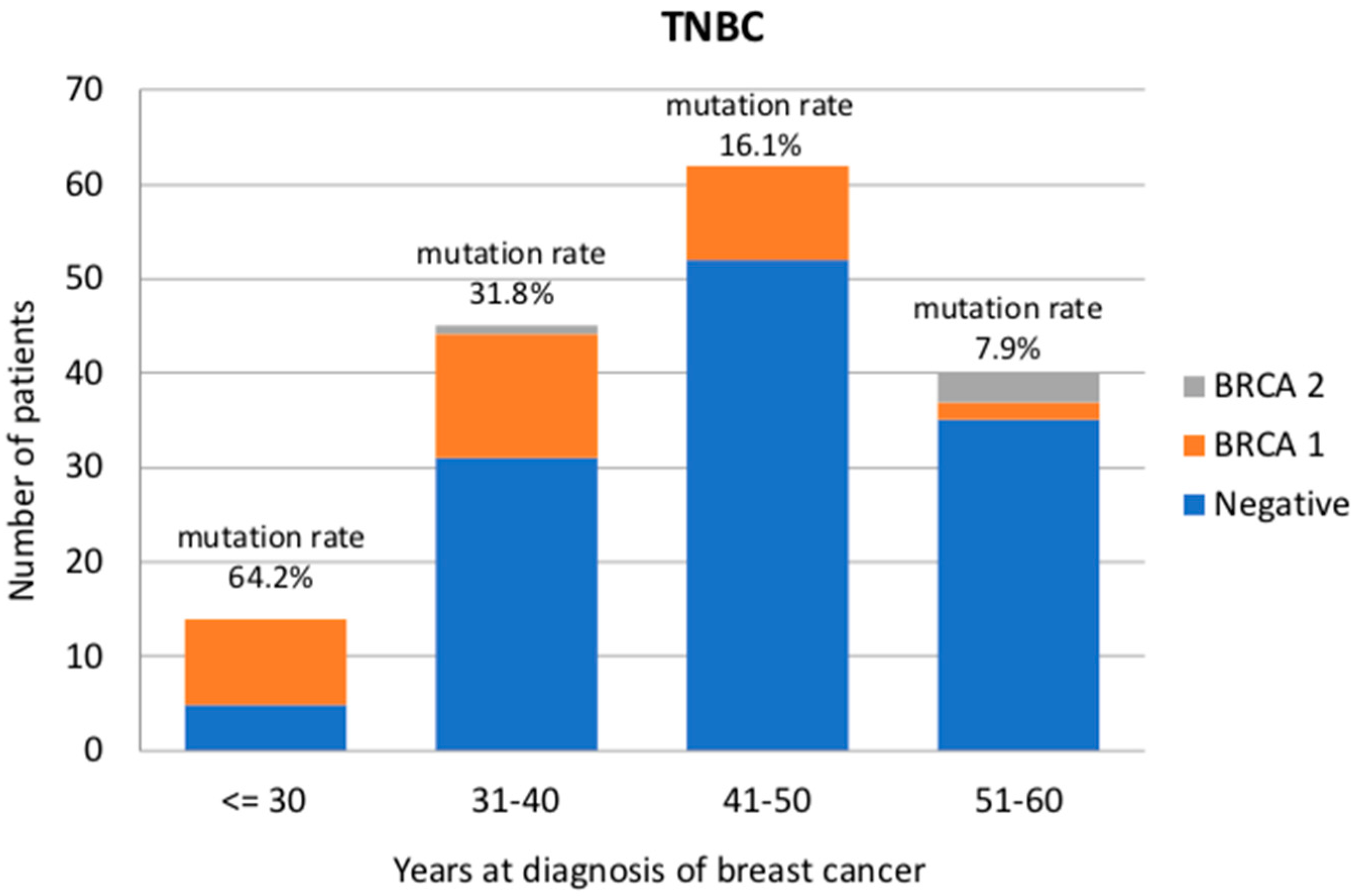
2.1. Triple-Negative Breast Cancer
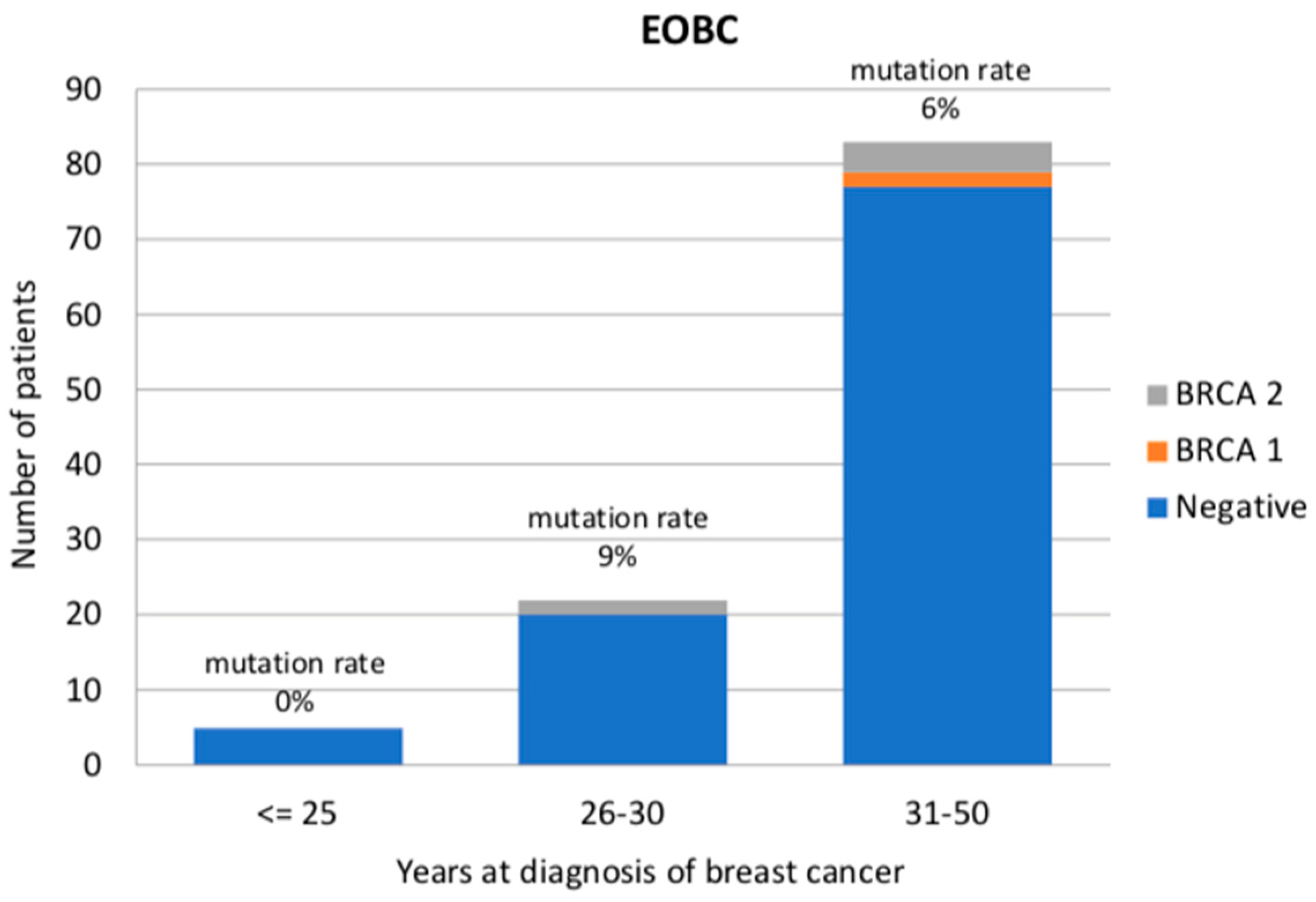
2.2. Early-Onset Luminal-like Breast Cancer
3. Discussion
4. Materials and Methods
4.1. Study Population and Design
4.2. BRCA Testing Procedures
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Toss, A.; Molinaro, E.; Sammarini, M.; Del Savio, M.C.; Cortesi, L.; Facchinetti, F.; Grandi, G. Hereditary ovarian cancers: State of the art. Minerva Med. 2019, 110, 301–319. [Google Scholar] [CrossRef]
- Toss, A.; Venturelli, M.; Molinaro, E.; Pipitone, S.; Barbieri, E.; Marchi, I.; Tenedini, E.; Artuso, L.; Castellano, S.; Marino, M.; et al. Hereditary Pancreatic Cancer: A Retrospective Single-Center Study of 5143 Italian Families with History of BRCA-Related Malignancies. Cancers 2019, 11, 193. [Google Scholar] [CrossRef]
- Lecarpentier, J.; Silvestri, V.; Kuchenbaecker, K.B.; Barrowdale, D.; Dennis, J.; McGuffog, L.; Soucy, P.; Leslie, G.; Rizzolo, P.; Navazio, A.S.; et al. Prediction of Breast and Prostate Cancer Risks in Male BRCA1 and BRCA2 Mutation Carriers Using Polygenic Risk Scores. J. Clin. Oncol. 2017, 35, 2240–2250. [Google Scholar] [CrossRef]
- Kuchenbaecker, K.B.; Hopper, J.L.; Barnes, D.R.; Phillips, K.A.; Mooij, T.M.; Roos-Blom, M.J.; Jervis, S.; van Leeuwen, F.E.; Milne, R.L.; Andrieu, N.; et al. Risks of Breast, Ovarian, and Contralateral Breast Cancer for BRCA1 and BRCA2 Mutation Carriers. JAMA 2017, 317, 2402–2416. [Google Scholar] [CrossRef]
- Grandi, G.; Sammarini, M.; Del Savio, M.C.; Toss, A.; Facchinetti, F. Combined hormonal contraceptives in BRCA gene mutation carriers: Why not? Eur. J. Contracept. Reprod Health Care 2019, 24, 417–419. [Google Scholar] [CrossRef]
- Cortesi, L.; Canossi, B.; Battista, R.; Pecchi, A.; Drago, A.; Dal Molin, C.; Toss, A.; De Matteis, E.; Marchi, I.; Torricelli, P.; et al. Breast ultrasonography (BU) in the screening protocol for women at hereditary-familial risk of breast cancer: Has the time come to rethink the role of BU according to different risk categories? Int. J. Cancer 2019, 144, 1001–1009. [Google Scholar] [CrossRef]
- Cortesi, L.; De Matteis, E.; Toss, A.; Marchi, I.; Medici, V.; Contu, G.; Xholli, A.; Grandi, G.; Cagnacci, A.; Federico, M. Evaluation of Transvaginal Ultrasound plus CA-125, Measurement and Prophylactic Salpingo-Oophorectomy in Women at Different Risk Levels of Ovarian Cancer: The Modena Study Group Cohort Study. Oncology 2017, 93, 377–386. [Google Scholar] [CrossRef]
- Toss, A.; Grandi, G.; Cagnacci, A.; Marcheselli, L.; Pavesi, S.; De Matteis, E.; Razzaboni, E.; Tomasello, C.; Cascinu, S.; Cortesi, L. The impact of reproductive life on breast cancer risk in women with family history or BRCA mutation. Oncotarget 2017, 8, 9144–9154. [Google Scholar] [CrossRef]
- Razzaboni, E.; Toss, A.; Cortesi, L.; Marchi, I.; Sebastiani, F.; De Matteis, E.; Federico, M. Acceptability and adherence in a chemoprevention trial among women at increased risk for breast cancer attending the Modena Familial Breast and Ovarian Cancer Center (Italy). Breast J. 2013, 19, 10–21. [Google Scholar] [CrossRef]
- Patel, V.L.; Busch, E.L.; Friebel, T.M.; Cronin, A.; Leslie, G.; McGuffog, L.; Adlard, J.; Agata, S.; Agnarsson, B.A.; Ahmed, M.; et al. Association of Genomic Domains in BRCA1 and BRCA2 with Prostate Cancer Risk and Aggressiveness. Cancer Res. 2020, 80, 624–638. [Google Scholar] [CrossRef]
- Cortesi, L.; Toss, A.; Cucinotto, I. PARP Inhibitors for the Treatment of Ovarian Cancer. Curr. Cancer Drug Targets 2018, 18, 877–893. [Google Scholar] [CrossRef]
- NICE Guideline. Familial Breast Cancer: Classification, Care and Managing Breast Cancer and Related Risks in People with a Family History of Breast Cancer. Available online: www.nice.org.uk/guidance/cg164 (accessed on 20 November 2019).
- NCCN Clinical Practice Guidelines in Oncology. Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic Version 1.2020. Available online: https://www.nccn.org/professionals/physician_gls/pdf/genetics_bop.pdf (accessed on 4 December 2019).
- Berliner, J.L.; Fay, A.M. Practice Issues Subcommittee of the National Society of Genetic Counselors’ Familial Cancer Risk Counseling Special Interest Group. Risk assessment and genetic counseling for hereditary breast and ovarian cancer: Recommendations of the National Society of Genetic Counselors. J. Genet. Couns. 2007, 16, 241–260. [Google Scholar]
- Calzone, K.A.; Soballe, P.W. Genetic testing for cancer susceptibility. Surg. Clin. N. Am. 2008, 88, 705–721. [Google Scholar] [CrossRef]
- AIOM Guidelines 2019. Neoplasie Della Mammella. Available online: https://www.aiom.it/wp-content/uploads/2019/10/2019_LG_AIOM_Mammella.pdf (accessed on 25 October 2019).
- Weitzel, J.N.; Lagos, V.I.; Cullinane, C.A.; Gambol, P.J.; Culver, J.O.; Blazer, K.R.; Palomares, M.R.; Lowstuter, K.J.; MacDonald, D.J. Limited family structure and BRCA gene mutation status in single cases of breast cancer. JAMA 2007, 297, 2587–2595. [Google Scholar] [CrossRef]
- Kemp, Z.; Turnbull, A.; Yost, S.; Seal, S.; Mahamdallie, S.; Poyastro-Pearson, E.; Warren-Perry, M.; Eccleston, A.; Tan, M.M.; Teo, S.H.; et al. Evaluation of Cancer-Based Criteria for Use in Mainstream BRCA1 and BRCA2 Genetic Testing in Patients With Breast Cancer. JAMA Netw. Open 2019, 2, e194428. [Google Scholar] [CrossRef]
- Turnbull, C.; Sud, A.; Houlston, R.S. Cancer genetics, precision prevention and a call to action. Nat. Genet. 2018, 50, 1212–1218. [Google Scholar] [CrossRef]
- Turchetti, D.; Cortesi, L.; Federico, M.; Bertoni, C.; Mangone, L.; Ferrari, S.; Silingardi, V. BRCA1 mutations and clinicopathological features in a sample of Italian women with early-onset breast cancer. Eur. J. Cancer 2000, 36, 2083–2089. [Google Scholar] [CrossRef]
- Honrado, E.; Benítez, J.; Palacios, J. Histopathology of BRCA1- and BRCA2-associated breast cancer. Crit. Rev. Oncol. Hematol. 2006, 59, 27–39. [Google Scholar] [CrossRef]
- Lakhani, S.R.; Gusterson, B.A.; Jacquemier, J.; Sloane, J.P.; Anderson, T.J.; van de Vijver, M.J.; Venter, D.; Freeman, A.; Antoniou, A.; McGuffog, L.; et al. The pathology of familial breast cancer: Histological features of cancers in families not attributable to mutations in BRCA1 or BRCA2. Clin. Cancer Res. 2000, 6, 782–789. [Google Scholar]
- Litton, J.K.; Ready, K.; Chen, H.; Gutierrez-Barrera, A.; Etzel, C.J.; Meric-Bernstam, F.; Gonzalez-Angulo, A.M.; Le-Petross, H.; Lu, K.; Hortobagyi, G.N.; et al. Earlier age of onset of BRCA mutation-related cancers in subsequent generations. Cancer 2012, 118, 321–325. [Google Scholar] [CrossRef]
- Greenup, R.; Buchanan, A.; Lorizio, W.; Rhoads, K.; Chan, S.; Leedom, T.; King, R.; McLennan, J.; Crawford, B.; Kelly Marcom, P.; et al. Prevalence of BRCA mutations among women with triple-negative breast cancer (TNBC) in a genetic counseling cohort. Ann. Surg. Oncol. 2013, 20, 3254–3258. [Google Scholar] [CrossRef]
- Sharma, P.; Klemp, J.R.; Kimler, B.F.; Mahnken, J.D.; Geier, L.J.; Khan, Q.J.; Elia, M.; Connor, C.S.; McGinness, M.K.; Mammen, J.M.; et al. Germline BRCA mutation evaluation in a prospective triple-negative breast cancer registry: Implications for hereditary breast and/or ovarian cancer syndrome testing. Breast Cancer Res. Treat. 2014, 145, 707–714. [Google Scholar] [CrossRef]
- Muendlein, A.; Rohde, B.H.; Gasser, K.; Haid, A.; Rauch, S.; Kinz, E.; Drexel, H.; Hofmann, W.; Schindler, V.; Kapoor, R.; et al. Evaluation of BRCA1/2 mutational status among German and Austrian women with triple-negative breast cancer. J. Cancer Res. Clin. Oncol. 2015, 141, 2005–2012. [Google Scholar] [CrossRef]
- Engel, C.; Rhiem, K.; Hahnen, E.; Loibl, S.; Weber, K.E.; Seiler, S.; Zachariae, S.; Hauke, J.; Wappenschmidt, B.; Waha, A.; et al. Prevalence of pathogenic BRCA1/2 germline mutations among 802 women with unilateral triple-negative breast cancer without family cancer history. BMC Cancer 2018, 18, 265. [Google Scholar] [CrossRef]
- Allison, K.H.; Hammond, M.E.H.; Dowsett, M.; McKernin, S.E.; Carey, L.A.; Fitzgibbons, P.L.; Hayes, D.F.; Lakhani, S.R.; Chavez-MacGregor, M.; Perlmutter, J.; et al. Estrogen and Progesterone Receptor Testing in Breast Cancer: ASCO/CAP Guideline Update. J. Clin. Oncol. 2020, JCO1902309. [Google Scholar] [CrossRef]
- Fujii, T.; Kogawa, T.; Dong, W.; Sahin, A.A.; Moulder, S.; Litton, J.K.; Tripathy, D.; Iwamoto, T.; Hunt, K.K.; Pusztai, L.; et al. Revisiting the definition of estrogen receptor positivity in HER2-negative primary breast cancer. Ann. Oncol. 2017, 28, 2420–2428. [Google Scholar] [CrossRef]
- Cortesi, L.; Razzaboni, E.; Toss, A.; De Matteis, E.; Marchi, I.; Medici, V.; Tazzioli, G.; Andreotti, A.; De Santis, G.; Pignatti, M.; et al. Rapid genetic counselling and testing in newly diagnosed breast cancer is associated with high rate of risk-reducing mastectomy in BRCA1/2-positive Italian women. Ann. Oncol. 2014, 25, 57–63. [Google Scholar] [CrossRef]
- Copson, E.R.; Maishman, T.C.; Tapper, W.J.; Cutress, R.I.; Greville-Heygate, S.; Altman, D.G.; Eccles, B.; Gerty, S.; Durcan, L.T.; Jones, L.; et al. Germline BRCA mutation and outcome in young-onset breast cancer (POSH): A prospective cohort study. Lancet Oncol. 2018, 19, 169–180. [Google Scholar] [CrossRef]
- Litton, J.K.; Rugo, H.S.; Ettl, J.; Hurvitz, S.A.; Gonçalves, A.; Lee, K.H.; Fehrenbacher, L.; Yerushalmi, R.; Mina, L.A.; Martin, M.; et al. Talazoparib in Patients with Advanced Breast Cancer and a Germline BRCA Mutation. N. Engl. J. Med. 2018, 379, 753–763. [Google Scholar] [CrossRef]
- Federico, M.; Maiorana, A.; Mangone, L.; Turchetti, D.; Canossi, B.; Romagnoli, R.; Silingardi, V. Identification of families with hereditary breast and ovarian cancer for clinical and mammographic surveillance: The Modena Study Group proposal. Breast Cancer Res. Treat. 1999, 55, 213–221. [Google Scholar] [CrossRef]
- Cortesi, L.; Turchetti, D.; Marchi, I.; Fracca, A.; Canossi, B.; Rachele, B.; Silvia, R.; Rita, P.A.; Pietro, T.; Massimo, F. Breast cancer screening in women at increased risk according to different family histories: An update of the Modena Study Group experience. BMC Cancer 2006, 6, 210. [Google Scholar] [CrossRef]
- Tyrer, J.; Duffy, S.W.; Cuzick, J. A breast cancer prediction model incorporating familial and personal risk factors. Stat. Med. 2004, 23, 1111–1130. [Google Scholar] [CrossRef]
- Wang, K.; Li, M.; Hakonarson, H. ANNOVAR: Functional annotation of genetic variants from high-throughput sequencing data. Nucleic Acids Res. 2010, 38, e164. [Google Scholar] [CrossRef]
- McLaren, W.; Pritchard, B.; Rios, D.; Chen, Y.; Flicek, P.; Cunningham, F. Deriving the consequences of genomic variants with the Ensembl API and SNP Effect Predictor. Bioinformatics 2010, 26, 2069–2070. [Google Scholar] [CrossRef]
- Artusi, V.; Chiesi, L.; Bernardis, I.; Tenedini, E.; Artuso, L.; Cavallini, G.M.; Percesepe, A.; Marigo, V.; Tagliafico, E. A Next Generation Sequencing amplicon-based strategy to explore inherited Retinal Degeneration complexity. Eur. J. Hum. Gen. 2015, 23, 1. [Google Scholar]
- Tenedini, E.; Artuso, L.; Bernardis, I.; Artusi, V.; Percesepe, A.; De Rosa, L.; Contini, R.; Manfredini, R.; Pellacani, G.; Pagani, J. Amplicon-based next-generation sequencing: An effective approach for the molecular diagnosis of epidermolysis bullosa. Br. J. Dermatol. 2015, 173, 731–738. [Google Scholar] [CrossRef]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and guidelines for the interpretation of sequence variants: A joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 2015, 17, 405–424. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| TNBC | Negative | BRCA1 | BRCA2 | p-Value | |
|---|---|---|---|---|---|
| Number of patients (159) | 123 | 34 | 2 | * | ** |
| Mean age at diagnosis (y) | 44.78 (24–59) SD 9.07 | 36.97 (26–54) SD 8.74 | 45.00 (39–51) SD 8.48 | 0.004 | <0.001 |
| Age group (y) | <0.001 | <0.001 | |||
| ≤30 | 5 (4.0%) | 9 (26.5%) | 0 | ||
| 31–40 | 31 (25.2%) | 13 (38.3%) | 1 (50%) | ||
| 41–50 | 52 (42.3%) | 10 (29.4%) | 0 | ||
| 51–60 | 35 (28.5%) | 2 (5.9%) | 1 (50%) | ||
| Ki 67 (%) | 0.508 | 0.462 | |||
| ≤20 | 11 (10.1%) | 1 (3.3%) | 0 | ||
| >20 | 98 (89.9%) | 29 (96.7%) | 1 (100%) | ||
| unknown | 14 | 4 | 1 | ||
| Bilaterality | 0.193 | 0.088 | |||
| Yes | 5 (4.2%) | 4 (12.9%) | 0 | ||
| No | 114 (95.7%) | 27 (87.1%) | 2 (100%) | ||
| unknown | 4 | 3 | 0 | ||
| Histotype | 0.466 | 0.301 | |||
| ductal | 103 (95.4%) | 28 (90.3%) | 2 (100%) | ||
| lobular | 0 | 1 (3.2%) | 0 | ||
| others | 5 (4.6%) | 2 (6.5%) | 0 | ||
| unknown | 15 | 3 | 0 | ||
| RO | 0.321 | 0.226 | |||
| negative | 116 (95.1%) | 30 (88.2%) | 2 (100%) | ||
| 1–9 % | 6 (4.9%) | 4 (11.8%) | 0 | ||
| unknown | 1 | 0 | 0 | ||
| EOBC | Negative | BRCA1 | BRCA2 | p-Value |
|---|---|---|---|---|
| Number of patients (109) | 102 | 2 | 5 | * |
| Mean age at diagnosis (y) | 31.95 (23–35) SD 2.85 | 34.0 (33–35) SD 2.93 | 30.6 (27–33) SD 2.89 | 0.488 |
| Age group (y) | 0.688 | |||
| ≤25 | 5 (4.9%) | 0 | 0 | |
| 26–30 | 20 (19.6%) | 0 | 2 (40%) | |
| 31–35 | 77 (75.5%) | 2 (100%) | 3 (60%) | |
| Ki 67 (%) | 0.920 | |||
| ≤20 | 35 (44.9%) | 0 | 2 (50%) | |
| >20 | 43 (55.1%) | 1 (100%) | 2 (50%) | |
| unknown | 24 | 1 | 1 | |
| Bilaterality | 0.249 | |||
| Yes | 5 (5.3%) | 1 (50%) | 0 | |
| No | 90 (94.7%) | 1 (50%) | 5 (100%) | |
| unknown | 7 | 0 | 0 | |
| Histotype | 1.00 | |||
| ductal | 74 (91.3%) | 2 (100%) | 4 (100%) | |
| lobular | 3 (3.7%) | 0 | 0 | |
| others | 4 (4.9%) | 0 | 0 | |
| unknown | 21 | 0 | 1 | |
| PR | 0.105 | |||
| ≤20 | 29 (33.7%) | 0 | 2 (40%) | |
| >20 | 57 (66.3%) | 0 | 3 (60%) | |
| unknown | 23 | 2 | 0 | |
| HER2 | 0.052 | |||
| negative | 54 (69.2%) | 0 | 5 (100%) | |
| positive | 24 (30.8%) | 0 | 0 | |
| unknown | 24 | 2 | 0 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toss, A.; Molinaro, E.; Venturelli, M.; Domati, F.; Marcheselli, L.; Piana, S.; Barbieri, E.; Grandi, G.; Piombino, C.; Marchi, I.; et al. BRCA Detection Rate in an Italian Cohort of Luminal Early-Onset and Triple-Negative Breast Cancer Patients without Family History: When Biology Overcomes Genealogy. Cancers 2020, 12, 1252. https://doi.org/10.3390/cancers12051252
Toss A, Molinaro E, Venturelli M, Domati F, Marcheselli L, Piana S, Barbieri E, Grandi G, Piombino C, Marchi I, et al. BRCA Detection Rate in an Italian Cohort of Luminal Early-Onset and Triple-Negative Breast Cancer Patients without Family History: When Biology Overcomes Genealogy. Cancers. 2020; 12(5):1252. https://doi.org/10.3390/cancers12051252
Chicago/Turabian StyleToss, Angela, Eleonora Molinaro, Marta Venturelli, Federica Domati, Luigi Marcheselli, Simonetta Piana, Elena Barbieri, Giovanni Grandi, Claudia Piombino, Isabella Marchi, and et al. 2020. "BRCA Detection Rate in an Italian Cohort of Luminal Early-Onset and Triple-Negative Breast Cancer Patients without Family History: When Biology Overcomes Genealogy" Cancers 12, no. 5: 1252. https://doi.org/10.3390/cancers12051252
APA StyleToss, A., Molinaro, E., Venturelli, M., Domati, F., Marcheselli, L., Piana, S., Barbieri, E., Grandi, G., Piombino, C., Marchi, I., Tenedini, E., Tagliafico, E., Tazzioli, G., & Cortesi, L. (2020). BRCA Detection Rate in an Italian Cohort of Luminal Early-Onset and Triple-Negative Breast Cancer Patients without Family History: When Biology Overcomes Genealogy. Cancers, 12(5), 1252. https://doi.org/10.3390/cancers12051252