Vitamin C Status and Cognitive Function: A Systematic Review

 ,
,
Abstract
:1. Introduction
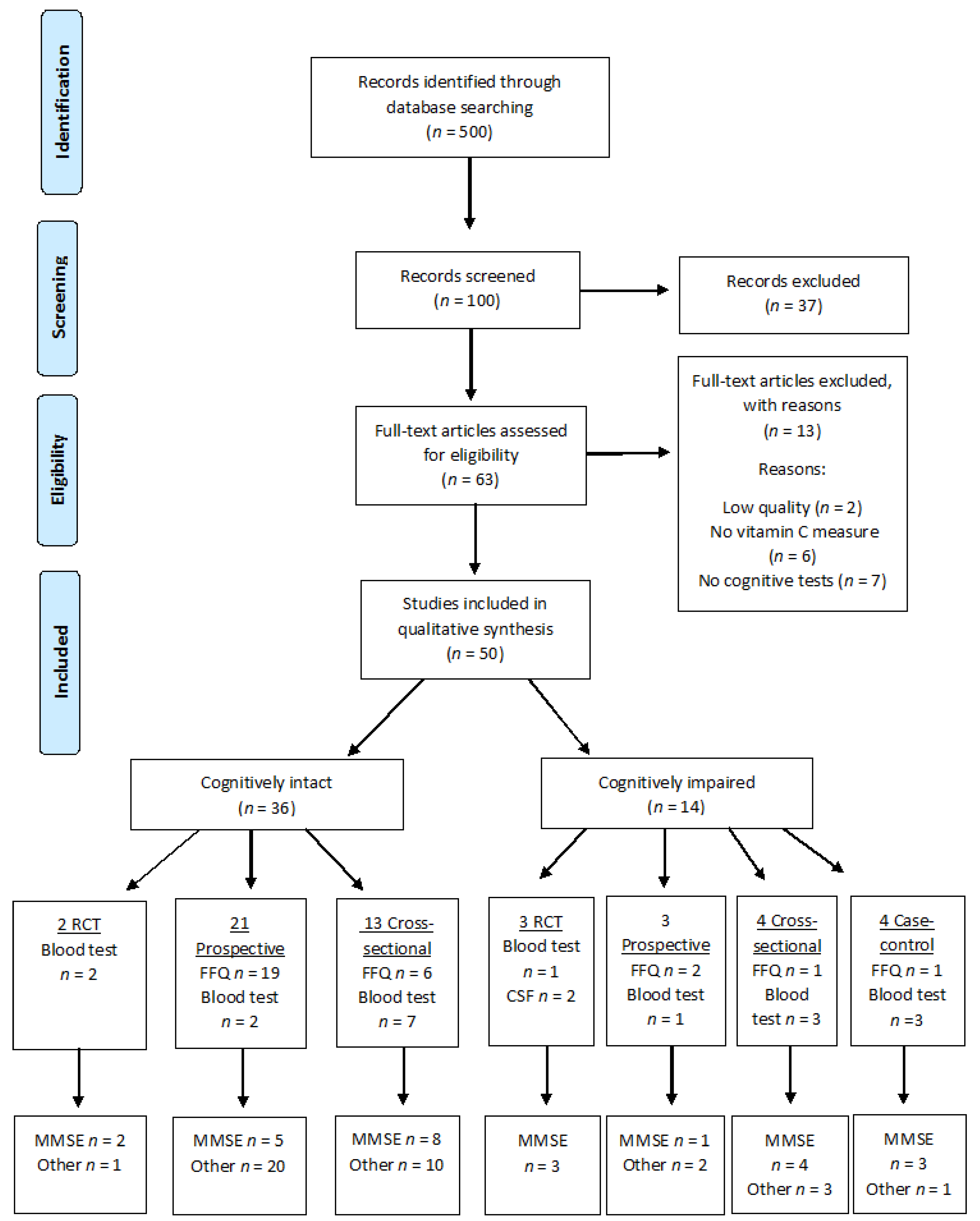
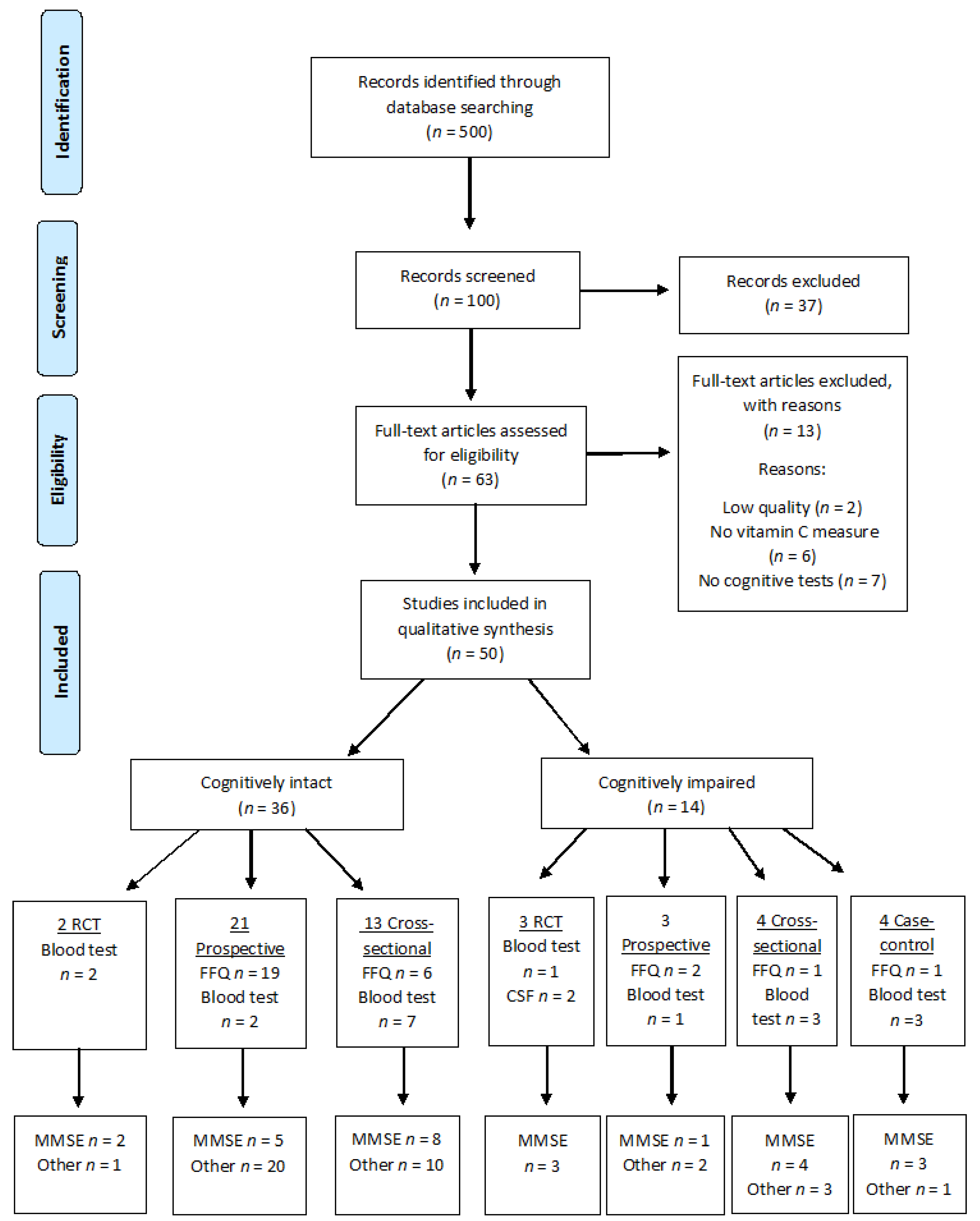
2. Methods
2.1. Search Strategy
2.2. Selection of Trials
2.3. Quality Assessment
2.4. Analysis of Trials Using Comparable Methods
2.5. Blood Plasma Vitamin C
2.6. Measure of Cognition
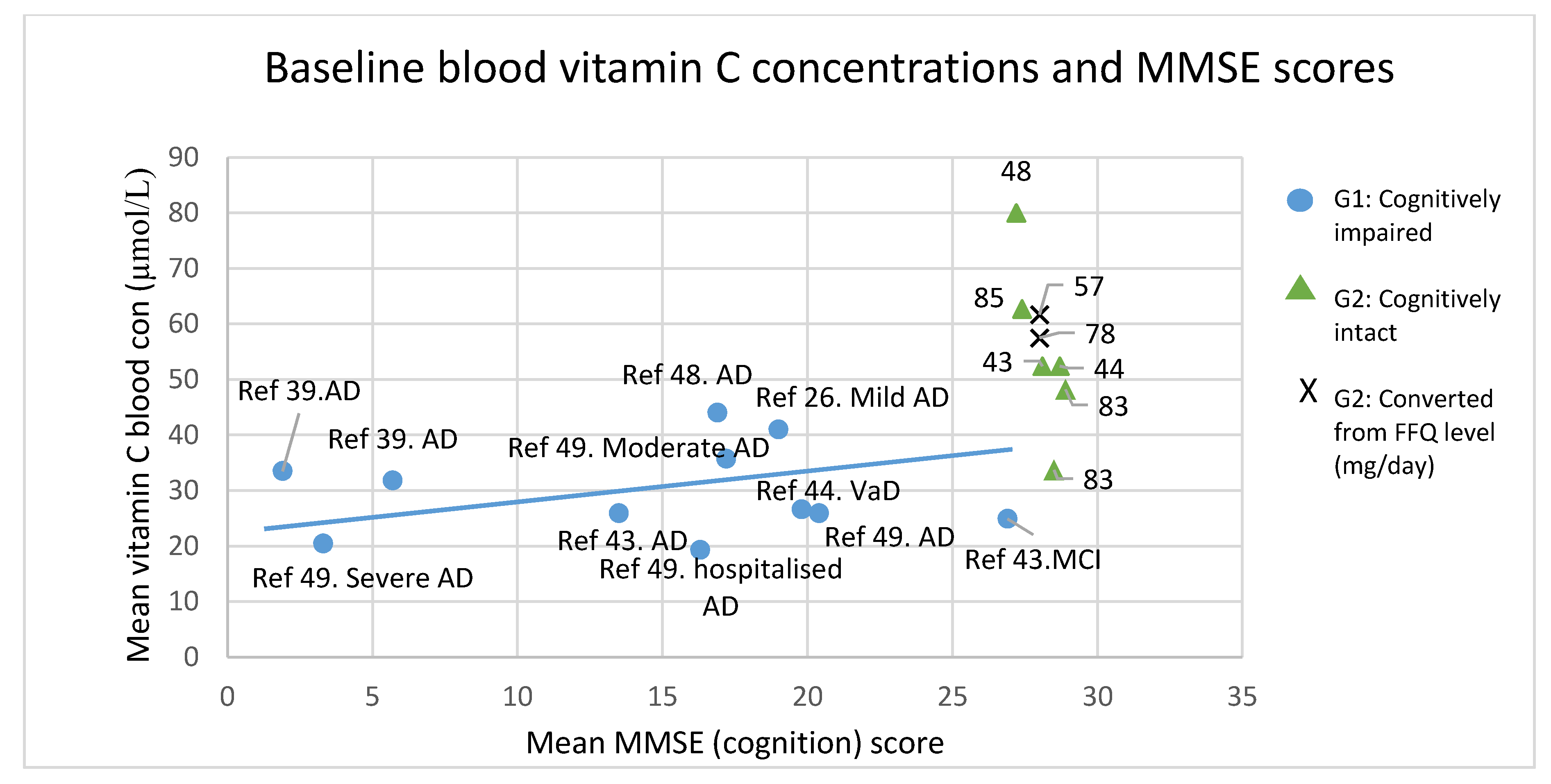
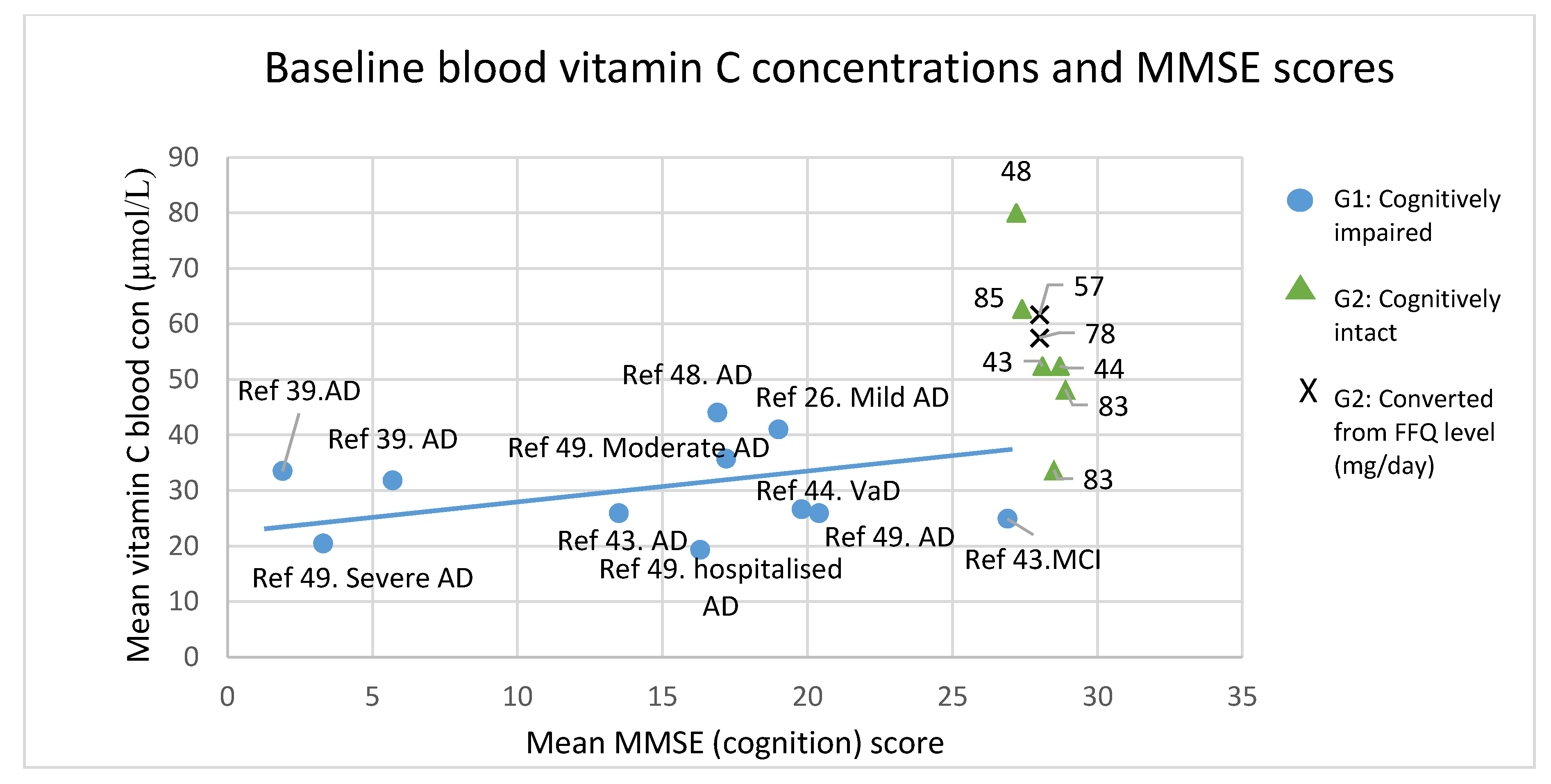
2.7. Z Statistical Analysis-Correlation Between Blood Vitamin C and MMSE Score
3. Results
4. Discussion
4.1. Limitations
4.2. Future Directions
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Trout, D.L. Vitamin c and cardiovascular risk factors. Am. J. Clin. Nutr. 1991, 53, 322S–325S. [Google Scholar] [PubMed]
- Vojdani, A.; Ghoneum, M. In vivo effect of ascorbic acid on enhancement of human natural killer cell activity. Nutr. Res. 1993, 13, 753–764. [Google Scholar] [CrossRef]
- Jacques, P.F.; Chylack, L.T. Epidemiologic evidence of a role for the antioxidant vitamins and carotenoids in cataract prevention. Am. J. Clin. Nutr. 1991, 53, 352S–355S. [Google Scholar] [PubMed]
- Hatch, G.E. Asthma, inhaled oxidants, and dietary antioxidants. Am. J. Clin. Nutr. 1995, 61, 625S–630S. [Google Scholar] [PubMed]
- Hemilä, H. Does vitamin c alleviate the symptoms of the common cold?—A review of current evidence. Scand. J. Infect. Dis. 1994, 26, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Gund, P. Three-dimensional pharmacophoric pattern searching. In Progress in Molecular and Subcellular Biology; Springer: Berlin/Heidelberg, Germany, 1977; pp. 117–143. [Google Scholar]
- Gaby, S.K.; Bendich, A.; Singh, V.; Machlin, L.J. Vitamin Intake and Health: A Scientific Review; CRC Press: Boca Raton, FL, USA, 1991; pp. 71–103. [Google Scholar]
- Levine, M.; Asher, A.; Pollard, H.; Zinder, O. Ascorbic acid and catecholamine secretion from cultured chromaffin cells. J. Biol. Chem. 1983, 258, 13111–13115. [Google Scholar] [PubMed]
- Hansen, S.N.; Tveden-Nyborg, P.; Lykkesfeldt, J. Does vitamin c deficiency affect cognitive development and function? Nutrients 2014, 6, 3818–3846. [Google Scholar] [CrossRef] [PubMed]
- Majewska, M.D.; Bell, J.A. Ascorbic acid protects neurons from injury induced by glutamate and nmda. Neuroreport 1990, 1, 194–196. [Google Scholar] [CrossRef] [PubMed]
- Levine, M.; Morita, K.; Heldman, E.; Pollard, H.B. Ascorbic acid regulation of norepinephrine biosynthesis in isolated chromaffin granules from bovine adrenal medulla. J. Biol. Chem. 1985, 260, 15598–15603. [Google Scholar] [PubMed]
- Levine, M.; Morita, K.; Pollard, H. Enhancement of norepinephrine biosynthesis by ascorbic acid in cultured bovine chromaffin cells. J. Biol. Chem. 1985, 260, 12942–12947. [Google Scholar] [PubMed]
- Sandstrom, M.I.; Rebec, G.V. Extracellular ascorbate modulates glutamate dynamics: Role of behavioral activation. BMC Neurosci. 2007, 8, 1. [Google Scholar] [CrossRef] [PubMed]
- Majewska, M.D.; Bell, J.A.; London, E.D. Regulation of the nmda receptor by redox phenomena: Inhibitory role of ascorbate. Brain Res. 1990, 537, 328–332. [Google Scholar] [CrossRef]
- Liu, X.; Wu, H.; Byrne, M.; Krane, S.; Jaenisch, R. Type iii collagen is crucial for collagen i fibrillogenesis and for normal cardiovascular development. Proc. Natl. Acad. Sci. USA 1997, 94, 1852–1856. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Agus, D.B.; Winfree, C.J.; Kiss, S.; Mack, W.J.; McTaggart, R.A.; Choudhri, T.F.; Kim, L.J.; Mocco, J.; Pinsky, D.J. Dehydroascorbic acid, a blood-brain barrier transportable form of vitamin c, mediates potent cerebroprotection in experimental stroke. Proc. Natl. Acad. Sci. USA 2001, 98, 11720–11724. [Google Scholar] [CrossRef] [PubMed]
- Iyer, N.V.; Kotch, L.E.; Agani, F.; Leung, S.W.; Laughner, E.; Wenger, R.H.; Gassmann, M.; Gearhart, J.D.; Lawler, A.M.; Aimee, Y.Y. Cellular and developmental control of o2 homeostasis by hypoxia-inducible factor 1α. Genes Dev. 1998, 12, 149–162. [Google Scholar] [CrossRef] [PubMed]
- Hediger, M.A. New view at c. Nat. Med. 2002, 8, 445–446. [Google Scholar] [CrossRef] [PubMed]
- Jackson, T.S.; Xu, A.; Vita, J.A.; Keaney, J.F. Ascorbate prevents the interaction of superoxide and nitric oxide only at very high physiological concentrations. Circ. Res. 1998, 83, 916–922. [Google Scholar] [CrossRef] [PubMed]
- Spector, R.; Johanson, C.E. Sustained choroid plexus function in human elderly and alzheimer’s disease patients. Fluids Barriers CNS 2013, 10, 1. [Google Scholar] [CrossRef] [PubMed]
- Harrison, F.; Allard, J.; Bixler, R.; Usoh, C.; Li, L.; May, J.; McDonald, M. Antioxidants and cognitive training interact to affect oxidative stress and memory in app/psen1 mice. Nutr. Neurosci. 2009, 12, 203–218. [Google Scholar] [CrossRef] [PubMed]
- Harrison, F.E.; Green, R.J.; Dawes, S.M.; May, J.M. Vitamin c distribution and retention in the mouse brain. Brain Res. 2010, 1348, 181–186. [Google Scholar] [CrossRef] [PubMed]
- May, J.M. Vitamin c transport and its role in the central nervous system. In Water Soluble Vitamins; Springer: Dordrecht, The Netherlands, 2012; pp. 85–103. [Google Scholar]
- Mefford, I.N.; Oke, A.F.; Adams, R.N. Regional distribution of ascorbate in human brain. Brain Res. 1981, 212, 223–226. [Google Scholar] [CrossRef]
- Oke, A.F.; May, L.; Adams, R.N. Ascorbic acid distribution patterns in human brain. Ann. N. Y. Acad. Sci. 1987, 498, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Bowman, G.L.; Dodge, H.; Frei, B.; Calabrese, C.; Oken, B.S.; Kaye, J.A.; Quinn, J.F. Ascorbic acid and rates of cognitive decline in alzheimer’s disease. J. Alzheimers Dis. 2009, 16, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Quinn, J.; Suh, J.; Moore, M.M.; Kaye, J.; Frei, B. Antioxidants in alzheimer’s disease-vitamin c delivery to a demanding brain. J. Alzheimers Dis. 2003, 5, 309–313. [Google Scholar] [CrossRef] [PubMed]
- May, J.M.; Li, L.; Hayslett, K.; Qu, Z.-C. Ascorbate transport and recycling by sh-sy5y neuroblastoma cells: Response to glutamate toxicity. Neurochem. Res. 2006, 31, 785–794. [Google Scholar] [CrossRef] [PubMed]
- Spector, R. Vitamin homeostasis in the central nervous system. N. Engl. J. Med. 1977, 296, 1393–1398. [Google Scholar] [PubMed]
- Hornig, D. Distribution of ascorbic acid, metabolites and analogues in man and animals. Ann. N. Y. Acad. Sci. 1975, 258, 103–118. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2011; Volume 4. [Google Scholar]
- Dehghan, M.; Akhtar-Danesh, N.; McMillan, C.R.; Thabane, L. Is plasma vitamin c an appropriate biomarker of vitamin c intake? A systematic review and meta-analysis. Nutr. J. 2007, 6, 41. [Google Scholar] [CrossRef] [PubMed]
- Hampl, J.S.; Taylor, C.A.; Johnston, C.S. Vitamin c deficiency and depletion in the united states: The third national health and nutrition examination survey, 1988 to 1994. Am. J. Public Health 2004, 94, 870–875. [Google Scholar] [CrossRef] [PubMed]
- Levine, M.; Conry-Cantilena, C.; Wang, Y.; Welch, R.W.; Washko, P.W.; Dhariwal, K.R.; Park, J.B.; Lazarev, A.; Graumlich, J.F.; King, J. Vitamin c pharmacokinetics in healthy volunteers: Evidence for a recommended dietary allowance. Proc. Natl. Acad. Sci. USA 1996, 93, 3704–3709. [Google Scholar] [CrossRef] [PubMed]
- Tombaugh, T.N.; McIntyre, N.J. The mini-mental state examination: A comprehensive review. J. Am. Geriatr. Soc. 1992, 40, 922–935. [Google Scholar] [CrossRef] [PubMed]
- Mungas, D. Iii-office mental status testing: A practical guide. Geriatrics 1991, 46, 54–67. [Google Scholar] [PubMed]
- Arlt, S.; Müller-Thomsen, T.; Beisiegel, U.; Kontush, A. Effect of one-year vitamin c-and e-supplementation on cerebrospinal fluid oxidation parameters and clinical course in alzheimer’s disease. Neurochem. Res. 2012, 37, 2706–2714. [Google Scholar] [CrossRef] [PubMed]
- Galasko, D.R.; Peskind, E.; Clark, C.M.; Quinn, J.F.; Ringman, J.M.; Jicha, G.A.; Cotman, C.; Cottrell, B.; Montine, T.J.; Thomas, R.G. Antioxidants for alzheimer disease: A randomized clinical trial with cerebrospinal fluid biomarker measures. Arch. Neurol. 2012, 69, 836–841. [Google Scholar] [CrossRef] [PubMed]
- Burns, A.; Marsh, A.; Bender, D.A. A trial of vitamin supplementation in senile dementia. Int. J. Geriatr. Psychiatry 1989, 4, 333–338. [Google Scholar] [CrossRef]
- Zandi, P.P.; Anthony, J.C.; Khachaturian, A.S.; Stone, S.V.; Gustafson, D.; Tschanz, J.T.; Norton, M.C.; Welsh-Bohmer, K.A.; Breitner, J.C. Reduced risk of alzheimer disease in users of antioxidant vitamin supplements: The cache county study. Arch. Neurol. 2004, 61, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Deijen, J.; Slump, E.; Wouters-Wesseling, W.; De Groot, C.; Galle, E.; Pas, H. Nutritional intake and daily functioning of psychogeriatric nursing home residents. J. Nutr. Health Aging 2002, 7, 242–246. [Google Scholar]
- Rinaldi, P.; Polidori, M.C.; Metastasio, A.; Mariani, E.; Mattioli, P.; Cherubini, A.; Catani, M.; Cecchetti, R.; Senin, U.; Mecocci, P. Plasma antioxidants are similarly depleted in mild cognitive impairment and in alzheimer’s disease. Neurobiol. Aging 2003, 24, 915–919. [Google Scholar] [CrossRef]
- Polidori, M.C.; Mattioli, P.; Aldred, S.; Cecchetti, R.; Stahl, W.; Griffiths, H.; Senin, U.; Sies, H.; Mecocci, P. Plasma antioxidant status, immunoglobulin g oxidation and lipid peroxidation in demented patients: Relevance to alzheimer disease and vascular dementia. Dement. Geriatr. Cogn. Disord. 2004, 18, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Richardson, T.; Ball, L.; Rosenfeld, T. Will an orange a day keep the doctor away? Postgrad. Med. J. 2002, 78, 292–294. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; An, Y.; Guo, J.; Zhang, X.; Wang, H.; Rong, H.; Xiao, R. Dietary intake of nutrients and lifestyle affect the risk of mild cognitive impairment in the chinese elderly population: A cross-sectional study. Front. Behav. Neurosci. 2016, 10, 229. [Google Scholar] [CrossRef] [PubMed]
- Charlton, K.E.; Rabinowitz, T.L.; Geffen, L.; Dhansay, M. Lowered plasma vitamin c, but not vitamin e, concentrations in dementia patients. J. Nutr. Health Aging 2004, 8, 99–108. [Google Scholar] [PubMed]
- Glasø, M.; Nordbø, G.; Diep, L.; Bøhmer, T. Reduced concentrations of several vitamins in normal weight patients with late-onset dementia of the alzheimer type without vascular disease. J. Nutr. Health Aging 2003, 8, 407–413. [Google Scholar]
- Rivière, S.; Birlouez-Aragon, I.; Nourhashémi, F.; Vellas, B. Low plasma vitamin c in alzheimer patients despite an adequate diet. Int. J. Geriatr. Psychiatry 1998, 13, 749–754. [Google Scholar] [CrossRef]
- Masaki, K.; Losonczy, K.; Izmirlian, G.; Foley, D.; Ross, G.; Petrovitch, H.; Havlik, R.; White, L. Association of vitamin e and c supplement use with cognitive function and dementia in elderly men. Neurology 2000, 54, 1265–1272. [Google Scholar] [CrossRef] [PubMed]
- Chandra, R.K. Retracted: Effect of vitamin and trace-element supplementation on cognitive function in elderly subjects. Nutrition 2001, 17, 709–712. [Google Scholar] [CrossRef]
- Dror, Y.; Stern, F.; Nemesh, L.; Hart, J.; Grinblat, J. Estimation of vitamin needs—Riboflavin, vitamin b6 and ascorbic acid-according to blood parameters and functional-cognitive and emotional indices in a selected well-established group of elderly in a home for the aged in israel. J. Am. Coll. Nutr. 1996, 15, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Gale, C.R.; Martyn, C.N.; Cooper, C. Cognitive impairment and mortality in a cohort of elderly people. BMJ 1996, 312, 608–611. [Google Scholar] [CrossRef] [PubMed]
- La Rue, A.; Koehler, K.M.; Wayne, S.J.; Chiulli, S.J.; Haaland, K.Y.; Garry, P.J. Nutritional status and cognitive functioning in a normally aging sample: A 6-y reassessment. Am. J. Clin. Nutr. 1997, 65, 20–29. [Google Scholar] [PubMed]
- Paleologos, M.; Cumming, R.G.; Lazarus, R. Cohort study of vitamin c intake and cognitive impairment. Am. J. Epidemiol. 1998, 148, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Devore, E.E.; Kang, J.H.; Stampfer, M.J.; Grodstein, F. The association of antioxidants and cognition in the nurses’ health study. Am. J. Epidemiol. 2013, 177, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Engelhart, M.J.; Geerlings, M.I.; Ruitenberg, A.; van Swieten, J.C.; Hofman, A.; Witteman, J.C.; Breteler, M.M. Dietary intake of antioxidants and risk of alzheimer disease. JAMA 2002, 287, 3223–3229. [Google Scholar] [CrossRef] [PubMed]
- Kalmijn, S.; Feskens, E.; Launer, L.J.; Kromhout, D. Polyunsaturated fatty acids, antioxidants, and cognitive function in very old men. Am. J. Epidemiol. 1997, 145, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Laurin, D.; Masaki, K.H.; Foley, D.J.; White, L.R.; Launer, L.J. Midlife dietary intake of antioxidants and risk of late-life incident dementia the honolulu-asia aging study. Am. J. Epidemiol. 2004, 159, 959–967. [Google Scholar] [CrossRef] [PubMed]
- Basambombo, L.L.; Carmichael, P.-H.; Côté, S.; Laurin, D. Use of vitamin e and c supplements for the prevention of cognitive decline. Ann. Pharmacother. 2016, 51, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Nooyens, A.C.; Milder, I.E.; Van Gelder, B.M.; Bueno-de-Mesquita, H.B.; Van Boxtel, M.P.; Verschuren, W.M. Diet and cognitive decline at middle age: The role of antioxidants. Br. J. Nutr. 2015, 113, 1410–1417. [Google Scholar] [CrossRef] [PubMed]
- Péneau, S.; Galan, P.; Jeandel, C.; Ferry, M.; Andreeva, V.; Hercberg, S.; Kesse-Guyot, E.; Group, S.V.M.R. Fruit and vegetable intake and cognitive function in the su. Vi. Max 2 prospective study. Am. J. Clin. Nutr. 2011, 94, 1295–1303. [Google Scholar] [CrossRef] [PubMed]
- Fotuhi, M.; Zandi, P.P.; Hayden, K.M.; Khachaturian, A.S.; Szekely, C.A.; Wengreen, H.; Munger, R.G.; Norton, M.C.; Tschanz, J.T.; Lyketsos, C.G. Better cognitive performance in elderly taking antioxidant vitamins e and c supplements in combination with nonsteroidal anti-inflammatory drugs: The cache county study. Alzheimers Dement. 2008, 4, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Gray, S.L.; Anderson, M.L.; Crane, P.K.; Breitner, J.; McCormick, W.; Bowen, J.D.; Teri, L.; Larson, E. Antioxidant vitamin supplement use and risk of dementia or alzheimer’s disease in older adults. J. Am. Geriatr. Soc. 2008, 56, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Wengreen, H.; Munger, R.; Corcoran, C.; Zandi, P. Antioxidant intake and cognitive function of elderly men and women: The cache county study. J. Nutr. Health Aging 2007, 11, 230. [Google Scholar] [PubMed]
- Fillenbaum, G.G.; Kuchibhatla, M.N.; Hanlon, J.T.; Artz, M.B.; Pieper, C.F.; Schmader, K.E.; Dysken, M.W.; Gray, S.L. Dementia and alzheimer’s disease in community-dwelling elders taking vitamin c and/or vitamin e. Ann. Pharmacother. 2005, 39, 2009–2014. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, C.J.; Hicks, M.S.; Hogan, D.B.; Basran, J.; Ebly, E.M. Supplemental use of antioxidant vitamins and subsequent risk of cognitive decline and dementia. Dement. Geriatr. Cogn. Disord. 2005, 20, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Grodstein, F.; Chen, J.; Willett, W.C. High-dose antioxidant supplements and cognitive function in community-dwelling elderly women. Am. J. Clin. Nutr. 2003, 77, 975–984. [Google Scholar] [PubMed]
- Luchsinger, J.A.; Tang, M.-X.; Shea, S.; Mayeux, R. Antioxidant vitamin intake and risk of alzheimer disease. Arch. Neurol. 2003, 60, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.C.; Evans, D.A.; Bienias, J.L.; Tangney, C.C.; Bennett, D.A.; Aggarwal, N.; Wilson, R.S.; Scherr, P.A. Dietary intake of antioxidant nutrients and the risk of incident alzheimer disease in a biracial community study. JAMA 2002, 287, 3230–3237. [Google Scholar] [CrossRef] [PubMed]
- Peacock, J.M.; Folsom, A.R.; Knopman, D.S.; Mosley, T.H.; Goff, D.C.; Szklo, M. Dietary antioxidant intake and cognitive performance in middle-aged adults. Public Health Nutr. 2000, 3, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.C.; Beckett, L.A.; Scherr, P.A.; Hebert, L.E.; Bennett, D.A.; Field, T.S.; Evans, D.A. Vitamin e and vitamin c supplement use and risk of incident alzheimer disease. Alzheimer Dis. Assoc. Disord. 1998, 12, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Mendelsohn, A.B.; Belle, S.H.; Stoehr, G.P.; Ganguli, M. Use of antioxidant supplements and its association with cognitive function in a rural elderly cohort the movies project. Am. J. Epidemiol. 1998, 148, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Berti, V.; Murray, J.; Davies, M.; Spector, N.; Tsui, W.; Li, Y.; Williams, S.; Pirraglia, E.; Vallabhajosula, S.; McHugh, P. Nutrient patterns and brain biomarkers of alzheimer’s disease in cognitively normal individuals. J. Nutr. Health Aging 2015, 19, 413–423. [Google Scholar] [CrossRef] [PubMed]
- Beydoun, M.A.; Kuczmarski, M.F.; Kitner-Triolo, M.H.; Beydoun, H.A.; Kaufman, J.S.; Mason, M.A.; Evans, M.K.; Zonderman, A.B. Dietary antioxidant intake and its association with cognitive function in an ethnically diverse sample of us adults. Psychosom. Med. 2015, 77, 68. [Google Scholar] [CrossRef] [PubMed]
- Chaudhari, K.; Sumien, N.; Johnson, L.; D’Agostino, D.; Edwards, M.; Paxton, R.; Hall, J.; O’Bryant, S.E. Vitamin c supplementation, apoe4 genotype and cognitive functioning in a rural-dwelling cohort. J. Nutr. Health Aging 2016, 20, 841–844. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, J.S.; Goodwin, J.M.; Garry, P.J. Association between nutritional status and cognitive functioning in a healthy elderly population. JAMA 1983, 249, 2917–2921. [Google Scholar] [CrossRef] [PubMed]
- Jama, J.W.; Launer, L.J.; Witteman, J.; Den Breeijen, J.; Breteler, M.; Grobbee, D.; Hofman, A. Dietary antioxidants and cognitive function in a population-based sample of older persons the rotterdam study. Am. J. Epidemiol. 1996, 144, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Lindeman, R.D.; Romero, L.J.; Koehler, K.M.; Liang, H.C.; LaRue, A.; Baumgartner, R.N.; Garry, P.J. Serum vitamin b12, c and folate concentrations in the new mexico elder health survey: Correlations with cognitive and affective functions. J. Am. Coll. Nutr. 2000, 19, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Perrig, W.J.; Perrig, P.; Stähelin, H. The relation between antioxidants and memory performance in the old and very old. J. Am. Geriatr. Soc. 1997, 45, 718–724. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, R.; Hayn, M.; Reinhart, B.; Roob, G.; Schmidt, H.; Schumacher, M.; Watzinger, N.; Launer, L. Plasma antioxidants and cognitive performance in middle-aged and older adults: Results of the austrian stroke prevention study. J. Am. Geriatr. Soc. 1998, 46, 1407–1410. [Google Scholar] [CrossRef] [PubMed]
- Sato, R.; Helzlsouer, K.; Comstock, G.; Hoffman, S. A cross-sectional study of vitamin c and cognitive function in older adults: The differential effects of gender. J. Nutr. Health Aging 2006, 10, 37. [Google Scholar] [PubMed]
- Whalley, L.; Fox, H.; Lemmon, H.; Duthie, S.; Collins, A.; Peace, H.; Starr, J.; Deary, I. Dietary supplement use in old age: Associations with childhood iq, current cognition and health. Int. J. Geriatr. Psychiatry 2003, 18, 769–776. [Google Scholar] [CrossRef] [PubMed]
- Perkins, A.J.; Hendrie, H.C.; Callahan, C.M.; Gao, S.; Unverzagt, F.W.; Xu, Y.; Hall, K.S.; Hui, S.L. Association of antioxidants with memory in a multiethnic elderly sample using the third national health and nutrition examination survey. Am. J. Epidemiol. 1999, 150, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Ortega, R.M.; Requejo, A.M.; Andrés, P.; López-Sobaler, A.M.; Quintas, M.E.; Redondo, M.R.; Navia, B.; Rivas, T. Dietary intake and cognitive function in a group of elderly people. Am. J. Clin. Nutr. 1997, 66, 803–809. [Google Scholar] [PubMed]
- Requejo, A.; Ortega, R.; Robles, F.; Navia, B.; Faci, M.; Aparicio, A. Influence of nutrition on cognitive function in a group of elderly, independently living people. Eur. J. Clin. Nutr. 2003, 57, S54–S57. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, D.O.; Veasey, R.C.; Watson, A.W.; Dodd, F.L.; Jones, E.K.; Tiplady, B.; Haskell, C.F. Vitamins and psychological functioning: A mobile phone assessment of the effects of a b vitamin complex, vitamin c and minerals on cognitive performance and subjective mood and energy. Hum. Psychopharmacol. 2011, 26, 338–347. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.P.; Clark, R.; Nutt, D.; Haller, J.; Hayward, S.; Perry, K. Vitamin c, mood and cognitive functioning in the elderly. Nutr. Neurosci. 1999, 2, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.V.; Rajagopalan, S. Trial using multiple micronutrient food supplement and its effect on cognition. Indian J. Pediatr. 2008, 75, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Yaffe, K.; Clemons, T.; McBee, W.; Lindblad, A. Impact of antioxidants, zinc, and copper on cognition in the elderly: A randomized, controlled trial. Neurology 2004, 63, 1705–1707. [Google Scholar] [PubMed]
- Kang, J.H.; Cook, N.R.; Manson, J.E.; Buring, J.E.; Albert, C.M.; Grodstein, F. Vitamin e, vitamin c, beta carotene, and cognitive function among women with or at risk of cardiovascular disease. Circulation 2009, 119, 2772–2780. [Google Scholar] [CrossRef] [PubMed]
- Chui, M.H.; Greenwood, C.E. Antioxidant vitamins reduce acute meal-induced memory deficits in adults with type 2 diabetes. Nutr. Res. 2008, 28, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Day, J.; Bayer, A.; McMahon, M.; Pathy, M.; Spragg, B.; Rowlands, D. Thiamine status, vitamin supplements and postoperative confusion. Age Ageing 1988, 17, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Paraskevas, G.; Kapaki, E.; Libitaki, G.; Zournas, C.; Segditsa, I.; Papageorgiou, C. Ascorbate in healthy subjects, amyotrophic lateral sclerosis and alzheimer’s disease. Acta Neurol. Scand. 1997, 96, 88–90. [Google Scholar] [CrossRef] [PubMed]
- Woo, J.; Ho, S.; Mak, Y.; MacDonald, D.; Swaminathan, R. Vitamin nutritional status in elderly chinese subjects living in chronic care institutions. Nutr. Res. 1989, 9, 1071–1080. [Google Scholar] [CrossRef]
- Polidori, M.C.; Mecocci, P. Plasma susceptibility to free radical-induced antioxidant consumption and lipid peroxidation is increased in very old subjects with alzheimer disease. J. Alzheimers Dis. 2002, 4, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Foy, C.; Passmore, A.; Vahidassr, M.; Young, I.; Lawson, J. Plasma chain-breaking antioxidants in alzheimer’s disease, vascular dementia and parkinson’s disease. QJM 1999, 92, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Talley V, H.C.; Wicks, M.N.; Carter, M.; Roper, B. Ascorbic acid does not influence consciousness recovery after anesthesia. Biol. Res. Nurs. 2009, 10, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Luchsinger, J.A.; Mayeux, R. Dietary factors and alzheimer’s disease. Lancet Neurol. 2004, 3, 579–587. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Mowe, M.; Bøhmer, T.; Kindt, E. Reduced nutritional status in an elderly population (>70 years) is probable before disease and possibly contributes to the development of disease. Am. J. Clin. Nutr. 1994, 59, 317–324. [Google Scholar] [PubMed]
- Monget, A.; Galan, P.; Preziosi, P.; Keller, H.; Bourgeois, C.; Arnaud, J.; Favier, A.; Hercberg, S. Micronutrient status in elderly people. Geriatrie/min. Vit. Aux network. Int. J. Vitam. Nutr. Res. 1996, 66, 71–76. [Google Scholar] [PubMed]
- Frei, B.; Stocker, R.; Ames, B.N. Antioxidant defenses and lipid peroxidation in human blood plasma. Proc. Natl. Acad. Sci. USA 1988, 85, 9748–9752. [Google Scholar] [CrossRef] [PubMed]
- Richardson, J.S. Free radicals in the genesis of alzheimer’s disease. Ann. N. Y. Acad. Sci. 1993, 695, 73–76. [Google Scholar] [CrossRef] [PubMed]
- Markesbery, W.R.; Carney, J.M. Oxidative alterations in alzheimer’s disease. Brain Pathol. 1999, 9, 133–146. [Google Scholar] [CrossRef] [PubMed]
- Beal, M.F. Aging, energy, and oxidative stress in neurodegenerative diseases. Ann. Neurol. 1995, 38, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Gouras, G.K.; Tsai, J.; Naslund, J.; Vincent, B.; Edgar, M.; Checler, F.; Greenfield, J.P.; Haroutunian, V.; Buxbaum, J.D.; Xu, H. Intraneuronal aβ42 accumulation in human brain. Am. J. Pathol. 2000, 156, 15–20. [Google Scholar] [CrossRef]
- Sayre, L.; Perry, G.; Atwood, C.; Smith, M. The role of metals in neurodegenerative diseases. Cell. Mol. Biol. 2000, 46, 731–741. [Google Scholar] [PubMed]
- Connor, J.; Menzies, S.; St Martin, S.; Mufson, E. A histochemical study of iron, transferrin, and ferritin in alzheimer’s diseased brains. J. Neurosci. Res. 1992, 31, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Thomas, T.; Thomas, G.; McLendon, C.; Sutton, T.; Mullan, M. Beta-amyloid-mediated vasoactivity and vascular endothelial damage. Nature 1996, 380, 168. [Google Scholar] [CrossRef] [PubMed]
- Michels, A.J.; Frei, B. Myths, artifacts, and fatal flaws: Identifying limitations and opportunities in vitamin c research. Nutrients 2013, 5, 5161–5192. [Google Scholar] [CrossRef] [PubMed]
- Harrison, F.E. A critical review of vitamin c for the prevention of age-related cognitive decline and alzheimer’s disease. J. Alzheimers Dis. 2012, 29, 711–726. [Google Scholar] [PubMed]
- Benzie, I.; Strain, J. Simultaneous automated measurement of total’antioxidant’(reducing) capacity and ascorbic acid concentration. Redox Rep. 1997, 3, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Cahill, L.E.; El-Sohemy, A. Vitamin c transporter gene polymorphisms, dietary vitamin c and serum ascorbic acid. J. Nutrigenet. Nutrigenomics 2010, 2, 292–301. [Google Scholar] [CrossRef] [PubMed]
- Bowman, G.L.; Shannon, J.; Ho, E.; Traber, M.G.; Frei, B.; Oken, B.S.; Kaye, J.A.; Quinn, J.F. Reliability and validity of food frequency questionnaire and nutrient biomarkers in elders with and without mild cognitive impairment. Alzheimer Dis. Assoc. Disord. 2011, 25, 49. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, M.; Babyn, P.; Zlotkin, S. An orange a day keeps the doctor away: Scurvy in the year 2000. Pediatrics 2001, 108, e55. [Google Scholar] [CrossRef] [PubMed]
- Vizuete, A.A.; Robles, F.; Rodríguez-Rodríguez, E.; López-Sobaler, A.M.; Ortega, R.M. Association between food and nutrient intakes and cognitive capacity in a group of institutionalized elderly people. Eur. J. Nutr. 2010, 49, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Clarke, R.; Smith, A.D.; Jobst, K.A.; Refsum, H.; Sutton, L.; Ueland, P.M. Folate, vitamin b12, and serum total homocysteine levels in confirmed alzheimer disease. Arch. Neurol. 1998, 55, 1449–1455. [Google Scholar] [CrossRef] [PubMed]
- Grundman, M. Vitamin e and alzheimer disease: The basis for additional clinical trials. Am. J. Clin. Nutr. 2000, 71, 630S–636S. [Google Scholar] [PubMed]
- Evatt, M.L.; DeLong, M.R.; Khazai, N.; Rosen, A.; Triche, S.; Tangpricha, V. Prevalence of vitamin d insufficiency in patients with parkinson disease and alzheimer disease. Arch. Neurol. 2008, 65, 1348–1352. [Google Scholar] [CrossRef] [PubMed]
- Presse, N.; Shatenstein, B.; Kergoat, M.-J.; Ferland, G. Low vitamin k intakes in community-dwelling elders at an early stage of alzheimer’s disease. J. Am. Diet. Assoc. 2008, 108, 2095–2099. [Google Scholar] [CrossRef] [PubMed]
- Rodrigue, K.; Kennedy, K.; Devous, M.; Rieck, J.; Hebrank, A.; Diaz-Arrastia, R.; Mathews, D.; Park, D. B-amyloid burden in healthy aging regional distribution and cognitive consequences. Neurology 2012, 78, 387–395. [Google Scholar] [CrossRef] [PubMed]
- WIND, A.W.; Schellevis, F.G.; Van Staveren, G.; Scholten, R.J.; Jonker, C.; Van Eijk, J.T.M. Limitations of the mini-mental state examination in diagnosing dementia in general practice. Int. J. Geriatr. Psychiatry 1997, 12, 101–108. [Google Scholar] [CrossRef]
- Crum, R.M.; Anthony, J.C.; Bassett, S.S.; Folstein, M.F. Population-based norms for the mini-mental state examination by age and educational level. JAMA 1993, 269, 2386–2391. [Google Scholar] [CrossRef] [PubMed]
- Polidori, M.C.; Praticó, D.; Mangialasche, F.; Mariani, E.; Aust, O.; Anlasik, T.; Mang, N.; Pientka, L.; Stahl, W.; Sies, H. High fruit and vegetable intake is positively correlated with antioxidant status and cognitive performance in healthy subjects. J. Alzheimers Dis. 2009, 17, 921–927. [Google Scholar] [CrossRef] [PubMed]
- Sahakian, B.J.; Morris, R.G.; Evenden, J.L.; Heald, A.; Levy, R.; Philpot, M.; Robbins, T.W. A comparative study of visuospatial memory and learning in alzheimer-type dementia and parkinson’s disease. Brain 1988, 111, 695–718. [Google Scholar] [CrossRef] [PubMed]
- Weintraub, S.; Dikmen, S.S.; Heaton, R.K.; Tulsky, D.S.; Zelazo, P.D.; Bauer, P.J.; Carlozzi, N.E.; Slotkin, J.; Blitz, D.; Wallner-Allen, K. Cognition assessment using the nih toolbox. Neurology 2013, 80, S54–S64. [Google Scholar] [CrossRef] [PubMed]
- Pipingas, A.; Harris, E.; Tournier, E.; King, R.; Kras, M.; Stough, C.K. Assessing the efficacy of nutraceutical interventions on cognitive functioning in the elderly. Curr. Top. Nutraceutical Res. 2010, 8, 79. [Google Scholar]

{kind=link}
{kind=link}
| Paper | Study Design | N | Age (years) | Condition | Quality Rating | Cognitive Measure | Vitamin C Measure | Outcome |
|---|---|---|---|---|---|---|---|---|
| Arlt, 2012 [37] | RCT | 23 | 60–80 | AD | 6 | MMSE, Word fluency, Immediate/delayed verbal recall, Trail-making task | CSF | 1000 mg/day of vit C and E (400 mg/day) increased CSF concentrations after 1 year, but decreased MMSE score and no effect on other measures |
| Galasko, 2012 [47] | RCT | 78 | 50–85 | AD | 4.5 | MMSE | CSF | Decline in MMSE score occurred in E/C/ALA group. (500 mg/day vit C, vit E, alpha lipoic acid) did not influence CSF biomarkers related to amyloid |
| Burns, 1989 [39] | RCT | 81 | ≥65 | Senile Dementia, Community dementia | 4.5 | MMSE | Blood tests | 200 mg Vit C, vits B1, B2, B3 No correlation between vit C intake and cognitive impairment |
| Bowman, 2009 [26] | Pros | 32 | 71 | AD | 5 | MMSE | CSF, plasma ascorbate | Neither Plasma nor CSF AA predictive of AD across 1 year |
| Zandi, 2004 [40] | Pros | 4740 (4540 healthy) | ≥65 | AD | 3.5 | 3MS, Dementia Questionnaire (DQ) | Supplement, Interview | vit E (>400 IU) and C (500 mg) supplements reduced the AD prevalence and incidence. Supplements alone had no protective affect across 2 years |
| Deijen, 2003 [41] | Pros | 90 | >65 | Psychiatry nursing home | 4.5 | Dutch geriatric nursing scale, Zorg Index geriatrie (ZIG) | Food record | Higher vitamin intakes were associated with a worse daily functioning across 6 months |
| Rinaldi, 2003 [42] | Cross | 141 | >70 | MCI, AD | 3 | Clinical dementia rating scale, MMSE, clock drawing test, Babcock story recall, auditory verbal learning test, Corsi block tapping test, Token test, category naming test, Oral word association test, visual search test, digit forward and backward test, Raven’s progressive colored matrices | Plasma ascorbate | Lower vit C concentrations in patients with AD and MCI. MCI sig lower then controls |
| Polidori, 2004 [43] | Cross | 141 | ≥65 | AD, VaD | 2 | MMSE | Plasma ascorbate | Plasma AA lower in AD and VD |
| Richardson, 2002 [44] | Cross | 37 | 65–97 | In-patient ward | 2 | MMSE | Plasma ascorbate | 75% with dementia had low concentrations of vitamin C |
| Lu, 2016 [45] | Cross | 2892 (768 MCI) | 58 | MCI | 2.5 | Montreal cognitive assessment | FFQ | Carotenoids, vit C, and vitamin B6 exhibited the highest protective factor loadings |
| Charlton, 2004 [46] | CC | 93 | ≥65 | Dementia | 4 | MMSE | Plasma Ascorbate/FFQ | Plasma AA lower in dementia, not explained by diet |
| Glaso, 2004 [47] | CC | 38 | 75–85 | AD | 4 | MMSE | Serum ascorbate/CSF | Both plasma vitamin C and CSF lower in AD. CSF: plasma AA ratio higher in AD |
| Riviere,1999 [48] | CC | 69 | >75 | Severe AD, Moderate AD, Hospitalised AD | 3.5 | MMSE | Plasma ascorbate, FFQ | Nutritional intake lower in Severe AD, plasma vit C lower in more severe AD, not explained by vit C intake |
| Masaki, 2000 [49] | CC | 3735 men | 71–93 | Dementia | 3 | Hasegawa scale, MMSE | Self-report supplementation | After controlling for factors such as age, education, stroke, there was an association with cognitive performance |
| Paper | Study Design | N | Age (years) | Quality Assessment | Cognitive Measure | Vitamin C Measure | Outcome |
|---|---|---|---|---|---|---|---|
| Chandra, 2001 [50] | RCT | 86 | ≥65 | 5.5 | Wechsler memory test, Halstead-Reitan categories test, Buschke consistent long-term retrieval, digit span forward, salthouse listening span test, long-term memory recall, MMSE | Plasma spectrophotometry | 80 mg of vitamin C in a multivitamin improved cognitive performance, not Long-term memory across 1 year |
| Dror, 1996 [51] | RCT | 21 | >80 | 3.5 | MMSE | Plasma Assay | No changes in MMSE scores following 42-day supplementation with 45mg/day of vitamin C with other vitamins (Vit D, E B12, B6) |
| Gale, 1996 [52] | Pros | 921 | ≥65 | 2.5 | Hodkinson mental test (Dementia assessment) | Dietary intake/Ascorbate plasma | Cognitive function was poorest in those with the lowest vitamin C over 1 year |
| La Rue, 1997 [53] | Pros | 137 | 66–90 | 5 | Abstract performance, visuospatial performance, memory assessment | Plasma Ascorbate, Nutritional status | Visuospatial performance was higher with higher ascorbate concentrations after 6 years |
| Paleologos, 1998 [54] | Pros | 117 | 69–91 | 4 | MMSE, Reid brief neuropsychological Screen, the animals test of category fluency, the F, A, S test of verbal fluency | Semi-quantitative food frequency | After adjusting for age, sex, smoking, education, energy, vit C supplement linked to less severe cognitive decline, not verbal/category fluency across 4 years |
| Devore, 2002 [55] | Pros | 16,010 | >70 Women | 5 | MMSE, Telephone interview for cognitive status (TICS). East Boston memory test (immediate/delayed) category fluency, Delayed TICS, Digit span backwards | Semi-quantitative food frequency | Dietary vitamin C intake not associated with cognitive decline. Supplemental vit C associated with worse decline over 6 years |
| Engelhart, 2002 [56] | Pros | 5395 | >55 | 3.5 | DSM-III-R criteria, MMSE | Semi-quantitative food frequency (SFFQ) | Higher dietary vit C intake associated with less AD after a mean of 6.5 years, controlling for supplements |
| Kalmijn, 1997 [57] | Pros | 342 Men | 69–89 | 3 | MMSE | Dietary history FFQ | Higher vit C intake not correlated with cognitive decline or impairment after 3 years |
| Laurin, 2003 [58] | Pros | 2549 Men | 45–68 | 4 | Hasegawa dementia screening instrument, MMSE, 3MS | 24-h dietary recall | Vit C was not associated with the risk of dementia or its subtypes across an 8-year period |
| Basambombo, 2016 [59] | Pros | 5269 | ≥65 | 2.5 | Diagnostic and Statistical Manual of Mental Disorders (DSM-III-R) | Self-reported supplementation | The use of vitamin C supplements associated with a reduced risk of cognitive decline during 3, 5 year intervals |
| Nooyens, 2015 [60] | Pros | 2613 | 43–70 | 5 | 15 Words Learning Test, the Stroop Test, Word Fluency test, Letter Digit Substitution Test | 178-item semi-quantitative FFQ | No associations between intakes of vit C and cognitive decline across 5 years |
| Peneau, 2011 [61] | Pros | 2533 | 45–60 | 4.5 | RI-48 cued recall, semantic, and phonemic fluency tests, trail-making and forward and backward digit span tests | 24-h dietary record | vit C–rich FVs (P-trend = 0.03), vitamin C (P-trend = 0.005) positively associated with verbal memory across 13 years |
| Fotuhi, 2008 [62] | Pros | 3376 | ≥65 | 2.5 | 3MS | Self-report | Combined vit C, E, and anti-inflammatory resulted in a lower decline on the 3MS across 8 years. Vit C alone had no affect |
| Gray, 2008 [63] | Pros | 2969 | ≥65 | 3.5 | Cognitive abilities screening instrument | Self-report | No association between vitamin C and AD incidence, or vit C and E together after 2.8–8.7 years |
| Wengreen, 2007 [64] | Pros | 3831 | ≥65 | 3.5 | 3MS | Food frequency | Higher quartiles of vit C intake had a greater 3MS score and lower vit C intake had a greater rate of decline during 7 years |
| Fillenbaum, 2005 [65] | Pros | 616 | 65–105 | 3.5 | Short portable mental status questionnaire | In home interview | Vitamin C did not reduce AD or dementia incidence over either 3 or 14-year interval |
| Maxwell, 2005 [66] | Pros | 894 | ≥65 | 3.5 | 3MS | Self-report | Subjects reporting supplementation of vit C were less likely to have cognitive decline or to be diagnosed with VCI after 5 years |
| Grodstein, 2003 [67] | Pros | 14,968 | 70–79 women | 4.5 | Telephone Interview of Cognitive Status, Delayed recall of 10 word lists, Immediate and delayed recall of paragraph, Verbal fluency, Digit span backwards | Supplementation questionnaire | Vit C and E had higher mean global scores than non-supplemented. Vit C alone did not affect global score after 5 years |
| Luchsinger, 2003 [68] | Pros | 980 | ≥65 | 4.5 | Neuropsychological test battery | Semi quantitative food frequency | Neither dietary, supplemental nor total intake of vit C across 4 years was linked to AD Incidence |
| Morris, 2002 [69] | Pros | 815 | >65 | 3 | Consortium Established for Research on AD | FFQ | Intake of vitamin C was not significantly associated with risk of AD across 3.9 years |
| Peacock, 2000 [70] | Pros | 12,187 | 48–67 | 4.5 | Delayed word recall test, Wechsler adult intelligence scale, Revised digit symbol subtest, word fluency test | Food frequency questionnaire | No consistent association between dietary and supplemental vit C and cognition across 8 years |
| Morris, 1998 [71] | Pros | 633 | ≥65 | 3.5 | Criteria for clinical diagnosis | Supplementation questionnaire | None of the vitamin C users were diagnosed after a mean of 4.3 years |
| Mendelsohm, 1996 [72] | Pros | 1059 | ≥65 | 2.5 | Neuropsychological battery (15 items) | 297 vitamin C self-report supplementation | After adjustment for age, race, income, education, vit C supplementation did not relate to cognitive scores during 2 years |
| Berti, 2015 [73] | Cross | 52 Women | 54–66 | 1.5 | Clinical dementia rating, Global deterioration score, MMSE | Harvard/Willet FFQ | Antioxidant consumption positively associated with METglc (p < 0.001) |
| Beydoun, 2015 [74] | Cross | 1274 | 30–60 | 2 | MMSE, CLVT-list A, CVLT-DFR, digit span forward/backwards, Benten visual retention test, Animal fluency test, Brief test of attention, trail making test, Clock drawing test, card rotations, identical pictures | Two 24-h recalls | Vitamin C not associated with cognition on either cognitive task, MMSE error count (p = 0.17) |
| Chaudhari, 2015 [75] | Cross | 582 | 40–96 | 2 | Repeatable battery for the assessment of neurological status, The executive interview | Ascorbate supplementation (self-report) | Vit C led to better immediate memory (p = 0.04), visuospatial skills (p = 0.002), language (p = 0.01), global cognition (p = 0.006) |
| Goodwin, 1983 [76] | Cross | 260 | >60 | 2 | Halstead-Reitan Categories, (Non-verbal abstract thinking), Wechsler Memory Test | Dietary intake/Ascorbate plasma | Performance worse on both tasks in those with low vit C (5–10% lowest levels) |
| Jama, 1996 [77] | Cross | 5182 | 55–95 | 2.5 | MMSE | Semi-quantitative food frequency questionnaire | No association between cognitive function and intake of vitamin C intake (<70mg/day (odd ratio) = 1.14, 130–160 mg/day (od) = 1.21 |
| Lindemann, 2000 [78] | Cross | 195 | ≥65 | 3 | MMSE, WAIS-R Digits Forward, Fuld Object Memory Evaluation, Clock drawing, Two Color Trail Making Tests | Serum ascorbate | Lower vit C not associated with cognition. There was a trend. Low vit C linked with a history of depression |
| Perrig, 1997 [79] | Cross | 442 | ≥65 | 3 | Computerised cognitive test (assessed working, implicit and explicit memory), WAIS-R vocabulary test | Plasma Ascorbate | Free recall, recognition, and vocabulary (not priming or working memory) correlated with ascorbic acid concentrations (semantic memory p = 0.034, vocabulary test p ≤ 0.021) |
| Schmidt, 1998 [80] | Cross | 1769 | 50–75 | 2 | Mattis Dementia Rating Scale | Plasma (chromatograph) | No association between cognitive scores and plasma concentrations (odds ratio = 1, p = 0.87) |
| Sato, 2006 [81] | Cross | 544 | ≥65 | 2.5 | Digit symbol substitution task (DSST), MMSE | Ascorbate plasma, Block’s FFQ | Highest fifth of plasma ascorbate associated with better DSST, marginally with MMSE |
| Whalley, 2003 [82] | Cross | 176 | 77 | 2.5 | MMSE, Raven’s Progressive Matrices | Ascorbate plasma, FFQ (MONICA) | No difference between those taking vitamin C supplements and controls, after controlling for childhood IQ, education, socioeconomic status and cardiovascular health |
| Perkins, 1998 [83] | Cross | 4809 | >60 | 2 | Delayed word recall, Delayed story recall | Serum ascorbate | After adjusting for socioeconomic factors and other trace elements, vitamin C concentrations were not associated with poor memory performance |
| Ortega, 1997 [84] | Cross | 260 | 65–90 | 1.5 | MMSE, Pfeiffer’s mental status questionnaire | Food frequency for 7 days | Higher cognition correlated with great vitamin C intake across 7 days |
| Requejo, 2003 [85] | Cross | 168 | 65–90 | 0.5 | MMSE | Food record | Those with a greater intake of vitamin C were more likely to display adequate cognitive ability |
| Study | Study Design | Reason for Exclusion |
|---|---|---|
| Kennedy (2011) [86] | RCT | Mood/fatigue primary measures, vitamin C status not assessed |
| Smith (1999) [87] | RCT | Self-reported cognitive failures (subjective cognitive assessment) |
| Kumar (2008) [88] | RCT | Vitamin C status not assessed |
| Yaffe (2004) [89] | RCT | Cognition not assessed at baseline, vitamin C status not assessed |
| Kang (2009) [90] | RCT | Cognition not assessed at baseline, only 3.5 years after intervention |
| Chui (2008) [91] | RCT | Vitamin C status not assessed, no placebo/blinding |
| Day (1988) [92] | RCT | Vitamin C status not assessed, assessed only confusion |
| Paraskevas (1997) [93]/Quinn (2004) [27]/Woo (1989) [94]/Polidori (2002) [95]/Foy (1998) [96] | CS | No cognitive tests administered |
| Talley [97] | Pre-test post-test | Simple orientation/consciousness assessment |
| Paper | Study Design | N | Mean Vitamin C Level in μmol/L (SD) | Mean MMSE Score (SD) |
|---|---|---|---|---|
| Burns (1989) [39] | RCT | 81 | Intervention baseline-33.5 (28) Placebo baseline-31.8 (31) Placebo final-25 (28) # | 1.9 (3.3) 5.7 (9.1) 5.7 (10.6) # |
| Bowman (2009) [26] | Pros | 32 | 41 (30) | 19 (5) |
| Rinaldi (2003) [42] | CS | 25 63 | MCI-24.9 (2.4) AD-25.9 (8.9) | 26.9 (2) 13.5 (6.5) |
| Polidori (2004) [43] | CS | 63 23 | AD-25.9 (8.9) Vascular AD-26.6 (11.3) | 20.4 (3) 19.8 (3) |
| Glaso (2004) [47] | CC | 20 | AD-44 (25) | 16.9 |
| Rivierie (1999) [48] | CC | 24 9 20 | Moderate AD-35.7 Hospitalized AD-19.3 Severe AD-20.4 | 17.2 (4.9) 16.3 (6.1) 3.3 (3.1) |
| Paper | Study Design | N | Vitamin C Level in μmol/L (SD) | MMSE Score (SD) |
|---|---|---|---|---|
| Engelhart (2002) [56] * | Pros | 5395 | 61.7 (27) | 28 |
| Jama (1996) [77] * | CS | 5182 | 57.5 | 28 |
| Ortega (1997) [84] | CS | 260 | 62.7 (33.5) | 27.4 (4.8) |
| Whalley (2003) [82] | CS | 79 31 | Non-supplement user-33.7 (26.2) Supplement user-48.2 (25.7) | 28.5 (1.4) 28.9 (1.4) |
| Glaso (2004) [47] | CC | 18 | Control group-80 (28) | 27.2 |
| Polidori (2004) [43] | CS | 55 | Control group-52.4 (16.4) | 28.7 (1) |
| Rinaldi (2003) [42] | CS | 53 | Control group-52.4 (16.5) | 28.1 (1.4) |
| Chandra (2001) [50] # | RCT | 86 | Adequate Deficient | 28 (6.3) 17 (4) |
| Lindemann (2003) [78] # | CC | 195 | >57 <57 | 27.2 (2.4) 26.4 (2.9) |
| Sato (2006) [81] # | CC | 544 | Median = 74.9 (interquartile range = 57.8–90.7) Median = 78.9 (interquartile range = 64.1–99.2) | <27 >27 |
| Richardson (2002) [44] # | CC | 37 | <11 11–40 40–100 | 23 (12.3) 25 (6.0) 27 (5.1) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Travica, N.; Ried, K.; Sali, A.; Scholey, A.; Hudson, I.; Pipingas, A. Vitamin C Status and Cognitive Function: A Systematic Review. Nutrients 2017, 9, 960. https://doi.org/10.3390/nu9090960
Travica N, Ried K, Sali A, Scholey A, Hudson I, Pipingas A. Vitamin C Status and Cognitive Function: A Systematic Review. Nutrients. 2017; 9(9):960. https://doi.org/10.3390/nu9090960
Chicago/Turabian StyleTravica, Nikolaj, Karin Ried, Avni Sali, Andrew Scholey, Irene Hudson, and Andrew Pipingas. 2017. "Vitamin C Status and Cognitive Function: A Systematic Review" Nutrients 9, no. 9: 960. https://doi.org/10.3390/nu9090960
APA StyleTravica, N., Ried, K., Sali, A., Scholey, A., Hudson, I., & Pipingas, A. (2017). Vitamin C Status and Cognitive Function: A Systematic Review. Nutrients, 9(9), 960. https://doi.org/10.3390/nu9090960