Vitamin C Intake is Inversely Associated with Cardiovascular Mortality in a Cohort of Spanish Graduates: the SUN Project



Abstract
:
1. Introduction
2. Materials and Methods
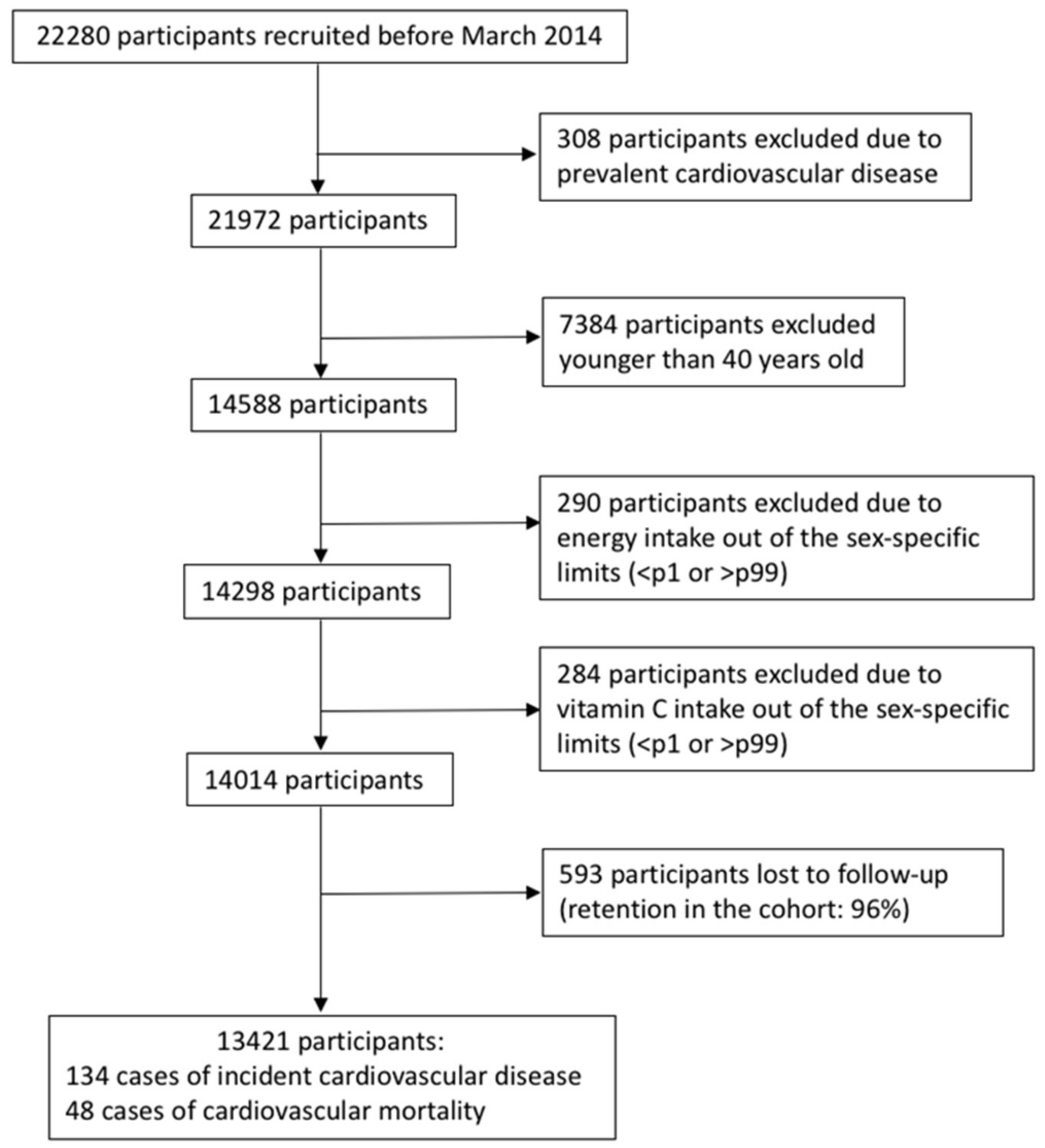
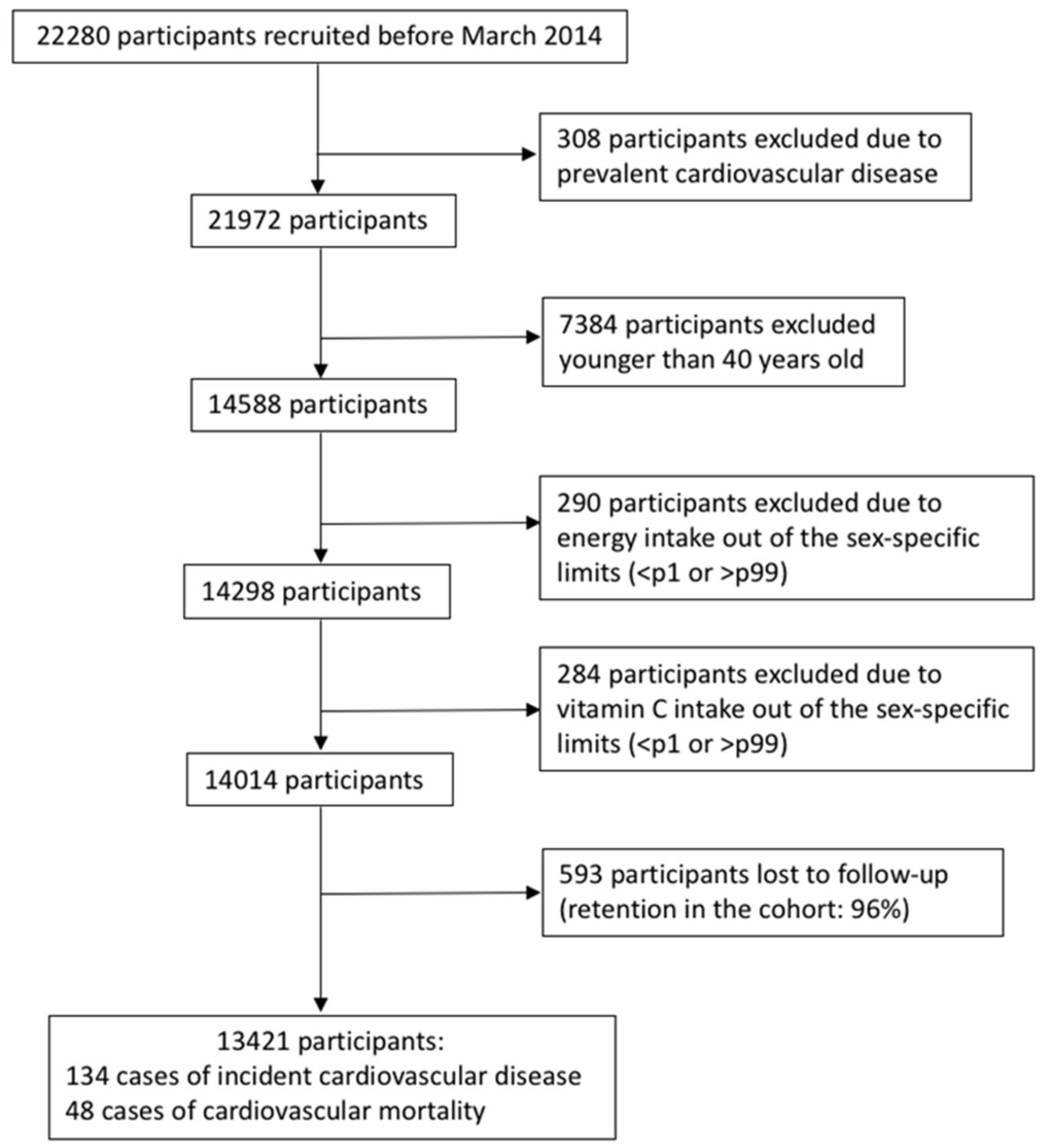
2.1. Study Population
2.2. Exposure Assessment
2.3. Outcome Assessment
2.4. Covariates
2.5. Statistical Analysis
3. Results
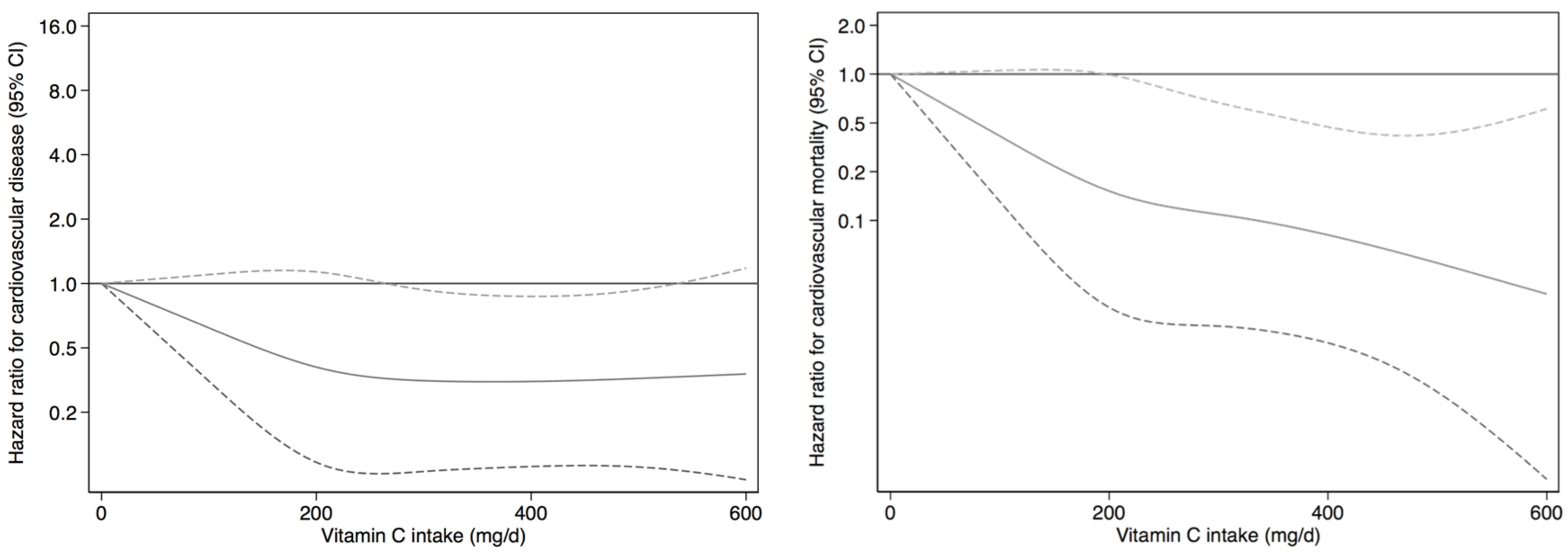
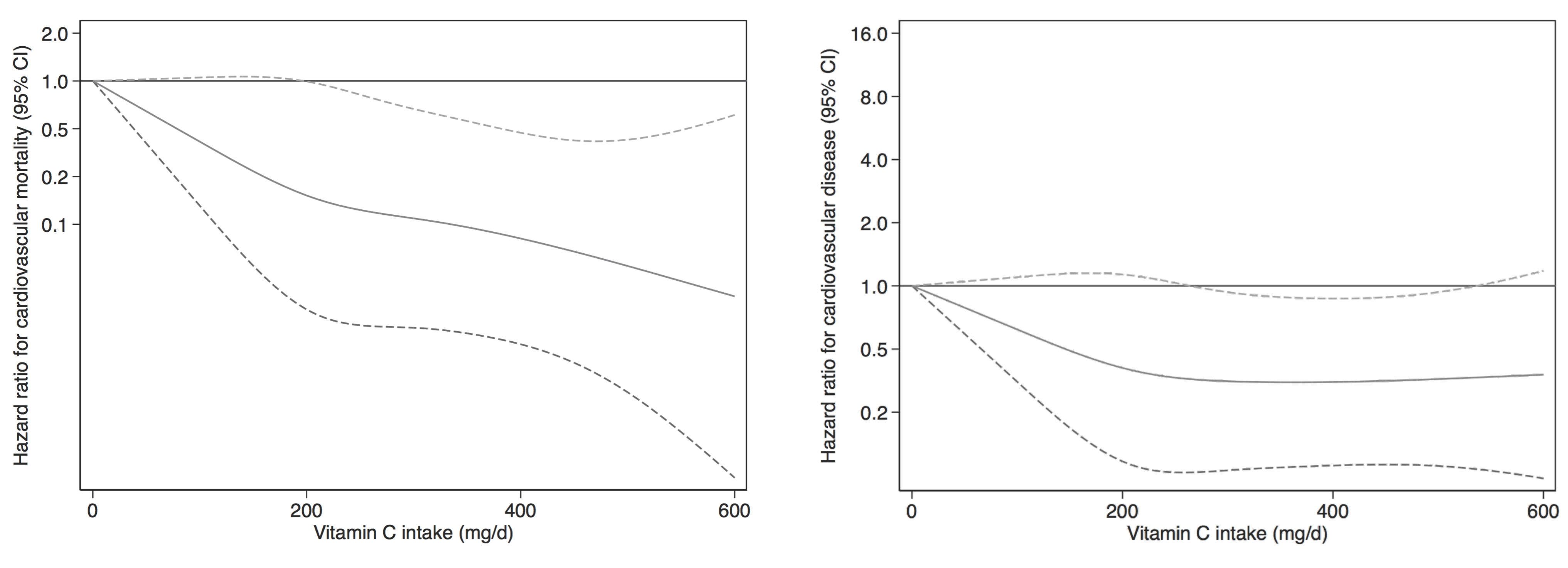
3.1. Cardiovascular Disease
3.2. Cardiovascular Mortality
3.3. Fiber-Adjusted Vitamin C Intake
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Chun, O.K.; Floegel, A.; Chung, S.J.; Chung, CE.; Song, W.O.; Koo, S.I. Estimation of Antioxidant Intakes from Diet and Supplements in U.S. Adults. J. Nutr. 2010, 140, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Moser, M.; Chun, O. Vitamin C and Heart Health: A Review Based on Findings from Epidemiologic Studies. Int. J. Mol. Sci. 2016, 17, 1328. [Google Scholar] [CrossRef] [PubMed]
- Joshipura, K.J.; Hu, F.B.; Manson, J.E.; Stampfer, M.J.; Rimm, E.B.; Speizer, F.E.; Colditz, G.; Ascherio, A.; Rosner, B.; Spiegelman, D.; et al. The effect of fruit and vegetable intake on risk for coronary heart disease. Ann. Intern. Med. 2001, 134, 1106–1114. [Google Scholar] [CrossRef] [PubMed]
- Holmberg, S.; Thelin, A.; Stiernström, E.L. Food Choices and Coronary Heart Disease: A Population Based Cohort Study of Rural Swedish Men with 12 Years of Follow-up. Int. J. Environ. Res. Public Health 2009, 6, 2626–2638. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; de la Fuente-Arrillaga, C.; López-Del-Burgo, C.; Vázquez-Ruiz, Z.; Benito, S.; Ruiz-Canela, M. Low consumption of fruit and vegetables and risk of chronic disease: A review of the epidemiological evidence and temporal trends among Spanish graduates. Public Health Nutr. 2011, 14, 2309–2315. [Google Scholar] [CrossRef] [PubMed]
- Buijsse, B.; Jacobs, D.R.; Steffen, L.M.; Kromhout, D.; Gross, M.D.; Abbott, R. Plasma Ascorbic Acid, A Priori Diet Quality Score, and Incident Hypertension: A Prospective Cohort Study. PLoS ONE 2015, 10, e0144920. [Google Scholar] [CrossRef] [PubMed]
- Pfister, R.; Sharp, S.J.; Luben, R.; Wareham, N.J.; Khaw, K.T. Plasma vitamin C predicts incident heart failure in men and women in European Prospective Investigation into Cancer and Nutrition-Norfolk prospective study. Am. Heart J. 2011, 162, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Khaw, K.T.; Bingham, S.; Welch, A.; Luben, R.; Wareham, N.; Oakes, S.; Day, N. Relation between plasma ascorbic acid and mortality in men and women in EPIC-Norfolk prospective study: A prospective population study. European Prospective Investigation into Cancer and Nutrition. Lancet 2001, 357, 657–663. [Google Scholar] [CrossRef]
- Mangels, A.R.; Block, G.; Frey, C.M.; Patterson, B.H.; Taylor, P.R.; Norkus, E.P.; Levander, O.A. The bioavailability to humans of ascorbic acid from oranges, orange juice and cooked broccoli is similar to that of synthetic ascorbic acid. J. Nutr. 1993, 123, 1054–1061. [Google Scholar] [PubMed]
- Sesso, H.D.; Buring, J.E.; Christen, W.G.; Kurth, T.; Belanger, C.; MacFadyen, J.; Bubes, V.; Manson, J.E.; Glynn, R.J.; Gaziano, J.M. Vitamins E and C in the Prevention of Cardiovascular Disease in Men. JAMA 2008, 300, 2123–2133. [Google Scholar] [CrossRef] [PubMed]
- Cook, N.R.; Albert, C.M.; Gaziano, J.M.; Zaharris, E.; MacFadyen, J.; Danielson, E; Buring, J.E.; Manson, J.E. A Randomized Factorial Trial of Vitamins C and E and Beta Carotene in the Secondary Prevention of Cardiovascular Events in Women. Arch. Intern. Med. 2007, 167, 1610–1618. [Google Scholar] [CrossRef] [PubMed]
- Ellulu, M.S.; Rahmat, A.; Ismail, P.; Khaza’ ai, H.; Abed, Y. Effect of vitamin C on inflammation and metabolic markers in hypertensive and/or diabetic obese adults: A randomized controlled trial. Drug Des. Devel. Ther. 2015, 9, 3405–3412. [Google Scholar] [CrossRef] [PubMed]
- Brown, B.G.; Zhao, X.Q.; Chait, A.; Fisher, L.D.; Cheung, M.C.; Morse, J.S.; Dowdy, A.A.; Marino, E.K.; Bolson, E.L.; Alaupovic, P. Simvastatin and Niacin, Antioxidant Vitamins, or the Combination for the Prevention of Coronary Disease. N. Engl. J. Med. 2001, 345, 1583–1592. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.H.; Folsom, A.R.; Harnack, L.; Halliwell, B.; Jacobs, D.R. Does supplemental vitamin C increase cardiovascular disease risk in women with diabetes? Am. J. Clin. Nutr. 2004, 80, 1194–1200. [Google Scholar] [PubMed]
- Waters, D.D.; Alderman, E.L.; Hsia, J.; Howard, B.V.; Cobb, F.R.; Rogers, W.J.; Ouyang, P.; Thompsom, P.; Tardif, J.C.; Higginson, L. Effects of hormone replacement therapy and antioxidant vitamin supplements on coronary atherosclerosis in postmenopausal women: a randomized controlled trial. JAMA 2002, 288, 2432–2440. [Google Scholar] [CrossRef] [PubMed]
- Ashor, A.W.; Lara, J.; Mathers, J.C.; Siervo, M. Effect of vitamin C on endothelial function in health and disease: A systematic review and meta-analysis of randomised controlled trials. Atherosclerosis 2014, 235, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Juraschek, S.P.; Guallar, E.; Appel, L.J.; Miller, E.R. Effects of vitamin C supplementation on blood pressure: A meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2012, 95, 1079–1088. [Google Scholar] [CrossRef] [PubMed]
- Seguí-Gómez, M.; de la Fuente, C.; Vázquez, Z.; de Irala, J.; Martínez-González, M.A. Cohort profile: The “Seguimiento Universidad de Navarra” (SUN) study. Int. J. Epidemiol. 2006, 35, 1417–1422. [Google Scholar] [CrossRef] [PubMed]
- Martin-Moreno, J.M.; Boyle, P.; Gorgojo, L.; Maisonneuve, P.; Fernandez-Rodriguez, J.C.; Salvini, S.; Willett, W.C. Development and validation of a food frequency questionnaire in Spain. Int. J. Epidemiol. 1993, 22, 512–519. [Google Scholar] [CrossRef] [PubMed]
- De la Fuente-Arrillaga, C.; Vázquez-Ruiz, Z.; Bes-Rastrollo, M.; Sampson, L.; Martínez-Gonzlez, M.A. Reproducibility of an FFQ validated in Spain. Public Health Nutr. 2010, 13, 1364–1372. [Google Scholar] [CrossRef] [PubMed]
- Mataix-Verdu, J.; Manas, M.; Martinez-Victoria, E.; Sanchez, J.J.; Borregon, A. Tabla de Composición de Alimentos Españoles (Spanish Food Composition Tables), 4th ed.; Universidad de Granada Press: Granada, Spain, 2003. [Google Scholar]
- Moreiras, O.; Carbajal, A.; Cabrera, L. Tablas de Composición de Alimentos (Food Composition Tables), 9th ed.; Pirámide: Madrid, Spain, 2005. [Google Scholar]
- World Health Organization. International Classification of Diseases; 10th Revision (ICD-10); World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Bes-Rastrollo, M.; Valdivieso, J.R.; Sánchez-Villegas, A.; Alonso, Á.; Martínez-González, M.A. Validación del peso e índice de masa corporal auto-declarados de los participantes de una cohorte de graduados universitarios. Rev. Española. Obes. 2005, 3, 183–189. [Google Scholar]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean Diet and Survival in a Greek Population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; López-Fontana, C.; Varo, J.J.; Sánchez-Villegas, A.; Martinez, J.A. Validation of the Spanish version of the physical activity questionnaire used in the Nurses’ Health Study and the Health Professionals’ Follow-up Study. Public Health Nutr. 2005, 8, 920–927. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O’brien, W.L.; Bassett, D.R.; Schmitz, K.H.; Emplaincourt, P.O. Compendium of physical activities: An update of activity codes and MET intensities. Med. Sci. Sports Exerc. 2000, 32, S498–S504. [Google Scholar] [CrossRef] [PubMed]
- Javier Basterra-Gortari, F.; Bes-Rastrollo, M.; Gea, A.; Núñez-Córdoba, J.; Toledo, E.; Martínez-González, M.Á. Television Viewing, Computer Use, Time Driving and All-Cause Mortality: The SUN Cohort. J. Am. Heart Assoc. 2014, 3, e000864. [Google Scholar] [CrossRef] [PubMed]
- Alonso, Á.; Beunza, J.J.; Delgado-Rodríguez, M.; Martínez-González, M.A. Validation of self reported diagnosis of hypertension in a cohort of university graduates in Spain. BMC Public Health 2005, 5, 94. [Google Scholar] [CrossRef] [PubMed]
- Barrio-Lopez, M.T.; Bes-Rastrollo, M.; Beunza, J.J.; Fernández-Montero, A.; García-López, M.; Martínez-González, M.A. Validation of metabolic syndrome using medical records in the SUN cohort. BMC Public Health 2011, 11, 867. [Google Scholar] [CrossRef] [PubMed]
- Salvayre, R.; Negre-Salvayre, A.; Camaré, C. Oxidative theory of atherosclerosis and antioxidants. Biochimie 2016, 125, 281–296. [Google Scholar] [CrossRef] [PubMed]
- Weber, C.; Erl, W.; Weber, K.; Weber, P.C. Increased Adhesiveness of Isolated Monocytes to Endothelium Is Prevented by Vitamin C Intake in Smokers. Circulation 1996, 93, 1488–1492. [Google Scholar] [CrossRef] [PubMed]
- Siow, R.C.M.; Richards, J.P.; Pedley, K.C.; Leake, D.S.; Mann, G.E. Vitamin C Protects Human Vascular Smooth Muscle Cells Against Apoptosis Induced by Moderately Oxidized LDL Containing High Levels of Lipid Hydroperoxides. Arterioscler. Thromb. Vasc. Biol. 1999, 19, 2387–2394. [Google Scholar] [CrossRef] [PubMed]
- D’Uscio, L.V.; Milstien, S.; Richardson, D.; Smith, L.; Katusic, Z.S. Long-Term Vitamin C Treatment Increases Vascular Tetrahydrobiopterin Levels and Nitric Oxide Synthase Activity. Circ. Res. 2003, 92, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | Tertiles of Vitamin C Intake | ||||
|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | p | ||
| N | 4474 | 4474 | 4473 | ||
| Vitamin C intake (mg/day) | 148 (44.2) | 257 (33.0) | 445 (114) | <0.001 | |
| Fiber intake (g/day) | 23.0 (10.0) | 27.8 (9.8) | 38.3 (14.1) | <0.001 | |
| Vittamin C range (mg/day) | 0–205 | 206–319 | 320–1110 | ||
| Vittamin C from supplements (mg/day) | 0.56 (4.2) | 2.0 (10.0) | 9.6 (33.4) | <0.001 | |
| Sex (female) | 41.6 | 55.8 | 67.9 | <0.001 | |
| Age (years) | 41.2 (10.3) | 42.8 (10.7) | 43.7 (10.8) | <0.001 | |
| BMI (kg/m2) | 24.3 (3.6) | 24.1 (3.5) | 23.8 (3.5) | <0.001 | |
| Mediterranean Dietary Score § | <0.001 | ||||
| Low (0–2 points) | 39.0 | 29.6 | 21.4 | ||
| Medium (3–4 points) | 47.3 | 50.9 | 51.1 | ||
| High (5–7 points) | 13.7 | 19.5 | 27.5 | ||
| Energy intake (kcal/day) | 2548 (804) | 2346 (710) | 2530 (755) | 0.26 | |
| Physical activity (MET-h/week) | 23.4 (20.6) | 25.8 (21.6) | 29.2 (25.3) | <0.001 | |
| Television time (h/week) | 1.63 (1.1) | 1.57 (1.1) | 1.51 (1.1) | <0.001 | |
| Family history of myocardial infarction | 15.8 | 18.3 | 17.1 | 0.09 | |
| Smoking | 0.03 | ||||
| Never | 43 | 44 | 44 | ||
| Current | 29 | 23 | 22 | ||
| Former | 28 | 33 | 34 | ||
| Prevalent diseases | |||||
| Cancer | 3.7 | 4.6 | 5.6 | <0.001 | |
| Coronary heart disease | 0.38 | 0.47 | 0.27 | 0.39 | |
| Tachycardia | 1.9 | 1.6 | 2.3 | 0.12 | |
| Atrial fibrillation | 0.65 | 0.72 | 0.69 | 0.80 | |
| Aortic aneurism | 0.25 | 0.11 | 0.02 | 0.01 | |
| Heart failure | 0.42 | 0.56 | 0.38 | 0.75 | |
| Pulmonary embolism | 0.13 | 0.09 | 0.11 | 0.75 | |
| Venous thrombosis | 0.51 | 0.92 | 0.92 | 0.03 | |
| Claudication | 0.31 | 0.31 | 0.56 | 0.07 | |
| Diabetes | 1.4 | 2.2 | 3.0 | <0.001 | |
| Hypertension | 9.7 | 11.3 | 10.9 | 0.07 | |
| Hypercholesterolemia | 20.0 | 21.9 | 20.7 | 0.42 | |
| Hypertriglyceridemia | 8.5 | 8.9 | 7.3 | 0.04 | |
| Drugs | |||||
| Digoxin | 0.11 | 0.13 | 0.13 | 0.77 | |
| Diuretics | 1.0 | 1.6 | 1.7 | 0.01 | |
| Beta blockers | 1.7 | 2.3 | 1.9 | 0.40 | |
| Calcium antagonists | 0.40 | 0.45 | 0.63 | 0.13 | |
| Nitrite | 0.13 | 0.11 | 0.18 | 0.57 | |
| Antihypertensives | 2.8 | 4.1 | 3.7 | 0.03 | |
| Aspirin | 3.4 | 5.2 | 4.9 | 0.001 | |
| Other CV treatment drug | 5.2 | 6.9 | 6.6 | 0.01 | |
| Main Analyses § | Tertiles of Vitamin C Intake | ||
|---|---|---|---|
| Q1 (N = 4474) | Q2 (N = 4474) | Q3 (N = 4473) | |
| Incident CVD (person-years at risk) | 61 (50,792) | 38 (48,765) | 35 (47,415) |
| Age-adjusted | 1.00 (Ref.) | 0.52 (0.35–0.78) | 0.44 (0.29–0.67) |
| Sex- and age-adjusted | 1.00 (Ref.) | 0.59 (0.39–0.89) | 0.56 (0.37–0.86) |
| Multivariable adjusted model 1 | 1.00 (Ref.) | 0.59 (0.39–0.90) | 0.60 (0.39–0.93) |
| T2 + T3 vs. T1 | 1.00 (Ref.) | 0.60 (0.42–0.85) | |
| Multivariable adjusted model 2 | 1.00 (Ref.) | 0.58 (0.38–0.88) | 0.58 (0.37–0.90) |
| T2 + T3 vs. T1 | 1.00 (Ref.) | 0.58 (0.41–0.83) | |
| Multivariable adjusted model 3 | 1.00 (Ref.) | 0.58 (0.38–0.88) | 0.58 (0.37–0.90) |
| T2 + T3 vs. T1 | 1.00 (Ref.) | 0.58 (0.41–0.83) | |
| Multivariable adjusted model 4 | 1.00 (Ref.) | 0.60 (0.40–0.91) | 0.62 (0.40–0.97) |
| T2 + T3 vs. T1 | 1.00 (Ref.) | 0.61 (0.43–0.88) | |
| Main Analyses § | Tertiles of Vitamin C Intake | ||
|---|---|---|---|
| Q1 (N = 4474) | Q2 (N = 4474) | Q3 (N = 4473) | |
| Cardiovascular deaths (person-years at risk) | 22 (51,016) | 15 (48,901) | 11 (47,577) |
| Age-adjusted | 1.00 (Ref.) | 0.55 (0.28–1.06) | 0.34 (0.17–0.73) |
| Sex- and age-adjusted | 1.00 (Ref.) | 0.56 (0.29–1.10) | 0.37 (0.17–0.79) |
| Multivariable adjusted model 1 | 1.00 (Ref.) | 0.57 (0.29–1.12) | 0.39 (0.18–0.86) |
| Multivariable adjusted model 2 | 1.00 (Ref.) | 0.54 (0.27–1.08) | 0.40 (0.18–0.89) |
| Multivariable adjusted model 3 | 1.00 (Ref.) | 0.54 (0.27–1.09) | 0.41 (0.19–0.92) |
| Multivariable adjusted model 4 | 1.00 (Ref.) | 0.56 (0.28–1.12) | 0.45 (0.20–1.01) |
| Main Analyses § | Tertiles of Vitamin C Intake | ||
|---|---|---|---|
| Q1 (N = 4474) | Q2 (N = 4474) | Q3 (N = 4473) | |
| Incident CVD (person-time-1 at risk) | 58 (49,706) | 44 (49,080) | 32 (48,186) |
| Multivariable adjusted § ‡ | 1.00 (Ref.) | 0.86 (0.57–1.29) | 0.74 (0.47–1.15) |
| Additionally adjusted for MDS | 1.00 (Ref.) | 0.86 (0.57–1.29) | 0.74 (0.47–1.15) |
| Cardiovascular deaths (person-years at risk) | 27 (49,879) | 14 (49,247) | 7 (48,368) |
| Multivariable adjusted § ‡ | 1.00 (Ref.) | 0.52 (0.26–1.02) | 0.30 (0.13–0.73) |
| Additionally adjusted for MDS | 1.00 (Ref.) | 0.52 (0.26–1.04) | 0.30 (0.12–0.72) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martín-Calvo, N.; Martínez-González, M.Á. Vitamin C Intake is Inversely Associated with Cardiovascular Mortality in a Cohort of Spanish Graduates: the SUN Project. Nutrients 2017, 9, 954. https://doi.org/10.3390/nu9090954
Martín-Calvo N, Martínez-González MÁ. Vitamin C Intake is Inversely Associated with Cardiovascular Mortality in a Cohort of Spanish Graduates: the SUN Project. Nutrients. 2017; 9(9):954. https://doi.org/10.3390/nu9090954
Chicago/Turabian StyleMartín-Calvo, Nerea, and Miguel Ángel Martínez-González. 2017. "Vitamin C Intake is Inversely Associated with Cardiovascular Mortality in a Cohort of Spanish Graduates: the SUN Project" Nutrients 9, no. 9: 954. https://doi.org/10.3390/nu9090954
APA StyleMartín-Calvo, N., & Martínez-González, M. Á. (2017). Vitamin C Intake is Inversely Associated with Cardiovascular Mortality in a Cohort of Spanish Graduates: the SUN Project. Nutrients, 9(9), 954. https://doi.org/10.3390/nu9090954