Developing and Implementing All-in-One Standard Paediatric Parenteral Nutrition

Abstract
:1. Introduction
2. Methodology
2.1. Developing the Composition of the Standard PN

{kind=link}
{kind=link}
| Component | Name | Manufacturer |
|---|---|---|
| Amino acids | Aminoven Infant 10% | Fresenius Kabi, Oberdorf, Switzerland |
| Glucose | Glucose 50% | Grosse Apotheke Dr. Bichsel AG, Interlaken, Switzerland |
| Lipids | SMOF Lipid | Fresenius Kabi, Oberdorf, Switzerland |
| Vitamins | Soluvit N | Fresenius Kabi, Oberdorf, Switzerland |
| Vitalipid N Infant | Fresenius Kabi, Oberdorf, Switzerland | |
| Trace Elements | Peditrace | Fresenius Kabi, Oberdorf, Switzerland |
| Sodium | Sodiumchloride (Concentration 59 mg/mL) | Manufactured in the hospital pharmacy |
| Sodiumacetate (Concentration 1 mmol/mL) | Manufactured in the hospital pharmacy | |
| Potassium | Potassiumchloride 7.45% | Sintetica, Mendrisio, Switzerland |
| Magnesium | Magnesiumchloride 0.5 M | B. Braun, Sempach, Switzerland |
| Phosphate | Glycophos | Fresenius Kabi, Oberdorf, Switzerland |
| Calcium | Calcium Sandoz 10% | Sandoz Pharmaceuticals, Novartis, Switzerland |
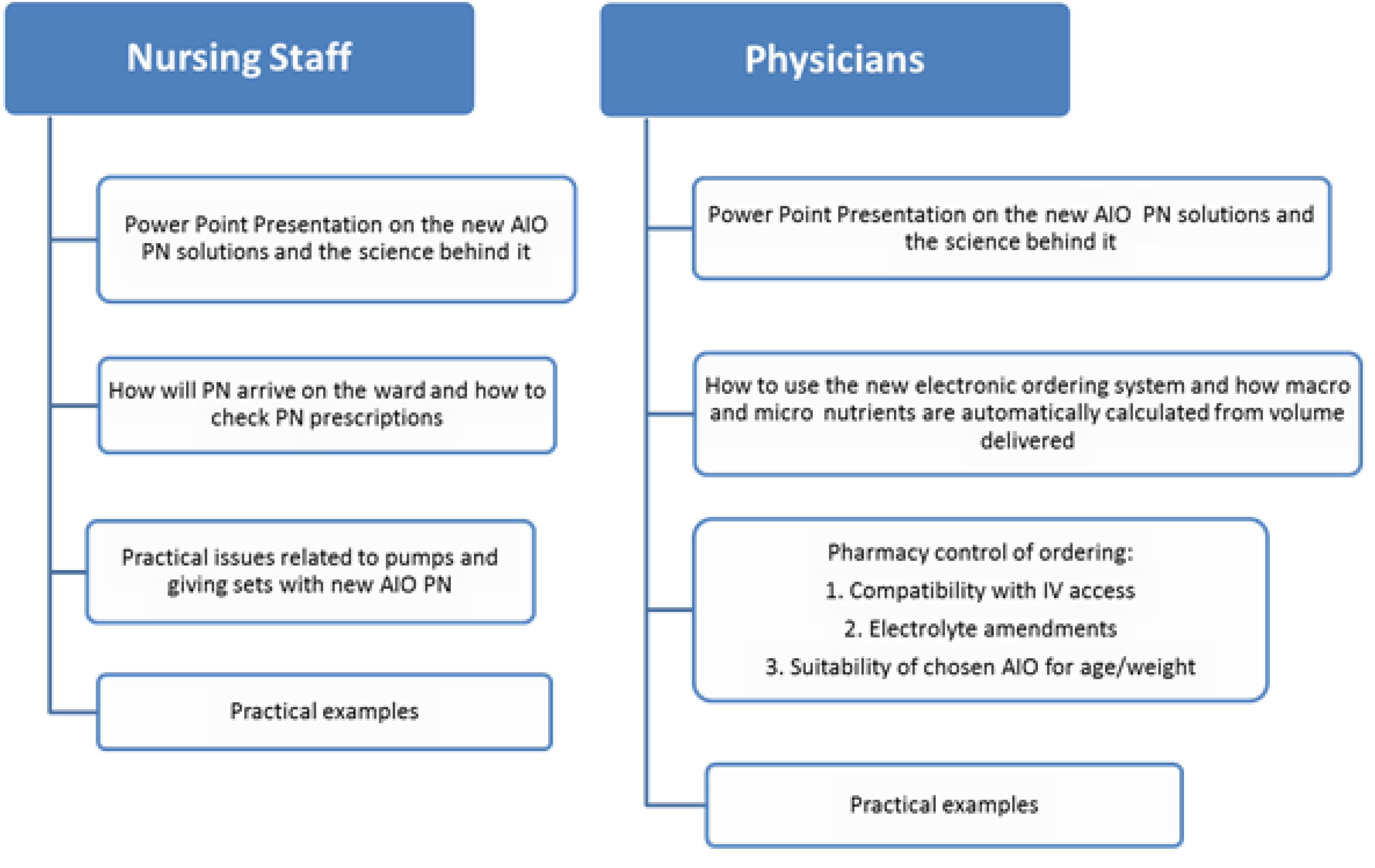
2.2. Implementation of the Standard PN


2.3. Review of Usage
- How many were ordered?
- How many children required electrolyte corrections?
- How many children required an individual PN solution?
- If any ordering/compounding errors were made.
3. Results
3.1. Composition
| Ped 1 | Ped 2 | Ped 3 | Ped 4 | |
|---|---|---|---|---|
| Birth–2 months | 2 months–10 kg | 11–16 kg | 16–30 kg | |
| (1000 mL) | (1000 mL) | (1500 mL) | (2000 mL) | |
| per 100 mL | per 100 mL | per 100 mL | per 100 mL | |
| 2.19 | 2.5 | 2.67 | 3.38 | |
| Glucose (g) | 10.5 | 14.5 | 14.47 | 14 |
| Lipids (g) | 2.5 | 2.8 | 3 | 3.5 |
| Energy (kcal) | 67 | 85 | 87 | 93 |
| Sodium (mmol) | 2.2 | 2.5 | 3 | 3.5 |
| Potassium (mmol) | 1.48 | 2 | 2.53 | 3.3 |
| Magnesium (mmol) | 0.15 | 0.2 | 0.19 | 0.18 |
| Calcium (mmol) | 0.5 | 0.8 | 0.25 | 0.3 |
| Phosphate (mmol) | 0.5 | 0.8 | 0.25 | 0.3 |
| Chloride (mmol) | 1.8 | 2.42 | 3.92 | 5.12 |
| Acetate (mmol) | 1.19 | 0.89 | 1.5 | 1.45 |
| Vitalipid/Soluvit 1:1 (mL) | 1.92 | 1.33 | 0.85 | 0.7 |
| 8Peditrace (mL) | 1 | 1 | 1 | 1 |
| Osmolarity (mOsmol/L) | 907 | 1185 | 1210 | 1280 |
| ESPGHAN requirements [1] | Nutrients delivered | |
|---|---|---|
| 80–120 | 90 | |
| Protein (g) | 1.5–2.5 | 2.4 |
| Glucose (g) | 12–14 | 13 |
| Lipids (g) | 2–3 | 2.7 |
| Energy (kcal) | 75–90 | 86 |
| Sodium (mmol) | 2–3 | 2.7 |
| Potassium (mmol) | 1–3 | 2.28 |
| Magnesium (mmol) | 0.2 | 0.17 |
| Calcium (mmol) | 0.2 | 0.23 |
| Phosphate (mmol) | 0.2 | 0.23 |
| Vitalipid/Soluvit 1:1 (mL) | 10 | 9 |
| Peditrace (mL) | 15 | 9 |
3.2. Data on Ordering of Standard PN
| AIO PN with/without electrolyte changes | Individual PN | |
|---|---|---|
| 5 | 3 | |
| Age in years (median) | 2.2 (range 0.8–5) | 12.6 (range 7–17) |
| Gender | 2 male | 3 male |
| Diagnosis | 4 short gut1 post gastrointestinal surgery | 3 graft versus host disease post bone marrow transplantation |
| Electrolyte amendments/reason for individual PN | 4 required amended potassium1 required the removing of sodium acetate | All 3 had hyperglycaemia, hyperlipidaemia and significant electrolyte disturbances. |
4. Discussion
5. Conclusions
Implications
Acknowledgements
Conflict of Interest
References
- Koletzko, B.; Goulet, O.; Hunt, J.; Krohn, K.; Shamir, R.; Parenteral Nutrition Guidelines Working Group; European Society for Clinical Nutrition and Metabolism; European Society of Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN); European Society of Paediatric Research (ESPR). Guidelines on Paediatric Parenteral Nutrition of the European Society of Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) and the European Society for Clinical Nutrition and Metabolism (ESPEN), Supported by the European Society of Paediatric Research (ESPR). J. Pediatr. Gastroenterol. Nutr. 2005, 41, S1–S87. [Google Scholar]
- Goulet, O.; Ruemmele, F.; Lacaille, F.; Colomb, V. Irreversible intestinal failure. J. Pediatr. Gastroenterol. Nutr. 2004, 38, 250–269. [Google Scholar] [CrossRef]
- Shulman, R.J.; Phillips, S. Parenteral nutrition in infants and children. J. Pediatr. Gastroenterol. Nutr. 2003, 36, 587–607. [Google Scholar] [CrossRef]
- Bonnabry, P.; Cingria, L.; Sadeghipour, F.; Ing, H.; Fonzo-Christe, C.; Pfister, R. Use of a systematic risk analysis method to improve safety in the production of paediatric parenteral nutrition solutions. Qual. Saf. Health Care 2005, 14, 93–98. [Google Scholar] [CrossRef]
- Mirtallo, J.; Canada, T.; Johnson, D.; Kumpf, V.; Petersen, C.; Sacks, G.; Seres, D.; Guenter, P. Safe practices for parenteral nutrition. JPEN J. Parenter. Enteral Nutr. 2004, 28, S39–S70. [Google Scholar] [CrossRef]
- Brown, C.L.; Garrison, N.A.; Hutchison, A.A. Error reduction when prescribing neonatal parenteral nutrition. Am. J. Perinatol. 2007, 24, 417–427. [Google Scholar] [CrossRef]
- Kochevar, M.; Guenter, P.; Holcombe, B.; Malone, A.; Mirtallo, J. ASPEN statement on parenteral nutrition standardization. J. Parenter. Enteral Nutr. 2007, 31, 441–448. [Google Scholar] [CrossRef]
- A Mixed Bag: An Enquiry into the Care of Hospital Patients Receiving Parenteral Nutrition. Available online: http://www.ncepod.org.uk/2010pn.htm (accessed on 21 November 2012).
- Fusch, C.; Bauer, K.; Bohles, H.J.; Jochum, F.; Koletzko, B.; Krawinkel, M.; Krohn, K.; Muhlebach, S.; Working Group for Developing The Guidelines for Parenteral Nutrition of The German Society for Nutritional Medicine. Neonatology/Paediatrics—Guidelines on Parenteral Nutrition, Chapter 13. Ger. Med. Sci. 2009, 7, Doc15. [Google Scholar] [CrossRef]
- Mackay, M.W.; Cash, J.; Farr, F.; Holley, M.; Jones, K.; Boehme, S. Improving pediatric outcomes through intravenous and oral medication standardization. J. Pediatr. Pharmacol. Ther. 2009, 14, 226–235. [Google Scholar]
- Improving Practice and Reducing Risk in the Provision of Parenteral Nutrition for Neonates and Children. Available online: http://www.nppg.scot.nhs.uk/Minimising%20risk%20in%20PN%20for%20children.pdf (accessed on 10 November 2012).
- Klüttgens, B.U.; Sewell, G.J.; Nunn, A.J. Current clinical practice in neonatal and paediatric parenteral nutrition in Europe. Eur. J. Hosp. Pharm. 2003, 9, 122–126. [Google Scholar]
- Bouchoud, L.; Fonzo-Christe, C.; Sadeghipour, F.; Bonnabry, P. How standardised are paediatric parenteral nutrition formulations in Europe? EJHP 2010, 16, 13–16. [Google Scholar]
- Clayton, P.T.; Whitfield, P.; Iyer, K. The role of phytosterols in the pathogenesis of liver complications of pediatric parenteral nutrition. Nutrition 1998, 14, 158–164. [Google Scholar] [CrossRef]
- Goulet, O.; Antebi, H.; Wolf, C.; Talbotec, C.; Alcindor, L.G.; Corriol, O.; Lamor, M.; Colomb-Jung, V. A new intravenous fat emulsion containing soybean oil, medium-chain triglycerides, olive oil, and fish oil: A single-center, double-blind randomized study on efficacy and safety in pediatric patients receiving home parenteral nutrition. J. Parenter. Enteral Nutr. 2010, 34, 485–495. [Google Scholar] [CrossRef]
- Diamond, I.R.; Pencharz, P.B.; Wales, P.W. What is the current role for parenteral lipid emulsions containing omega-3 fatty acids in infants with short bowel syndrome? Minerva Pediatr. 2009, 61, 263–272. [Google Scholar]
- Diamond, I.R.; Sterescu, A.; Pencharz, P.B.; Wales, P.W. The rationale for the use of parenteral omega-3 lipids in children with short bowel syndrome and liver disease. Pediatr. Surg. Int. 2008, 24, 773–778. [Google Scholar] [CrossRef]
- Krohn, K.; Babl, J.; Reiter, K.; Koletzko, B. Parenteral nutrition with standard solutions in paediatric intensive care patients. Clin. Nutr. 2005, 24, 274–280. [Google Scholar] [CrossRef]
- Rigo, J.; Marlowe, M.L.; Bonnot, D.; Senterre, T.; Lapillonne, A.; Kermorvant-Duchemin, E.; Hascoet, J.M.; Desandes, R.; Malfilatre, G.; Pladys, P.; et al. Benefits of a new pediatric triple-chamber bag for parenteral nutrition in preterm infants. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 210–217. [Google Scholar] [CrossRef]
- Porras, I.; Cabello, M.A.; Oya Alvarez de, M.B.; Marin Pozo, J.F.; Garcia, A.J.; Llacer, P.C. Assessment of standard parenteral nutrition in children (in Spanish). Nutr. Hosp. 2010, 25, 449–455. [Google Scholar]
- Narula, P.; Hartigan, D.; Puntis, J.W. The frequency and importance of reported errors related to parenteral nutrition in a regional paediatric centre. e-SPEN 2011, 6, e131–e134. [Google Scholar] [CrossRef]
- Bozzetti, F.; Arends, J.; Lundholm, K.; Micklewright, A.; Zurcher, G.; Muscaritoli, M. ESPEN Guidelines on Parenteral Nutrition: Non-surgical oncology. Clin. Nutr. 2009, 28, 445–454. [Google Scholar] [CrossRef]
- Wessel, J.J.; Kocoshis, S.A. Nutritional management of infants with short bowel syndrome. Semin. Perinatol. 2007, 31, 104–111. [Google Scholar] [CrossRef]
- Muhlebach, S.; Franken, C.; Stanga, Z. Practical handling of AIO admixtures—Guidelines on Parenteral Nutrition, Chapter 10. Ger. Med. Sci. 7, Doc18. [CrossRef]
- Seida, J.C.; Mager, D.R.; Hartling, L.; Vandermeer, B.; Turner, J.M. Parenteral omega-3 fatty acid lipid emulsions for children with intestinal failure and other conditions: A systematic review. J. Parenter. Enteral Nutr. 2013, 37, 44–55. [Google Scholar] [CrossRef]
- Muhammed, R.; Bremnerm, R.; Protheroe, S.; Johnson, T.; Holden, C.; Murphy, M.S. Resolution of parenteral nutrition-associated jaundice on changing from a soybean oil emulsion to a complex mixed-lipid emulsion. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 797–802. [Google Scholar] [CrossRef]
- Skouroliakou, M.; Matthaiou, C.; Chiou, A.; Panagiotakos, D.; Gounaris, A.; Nunn, T.; Andrikopoulos, N. Physicochemical stability of parenteral nutrition supplied as all-in-one for neonates. J. Parenter. Enteral Nutr. 2008, 32, 201–209. [Google Scholar] [CrossRef]
- Wong, T. Parenteral trace elements in children: Clinical aspects and dosage recommendations. Curr. Opin. Clin. Nutr. Metab. Care 2012, 15, 649–656. [Google Scholar] [CrossRef]
- Keady, S.; Morgan, C.; Ozzard, A.; Chauhan, B. Effect of a neonatal standard aquaous parenteral nutrition formulation on aceptic unit capacity planning. e-SPEN 2010, 5, e14–e17. [Google Scholar] [CrossRef]
- Gamsjager, T.; Brenner, L.; Schaden, E.; Sitzwohl, C.; Weinstabl, C. Cost analysis of two approaches to parenteral nutrition in critically ill children. Pediatr. Crit. Care Med. 2009, 10, 163–165. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Meyer, R.; Timmermann, M.; Schulzke, S.; Kiss, C.; Sidler, M.A.; Furlano, R.I. Developing and Implementing All-in-One Standard Paediatric Parenteral Nutrition. Nutrients 2013, 5, 2006-2018. https://doi.org/10.3390/nu5062006
Meyer R, Timmermann M, Schulzke S, Kiss C, Sidler MA, Furlano RI. Developing and Implementing All-in-One Standard Paediatric Parenteral Nutrition. Nutrients. 2013; 5(6):2006-2018. https://doi.org/10.3390/nu5062006
Chicago/Turabian StyleMeyer, Rosan, Meike Timmermann, Sven Schulzke, Caroline Kiss, Marc A. Sidler, and Raoul I. Furlano. 2013. "Developing and Implementing All-in-One Standard Paediatric Parenteral Nutrition" Nutrients 5, no. 6: 2006-2018. https://doi.org/10.3390/nu5062006
APA StyleMeyer, R., Timmermann, M., Schulzke, S., Kiss, C., Sidler, M. A., & Furlano, R. I. (2013). Developing and Implementing All-in-One Standard Paediatric Parenteral Nutrition. Nutrients, 5(6), 2006-2018. https://doi.org/10.3390/nu5062006