

Effects of 4:3 Intermittent Fasting on Eating Behaviors and Appetite Hormones: A Secondary Analysis of a 12-Month Behavioral Weight Loss Intervention

 , ,
, ,  , and
, and
Abstract

1. Introduction
2. Material and Methods
2.1. Trial Registration
2.2. Study Participants
2.3. Randomization and Interventions
2.4. Behavioral Support
2.5. Assessments
2.5.1. Eating Behaviors
Three-Factor Eating Questionnaire
Binge Eating Scale
Reward-Based Eating Drive Scale
2.5.2. Appetite Hormones
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
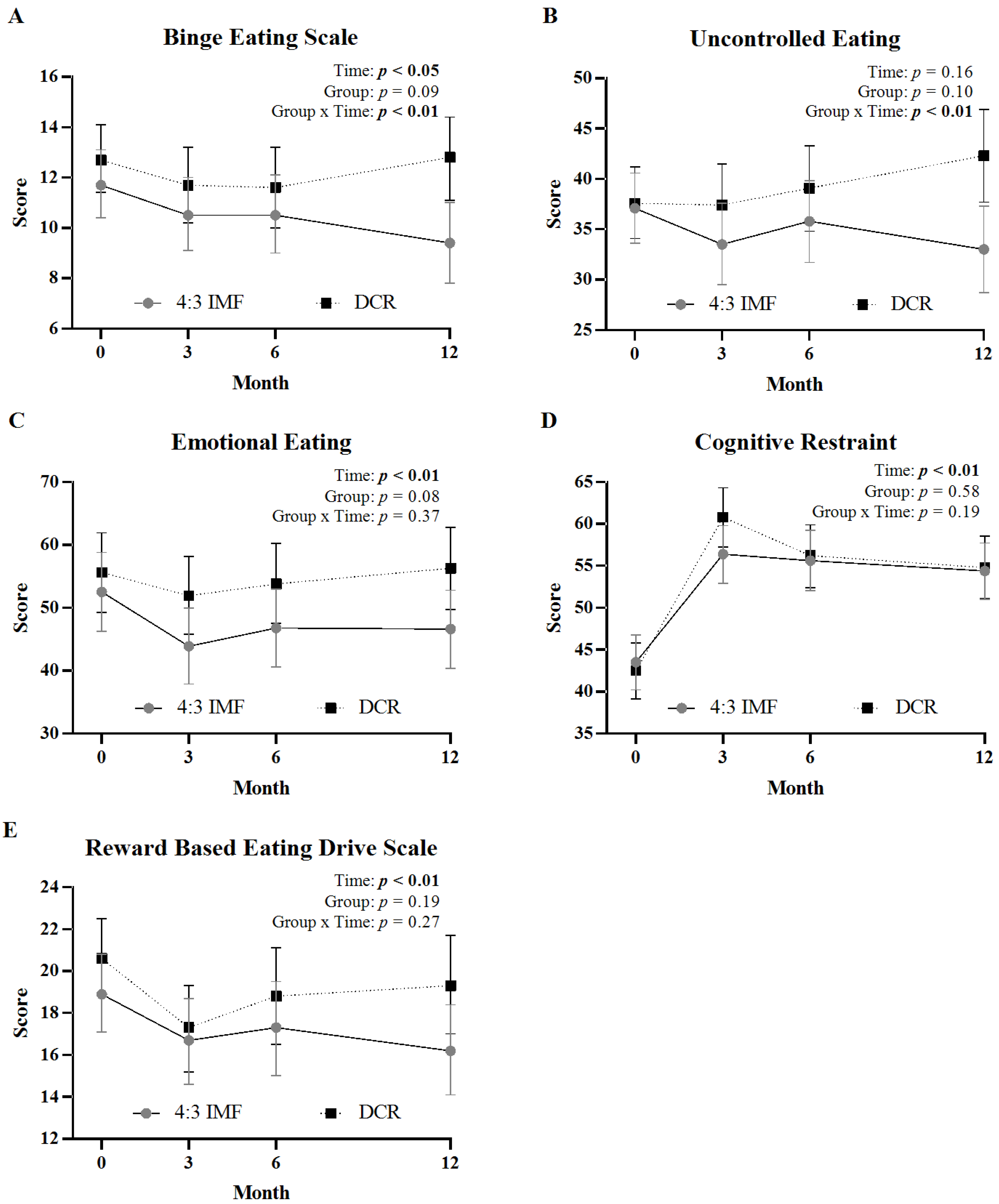
3.2. Change in Eating Behavior Scores over 12 Months
3.3. Correlation Between Eating Behavior Scores and Weight Loss
3.4. Change in Appetite-Related Hormones over 12 Months
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 4:3 IMF | 4:3 intermittent fasting |
| 5:2 IMF | 5:2 intermittent fasting |
| ADF | alternate day fasting |
| BDNF | brain-derived neurotrophic factor |
| BES | Binge Eating Scale |
| BMI | body mass index |
| CCTSI | Colorado Clinical and Translational Sciences Institute |
| CI | confidence interval |
| CU AMC | University of Colorado Anschutz Medical Campus |
| DCR | daily caloric restriction |
| DLW | doubly labeled water |
| EI | energy intake |
| fMRI | functional magnetic resonance imaging |
| IMF | intermittent fasting |
| kcal | kilocalorie |
| kg | kilogram |
| PYY | peptide YY |
| RDN | registered dietitian nutritionist |
| RED-13 | Reward-Based Eating Drive Scale, Revised 13-item |
| TFEQ-R18 | Three-Factor Eating Questionnaire, Revised 18-item |
| QEWP-5 | Questionnaire on Eating and Weight Patterns |
References
- Ng, M.; Gakidou, E.; Lo, J.; Abate, Y.H.; Abbafati, C.; Abbas, N.; Abbasian, M.; Abd ElHafeez, S.; Abdel-Rahman, W.M.; Abd-Elsalam, S.; et al. Global, regional, and national prevalence of adult overweight and obesity, 1990–2021, with forecasts to 2050: A forecasting study for the Global Burden of Disease Study 2021. Lancet 2025, 405, 813–838. [Google Scholar] [CrossRef]
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. Circulation 2014, 129, S102–S138. [Google Scholar] [CrossRef]
- Melby, C.L.; Paris, H.L.; Foright, R.M.; Peth, J. Attenuating the Biologic Drive for Weight Regain Following Weight Loss: Must What Goes Down Always Go Back Up? Nutrients 2017, 9, 468. [Google Scholar] [CrossRef]
- Sumithran, P.; Prendergast, L.A.; Delbridge, E.; Purcell, K.; Shulkes, A.; Kriketos, A.; Proietto, J. Long-term persistence of hormonal adaptations to weight loss. N. Engl. J. Med. 2011, 365, 1597–1604. [Google Scholar] [CrossRef]
- Casanova, N.; Beaulieu, K.; Finlayson, G.; Hopkins, M. Metabolic adaptations during negative energy balance and their potential impact on appetite and food intake. Proc. Nutr. Soc. 2019, 78, 279–289. [Google Scholar] [CrossRef]
- Carter, S.; Clifton, P.M.; Keogh, J.B. Effect of Intermittent Compared With Continuous Energy Restricted Diet on Glycemic Control in Patients With Type 2 Diabetes: A Randomized Noninferiority Trial. JAMA Netw. Open 2018, 1, e180756. [Google Scholar] [CrossRef]
- Gray, K.L.; Clifton, P.M.; Keogh, J.B. The effect of intermittent energy restriction on weight loss and diabetes risk markers in women with a history of gestational diabetes: A 12-month randomized control trial. Am. J. Clin. Nutr. 2021, 114, 794–803. [Google Scholar] [CrossRef]
- Headland, M.L.; Clifton, P.M.; Keogh, J.B. Effect of intermittent compared to continuous energy restriction on weight loss and weight maintenance after 12 months in healthy overweight or obese adults. Int. J. Obes. 2019, 43, 2028–2036. [Google Scholar] [CrossRef]
- Sundfor, T.M.; Svendsen, M.; Tonstad, S. Effect of intermittent versus continuous energy restriction on weight loss, maintenance and cardiometabolic risk: A randomized 1-year trial. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 698–706. [Google Scholar] [CrossRef]
- Trepanowski, J.F.; Kroeger, C.M.; Barnosky, A.; Klempel, M.C.; Bhutani, S.; Hoddy, K.K.; Gabel, K.; Freels, S.; Rigdon, J.; Rood, J.; et al. Effect of Alternate-Day Fasting on Weight Loss, Weight Maintenance, and Cardioprotection Among Metabolically Healthy Obese Adults: A Randomized Clinical Trial. JAMA Intern. Med. 2017, 177, 930–938. [Google Scholar] [CrossRef]
- Catenacci, V.A.; Ostendorf, D.M.; Pan, Z.; Kaizer, L.K.; Creasy, S.A.; Zaman, A.; Caldwell, A.E.; Dahle, J.; Swanson, B.; Breit, M.J.; et al. The Effect of 4:3 Intermittent Fasting on Weight Loss at 12 Months: A Randomized Clinical Trial. Ann. Intern. Med. 2025, 178, 634–644. [Google Scholar] [CrossRef]
- Grimm, E.R.; Steinle, N.I. Genetics of eating behavior: Established and emerging concepts. Nutr. Rev. 2011, 69, 52–60. [Google Scholar] [CrossRef]
- French, S.A.; Epstein, L.H.; Jeffery, R.W.; Blundell, J.E.; Wardle, J. Eating behavior dimensions. Associations with energy intake and body weight. A review. Appetite 2012, 59, 541–549. [Google Scholar] [CrossRef]
- Konttinen, H. Emotional eating and obesity in adults: The role of depression, sleep and genes. Proc. Nutr. Soc. 2020, 79, 283–289. [Google Scholar] [CrossRef]
- Vainik, U.; Garcia-Garcia, I.; Dagher, A. Uncontrolled eating: A unifying heritable trait linked with obesity, overeating, personality and the brain. Eur. J. Neurosci. 2019, 50, 2430–2445. [Google Scholar] [CrossRef]
- McCuen-Wurst, C.; Ruggieri, M.; Allison, K.C. Disordered eating and obesity: Associations between binge-eating disorder, night-eating syndrome, and weight-related comorbidities. Ann. N. Y. Acad. Sci. 2018, 1411, 96–105. [Google Scholar] [CrossRef]
- Polivy, J.; Herman, C.P. Dieting and binging. A causal analysis. Am. Psychol. 1985, 40, 193–201. [Google Scholar] [CrossRef]
- Howard, C.E.; Porzelius, L.K. The role of dieting in binge eating disorder: Etiology and treatment implications. Clin. Psychol. Rev. 1999, 19, 25–44. [Google Scholar] [CrossRef]
- Ban, K.F.; O’Connor, S.M. Do impulse control difficulties moderate the relationship between intermittent fasting and disordered eating? Eat. Behav. 2024, 55, 101926. [Google Scholar] [CrossRef]
- Colombarolli, M.S.; de Oliveira, J.; Cordas, T.A. Craving for carbs: Food craving and disordered eating in low-carb dieters and its association with intermittent fasting. Eat. Weight. Disord. 2022, 27, 3109–3117. [Google Scholar] [CrossRef]
- Ganson, K.T.; Cuccolo, K.; Hallward, L.; Nagata, J.M. Intermittent fasting: Describing engagement and associations with eating disorder behaviors and psychopathology among Canadian adolescents and young adults. Eat. Behav. 2022, 47, 101681. [Google Scholar] [CrossRef]
- Domaszewski, P.; Rogowska, A.M.; Zylak, K. Examining Associations Between Fasting Behavior, Orthorexia Nervosa, and Eating Disorders. Nutrients 2024, 16, 4275. [Google Scholar] [CrossRef]
- Hoddy, K.K.; Kroeger, C.M.; Trepanowski, J.F.; Barnosky, A.R.; Bhutani, S.; Varady, K.A. Safety of alternate day fasting and effect on disordered eating behaviors. Nutr. J. 2015, 14, 44. [Google Scholar] [CrossRef]
- Bhutani, S.; Klempel, M.C.; Kroeger, C.M.; Aggour, E.; Calvo, Y.; Trepanowski, J.F.; Hoddy, K.K.; Varady, K.A. Effect of exercising while fasting on eating behaviors and food intake. J. Int. Soc. Sports Nutr. 2013, 10, 50. [Google Scholar] [CrossRef]
- Kroeger, C.M.; Trepanowski, J.F.; Klempel, M.C.; Barnosky, A.; Bhutani, S.; Gabel, K.; Varady, K.A. Eating behavior traits of successful weight losers during 12 months of alternate-day fasting: An exploratory analysis of a randomized controlled trial. Nutr. Health 2018, 24, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Beaulieu, K.; Casanova, N.; Oustric, P.; Turicchi, J.; Gibbons, C.; Hopkins, M.; Varady, K.; Blundell, J.; Finlayson, G. Matched Weight Loss Through Intermittent or Continuous Energy Restriction Does Not Lead To Compensatory Increases in Appetite and Eating Behavior in a Randomized Controlled Trial in Women with Overweight and Obesity. J. Nutr. 2020, 150, 623–633. [Google Scholar] [CrossRef] [PubMed]
- Steger, F.L.; Jamshed, H.; Martin, C.K.; Richman, J.S.; Bryan, D.R.; Hanick, C.J.; Salvy, S.J.; Warriner, A.H.; Peterson, C.M. Impact of early time-restricted eating on diet quality, meal frequency, appetite, and eating behaviors: A randomized trial. Obesity 2023, 31 (Suppl. S1), 127–138. [Google Scholar] [CrossRef] [PubMed]
- Naleid, A.M.; Grace, M.K.; Cummings, D.E.; Levine, A.S. Ghrelin induces feeding in the mesolimbic reward pathway between the ventral tegmental area and the nucleus accumbens. Peptides 2005, 26, 2274–2279. [Google Scholar] [CrossRef]
- Tavakoli, A.; Bideshki, M.V.; Zamani, P.; Tavakoli, F.; Dehghan, P.; Gargari, B.P. The effectiveness of fasting regimens on serum levels of some major weight regulating hormones: A GRADE-assessed systematic review and meta-analysis in randomized controlled trial. J. Health Popul. Nutr. 2025, 44, 104. [Google Scholar] [CrossRef]
- Jin, Z.; Li, J.; Thackray, A.E.; Shen, T.; Deighton, K.; King, J.A.; Stensel, D.J. Fasting appetite-related gut hormone responses after weight loss induced by calorie restriction, exercise, or both in people with overweight or obesity: A meta-analysis. Int. J. Obes. 2025, 49, 776–792. [Google Scholar] [CrossRef]
- Varkaneh Kord, H.; Tinsley, G.M.; Santos, H.O.; Zand, H.; Nazary, A.; Fatahi, S.; Mokhtari, Z.; Salehi-Sahlabadi, A.; Tan, S.C.; Rahmani, J.; et al. The influence of fasting and energy-restricted diets on leptin and adiponectin levels in humans: A systematic review and meta-analysis. Clin. Nutr. 2021, 40, 1811–1821. [Google Scholar] [CrossRef]
- Mattson, M.P.; Moehl, K.; Ghena, N.; Schmaedick, M.; Cheng, A. Intermittent metabolic switching, neuroplasticity and brain health. Nat. Rev. Neurosci. 2018, 19, 63–80. [Google Scholar] [CrossRef]
- Sleiman, S.F.; Henry, J.; Al-Haddad, R.; El Hayek, L.; Abou Haidar, E.; Stringer, T.; Ulja, D.; Karuppagounder, S.S.; Holson, E.B.; Ratan, R.R.; et al. Exercise promotes the expression of brain derived neurotrophic factor (BDNF) through the action of the ketone body beta-hydroxybutyrate. eLife 2016, 5, e15092. [Google Scholar] [CrossRef]
- Alkurd, R.; Mahrous, L.; Zeb, F.; Khan, M.A.; Alhaj, H.; Khraiwesh, H.M.; Faris, M.E. Effect of Calorie Restriction and Intermittent Fasting Regimens on Brain-Derived Neurotrophic Factor Levels and Cognitive Function in Humans: A Systematic Review. Medicina 2024, 60, 191. [Google Scholar] [CrossRef]
- Ostendorf, D.M.; Caldwell, A.E.; Zaman, A.; Pan, Z.; Bing, K.; Wayland, L.T.; Creasy, S.A.; Bessesen, D.H.; MacLean, P.; Melanson, E.L.; et al. Comparison of weight loss induced by daily caloric restriction versus intermittent fasting (DRIFT) in individuals with obesity: Study protocol for a 52-week randomized clinical trial. Trials 2022, 23, 718. [Google Scholar] [CrossRef]
- Garner, D.M.; Olmsted, M.P.; Bohr, Y.; Garfinkel, P.E. The eating attitudes test: Psychometric features and clinical correlates. Psychol. Med. 1982, 12, 871–878. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Yanovski, S.; Wadden, T.; Wing, R.; Marcus, M.D.; Stunkard, A.; Devlin, M.; Mitchell, J.; Hasin, D.; Horne, R.L. Binge eating disorder: Its further validation in a multisite study. Int. J. Eat. Disord. 1993, 13, 137–153. [Google Scholar] [CrossRef] [PubMed]
- Human energy requirements: Report of a joint FAO/WHO/UNU Expert Consultation. Food Nutr. Bull. 2005, 26, 166.
- Peters, J.C.; Wyatt, H.R.; Foster, G.D.; Pan, Z.; Wojtanowski, A.C.; Vander Veur, S.S.; Herring, S.J.; Brill, C.; Hill, J.O. The effects of water and non-nutritive sweetened beverages on weight loss during a 12-week weight loss treatment program. Obesity 2014, 22, 1415–1421. [Google Scholar] [CrossRef] [PubMed]
- Wyatt, H.R.; Jortberg, B.T.; Babbel, C.; Garner, S.; Dong, F.; Grunwald, G.K.; Hill, J.O. Weight loss in a community initiative that promotes decreased energy intake and increased physical activity and dairy consumption: Calcium Weighs-In. J. Phys. Act. Health 2008, 5, 28–44. [Google Scholar] [CrossRef]
- Karlsson, J.; Persson, L.O.; Sjostrom, L.; Sullivan, M. Psychometric properties and factor structure of the Three-Factor Eating Questionnaire (TFEQ) in obese men and women. Results from the Swedish Obese Subjects (SOS) study. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1715–1725. [Google Scholar] [CrossRef]
- Gormally, J.; Black, S.; Daston, S.; Rardin, D. The assessment of binge eating severity among obese persons. Addict. Behav. 1982, 7, 47–55. [Google Scholar] [CrossRef]
- Mason, A.E.; Vainik, U.; Acree, M.; Tomiyama, A.J.; Dagher, A.; Epel, E.S.; Hecht, F.M. Improving Assessment of the Spectrum of Reward-Related Eating: The RED-13. Front. Psychol. 2017, 8, 795. [Google Scholar] [CrossRef] [PubMed]
- Fruhbeck, G.; Catalan, V.; Rodriguez, A.; Ramirez, B.; Becerril, S.; Salvador, J.; Colina, I.; Gomez-Ambrosi, J. Adiponectin-leptin Ratio is a Functional Biomarker of Adipose Tissue Inflammation. Nutrients 2019, 11, 454. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.O. Understanding and addressing the epidemic of obesity: An energy balance perspective. Endocr. Rev. 2006, 27, 750–761. [Google Scholar] [CrossRef] [PubMed]
- Stewart, T.M.; Williamson, D.A.; White, M.A. Rigid vs. flexible dieting: Association with eating disorder symptoms in nonobese women. Appetite 2002, 38, 39–44. [Google Scholar] [CrossRef]
- Tomiyama, A.J.; Mann, T.; Vinas, D.; Hunger, J.M.; Dejager, J.; Taylor, S.E. Low calorie dieting increases cortisol. Psychosom. Med. 2010, 72, 357–364. [Google Scholar] [CrossRef]
- Blumberg, J.; Hahn, S.L.; Bakke, J. Intermittent fasting: Consider the risks of disordered eating for your patient. Clin. Diabetes Endocrinol. 2023, 9, 4. [Google Scholar] [CrossRef]
- Schueler, J.; Philip, S.R.; Vitus, D.; Engler, S.; Fields, S.A. Group differences in binge eating, impulsivity, and intuitive and mindful eating among intermittent fasters and non-fasters. Appetite 2023, 182, 106416. [Google Scholar] [CrossRef]
- Cuccolo, K.; Kramer, R.; Petros, T.; Thoennes, M. Intermittent fasting implementation and association with eating disorder symptomatology. Eat. Disord. 2022, 30, 471–491. [Google Scholar] [CrossRef]
- Sundfor, T.M.; Tonstad, S.; Svendsen, M. Effects of intermittent versus continuous energy restriction for weight loss on diet quality and eating behavior. A randomized trial. Eur. J. Clin. Nutr. 2019, 73, 1006–1014. [Google Scholar] [CrossRef]
- Keranen, A.M.; Savolainen, M.J.; Reponen, A.H.; Kujari, M.L.; Lindeman, S.M.; Bloigu, R.S.; Laitinen, J.H. The effect of eating behavior on weight loss and maintenance during a lifestyle intervention. Prev. Med. 2009, 49, 32–38. [Google Scholar] [CrossRef]
- James, B.L.; Roe, L.S.; Loken, E.; Rolls, B.J. Early predictors of weight loss in a 1-year behavioural weight-loss programme. Obes. Sci. Pract. 2018, 4, 20–28. [Google Scholar] [CrossRef]
- Westerterp-Plantenga, M.S.; Kempen, K.P.; Saris, W.H. Determinants of weight maintenance in women after diet-induced weight reduction. Int. J. Obes. Relat. Metab. Disord. 1998, 22, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Hutchinson, E. Systems neuroscience: The stress of dieting. Nat. Rev. Neurosci. 2011, 12, 65. [Google Scholar] [CrossRef] [PubMed]
- Goldstone, A.P.; Prechtl de Hernandez, C.G.; Beaver, J.D.; Muhammed, K.; Croese, C.; Bell, G.; Durighel, G.; Hughes, E.; Waldman, A.D.; Frost, G.; et al. Fasting biases brain reward systems towards high-calorie foods. Eur. J. Neurosci. 2009, 30, 1625–1635. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Wu, X.; Gao, H.; Xiang, T.; Zhou, J.; Zou, Z.; Tong, L.; Yan, B.; Zhang, C.; Wang, L.; et al. Intermittent energy restriction changes the regional homogeneity of the obese human brain. Front. Neurosci. 2023, 17, 1201169. [Google Scholar] [CrossRef]
- Hoddy, K.K.; Gibbons, C.; Kroeger, C.M.; Trepanowski, J.F.; Barnosky, A.; Bhutani, S.; Gabel, K.; Finlayson, G.; Varady, K.A. Changes in hunger and fullness in relation to gut peptides before and after 8 weeks of alternate day fasting. Clin. Nutr. 2016, 35, 1380–1385. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Characteristic | 4:3 IMF (n = 84) | DCR (n = 81) |
|---|---|---|
| Age, years | 42 (10) | 42 (8) |
| Sex | ||
| Female | 73.8% | 74.1% |
| Male | 26.2% | 25.9% |
| Race (%) | ||
| White | 85.7% | 86.4% |
| Asian | 7.1% | 2.5% |
| Black | 6.0% | 6.2% |
| Other | 1.2% | 4.9% |
| Ethnicity (%) | ||
| Hispanic or Latino | 17.9% | 29.6% |
| Not Hispanic or Latino | 82.1% | 70.4% |
| Body Composition | ||
| BMI, kg/m2 | 34.3 (4.4) | 33.9 (4.4) |
| Weight, kg | 99.2 (16.0) | 95.5 (16.0) |
| Total Body Fat Mass (%) | 40.6 (7.8) | 41.1 (7.2) |
| Eating Behaviors (95% CI) | ||
| BES Score | 11.7 (10.4 to 13.1) | 12.7 (11.4 to 14.1) |
| TFEQ-R18 Subscale Scores | ||
| Uncontrolled Eating | 37.1 (33.6 to 40.6) | 37.6 (34.1 to 41.2) |
| Emotional Eating | 52.5 (46.3 to 58.8) | 55.6 (49.2 to 61.9) |
| Cognitive Restraint | 43.5 (40.2 to 46.8) | 42.5 (39.1 to 45.8) |
| RED-13 Score | 18.9 (17.1 to 20.8) | 20.6 (18.8 to 22.5) |
| Appetite Hormones (95% CI) | ||
| Leptin (ng/mL) | 68.3 (59.7 to 76.9) | 67.7 (58.9 to 76.5) |
| Ghrelin (pg/mL) | 788.0 (721.5 to 854.4) | 795.5 (727.8 to 863.2) |
| PYY (pg/mL) | 97.2 (89.5 to 104.9) | 95.8 (87.9 to 103.6) |
| BDNF (ng/mL) | 17.4 (15.7 to 19.1) | 16.0 (14.3 to 17.8) |
| Adiponectin (µg/mL) | 8.2 (7.1 to 9.2) | 9.8 (8.7 to 10.9) |
| Adiponectin (µg/mL)/Leptin (ng/mL) Ratio | 0.18 (0.14 to 0.22) | 0.23 (0.18 to 0.27) |
| Characteristic | 4:3 IMF | DCR | ||||||
|---|---|---|---|---|---|---|---|---|
| M0 | M3 | M6 | M12 | M0 | M3 | M6 | M12 | |
| Eating Behaviors | ||||||||
| BES | 84 | 78 | 72 | 68 | 81 | 74 | 65 | 53 |
| TFEQ-R18 | 83 | 76 | 71 | 68 | 81 | 74 | 65 | 52 |
| RED-13 | 84 | 78 | 72 | 68 | 81 | 73 | 65 | 53 |
| Appetite Hormones | ||||||||
| Leptin | 83 | 66 | 65 | 79 | 56 | 52 | ||
| Ghrelin | 83 | 66 | 65 | 80 | 57 | 52 | ||
| PYY | 83 | 66 | 65 | 80 | 57 | 52 | ||
| BDNF | 82 | 66 | 65 | 78 | 57 | 52 | ||
| Adiponectin | 78 | 66 | 65 | 70 | 57 | 52 | ||
| Variable | Month | 4:3 IMF | Change from Baseline in 4:3 IMF | DCR | Change from Baseline in DCR | Difference in Change from Baseline Between Groups | Main Effects and Interaction |
|---|---|---|---|---|---|---|---|
| Leptin (ng/mL) | 0 | 68.3 (59.7 to 76.9) | 67.7 (58.9 to 76.5) | T: <0.01 | |||
| 6 | 43.4 (36.4 to 50.5) | −24.9 (−31.9 to −17.8) | 45.6 (38.2 to 53.0) | −22.1 (−29.5 to −14.7) | 2.8 (−7.5 to 13.0) | G: 0.71 | |
| 12 | 47.5 (40.1 to 54.9) | −20.8 (−27.5 to −14.1) | 51.5 (43.6 to 59.3) | −16.2 (−23.4 to −9.6) | 4.6 (−5.2 to 14.4) | GxT: 0.63 | |
| Ghrelin (pg/mL) | 0 | 788.0 (721.5 to 854.4) | 795.5 (727.8 to 863.2) | T: <0.01 | |||
| 6 | 902.2 (823.1 to 981.3) | 114.2 (59.2 to 169.3) | 872.4 (790.0 to 954.7) | 76.8 (18.2 to 135.4) | −37.4 (−117.8 to 43.0) | G: 0.71 | |
| 12 | 921.7 (839.0 to 1004.4) | 133.7 (81.6 to 185.8) | 886.6 (799.3 to 973.9) | 91.1 (33.3 to 148.9) | −42.7 (−120.5 to 35.2) | GxT: 0.53 | |
| PYY (pg/mL) | 0 | 97.2 (89.5 to 104.9) | 95.8 (87.9 to 103.6) | T: 0.31 | |||
| 6 | 92.9 (86.5 to 99.3) | −4.3 (−12.0 to 3.3) | 92.1 (85.4 to 98.9) | −3.6 (−11.6 to 4.4) | 0.7 (−10.4 to 11.8) | G: 0.70 | |
| 12 | 97.1 (89.7 to 104.6) | −0.1 (−8.3 to 8.2) | 94.5 (86.2 to 102.8) | −1.3 (−10.3 to 7.8) | −1.2 (−13.5 to 11.0) | GxT: 0.95 | |
| BDNF (ng/mL) | 0 | 17.4 (15.7 to 19.1) | 16.0 (14.3 to 17.8) | T: 0.14 | |||
| 6 | 14.7 (12.9 to 16.6) | −2.7 (−5.0 to 0.4) | 15.5 (13.5 to 17.4) | −0.5 (−3.0 to 1.9) | 2.1 (−1.2 to 5.5) | G: 0.78 | |
| 12 | 15.4 (13.6 to 17.2) | −2.0 (−4.4 to 0.4) | 15.4 (13.4 to 17.4) | −0.6 (−3.2 to 2.0) | 1.4 (−2.1 to 4.9) | GxT: 0.44 | |
| Adiponectin (μg/mL) | 0 | 8.2 (7.1 to 9.2) | 9.8 (8.7 to 10.9) | T: <0.01 | |||
| 6 | 8.6 (7.5 to 9.6) | 0.4 (−0.2 to 1.0) | 10.3 (9.2 to 11.4) | 0.6 (−0.1 to 1.2) | 0.2 (−0.7 to 1.1) | G: <0.05 | |
| 12 | 10.2 (8.9 to 11.4) | 2.0 (1.3 to 2.7) | 11.6 (10.3 to 12.9) | 1.8 (1.0 to 2.6) | −0.2 (−1.3 to 0.9) | GxT: 0.74 | |
| Adiponectin/ Leptin Ratio | 0 | 0.18 (0.14 to 0.22) | 0.23 (0.18 to 0.27) | T: <0.01 | |||
| 6 | 0.49 (0.31 to 0.67) | 0.31 (0.15 to 0.48) | 0.45 (0.26 to 0.64) | 0.22 (0.05 to 0.40) | −0.09 (−0.33 to 0.15 | G: 0.80 | |
| 12 | 0.49 (0.34 to 0.64) | 0.31 (0.18 to 0.44) | 0.42 (0.27 to 0.58) | 0.20 (0.05 to 0.34) | −0.11 (−0.31 to 0.08) | GxT: 0.54 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Breit, M.J.; Caldwell, A.E.; Ostendorf, D.M.; Pan, Z.; Creasy, S.A.; Swanson, B.; Clark, K.; Hill, E.B.; MacLean, P.S.; Bessesen, D.H.; et al. Effects of 4:3 Intermittent Fasting on Eating Behaviors and Appetite Hormones: A Secondary Analysis of a 12-Month Behavioral Weight Loss Intervention. Nutrients 2025, 17, 2385. https://doi.org/10.3390/nu17142385
Breit MJ, Caldwell AE, Ostendorf DM, Pan Z, Creasy SA, Swanson B, Clark K, Hill EB, MacLean PS, Bessesen DH, et al. Effects of 4:3 Intermittent Fasting on Eating Behaviors and Appetite Hormones: A Secondary Analysis of a 12-Month Behavioral Weight Loss Intervention. Nutrients. 2025; 17(14):2385. https://doi.org/10.3390/nu17142385
Chicago/Turabian StyleBreit, Matthew J., Ann E. Caldwell, Danielle M. Ostendorf, Zhaoxing Pan, Seth A. Creasy, Bryan Swanson, Kevin Clark, Emily B. Hill, Paul S. MacLean, Daniel H. Bessesen, and et al. 2025. "Effects of 4:3 Intermittent Fasting on Eating Behaviors and Appetite Hormones: A Secondary Analysis of a 12-Month Behavioral Weight Loss Intervention" Nutrients 17, no. 14: 2385. https://doi.org/10.3390/nu17142385
APA StyleBreit, M. J., Caldwell, A. E., Ostendorf, D. M., Pan, Z., Creasy, S. A., Swanson, B., Clark, K., Hill, E. B., MacLean, P. S., Bessesen, D. H., Melanson, E. L., & Catenacci, V. A. (2025). Effects of 4:3 Intermittent Fasting on Eating Behaviors and Appetite Hormones: A Secondary Analysis of a 12-Month Behavioral Weight Loss Intervention. Nutrients, 17(14), 2385. https://doi.org/10.3390/nu17142385