
Acceptability of a Colorectal Cancer-Preventive Diet Promoting Red Meat Reduction and Increased Fiber and Micronutrient Intake: A Cross-Sectional Study in Romanian Adults

 , , , ,
, , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
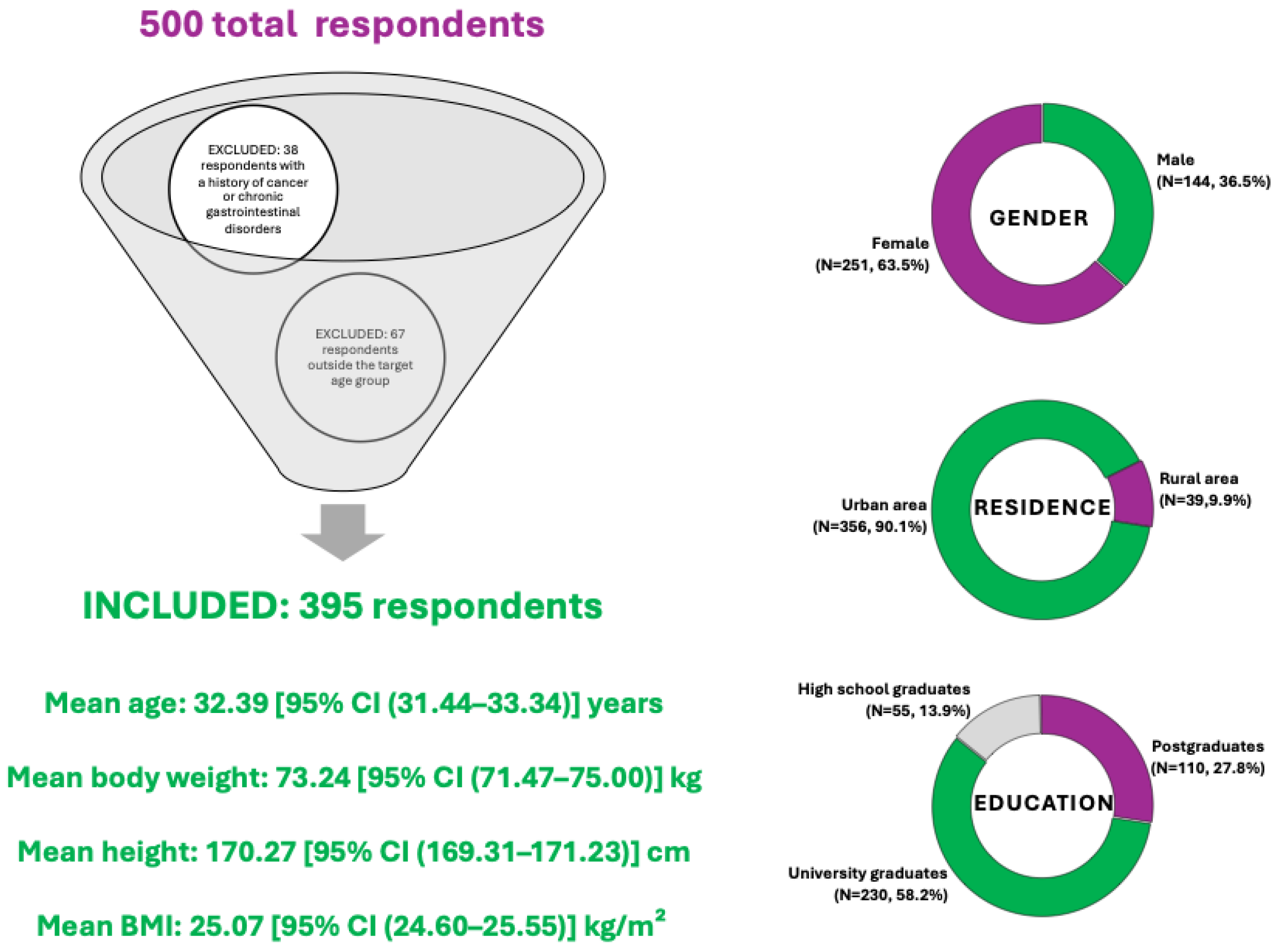
2.2. Sampling Method and Participant Selection
2.2.1. Inclusion Criteria
- Adults aged over 18 years old.
2.2.2. Exclusion Criteria
- Individuals younger than 18 or older than 50 years;
- History of cancer or chronic gastrointestinal disorders.
2.3. Questionnaire Description
- Sociodemographic data, including age, sex, education level, and area of residence;
- Dietary habits and perceptions, assessing the frequency of consumption of various food groups (red meat);
- Acceptability of the proposed dietary model, evaluated using a series of Likert-scale questions (1–5) covering perceived attractiveness, feasibility, compatibility with personal lifestyle, cost implications, and intention to adopt. Adjacently, open-ended questions were included to allow participants to share observations or suggestions regarding the menu (data not included).
2.4. Statistical Analysis
2.5. Ethics and Consent
3. Results
3.1. Dietary Model
3.2. Sample Size Estimation for the Validity of the Questionaire
3.3. Diet Acceptability Questionaire Analysis
3.3.1. Respondent Demographics
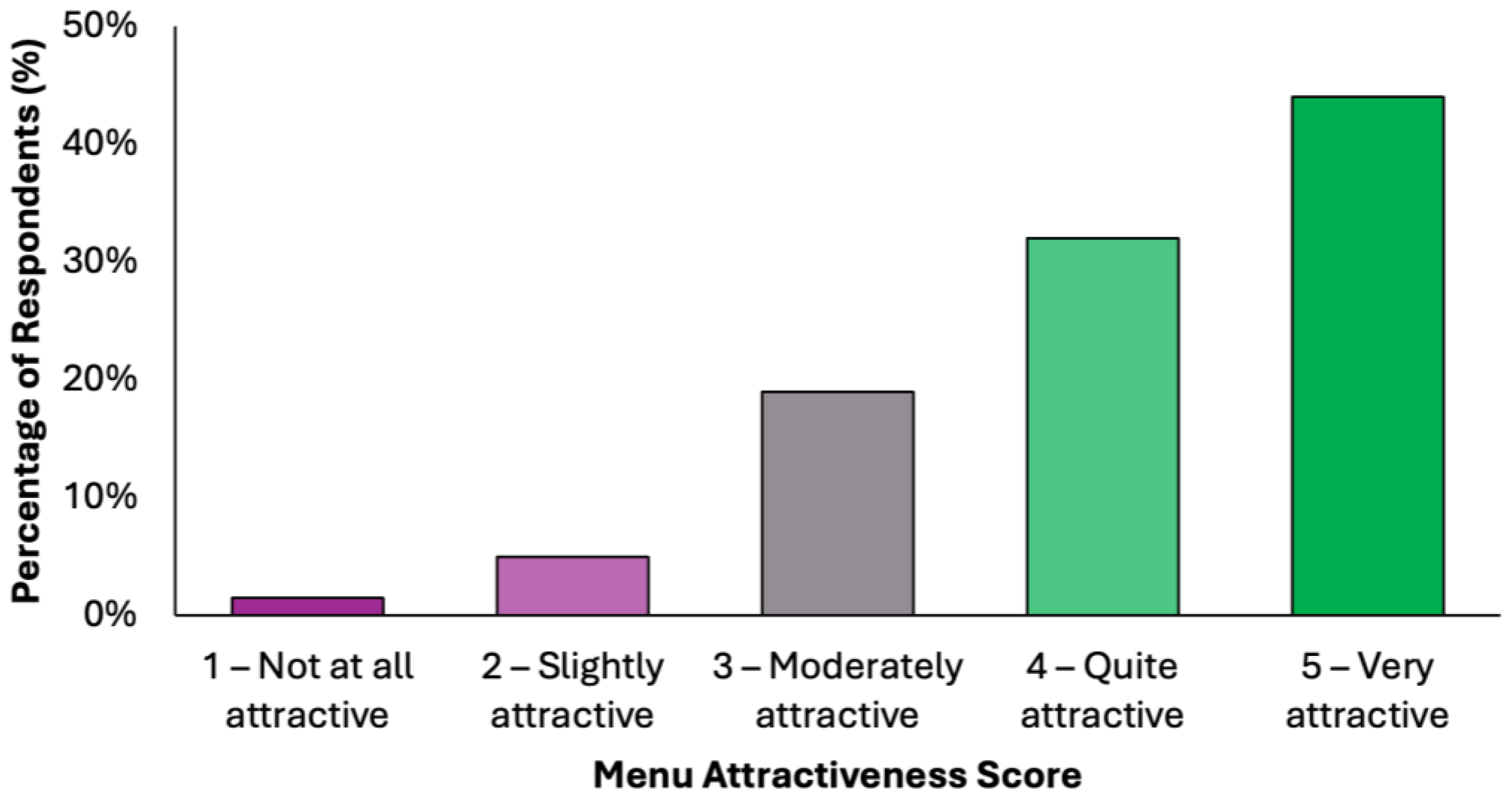
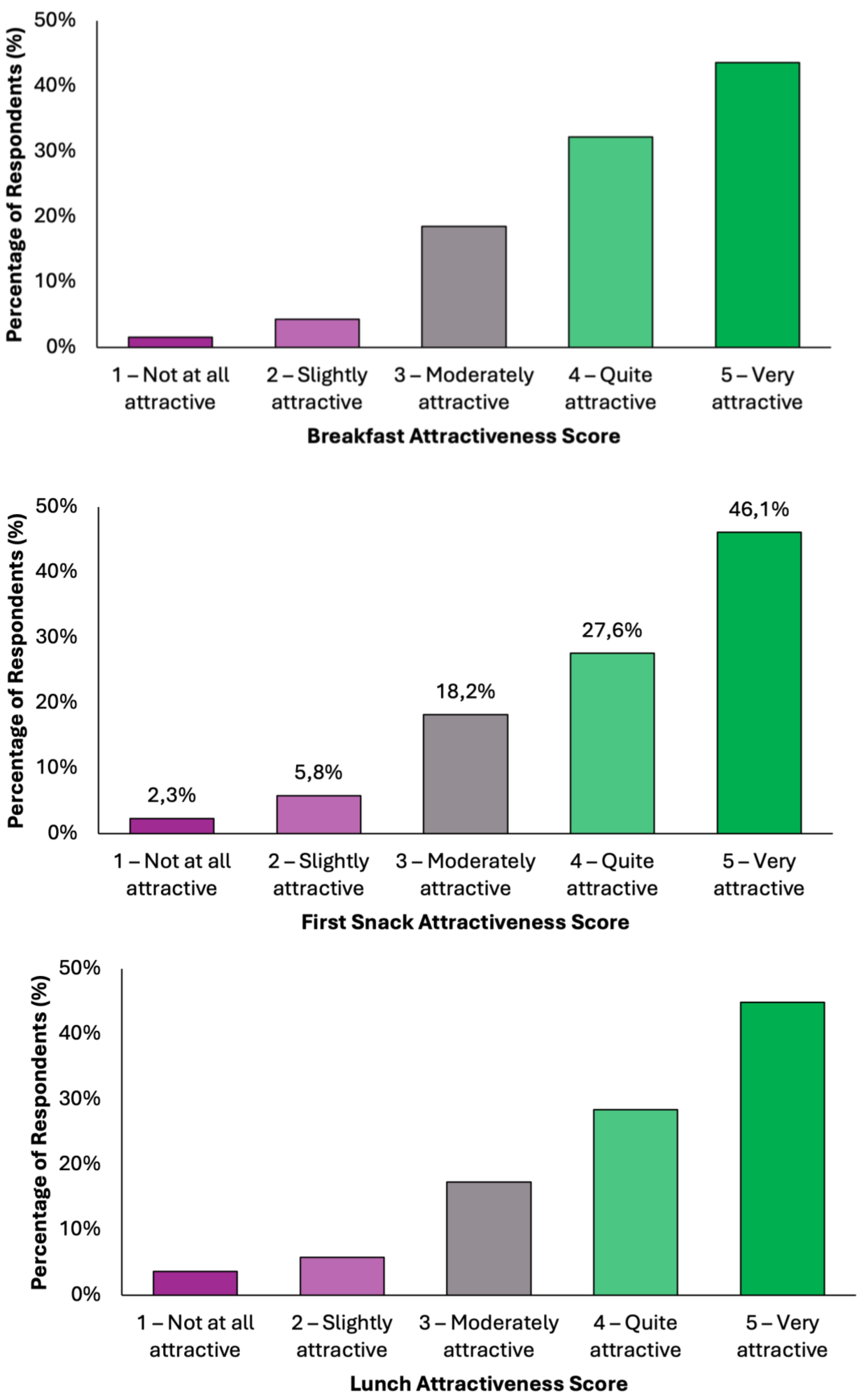
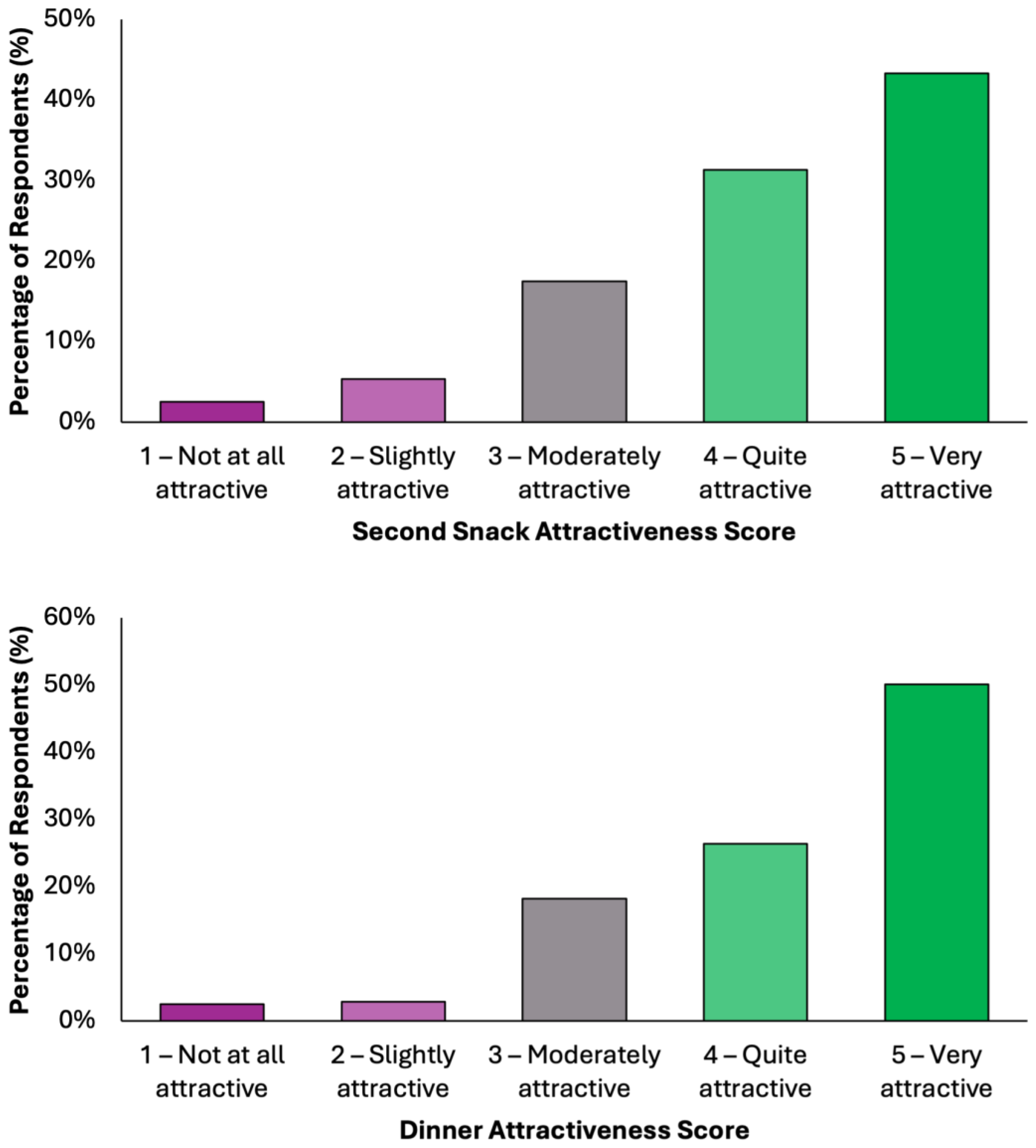
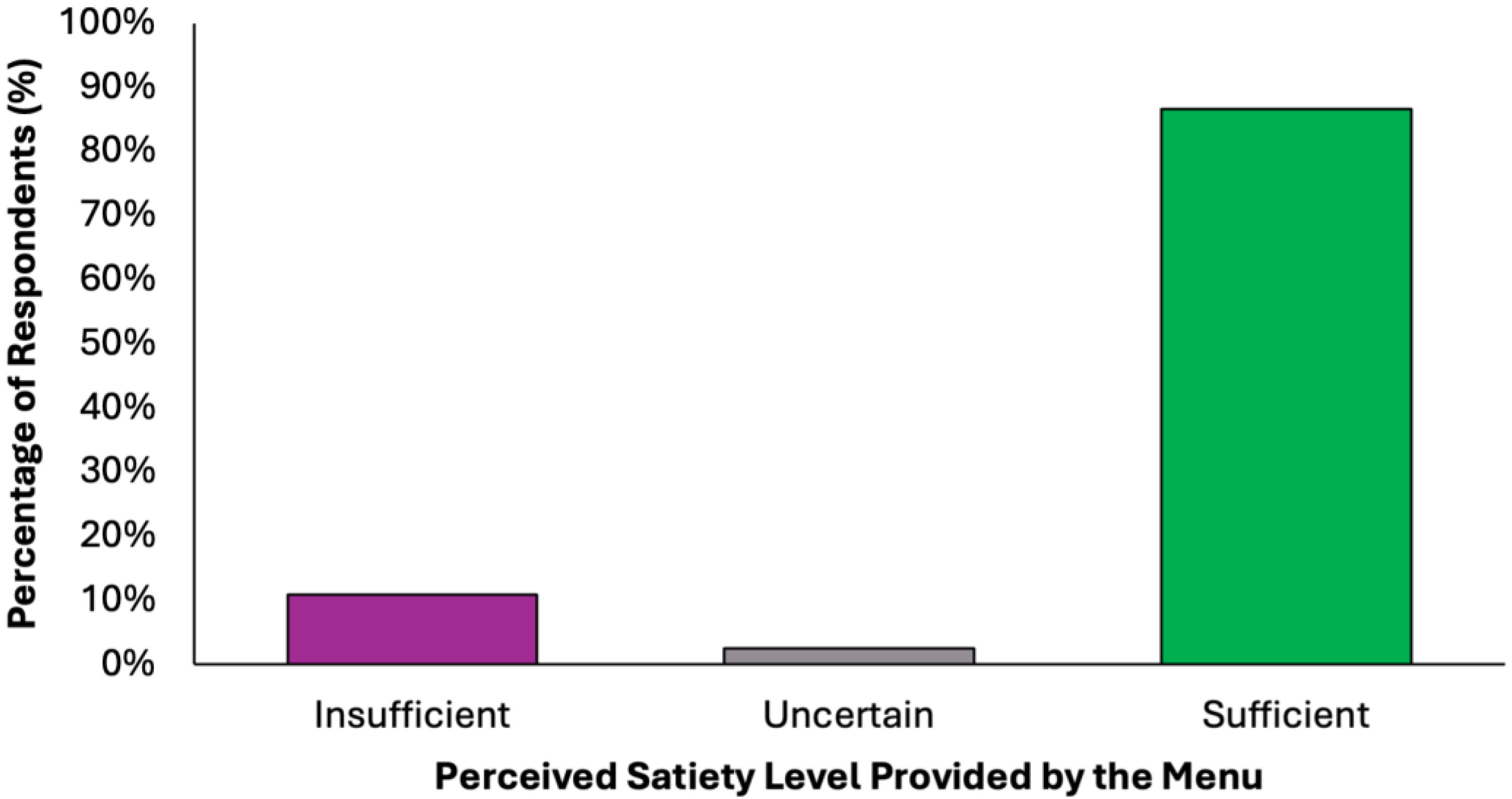
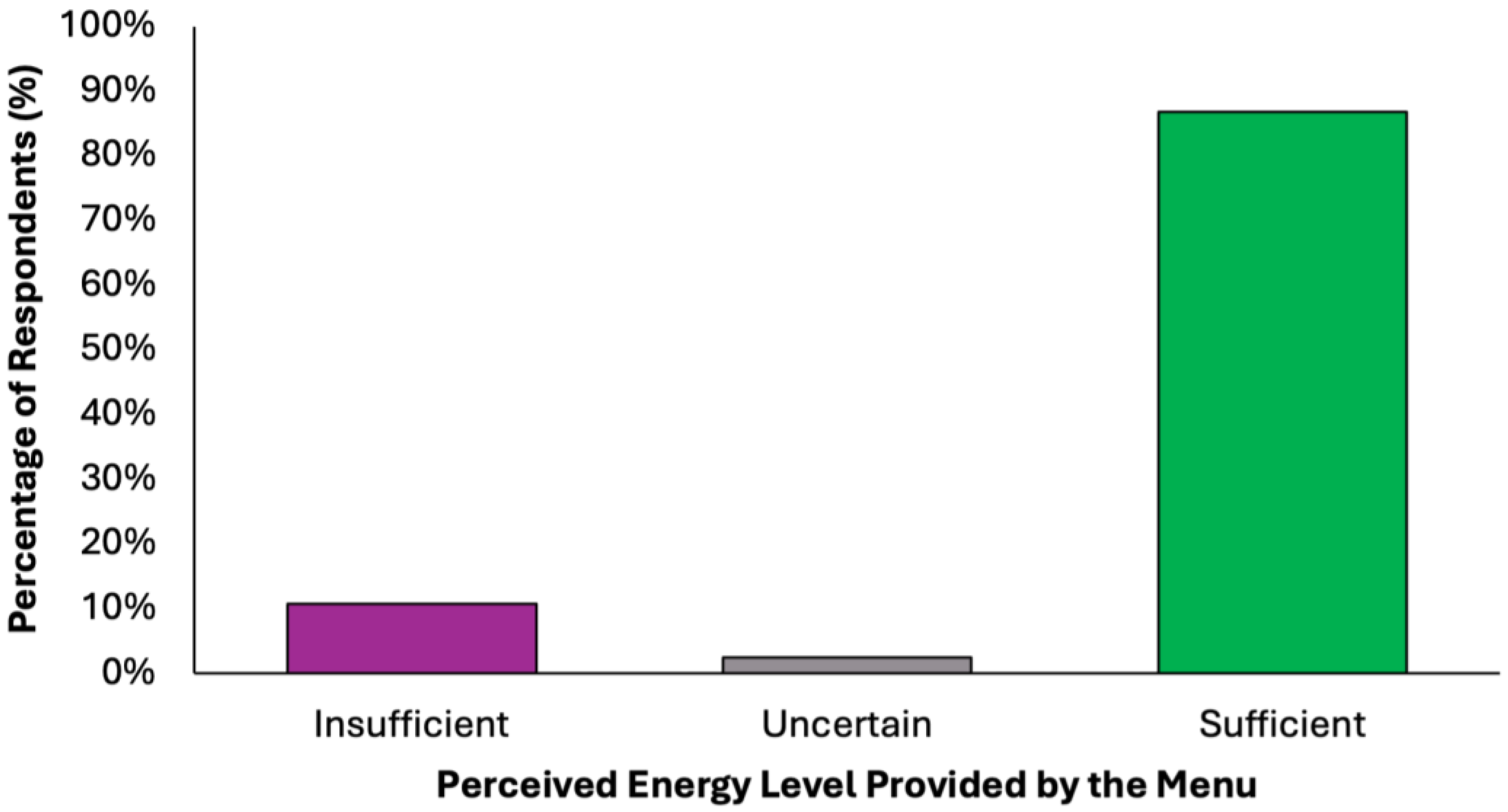
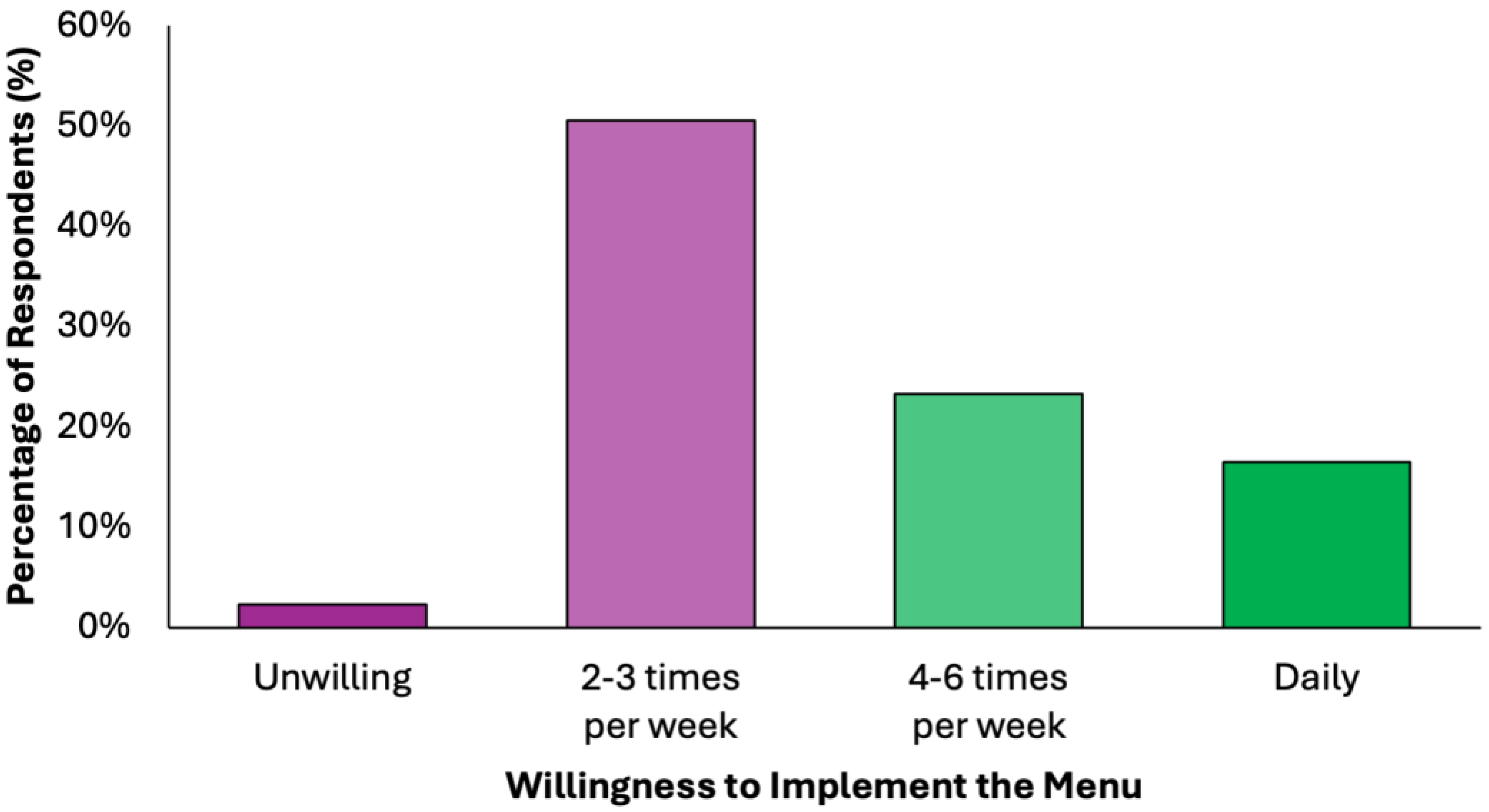
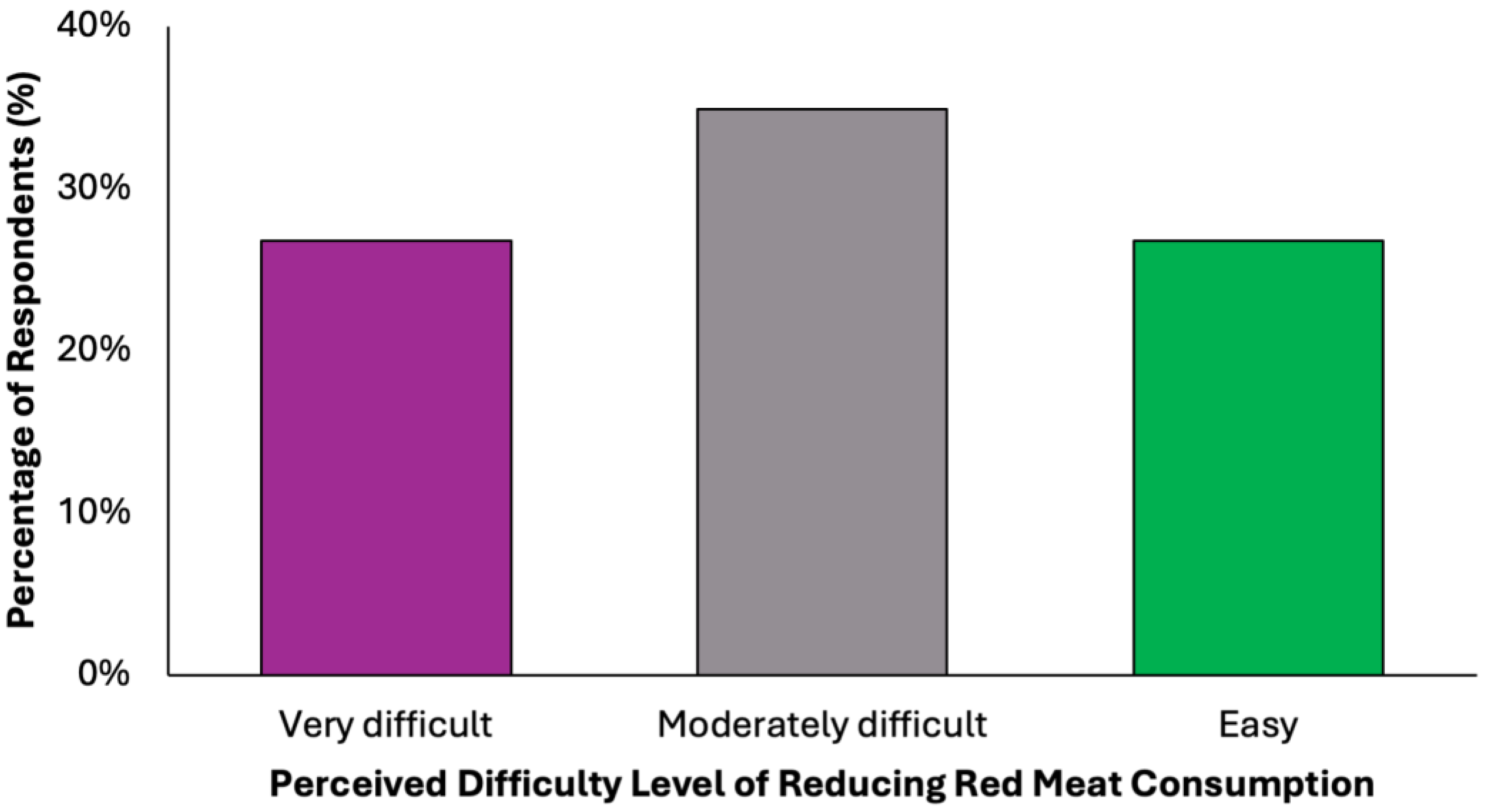
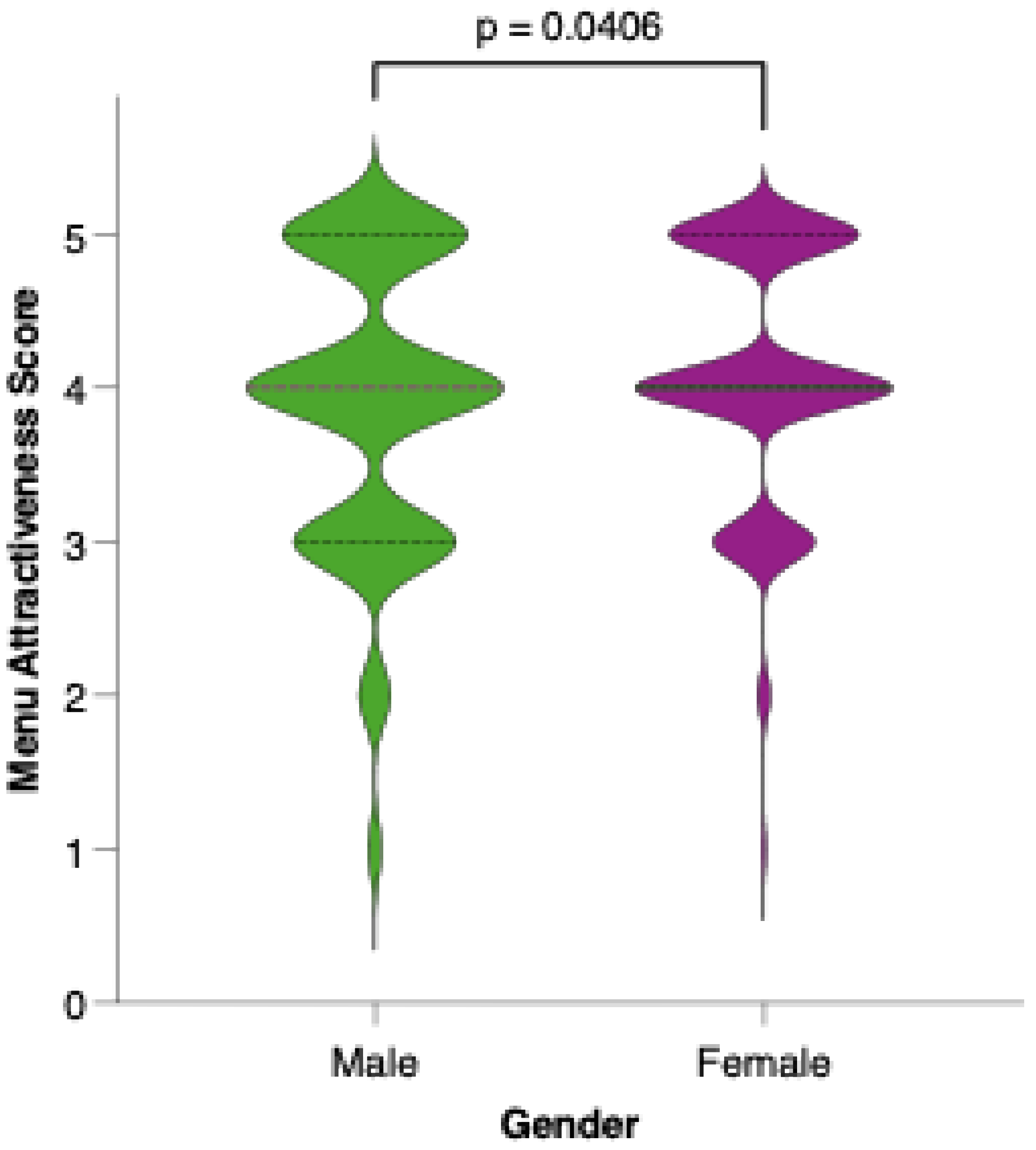
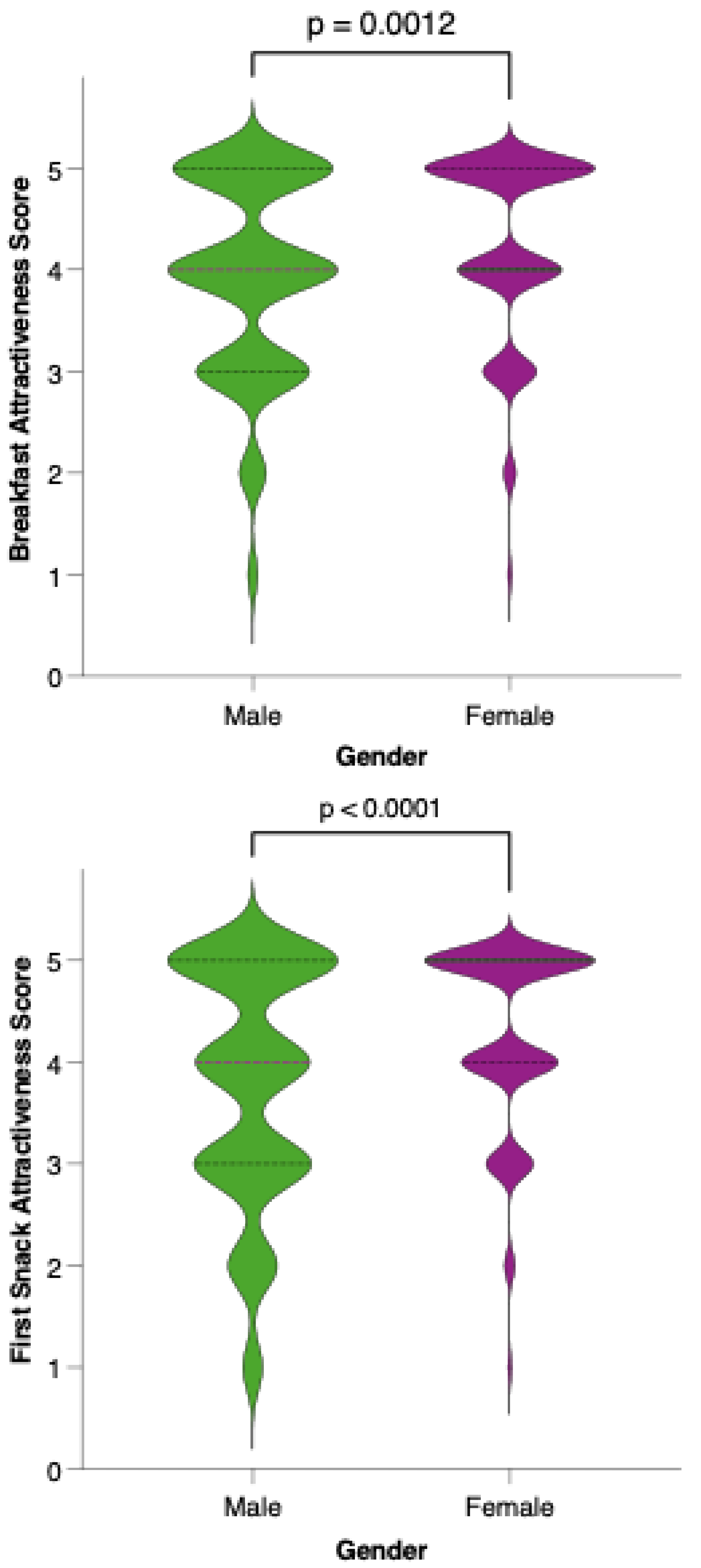
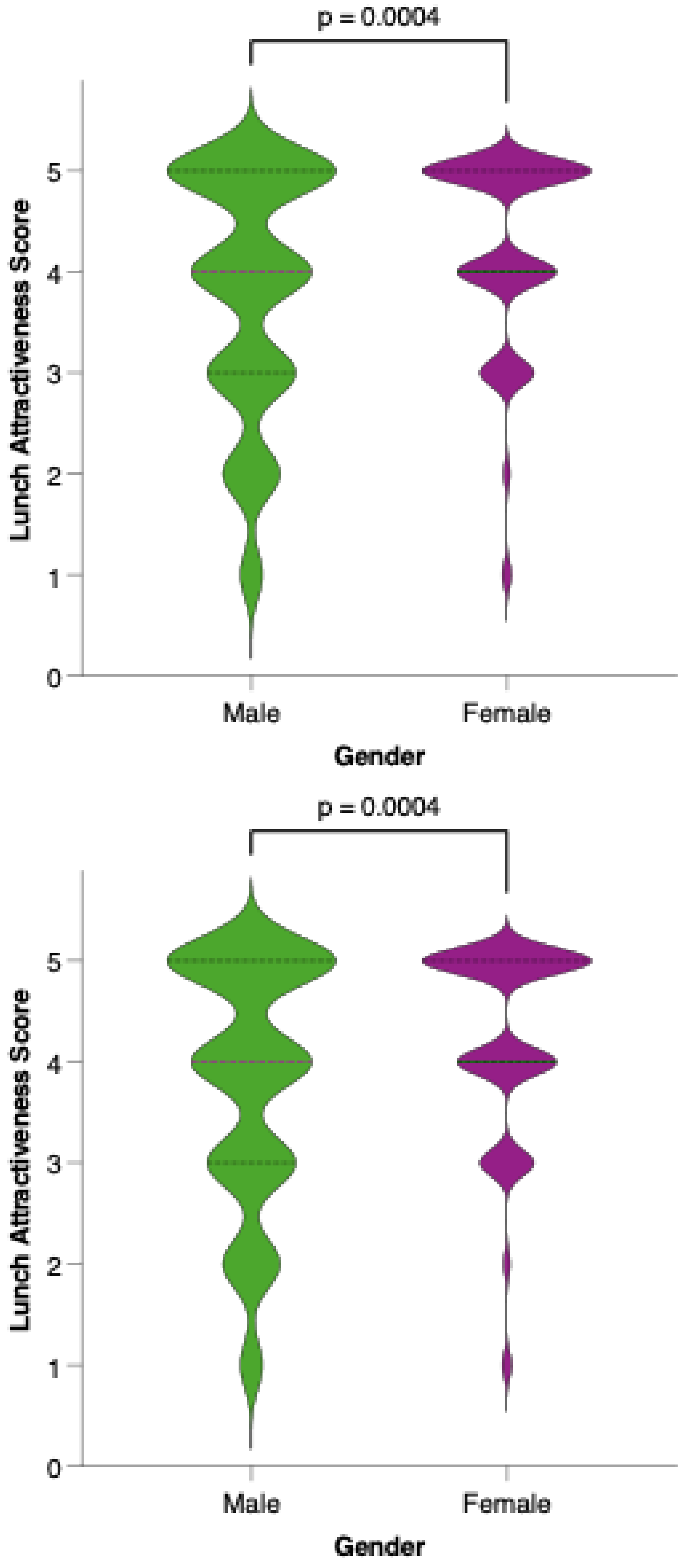
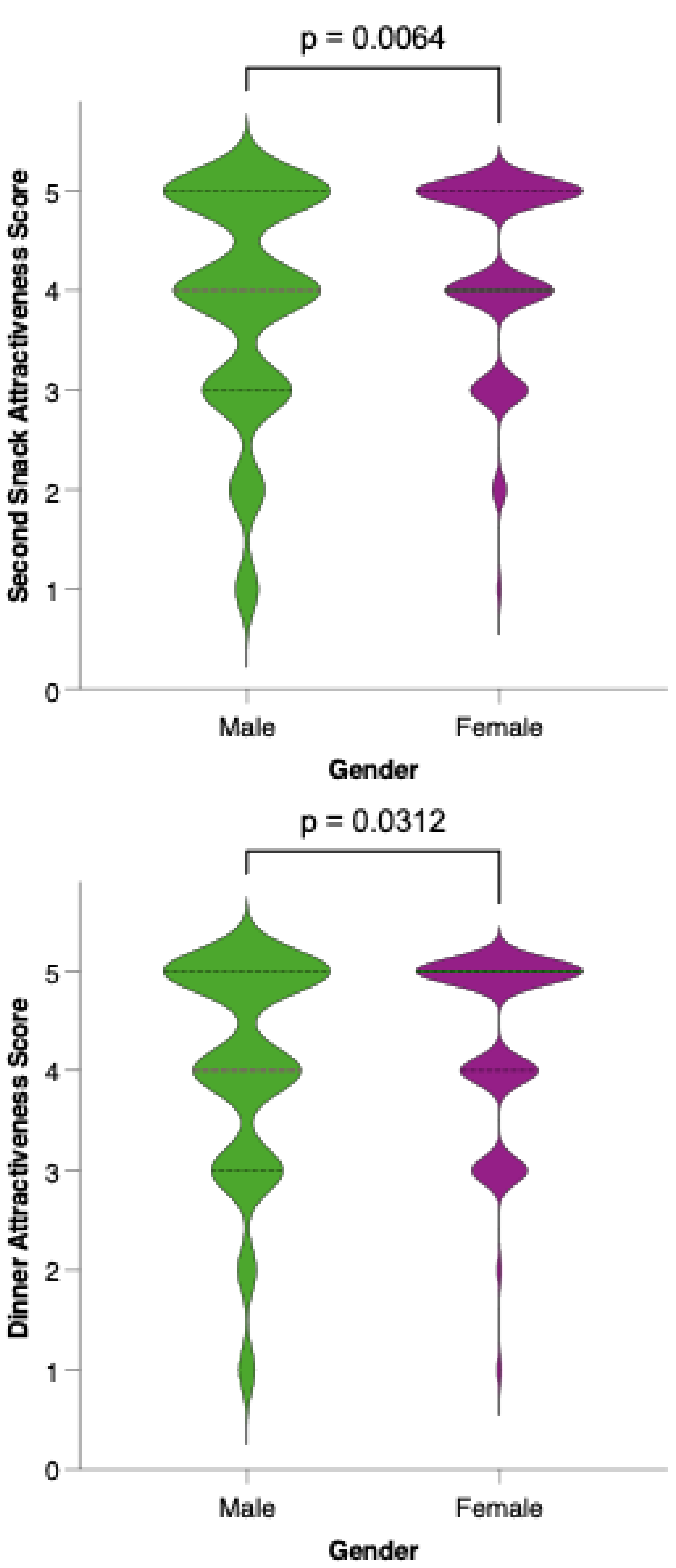
3.3.2. Menu Acceptability Among Respondents
3.4. Factors Influencing Diet Acceptability
4. Discussion
4.1. Dietary Model
4.2. Diet Acceptability
4.3. Limitations
4.4. Implications for Practice and Policy
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- American Cancer Society. Cancer Prevention & Early Detection: Facts & Figures 2025–2026; American Cancer Society: Atlanta, GA, USA, 2025. [Google Scholar]
- Morgan, E.; Arnold, M.; Gini, A.; Lorenzoni, V.; Cabasag, C.J.; Laversanne, M.; Vignat, J.; Ferlay, J.; Murphy, N.; Bray, F. Global burden of colorectal cancer in 2020 and 2040: Incidence and mortality estimates from GLOBOCAN. Gut 2023, 72, 338–344. [Google Scholar] [CrossRef]
- Carroll, K.L.; Frugé, A.D.; Heslin, M.J.; Lipke, E.A.; Greene, M.W. Diet as a Risk Factor for Early-Onset Colorectal Adenoma and Carcinoma: A Systematic Review. Front. Nutr. 2022, 9, 896330. [Google Scholar] [CrossRef]
- Pan, H.; Tang, Y.; Zhu, H.; Sun, Y.; Chi, P.; Huang, Y. Global burden, trends, and risk factors of early-onset and late-onset colorectal cancer from 1990 to 2021, with projections to 2040: A population-based study. BMC Gastroenterol. 2025, 25, 486. [Google Scholar] [CrossRef] [PubMed]
- Fardet, A.; Druesne-Pecollo, N.; Touvier, M.; Latino-Martel, P. Do alcoholic beverages, obesity and other nutritional factors modify the risk of familial colorectal cancer? A systematic review. Crit. Rev. Oncol. Hematol. 2017, 119, 94–112. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Xia, R.; Si, W.; Zhang, W.; Zhang, Y.; Zhuang, G. Cost Effectiveness of Colorectal Cancer Screening Strategies in Middle- and High-Income Countries: A Systematic Review. J. Gastroenterol. Hepatol. 2025, 40, 584–598. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Colorectal Cancer Collaborators. Global, regional, and national burden of colorectal cancer and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Gastroenterol. Hepatol. 2022, 7, 627–647. [Google Scholar] [CrossRef]
- Unger-Saldaña, K.; Saldaña-Tellez, M.; Potter, M.B.; Van Loon, K.; Allen-Leigh, B.; Lajous, M. Barriers and facilitators for colorectal cancer screening in a low-income urban community in Mexico City. Implement. Sci. Commun. 2020, 1, 64. [Google Scholar] [CrossRef]
- Desai, M.S.; Seekatz, A.M.; Koropatkin, N.M.; Kamada, N.; Hickey, C.A.; Wolter, M.; Pudlo, N.A.; Kitamoto, S.; Terrapon, N.; Muller, A.; et al. A dietary fiber-deprived gut microbiota degrades the colonic mucus barrier and enhances pathogen susceptibility. Cell 2016, 167, 1339–1353.e21. [Google Scholar] [CrossRef]
- Lazăr, D.-C.; Chiriac, S.-D.; Drăghici, G.-A.; Moacă, E.-A.; Faur, A.C.; Avram, M.-F.; Turi, V.-R.; Nicolin, M.-R.; Goldiș, A.; Salehi, M.A.; et al. Gastric Cancer and Microbiota: Exploring the Microbiome’s Role in Carcinogenesis and Treatment Strategies. Life 2025, 15, 999. [Google Scholar] [CrossRef]
- Howell, M.C.; Green, R.; McGill, A.R.; Dutta, R.; Mohapatra, S.; Mohapatra, S.S. SARS-CoV-2-Induced Gut Microbiome Dysbiosis: Implications for Colorectal Cancer. Cancers 2021, 13, 2676. [Google Scholar] [CrossRef]
- Cristian, M.; Așchie, M.; Deacu, M.; Boșoteanu, M.; Bălțătescu, G.I.; Stoica, A.G.; Nicolau, A.A.; Poinăreanu, I.; Orășanu, C.I. Comparison of Ki67 Proliferation Index in Gastrointestinal Non-Hodgkin Large B-Cell Lymphomas: The Conventional Method of Evaluation or AI Evaluation? Diagnostics 2023, 13, 2775. [Google Scholar] [CrossRef]
- Markozannes, G.; Cividini, S.; Aune, D.; Becerra-Tomás, N.; Kiss, S.; Balducci, K.; Vieira, R.; Cariolou, M.; Jayedi, A.; Greenwood, D.C.; et al. The role of physical activity, sedentary behaviour, diet, adiposity and body composition on health-related quality of life and cancer-related fatigue after diagnosis of colorectal cancer: A Global Cancer Update Programme (CUP Global) systematic literature review and meta-analysis. ESMO Open 2025, 10, 104301. [Google Scholar] [CrossRef]
- Huang, Y.; Cao, D.; Chen, Z.; Chen, B.; Li, J.; Guo, J.; Dong, Q.; Liu, L.; Wei, Q. Red and processed meat consumption and cancer outcomes: Umbrella review. Food Chem. 2021, 356, 129697. [Google Scholar] [CrossRef] [PubMed]
- Farvid, M.S.; Sidahmed, E.; Spence, N.D.; Mante Angua, K.; Rosner, B.A.; Barnett, J.B. Consumption of red meat and processed meat and cancer incidence: A systematic review and meta-analysis of prospective studies. Eur. J. Epidemiol. 2021, 36, 937–951. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.; Deka, D.; Kondaveeti, S.B.; Ayyadurai, P.; Siripragada, S.; Philip, N.; Pathak, S.; Duttaroy, A.K.; Banerjee, A. An overview of potential of natural compounds to regulate epigenetic modifications in colorectal cancer: A recent update. Epigenetics 2025, 20, 2491316. [Google Scholar] [CrossRef]
- Goldbaum, A.A.; Bowers, L.W.; Cox, A.D.; Gillig, M.; Clapp Organski, A.; Cross, T.W.L. The Role of Diet and the Gut Microbiota in the Obesity-Colorectal Cancer Link. Nutr. Cancer 2025, 77, 626–639. [Google Scholar] [CrossRef]
- Parada Venegas, D.; De la Fuente, M.K.; Landskron, G.; González, M.J.; Quera, R.; Dijkstra, G.; Harmsen, H.J.M.; Faber, K.N.; Hermoso, M.A. Short Chain Fatty Acids (SCFAs)-Mediated Gut Epithelial and Immune Regulation and Its Relevance for Inflammatory Bowel Diseases. Front. Immunol. 2019, 10, 277. [Google Scholar] [CrossRef]
- Hančinová, M.; Ondruš, D.; Ondrušová, M.; Mriňáková, B. Colorectal carcinoma—Epidemiology, risk factors, prognostic biomarkers. Klin. Onkol. 2025, 38, 16–24. [Google Scholar] [CrossRef]
- Diakité, M.T.; Diakité, B.; Koné, A.; Balam, S.; Fofana, D.; Diallo, D.; Kassogué, Y.; Traoré, C.B.; Kamaté, B.; Ba, D.; et al. Relationships between gut microbiota, red meat consumption and colorectal cancer. J. Carcinog. Mutagen. 2022, 13, 1000385. [Google Scholar] [PubMed] [PubMed Central]
- Grosso, G.; La Vignera, S.; Condorelli, R.A.; Godos, J.; Marventano, S.; Tieri, M.; Ghelfi, F.; Titta, L.; Lafranconi, A.; Gambera, A.; et al. Total, red and processed meat consumption and human health: An umbrella review of observational studies. Int. J. Food Sci. Nutr. 2022, 73, 726–737. [Google Scholar] [CrossRef]
- Luo, L.; Liu, Z.; Gan, Q.; Feng, J.; Wang, L.; Ouyang, W. Relationships of triglyceride-glucose-related indices with colorectal cancer incidence and mortality in an American population: A dose-response meta-analysis and cohort study. Lipids Health Dis. 2025, 24, 151. [Google Scholar] [CrossRef] [PubMed]
- Alkhaldy, A.A. Knowledge, attitudes, and practices toward colorectal cancer lifestyle risk factors among adults in Saudi Arabia. Front. Nutr. 2025, 12, 1507563. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Yan, J.; Sun, H.; Zhang, L.; Liu, Y.; Luo, X.; He, S.; Liu, Y.; Xu, W.; Gao, M.; et al. Not all colon cancer patients with preoperative hyperinflammatory status are at high risk of muscle loss and poor prognosis. Int. J. Color. Dis. 2025, 40, 100. [Google Scholar] [CrossRef] [PubMed]
- Deacu, M.; Enciu, M.; Nicolau, A.A.; Bălţătescu, G.I.; Neculai-Cândea, L.S.; Deacu, S.; Popa, M.F. Morphopathological features induced by SARS-CoV-2 infection—A series of 57 autopsies. Histol. Histopathol. 2023, 38, 513–524. [Google Scholar] [CrossRef]
- Gong, S.; Jin, X.; Guo, Y.; Yu, J. NLP for computational insights into nutritional impacts on colorectal cancer care. SLAS Technol. 2025, 32, 100295. [Google Scholar] [CrossRef]
- Atashi, N.; Eshaghian, N.; Anjom-Shoae, J.; Askari, G.; Asadi, M.; Sadeghi, O. Dietary intake and tissue biomarkers of omega-6 fatty acids and risk of colorectal cancer in adults: A systematic review and dose-response meta-analysis of prospective cohort studies. Nutr. Diabetes 2025, 15, 17. [Google Scholar] [CrossRef]
- Thakur, B.K.; Malaise, Y.; Choudhury, S.R.; Neustaeter, A.; Turpin, W.; Streutker, C.; Copeland, J.; Wong, E.O.Y.; Navarre, W.W.; Guttman, D.S.; et al. Dietary fibre counters the oncogenic potential of colibactin-producing Escherichia coli in colorectal cancer. Nat. Microbiol. 2025, 10, 855–870. [Google Scholar] [CrossRef]
- He, X.; Hou, J.; Liu, L.; Chen, X.; Zhang, L.; Pang, C.; Tong, Y.; Li, H.; Chen, F.; Peng, R.; et al. Dietary fiber consumption and outcomes of different cancers: An umbrella review. Food Nutr. Res. 2025, 69, 11034. [Google Scholar] [CrossRef]
- Ji, X.; Wang, L.; Luan, P.; Liang, J.; Cheng, W. The impact of dietary fiber on colorectal cancer patients based on machine learning. Front. Nutr. 2025, 12, 1508562. [Google Scholar] [CrossRef]
- Ma, T.; Tu, K.; Ou, Q.; Fang, Y.; Zhang, C. Comparing the Associations of Dietary Patterns Identified through Principal Component Analysis and Cluster Analysis with Colorectal Cancer Risk: A Large Case–Control Study in China. Nutrients 2024, 16, 147. [Google Scholar] [CrossRef]
- Liu, F.; Lv, Y.; Peng, Y.; Qiao, Y.; Wang, P.; Si, C.; Wang, X.; Gong, J.; Zhou, H.; Zhang, M.; et al. Plant-based dietary patterns, genetic predisposition and risk of colorectal cancer: A prospective study from the UK Biobank. J. Transl. Med. 2023, 21, 669. [Google Scholar] [CrossRef]
- Tsukanov, V.V.; Vasyutin, A.V.; Tonkikh, J.L. Risk factors, prevention and screening of colorectal cancer: A rising problem. World J. Gastroenterol. 2025, 31, 98629. [Google Scholar] [CrossRef] [PubMed]
- Celiberto, F.; Aloisio, A.; Girardi, B.; Pricci, M.; Iannone, A.; Russo, F.; Riezzo, G.; D’Attoma, B.; Ierardi, E.; Losurdo, G.; et al. Fibres and Colorectal Cancer: Clinical and Molecular Evidence. Int. J. Mol. Sci. 2023, 24, 13501. [Google Scholar] [CrossRef] [PubMed]
- Poorolajal, J.; Mohammadi, Y.; Fattahi-Darghlou, M.; Almasi-Moghadam, F. The association between major gastrointestinal cancers and red and processed meat and fish consumption: A systematic review and meta-analysis of the observational studies. PLoS ONE 2024, 19, e0305994. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, M.; Moreira, D.N.; Ghidini, M. Colon and rectal cancer: An emergent public health problem. World J. Gastroenterol. 2024, 30, 644–651. [Google Scholar] [CrossRef]
- Keum, N.; Giovannucci, E. Global burden of colorectal cancer: Emerging trends, risk factors and prevention strategies. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 713–732. [Google Scholar] [CrossRef]
- World Cancer Research Fund/American Institute for Cancer Research. Diet, Nutrition, Physical Activity and Cancer: A Global Perspective. Summary of the Third Expert Report; World Cancer Research Fund: London, UK, 2018; Available online: https://www.wcrf.org/wp-content/uploads/2024/11/Summary-of-Third-Expert-Report-2018.pdf (accessed on 13 June 2025).
- National Academies of Sciences, Engineering, and Medicine. Dietary Reference Intakes for Energy; The National Academies Press: Washington, DC, USA, 2023. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Colorectal Cancer Risk Factors; CDC: Atlanta, GA, USA, 2023. Available online: https://www.cdc.gov/colorectal-cancer/risk-factors/index.html (accessed on 14 June 2025).
- Institutul Național de Statistică. Migrația Internă. Available online: https://insse.ro/cms/files/Rapoarte%20de%20calitate/populatie/Migratia-interna.pdf (accessed on 24 June 2025).
- Fekete, M.; Lehoczki, A.; Szappanos, Á.; Zábó, V.; Kaposvári, C.; Horváth, A.; Farkas, Á.; Fazekas-Pongor, V.; Major, D.; Lipécz, Á.; et al. Vitamin D and Colorectal Cancer Prevention: Immunological Mechanisms, Inflammatory Pathways, and Nutritional Implications. Nutrients 2025, 17, 1351. [Google Scholar] [CrossRef]
- Aborode, A.T.; Onifade, I.A.; Olorunshola, M.M.; Adenikinju, G.O.; Aruorivwooghene, I.J.; Femi, A.C.; Osayawe, O.J.; Osinuga, A.; Omojowolo, E.A.; Adeoye, A.F.; et al. Biochemical mechanisms and molecular interactions of vitamins in cancer therapy. Cancer Pathog. Ther. 2024, 16, 3–15. [Google Scholar] [CrossRef]
- Burd, N.A.; McKenna, C.F.; Salvador, A.F.; Paulussen, K.J.M.; Moore, D.R. Dietary Protein Quantity, Quality, and Exercise Are Key to Healthy Living: A Muscle-Centric Perspective Across the Lifespan. Front. Nutr. 2019, 6, 83. [Google Scholar] [CrossRef]
- Seyyedsalehi, M.S.; Rossi, M.; Hadji, M.; Rashidian, H.; Marzban, M.; Parpinel, M.; Fiori, F.; Naghibzadeh-Tahami, A.; Hannun, Y.A.; Luberto, C.; et al. Dietary Choline and Betaine Intake and Risk of Colorectal Cancer in an Iranian Population. Cancers 2023, 15, 2557. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, R.L.U.; Sena-Evangelista, K.C.M.; de Azevedo, E.P.; Pinheiro, F.I.; Cobucci, R.N.; Pedrosa, L.F.C. Selenium in Human Health and Gut Microflora: Bioavailability of Selenocompounds and Relationship with Diseases. Front. Nutr. 2021, 8, 685317. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, S.M.; Zargarzadeh, N.; Rigi, S.; Persad, E.; Pizarro, A.B.; Hasani-Ranjbar, S.; Larijani, B.; Willett, W.C.; Esmaillzadeh, A. Egg Consumption and Risk of All-Cause and Cause-Specific Mortality: A Systematic Review and Dose-Response Meta-analysis of Prospective Studies. Adv Nutr. 2022, 2, 1762–1773. [Google Scholar] [CrossRef] [PubMed]
- Liang, Z.; Song, X.; Hu, J.; Wu, R.; Li, P.; Dong, Z.; Liang, L.; Wang, J. Fermented Dairy Food Intake and Risk of Colorectal Cancer: A Systematic Review and Meta-Analysis. Front Oncol. 2022, 25, 812679. [Google Scholar] [CrossRef]
- Slavin, J.L. Nutrients, foods, and colorectal cancer prevention. Nutr. Res. 2015, 35, 193–198. [Google Scholar]
- Shin, A.; Cho, S.; Sandin, S.; Lof, M.; Oh, M.Y.; Weiderpass, E. Omega-3 and -6 Fatty Acid Intake and Colorectal Cancer Risk in Swedish Women’s Lifestyle and Health Cohort. Cancer Res. Treat. 2020, 52, 848–854. [Google Scholar] [CrossRef]
- Volpato, M.; Hull, M.A. Omega-3 polyunsaturated fatty acids as adjuvant therapy of colorectal cancer. Cancer Metastasis Rev. 2018, 37, 545–555. [Google Scholar] [CrossRef]
- Fardet, A.; Boirie, Y. Associations between food and beverage groups and major diet-related chronic diseases: An exhaustive review of pooled/meta-analyses and systematic reviews. Nutr. Rev. 2014, 72, 741–762. [Google Scholar] [CrossRef]
- Aune, D.; Lau, R.; Chan, D.S.; Vieira, R.; Greenwood, D.C.; Kampman, E.; Norat, T. Dietary fibre, whole grains, and risk of colorectal cancer: Systematic review and dose-response meta-analysis of prospective studies. Gastroenterology 2011, 141, 106–118. [Google Scholar] [CrossRef]
- Wei, H.; Gao, Z.; Liang, R.; Li, Z.; Hao, H.; Liu, X. Whole-grain consumption and the risk of all-cause, CVD and cancer mortality: A meta-analysis of prospective cohort studies. Br. J. Nutr. 2016, 116, 514–525. [Google Scholar] [CrossRef]
- Vieira, A.R.; Abar, L.; Chan, D.S.M.; Vingeliene, S.; Polemiti, E.; Stevens, C.; Greenwood, D.; Norat, T. Foods and beverages and colorectal cancer risk: A systematic review and meta-analysis of cohort studies, an update of the evidence of the WCRF-AICR Continuous Update Project. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2017, 28, 1788–1802. [Google Scholar] [CrossRef]
- Fan, X.; Guo, H.; Teng, C.; Zhang, B.; Blecker, C.; Ren, G. Anti-Colon Cancer Activity of Novel Peptides Isolated from In Vitro Digestion of Quinoa Protein in Caco-2 Cells. Foods 2022, 11, 194. [Google Scholar] [CrossRef] [PubMed]
- Mueed, A.; Ibrahim, M.; Shibli, S.; Madjirebaye, P.; Deng, Z.; Jahangir, M. The fate of flaxseed-lignans after oral administration: A comprehensive review on its bioavailability, pharmacokinetics, and food design strategies for optimal application. Crit. Rev. Food Sci. Nutr. 2022, 64, 4312–4330. [Google Scholar] [CrossRef] [PubMed]
- Xi, X.; Fan, G.; Xue, H.; Peng, S.; Huang, W.; Zhan, J. Harnessing the Potential of Quinoa: Nutritional Profiling, Bioactive Components, and Implications for Health Promotion. Antioxidants 2024, 13, 829. [Google Scholar] [CrossRef] [PubMed]
- Cianfruglia, L.; Morresi, C.; Bacchetti, T.; Armeni, T.; Ferretti, G. Protection of Polyphenols against Glyco-Oxidative Stress: Involvement of Glyoxalase Pathway. Antioxidants 2020, 9, 1006. [Google Scholar] [CrossRef]
- Jedrychowski, W.; Maugeri, U.; Popiela, T.; Kulig, J.; Sochacka-Tatara, E.; Pac, A.; Sowa, A.; Musial, A. Case-control study on beneficial effect of regular consumption of apples on colorectal cancer risk in a population with relatively low intake of fruits and vegetables. Eur. J. Cancer Prev. Off. J. Eur. Cancer Prev. Organ. 2010, 19, 42–47. [Google Scholar] [CrossRef]
- Nezbedova, L.; McGhie, T.; Christensen, M.; Heyes, J.; Nasef, N.A.; Mehta, S. Onco-Preventive and Chemo-Protective Effects of Apple Bioactive Compounds. Nutrients 2021, 13, 4025. [Google Scholar] [CrossRef]
- Gallus, S.; Talamini, R.; Giacosa, A.; Montella, M.; Ramazzotti, V.; Franceschi, S.; Negri, E.; La Vecchia, C. Does an apple a day keep the oncologist away? Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2005, 16, 1841–1844. [Google Scholar] [CrossRef]
- Blando, F.; Calabriso, N.; Berland, H.; Maiorano, G.; Gerardi, C.; Carluccio, M.A.; Andersen, Ø.M. Radical Scavenging and Anti-Inflammatory Activities of Representative Anthocyanin Groupings from Pigment-Rich Fruits and Vegetables. Int. J. Mol. Sci. 2018, 19, 169. [Google Scholar] [CrossRef]
- Wu, Z.Y.; Chen, J.L.; Li, H.; Su, K.; Han, Y.W. Different types of fruit intake and colorectal cancer risk: A meta-analysis of observational studies. World J. Gastroenterol. 2023, 29, 2679–2700. [Google Scholar] [CrossRef] [PubMed]
- Mathers, J.C.; Elliott, F.; Macrae, F.; Mecklin, J.P.; Möslein, G.; McRonald, F.E.; Bertario, L.; Evans, D.G.; Gerdes, A.M.; CAPP2 Investigators; et al. Cancer Prevention with Resistant Starch in Lynch Syndrome Patients in the CAPP2-Randomized Placebo Controlled Trial: Planned 10-Year Follow-up. Cancer Prev. Res. 2022, 15, 623–634. [Google Scholar] [CrossRef]
- Lee, J.; Shin, A.; Oh, J.H.; Kim, J. Colors of vegetables and fruits and the risks of colorectal cancer. World J. Gastroenterol. 2017, 23, 2527–2538. [Google Scholar] [CrossRef]
- Collins, E.J.; Bowyer, C.; Tsouza, A.; Chopra, M. Tomatoes: An Extensive Review of the Associated Health Impacts of Tomatoes and Factors That Can Affect Their Cultivation. Biology 2022, 11, 239. [Google Scholar] [CrossRef]
- Chang, H.S.; Ko, M.; Ishizuka, M.; Fujita, S.; Yabuki, A.; Hossain, M.A.; Yamato, O. Sodium 2-propenyl thiosulfate derived from garlic induces phase II detoxification enzymes in rat hepatoma H4IIE cells. Nutr. Res. 2010, 30, 435–440. [Google Scholar] [CrossRef]
- McAlpine, P.L.; Fernández, J.; Villar, C.J.; Lombó, F. Organosulfur Compounds in Colorectal Cancer Prevention and Progression. Nutrients 2024, 16, 802. [Google Scholar] [CrossRef]
- Anjani, G.; Ayustaningwarno, F.; Eviana, R. Critical review on the immunomodulatory activities of carrot’s β-carotene and other bioactive compounds. J. Funct. Foods 2022, 99, 105303. [Google Scholar] [CrossRef]
- Roman, D.; Timar, B.; Avram, V.; Braha, A.; Saftescu, S.; Negru, Ș.; Timar, R. The Role of Nut and Seed Consumption in Colorectal Cancer: A Narrative Review. Medicina 2022, 58, 932. [Google Scholar] [CrossRef] [PubMed]
- Schulpen, M.; van den Brandt, P.A. Mediterranean diet adherence and risk of colorectal cancer: The prospective Netherlands Cohort Study. Eur. J. Epidemiol. 2020, 35, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Sieri, S.; Krogh, V.; Agnoli, C.; Ricceri, F.; Palli, D.; Masala, G.; Panico, S.; Mattiello, A.; Tumino, R.; Giurdanella, M.C.; et al. Dietary glycemic index and glycemic load and risk of colorectal cancer: Results from the EPIC-Italy study. Int. J. Cancer 2015, 136, 2923–2931. [Google Scholar] [CrossRef]
- Fike, L.T.; Munro, H.; Yu, D.; Dai, Q.; Shrubsole, M.J. Dietary polyphenols and the risk of colorectal cancer in the prospective Southern Community Cohort Study. Am. J. Clin. Nutr. 2022, 115, 1155–1165. [Google Scholar] [CrossRef]
- Bae, J.-M. Coffee Consumption and Colon Cancer Risk: A Meta-Epidemiological Study of Asian Cohort Studies. Asian Pac. J. Cancer Prev. 2020, 21, 1177–1179. [Google Scholar] [CrossRef]
- Zhao, L.G.; Li, Z.Y.; Feng, G.S.; Ji, X.W.; Tan, Y.T.; Li, H.L.; Gunter, M.J.; Xiang, Y.B. Coffee drinking and cancer risk: An umbrella review of meta-analyses of observational studies. BMC Cancer 2020, 20, 101. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority. Dietary reference values for nutrients: Summary report. EFSA Support. Publ. 2017, 14, e15121. [Google Scholar] [CrossRef]
- World Health Organization; Food and Agriculture Organization of the United Nations. Vitamin and Mineral Requirements in Human Nutrition, 2nd ed.; WHO: Geneva, Switzerland, 2004; Available online: https://www.who.int/publications/i/item/9241546123 (accessed on 14 June 2025).
- U.S. Department of Agriculture. FoodData Central; U.S. Department of Agriculture, Agricultural Research Service: Washington, DC, USA, 2025. Available online: https://fdc.nal.usda.gov/ (accessed on 24 June 2025).
- Popa, A.; Szuhanek, C.; Brad, S. Accurate Determination for Orthodontic Mini-implant Placement Using Acrylic Resin Surgical Guide and CBCT. Mat. Plast 2016, 53, 287. [Google Scholar]
- Elbaylek, H.; Ammor, S. Adherence to the Mediterranean Diet and Colorectal Cancer Risk Among Moroccan Population: Hospital-Based Case Control Study. Asian Pac. J. Cancer Prev. 2024, 25, 2853–2860. [Google Scholar] [CrossRef]
- Noori, F.; Behboodimoghadam, Z.; Haghani, S.; Pashaeypoor, S. The Effect of an Empowerment Program on the Health-promoting Behaviors of Iranian Women Workers: A Randomized Controlled Trial. J. Prev. Med. Public Health 2021, 54, 275–283. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Ghio, D.; Bosco, C.; Natale, F.; Loeschner, J.; Goujon, A. Age patterns of net migration and urbanisation dynamics across European municipalities. Popul. Space Place 2023, 29, e2599. [Google Scholar] [CrossRef]
- Caceres-Matos, R.; Castro-Méndez, A.; Domínguez, M.G.; Pabón-Carrasco, D.; Pabón-Carrasco, M. The Influence of Ultra-Processed Food on Colorectal Cancer: A Systematic Review. Gastrointest. Disord. 2024, 6, 164–179. [Google Scholar] [CrossRef]
- Chu, A.H.; Lin, K.; Croker, H.; Kefyalew, S.; Becerra-Tomás, N.; Dossus, L.; González-Gil, E.M.; Ahmadi, N.; Park, Y.; Krebs, J.; et al. Dietary patterns and colorectal cancer risk: Global Cancer Update Programme (CUP Global) systematic literature review. Am. J. Clin. Nutr. 2025, 121, 999–1016. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Hoffmann, G. Adherence to Mediterranean diet and risk of cancer: An updated systematic review and meta-analysis of observational studies. Cancer Med. 2015, 4, 1933–1947. [Google Scholar] [CrossRef]
- Sofi, F.; Abbate, R.; Gensini, G.F.; Casini, A. Accruing evidence on benefits of adherence to the Mediterranean diet on health: An updated systematic review and meta-analysis. Am. J. Clin. Nutr. 2010, 92, 1189–1196. [Google Scholar] [CrossRef] [PubMed]
- Rosato, V.; Guercio, V.; Bosetti, C.; Negri, E.; Serraino, D.; Giacosa, A.; Montella, M.; La Vecchia, C.; Tavani, A. Mediterranean diet and colorectal cancer risk: A pooled analysis of three Italian case-control studies. Br. J. Cancer 2016, 115, 862–865. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Y.; Zhu, Y.; Li, Q.; Wang, F.; Ge, X.; Zhou, G.; Miao, L. Association between Mediterranean diet adherence and colorectal cancer: A dose-response meta-analysis. Am. J. Clin. Nutr. 2020, 111, 1214–1225. [Google Scholar] [CrossRef] [PubMed]
- Chiurciu, I.-A.; Vlad, I.M.; Stoicea, P.; Zaharia, I.; David, L.; Soare, E.; Fîntîneru, G.; Micu, M.M.; Dinu, T.A.; Tudor, V.C.; et al. Romanian Meat Consumers’ Choices Favour Sustainability? Sustainability 2024, 16, 11193. [Google Scholar] [CrossRef]
- Marin, A.; Necula, D.M. Study on meat consumption in Romania in the period 2010–2020. In Agrarian Economy and Rural Development—Trends and Challenges. International Symposium, 13th ed.; Rodino, S., Dragomir, V., Eds.; The Research Institute for Agricultural Economy and Rural Development (ICEADR): Bucharest, Romania, 2022; pp. 119–125. [Google Scholar]
- Carr, P.R.; Banbury, B.L.; Berndt, S.I.; Campbell, P.T.; Chang-Claude, J.; Hayes, R.B.; Howard, B.V.; Jansen, L.; Jacobs, E.J.; Lane, D.S.; et al. Association Between Intake of Red and Processed Meat and Survival in Patients with Colorectal Cancer in a Pooled Analysis. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2019, 17, 1561–1570.e3. [Google Scholar] [CrossRef]
- Lea, E.J.; Crawford, D.; Worsley, A. Public views of the benefits and barriers to the consumption of a plant-based diet. Eur. J. Clin. Nutr. 2006, 60, 828–837. [Google Scholar] [CrossRef]
- Rosenfeld, D.L.; Tomiyama, A.J. Gender differences in meat consumption and attitudes: Findings from a nationally representative survey in the United States. Appetite 2021, 161, 105135. [Google Scholar]
- López-Olmedo, N.; Carriquiry, A.L.; Rodríguez-Ramírez, S.; Ramírez-Silva, I.; Espinosa-Montero, J.; Hernández-Barrera, L.; Campirano, F.; Martínez-Tapia, B.; Rivera, J.A. Usual Intake of Added Sugars and Saturated Fats Is High while Dietary Fiber Is Low in the Mexican Population. J. Nutr. 2016, 146, 1856S–1865S. [Google Scholar] [CrossRef]
- Renner, B.; Sproesser, G.; Strohbach, S.; Schupp, H.T. Why we eat what we eat. The Eating Motivation Survey (TEMS). Appetite 2012, 59, 117–128. [Google Scholar] [CrossRef]
- Paul Rozin Julia, M. Hormes, Myles S. Faith, Brian Wansink, Is Meat Male? A Quantitative Multimethod Framework to Establish Metaphoric Relationships. J. Consum. Res. 2012, 39, 629–643. [Google Scholar] [CrossRef]
- Stoll-Kleemann, S.; Schmidt, U.J. Reducing meat consumption in developed and transition countries to counter climate change and biodiversity loss: A review of influence factors. Reg. Environ. Change 2017, 17, 1261–1277. [Google Scholar] [CrossRef]
- Arnold, M.; Sierra, M.S.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017, 66, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Giskes, K.; Avendaňo, M.; Brug, J.; Kunst, A.E. A systematic review of studies on socioeconomic inequalities in dietary intakes associated with weight gain and overweight/obesity conducted among European adults. Obes. Rev. 2010, 11, 413–429. [Google Scholar] [CrossRef] [PubMed]
- Kliemann, N.; Wardle, J.; Johnson, F.; Croker, H. Reliability and validity of a revised version of the General Nutrition Knowledge Questionnaire. Eur. J. Clin. Nutr. 2016, 70, 1174–1180. [Google Scholar] [CrossRef]
- Prochaska, J.O.; Velicer, W.F. The transtheoretical model of health behavior change. Am. J. Health Promot. 1997, 12, 38–48. [Google Scholar] [CrossRef]
- Brug, J.; Oenema, A.; Ferreira, I. Theory, evidence and Intervention Mapping to improve behavior nutrition and physical activity interventions. Int. J. Behav. Nutr. Phys. Act. 2005, 2, 2. [Google Scholar] [CrossRef]
- Hebert, J.R.; Clemow, L.; Pbert, L.; Ockene, I.S.; Ockene, J.K. Social desirability bias in dietary self-report may compromise the validity of dietary intake measures. Int. J. Epidemiol. 1995, 24, 389–398. [Google Scholar] [CrossRef]
- James, R.H. Social Desirability Trait: Biaser or Driver of Self-Reported Dietary Intake? J. Acad. Nutr. Diet. 2016, 116, 1895–1898. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Physical Activity Level (PAL) | Predictive Equations of Individual Total Energy Expenditure (TEE) in Adults (>18 Years Old) | |
|---|---|---|
| Female | Male | |
| Inactive | 584.90 – (7.01 × age) + (5.72 × height) + (11.71 × weight) | 753.07 – (10.83 × age) + (6.50 × height) + (14.10 × weight) |
| Low active | 575.77 – (7.01 × age) + (6.60 × height) + (12.14 × weight) | 581.47 – (10.83 × age) + (8.30 × height) + (14.94 × weight) |
| Active | 710.25 – (7.01 × age) + (6.54 × height) + (12.34 × weight) | 1004.82 – (10.83 × age) + (6.52 × height) + (15.91 × weight) |
| Very active | 511.83 – (7.01 × age) + (9.07 × height) + (12.56 × weight) | – 517.88 – (10.83 × age) + (15.61 × height) + (19.11 × weight) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belean, M.-C.; Maghiar, T.-A.; Căpraru, A.-M.; Neamțu, A.-A.; Iliescu, D.; Iovin, V.-C.; Faur, F.-I.; Bugi, M.-A.; Totorean, A.; Tăban, S.; et al. Acceptability of a Colorectal Cancer-Preventive Diet Promoting Red Meat Reduction and Increased Fiber and Micronutrient Intake: A Cross-Sectional Study in Romanian Adults. Nutrients 2025, 17, 2386. https://doi.org/10.3390/nu17142386
Belean M-C, Maghiar T-A, Căpraru A-M, Neamțu A-A, Iliescu D, Iovin V-C, Faur F-I, Bugi M-A, Totorean A, Tăban S, et al. Acceptability of a Colorectal Cancer-Preventive Diet Promoting Red Meat Reduction and Increased Fiber and Micronutrient Intake: A Cross-Sectional Study in Romanian Adults. Nutrients. 2025; 17(14):2386. https://doi.org/10.3390/nu17142386
Chicago/Turabian StyleBelean, Marius-Cătălin, Teodor-Andrei Maghiar, Anca-Maria Căpraru, Andreea-Adriana Neamțu, Dan Iliescu, Valentin-Cristian Iovin, Flaviu-Ionuț Faur, Meda-Ada Bugi, Alina Totorean, Sorina Tăban, and et al. 2025. "Acceptability of a Colorectal Cancer-Preventive Diet Promoting Red Meat Reduction and Increased Fiber and Micronutrient Intake: A Cross-Sectional Study in Romanian Adults" Nutrients 17, no. 14: 2386. https://doi.org/10.3390/nu17142386
APA StyleBelean, M.-C., Maghiar, T.-A., Căpraru, A.-M., Neamțu, A.-A., Iliescu, D., Iovin, V.-C., Faur, F.-I., Bugi, M.-A., Totorean, A., Tăban, S., Dema, S., Dehelean, C.-A., Totolici, B. D., Pop, O. L., Crețu, O., & Neamțu, C. (2025). Acceptability of a Colorectal Cancer-Preventive Diet Promoting Red Meat Reduction and Increased Fiber and Micronutrient Intake: A Cross-Sectional Study in Romanian Adults. Nutrients, 17(14), 2386. https://doi.org/10.3390/nu17142386