
Impact of Short-Term Creatine Supplementation on Muscular Performance among Breast Cancer Survivors

 ,
,
Abstract
1. Introduction
2. Methods
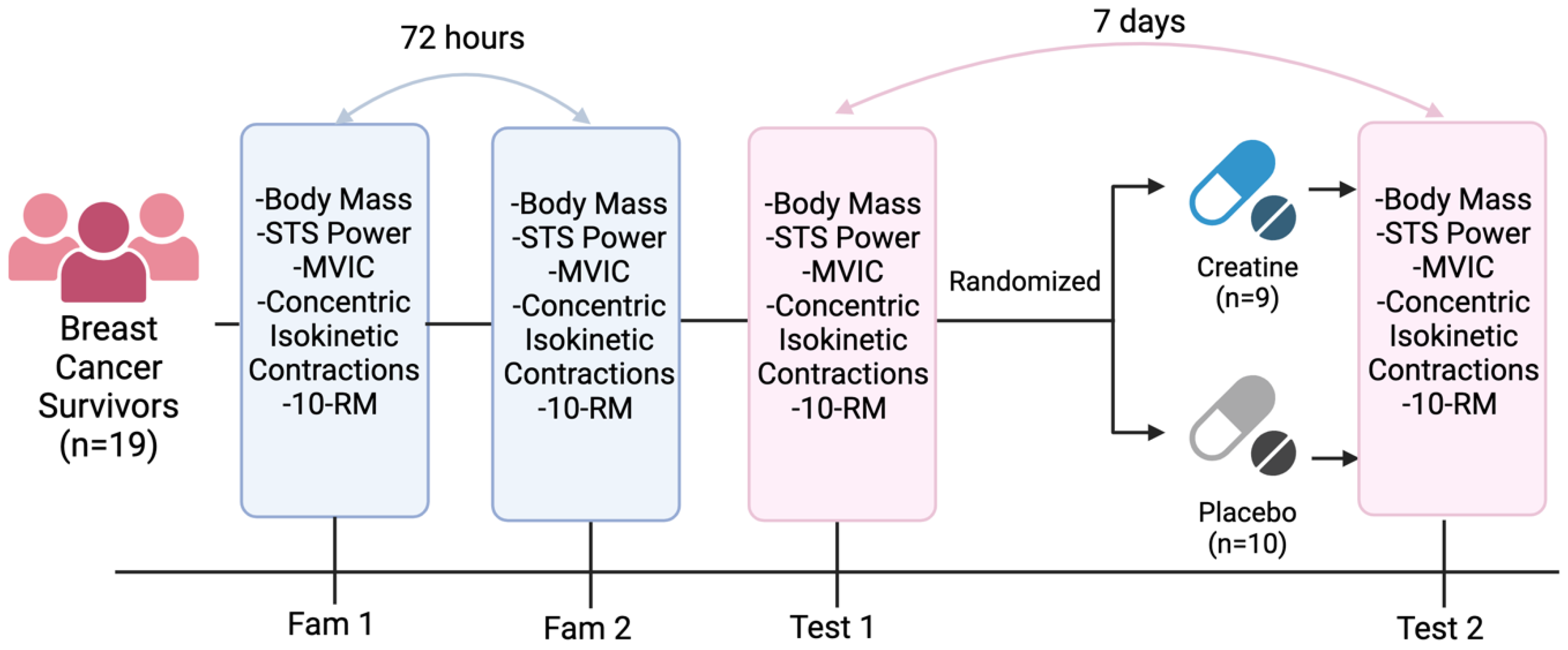
2.1. Experimental Approach to the Problem
2.2. Participants
2.3. Sit-to-Stand (STS) Power
2.4. 10 Repetition Maximum Strength
2.5. Maximal Voluntary Isometric and Concentric Isokinetic Knee Contractions
2.6. Supplementation
2.7. Statistical Analyses
3. Results
3.1. Participants
3.2. Body Mass
3.3. Sit-to-Stand Power
3.4. MVIC Peak Torque
3.5. 60°/Second Concentric Isokinetic Peak Torque
3.6. 120°/Second Concentric Isokinetic Peak Torque
3.7. 10RM Chest Press
3.8. 10RM Leg Extension
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef]
- Godinho-Mota, J.C.M.; Mota, J.F.; Gonçalves, L.V.; Soares, L.R.; Schincaglia, R.M.; Prado, C.M.; Martins, K.A.; Freitas-Junior, R. Chemotherapy Negatively Impacts Body Composition, Physical Function and Metabolic Profile in Patients with Breast Cancer. Clin. Nutr. 2021, 40, 3421–3428. [Google Scholar] [CrossRef] [PubMed]
- Stein, K.D.; Syrjala, K.L.; Andrykowski, M.A. Physical and Psychological Long-Term and Late Effects of Cancer. Cancer 2008, 112, 2577–2592. [Google Scholar] [CrossRef] [PubMed]
- Pin, F.; Couch, M.E.; Bonetto, A. Preservation of Muscle Mass as a Strategy to Reduce the Toxic Effects of Cancer Chemotherapy on Body Composition. Curr. Opin. Support. Palliat. Care 2018, 12, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Jia, M.; Zhang, X.; Wei, L.; Gao, J. Measurement, Outcomes and Interventions of Cognitive Function after Breast Cancer Treatment: A Narrative Review. Asia Pac. J. Clin. Oncol. 2021, 17, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Lee, E.; Jang, I.-Y. Frailty and Comprehensive Geriatric Assessment. J. Korean Med. Sci. 2019, 35, e16. [Google Scholar] [CrossRef] [PubMed]
- Rawson, E.S.; Venezia, A.C. Use of Creatine in the Elderly and Evidence for Effects on Cognitive Function in Young and Old. Amino Acids 2011, 40, 1349–1362. [Google Scholar] [CrossRef] [PubMed]
- Brosnan, M.E.; Brosnan, J.T. The Role of Dietary Creatine. Amino Acids 2016, 48, 1785–1791. [Google Scholar] [CrossRef]
- Balsom, P.D.; Söderlund, K.; Ekblom, B. Creatine in Humans with Special Reference to Creatine Supplementation. Sports Med. 1994, 18, 268–280. [Google Scholar] [CrossRef]
- Persky, A.M.; Brazeau, G.A.; Hochhaus, G. Pharmacokinetics of the Dietary Supplement Creatine. Clin. Pharmacokinet. 2003, 42, 557–574. [Google Scholar] [CrossRef]
- Antonio, J.; Candow, D.G.; Forbes, S.C.; Gualano, B.; Jagim, A.R.; Kreider, R.B.; Rawson, E.S.; Smith-Ryan, A.E.; VanDusseldorp, T.A.; Willoughby, D.S.; et al. Common Questions and Misconceptions about Creatine Supplementation: What Does the Scientific Evidence Really Show? J. Int. Soc. Sports Nutr. 2021, 18, 13. [Google Scholar] [CrossRef]
- Hultman, E.; Söderlund, K.; Timmons, J.A.; Cederblad, G.; Greenhaff, P.L. Muscle Creatine Loading in Men. J. Appl. Physiol. 1996, 81, 232–237. [Google Scholar] [CrossRef]
- Harris, R.C.; Söderlund, K.; Hultman, E. Elevation of Creatine in Resting and Exercised Muscle of Normal Subjects by Creatine Supplementation. Clin. Sci. 1992, 83, 367–374. [Google Scholar] [CrossRef]
- Gotshalk, L.A.; Kraemer, W.J.; Mendonca, M.A.G.; Vingren, J.L.; Kenny, A.M.; Spiering, B.A.; Hatfield, D.L.; Fragala, M.S.; Volek, J.S. Creatine Supplementation Improves Muscular Performance in Older Women. Eur. J. Appl. Physiol. 2008, 102, 223–231. [Google Scholar] [CrossRef]
- Maganaris, C.N.; Maughan, R.J. Creatine Supplementation Enhances Maximum Voluntary Isometric Force and Endurance Capacity in Resistance Trained Men. Acta Physiol. Scand. 1998, 163, 279–287. [Google Scholar] [CrossRef]
- Mills, S.; Candow, D.G.; Forbes, S.C.; Neary, J.P.; Ormsbee, M.J.; Antonio, J. Effects of Creatine Supplementation during Resistance Training Sessions in Physically Active Young Adults. Nutrients 2020, 12, 1880. [Google Scholar] [CrossRef]
- Dalbo, V.J.; Roberts, M.D.; Lockwood, C.M.; Tucker, P.S.; Kreider, R.B.; Kerksick, C.M. The Effects of Age on Skeletal Muscle and the Phosphocreatine Energy System: Can Creatine Supplementation Help Older Adults. Dyn. Med. 2009, 8, 6. [Google Scholar] [CrossRef]
- Avgerinos, K.I.; Spyrou, N.; Bougioukas, K.I.; Kapogiannis, D. Effects of Creatine Supplementation on Cognitive Function of Healthy Individuals: A Systematic Review of Randomized Controlled Trials. Exp. Gerontol. 2018, 108, 166–173. [Google Scholar] [CrossRef]
- Cramer, J.T.; Stout, J.R.; Culbertson, J.Y.; Egan, A.D. Effects of Creatine Supplementation and Three Days of Resistance Training on Muscle Strength, Power Output, and Neuromuscular Function. J. Strength Cond. Res. 2007, 21, 668–677. [Google Scholar] [CrossRef]
- Clifford, B.; Koizumi, S.; Wewege, M.A.; Leake, H.B.; Ha, L.; Macdonald, E.; Fairman, C.M.; Hagstrom, A.D. The Effect of Resistance Training on Body Composition During and After Cancer Treatment: A Systematic Review and Meta-Analysis. Sports Med. 2021, 51, 2527–2546. [Google Scholar] [CrossRef]
- Fairman, C.M.; Kendall, K.L.; Newton, R.U.; Hart, N.H.; Taaffe, D.R.; Chee, R.; Tang, C.I.; Galvão, D.A. Examining the Effects of Creatine Supplementation in Augmenting Adaptations to Resistance Training in Patients with Prostate Cancer Undergoing Androgen Deprivation Therapy: A Randomised, Double-Blind, Placebo-Controlled Trial. BMJ Open 2019, 9, e030080. [Google Scholar] [CrossRef] [PubMed]
- Lønbro, S.; Dalgas, U.; Primdahl, H.; Overgaard, J.; Overgaard, K. Feasibility and Efficacy of Progressive Resistance Training and Dietary Supplements in Radiotherapy Treated Head and Neck Cancer Patients--the DAHANCA 25A Study. Acta Oncol. 2013, 52, 310–318. [Google Scholar] [CrossRef]
- Pires, L.A.M.; Forbes, S.C.; Candow, D.G.; Machado, M. Creatine Supplementation on Cognitive Performance Following Exercise in Female Muay Thai Athletes. NeuroSports 2020, 1, 6. [Google Scholar]
- Alcazar, J.; Losa-Reyna, J.; Rodriguez-Lopez, C.; Alfaro-Acha, A.; Rodriguez-Mañas, L.; Ara, I.; García-García, F.J.; Alegre, L.M. The Sit-to-Stand Muscle Power Test: An Easy, Inexpensive and Portable Procedure to Assess Muscle Power in Older People. Exp. Gerontol. 2018, 112, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Balachandran, A.T.; Vigotsky, A.D.; Quiles, N.; Mokkink, L.B.; Belio, M.A.; Glenn, J.M. Validity, Reliability, and Measurement Error of a Sit-to-Stand Power Test in Older Adults: A Pre-Registered Study. Exp. Gerontol. 2021, 145, 111202. [Google Scholar] [CrossRef]
- Walker, S.; Avela, J.; Wikgren, J.; Meeusen, R.; Piitulainen, H.; Baker, S.N.; Parviainen, T.M. Aging and Strength Training Influence Knee Extensor Intermuscular Coherence During Low- and High-Force Isometric Contractions. Front. Physiol. 2019, 9, 1933. [Google Scholar] [CrossRef] [PubMed]
- Van Driessche, S.; Delecluse, C.; Bautmans, I.; Vanwanseele, B.; Van Roie, E. Age-Related Differences in Rate of Power Development Exceed Differences in Peak Power. Exp. Gerontol. 2018, 101, 95–100. [Google Scholar] [CrossRef]
- Van Roie, E.; Walker, S.; Van Driessche, S.; Baggen, R.; Coudyzer, W.; Bautmans, I.; Delecluse, C. Training Load Does Not Affect Detraining’s Effect on Muscle Volume, Muscle Strength and Functional Capacity among Older Adults. Exp. Gerontol. 2017, 98, 30–37. [Google Scholar] [CrossRef]
- Baggen, R.J.; Van Roie, E.; Verschueren, S.M.; Van Driessche, S.; Coudyzer, W.; van Dieën, J.H.; Delecluse, C. Bench Stepping with Incremental Heights Improves Muscle Volume, Strength and Functional Performance in Older Women. Exp. Gerontol. 2019, 120, 6–14. [Google Scholar] [CrossRef]
- Palmer, T.B.; Blinch, J.; Farrow, A.C.; Agu-Udemba, C.C.; Mitchell, E.A. Utility of Peak Torque and Rate of Torque Development Characteristics to Identify Walking Performance Ability in Older Women. J. Musculoskelet. Neuronal Interact. 2021, 21, 455–463. [Google Scholar]
- Klassen, O.; Schmidt, M.E.; Ulrich, C.M.; Schneeweiss, A.; Potthoff, K.; Steindorf, K.; Wiskemann, J. Muscle Strength in Breast Cancer Patients Receiving Different Treatment Regimes. J. Cachexia Sarcopenia Muscle 2017, 8, 305–316. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.; Trojian, T.H. Creatine Supplementation. Curr. Sports Med. Rep. 2013, 12, 240. [Google Scholar] [CrossRef] [PubMed]
- Greenhaff, P.L.; Bodin, K.; Soderlund, K.; Hultman, E. Effect of Oral Creatine Supplementation on Skeletal Muscle Phosphocreatine Resynthesis. Am. J. Physiol.-Endocrinol. Metab. 1994, 266, E725–E730. [Google Scholar] [CrossRef] [PubMed]
- Casey, A.; Constantin-Teodosiu, D.; Howell, S.; Hultman, E.; Greenhaff, P.L. Creatine Ingestion Favorably Affects Performance and Muscle Metabolism during Maximal Exercise in Humans. Am. J. Physiol.-Endocrinol. Metab. 1996, 271, E31–E37. [Google Scholar] [CrossRef] [PubMed]
- Ostojic, S.M.; Ahmetovic, Z. Gastrointestinal Distress after Creatine Supplementation in Athletes: Are Side Effects Dose Dependent? Res. Sports Med. Print 2008, 16, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: London, UK, 1988. [Google Scholar]
- JASP—A Fresh Way to Do Statistics. Available online: https://jasp-stats.org/ (accessed on 30 October 2023).
- Weir, C.B.; Jan, A. BMI Classification Percentile And Cut Off Points. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Earnest, C.P.; Snell, P.G.; Rodriguez, R.; Almada, A.L.; Mitchell, T.L. The Effect of Creatine Monohydrate Ingestion on Anaerobic Power Indices, Muscular Strength and Body Composition. Acta Physiol. Scand. 1995, 153, 207–209. [Google Scholar] [CrossRef]
- Chwalbiñska-Moneta, J. Effect of Creatine Supplementation on Aerobic Performance and Anaerobic Capacity in Elite Rowers in the Course of Endurance Training. Int. J. Sport Nutr. Exerc. Metab. 2003, 13, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Gotshalk, L.A.; Volek, J.S.; Staron, R.S.; Denegar, C.R.; Hagerman, F.C.; Kraemer, W.J. Creatine Supplementation Improves Muscular Performance in Older Men. Med. Sci. Sports Exerc. 2002, 34, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Selsby, J.T.; Beckett, K.D.; Kern, M.; Devor, S.T. Swim Performance Following Creatine Supplementation in Division III Athletes. J. Strength Cond. Res. 2003, 17, 421–424. [Google Scholar] [CrossRef]
- Warber, J.P.; Tharion, W.J.; Patton, J.F.; Champagne, C.M.; Mitotti, P.; Lieberman, H.R. The Effect of Creatine Monohydrate Supplementation on Obstacle Course and Multiple Bench Press Performance. J. Strength Cond. Res. 2002, 16, 500–508. [Google Scholar]
- Kreider, R.B.; Ferreira, M.; Wilson, M.; Grindstaff, P.; Plisk, S.; Reinardy, J.; Cantler, E.; Almada, A.L. Effects of Creatine Supplementation on Body Composition, Strength, and Sprint Performance. Med. Sci. Sports Exerc. 1998, 30, 73–82. [Google Scholar] [CrossRef] [PubMed]
- McNaughton, L.R.; Dalton, B.; Tarr, J. The Effects of Creatine Supplementation on High-Intensity Exercise Performance in Elite Performers. Eur. J. Appl. Physiol. 1998, 78, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Rossiter, H.B.; Cannell, E.R.; Jakeman, P.M. The Effect of Oral Creatine Supplementation on the 1000-m Performance of Competitive Rowers. J. Sports Sci. 1996, 14, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Volek, J.S.; Kraemer, W.J.; Bush, J.A.; Boetes, M.; Incledon, T.; Clark, K.L.; Lynch, J.M. Creatine Supplementation Enhances Muscular Performance during High-Intensity Resistance Exercise. J. Am. Diet. Assoc. 1997, 97, 765–770. [Google Scholar] [CrossRef]
- Odland, L.M.; MacDougall, J.D.; Tarnopolsky, M.A.; Elorriaga, A.; Borgmann, A. Effect of Oral Creatine Supplementation on Muscle [PCr] and Short-Term Maximum Power Output. Med. Sci. Sports Exerc. 1997, 29, 216–219. [Google Scholar] [CrossRef] [PubMed]
- Aedma, M.; Timpmann, S.; Lätt, E.; Ööpik, V. Short-Term Creatine Supplementation Has No Impact on Upper-Body Anaerobic Power in Trained Wrestlers. J. Int. Soc. Sports Nutr. 2015, 12, 45. [Google Scholar] [CrossRef] [PubMed]
- Deutekom, M.; Beltman, J.G.; de Ruiter, C.J.; de Koning, J.J.; de Haan, A. No Acute Effects of Short-Term Creatine Supplementation on Muscle Properties and Sprint Performance. Eur. J. Appl. Physiol. 2000, 82, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Greenhaff, P.L. The Nutritional Biochemistry of Creatine. J. Nutr. Biochem. 1997, 8, 610–618. [Google Scholar] [CrossRef]
- Syrotuik, D.G.; Bell, G.J. Acute Creatine Monohydrate Supplementation: A Descriptive Physiological Profile of Responders vs. Nonresponders. J. Strength Cond. Res. 2004, 18, 610–617. [Google Scholar] [CrossRef]
- Amitani, M.; Oba, T.; Kiyosawa, N.; Morikawa, H.; Chino, T.; Soma, A.; Shimizu, T.; Ohno, K.; Ono, M.; Ito, T.; et al. Skeletal Muscle Loss during Neoadjuvant Chemotherapy Predicts Poor Prognosis in Patients with Breast Cancer. BMC Cancer 2022, 22, 327. [Google Scholar] [CrossRef]
- Mallard, J.; Hucteau, E.; Hureau, T.J.; Pagano, A.F. Skeletal Muscle Deconditioning in Breast Cancer Patients Undergoing Chemotherapy: Current Knowledge and Insights from Other Cancers. Front. Cell Dev. Biol. 2021, 9, 719643. [Google Scholar] [CrossRef]
- Carroll, J.E.; Bower, J.E.; Ganz, P.A. Cancer-Related Accelerated Ageing and Biobehavioural Modifiers: A Framework for Research and Clinical Care. Nat. Rev. Clin. Oncol. 2022, 19, 173–187. [Google Scholar] [CrossRef]
- Guida, J.L.; Ahles, T.A.; Belsky, D.; Campisi, J.; Cohen, H.J.; DeGregori, J.; Fuldner, R.; Ferrucci, L.; Gallicchio, L.; Gavrilov, L.; et al. Measuring Aging and Identifying Aging Phenotypes in Cancer Survivors. J. Natl. Cancer Inst. 2019, 111, 1245–1254. [Google Scholar] [CrossRef]
- Bhatia, R.; Holtan, S.; Jurdi, N.E.; Prizment, A.; Blaes, A. Do Cancer and Cancer Treatments Accelerate Aging? Curr. Oncol. Rep. 2022, 24, 1401–1412. [Google Scholar] [CrossRef]
- Wang, S.; Prizment, A.; Thyagarajan, B.; Blaes, A. Cancer Treatment-Induced Accelerated Aging in Cancer Survivors: Biology and Assessment. Cancers 2021, 13, 427. [Google Scholar] [CrossRef]
- Chen, Y.-J.; Li, X.-X.; Ma, H.-K.; Zhang, X.; Wang, B.-W.; Guo, T.-T.; Xiao, Y.; Bing, Z.-T.; Ge, L.; Yang, K.-H.; et al. Exercise Training for Improving Patient-Reported Outcomes in Patients With Advanced-Stage Cancer: A Systematic Review and Meta-Analysis. J. Pain Symptom Manag. 2020, 59, 734–749.e10. [Google Scholar] [CrossRef]
- Mallard, J.; Hucteau, E.; Schott, R.; Trensz, P.; Pflumio, C.; Kalish-Weindling, M.; Favret, F.; Pivot, X.; Hureau, T.J.; Pagano, A.F. Early Skeletal Muscle Deconditioning and Reduced Exercise Capacity during (Neo)Adjuvant Chemotherapy in Patients with Breast Cancer. Cancer 2023, 129, 215–225. [Google Scholar] [CrossRef]
- Fairman, C.M.; Lønbro, S.; Cardaci, T.D.; VanderVeen, B.N.; Nilsen, T.S.; Murphy, A.E. Muscle Wasting in Cancer: Opportunities and Challenges for Exercise in Clinical Cancer Trials. JCSM Rapid Commun. 2022, 5, 52–67. [Google Scholar] [CrossRef]
- Bland, K.A.; Kouw, I.W.K.; van Loon, L.J.C.; Zopf, E.M.; Fairman, C.M. Exercise-Based Interventions to Counteract Skeletal Muscle Mass Loss in People with Cancer: Can We Overcome the Odds? Sports Med. 2022, 52, 1009–1027. [Google Scholar] [CrossRef]
- Yen, C.-J.; Hung, C.-H.; Tsai, W.-M.; Cheng, H.-C.; Yang, H.-L.; Lu, Y.-J.; Tsai, K.-L. Effect of Exercise Training on Exercise Tolerance and Level of Oxidative Stress for Head and Neck Cancer Patients Following Chemotherapy. Front. Oncol. 2020, 10, 1536. [Google Scholar] [CrossRef]
- Kreider, R.B.; Kalman, D.S.; Antonio, J.; Ziegenfuss, T.N.; Wildman, R.; Collins, R.; Candow, D.G.; Kleiner, S.M.; Almada, A.L.; Lopez, H.L. International Society of Sports Nutrition Position Stand: Safety and Efficacy of Creatine Supplementation in Exercise, Sport, and Medicine. J. Int. Soc. Sports Nutr. 2017, 14, 18. [Google Scholar] [CrossRef] [PubMed]
- Burke, R.; Piñero, A.; Coleman, M.; Mohan, A.; Sapuppo, M.; Augustin, F.; Aragon, A.A.; Candow, D.G.; Forbes, S.C.; Swinton, P.; et al. The Effects of Creatine Supplementation Combined with Resistance Training on Regional Measures of Muscle Hypertrophy: A Systematic Review with Meta-Analysis. Nutrients 2023, 15, 2116. [Google Scholar] [CrossRef] [PubMed]
- Chilibeck, P.D.; Kaviani, M.; Candow, D.G.; Zello, G.A. Effect of Creatine Supplementation during Resistance Training on Lean Tissue Mass and Muscular Strength in Older Adults: A Meta-Analysis. Open Access J. Sports Med. 2017, 8, 213–226. [Google Scholar] [CrossRef]

{kind=link}
| Total n, % | All | Creatine (SUPP) | Placebo (PLA) | |||
|---|---|---|---|---|---|---|
| 19 | % or (SD) | 9 | % or (SD) | % or (SD) | 100% | |
| Age (yrs), mean (SD) | 57.63 | (10.48) | 58.11 | (11.22) | 57.20 | (9.74) |
| Body mass (kg), mean (SD) | 76.04 | (15.31) | 77.20 | (13.10) | 74.99 | (16.99) |
| Height (cm), mean (SD) | 162.42 | (4.82) | 164.11 | (5.80) | 160.91 | (3.01) |
| BMI (kg/m2), mean (SD) | 29.97 | (5.79) | 30.91 | (5.97) | 28.09 | (4.90) |
| Smoking status, n% | ||||||
| No smoking since year before diagnosis | 13 | 68% | 5 | 56% | 8 | 80% |
| Ex-smoker | 6 | 32% | 4 | 44% | 2 | 20% |
| Cancer stage, n % | ||||||
| I | 11 | 58% | 5 | 56% | 6 | 60% |
| II | 6 | 32% | 3 | 33% | 3 | 30% |
| III | 2 | 10% | 1 | 11% | 1 | 10% |
| Cancer treatment, n % | ||||||
| Surgery | 19 | 100% | 9 | 100% | 10 | 100% |
| Chemotherapy | 15 | 79% | 7 | 78% | 8 | 80% |
| Immunotherapy | 2 | 21% | 1 | 11% | 1 | 10% |
| Hormone therapy | 6 | 32% | 3 | 33% | 3 | 30% |
| Radiotherapy | 16 | 84% | 8 | 89% | 8 | 80% |
| Osteoporosis or osteoarthritis, n% | ||||||
| Yes | 7 | 37% | 2 | 11% | 1 | 10% |
| Outcome | SUPP | PLA | p Value * | ||||
|---|---|---|---|---|---|---|---|
| Pre | Post | Mean Difference | Pre | Post | Mean Difference | ||
| Sit-to-stand power (W) | 1500.78 ± 635.11 | 1566.00 ± 636.03 | 65.22 | 1475.70 ± 614.59 | 1663.40± 642.76 | 187.70 | 0.47 |
| 60° concentric isokinetic peak torque (Nm) | 68.38 ± 16.07 | 71.06 ± 16.47 | 2.68 | 61.20 ± 19.79 | 67.60 ± 16.64 | 6.40 | 0.53 |
| 120° concentric isokinetic peak torque (Nm) | 52.48 ± 13.51 | 52.86 ± 10.64 | 0.38 | 51.28 ± 18.07 | 51.69 ± 10.17 | 0.41 | 0.99 |
| MVIC peak torque (Nm) | 85.53 ± 22.39 | 90.91 ± 30.19 | 5.38 | 69.78 ± 21.86 | 74.28 ± 23.19 | 4.50 | 0.91 |
| 10RM chest press (kg) | 19.15 ± 3.23 | 21.16 ± 3.40 | 2.01 | 20.41 ± 5.66 | 21.77 ± 6.25 | 1.36 | 0.41 |
| 10RM leg extension (kg) | 23.43 ± 4.94 | 24.94 ± 6.00 | 1.51 | 24.26 ± 8.49 | 25.85 ± 8.01 | 1.59 | 0.93 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parsowith, E.J.; Stock, M.S.; Kocuba, O.; Schumpp, A.; Jackson, K.; Brooks, A.M.; Larson, A.; Dixon, M.; Fairman, C.M. Impact of Short-Term Creatine Supplementation on Muscular Performance among Breast Cancer Survivors. Nutrients 2024, 16, 979. https://doi.org/10.3390/nu16070979
Parsowith EJ, Stock MS, Kocuba O, Schumpp A, Jackson K, Brooks AM, Larson A, Dixon M, Fairman CM. Impact of Short-Term Creatine Supplementation on Muscular Performance among Breast Cancer Survivors. Nutrients. 2024; 16(7):979. https://doi.org/10.3390/nu16070979
Chicago/Turabian StyleParsowith, Emily J., Matt S. Stock, Olivia Kocuba, Alec Schumpp, Kylah Jackson, Alexander M. Brooks, Alena Larson, Madison Dixon, and Ciaran M. Fairman. 2024. "Impact of Short-Term Creatine Supplementation on Muscular Performance among Breast Cancer Survivors" Nutrients 16, no. 7: 979. https://doi.org/10.3390/nu16070979
APA StyleParsowith, E. J., Stock, M. S., Kocuba, O., Schumpp, A., Jackson, K., Brooks, A. M., Larson, A., Dixon, M., & Fairman, C. M. (2024). Impact of Short-Term Creatine Supplementation on Muscular Performance among Breast Cancer Survivors. Nutrients, 16(7), 979. https://doi.org/10.3390/nu16070979