
Effect of a Low-Calorie Dietary Intervention on Liver Health and Body Weight in Adults with Metabolic-Dysfunction Associated Steatotic Liver Disease (MASLD) and Overweight/Obesity: A Systematic Review and Meta-Analysis

 ,
,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Definition of Low-Calorie Diet and Very-Low-Calorie Diet
2.3. Systematic Review Aim
2.4. Inclusion/Exclusion Criteria
2.5. Outcome Measures
- Biochemical outcomes: Change in Aspartate Aminotransferase (AST), Gamma-Glutamyl Transpeptidase (GGT), Fatty Liver Index (FLI) and SteatoTest.
- Body anthropometry outcomes: Change in body weight, body mass index (BMI) and body fat percentage.
- Liver imaging outcomes: Ultrasound (echogenicity), Transient elastography (including measurement of controlled attenuation parameter (CAP)), MRI-determined measurements of liver fat (PDFF, proton density fat fraction), Magnetic resonance spectroscopy (hepatic fat fraction) and Magnetic resonance elastography.
- Liver histology: Regression of histological changes in MASLD on liver biopsy, improvement in steatosis/reduction in NASH Activity Score (NAS) and improvement in fibrosis.
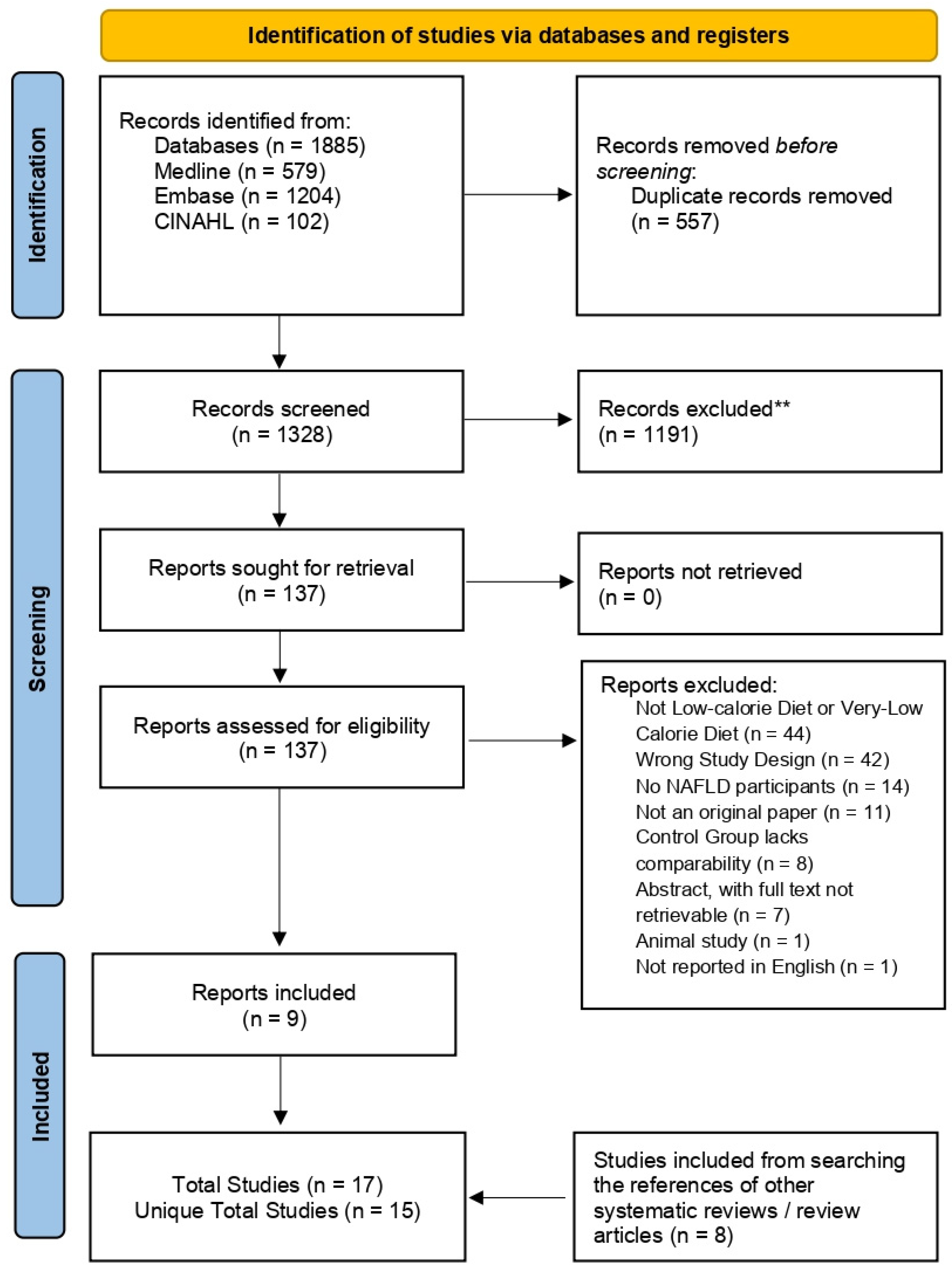
2.6. Literature Screening
2.7. Data Extraction
2.8. Quality Assessment
2.9. Statistics
3. Results
3.1. Systematic Review and Intervention Characteristics
3.1.1. Included Studies Subsection
3.1.2. Intervention Characteristics
3.1.3. Studies Nearly Meeting Inclusion
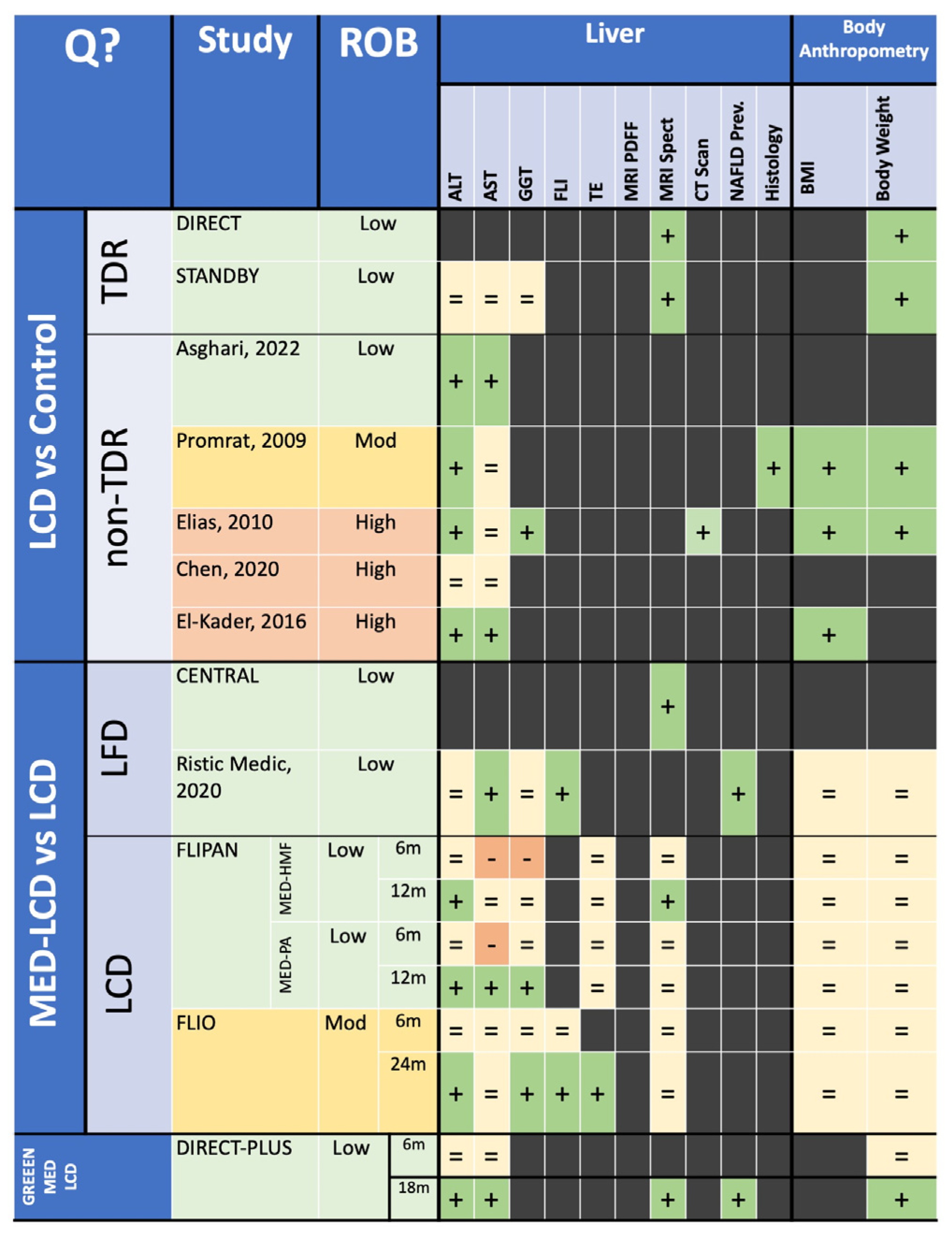
3.2. Risk of Bias Assessment
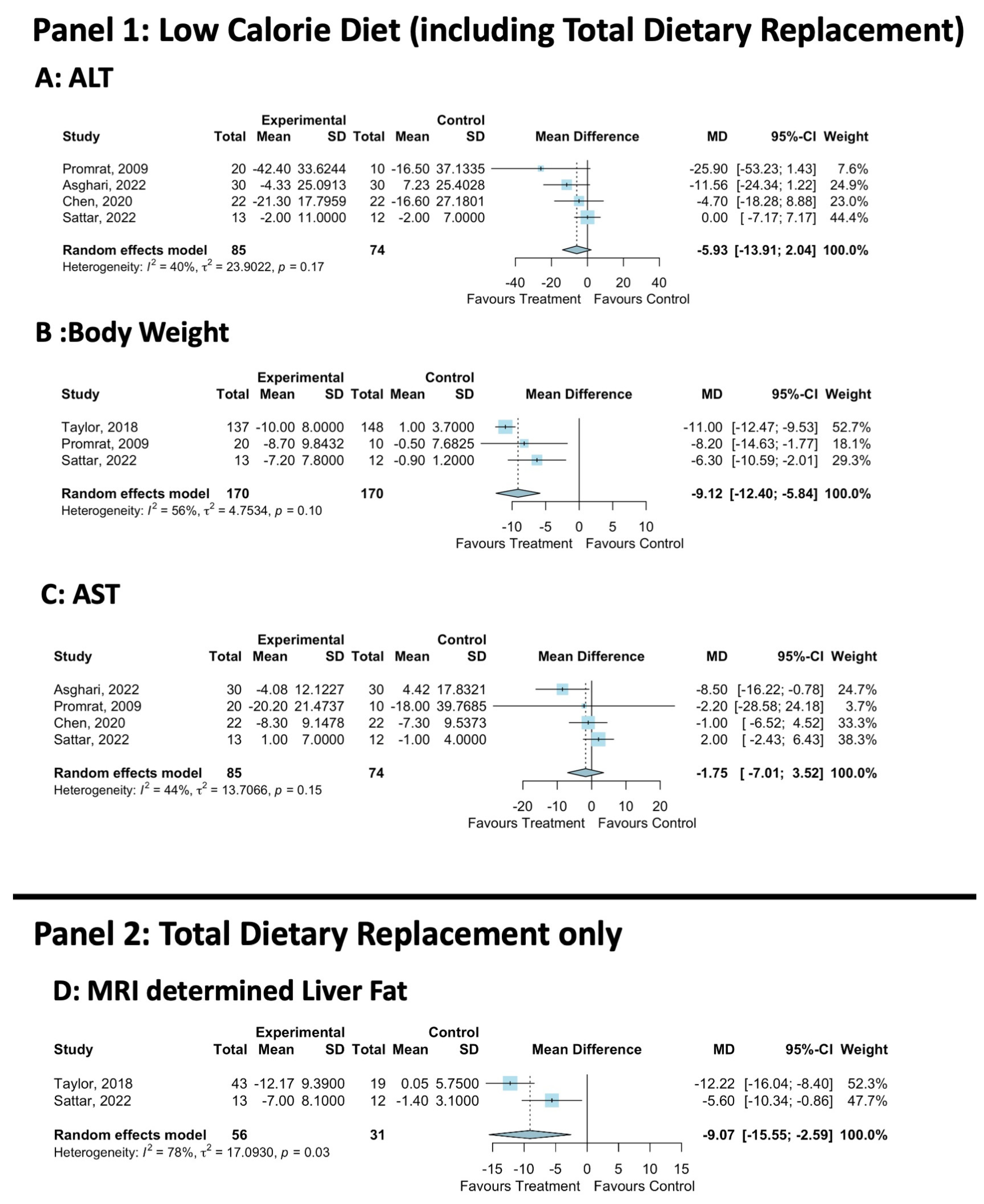
3.3. Trials Assessing LCD vs. Control (Including TDR)
3.3.1. Trial Demographics
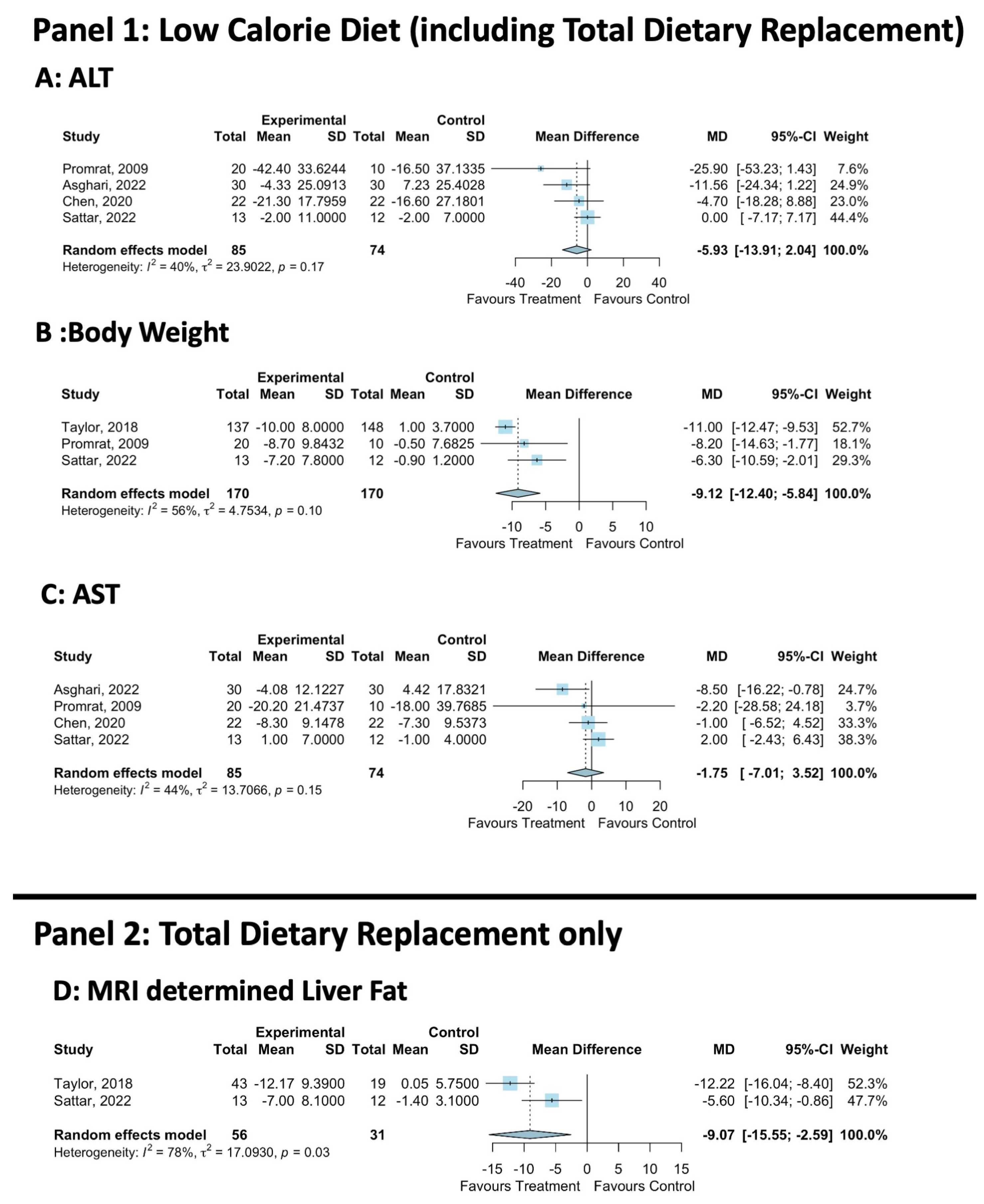
3.3.2. Primary Outcome—ALT
3.3.3. Secondary Liver Health Outcomes
3.3.4. Secondary Body Composition Outcomes
3.4. Trials Assessing TDR vs. Control
3.4.1. Trial Demographics
3.4.2. Liver Fat Quantification
3.4.3. Body Composition
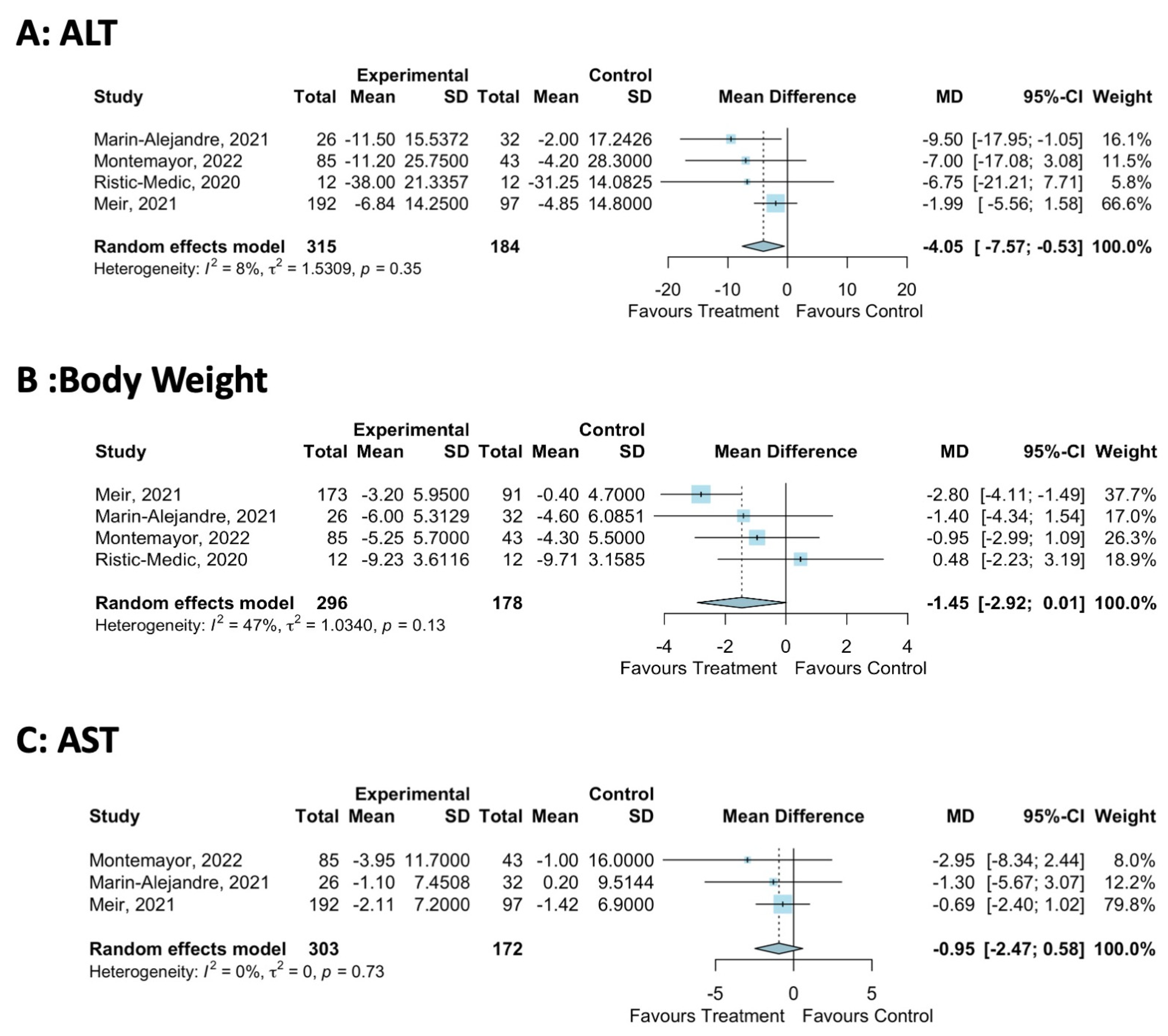
3.5. Trials Assessing Mediterranean-LCD vs. Other LCDs
3.5.1. Trial Demographics
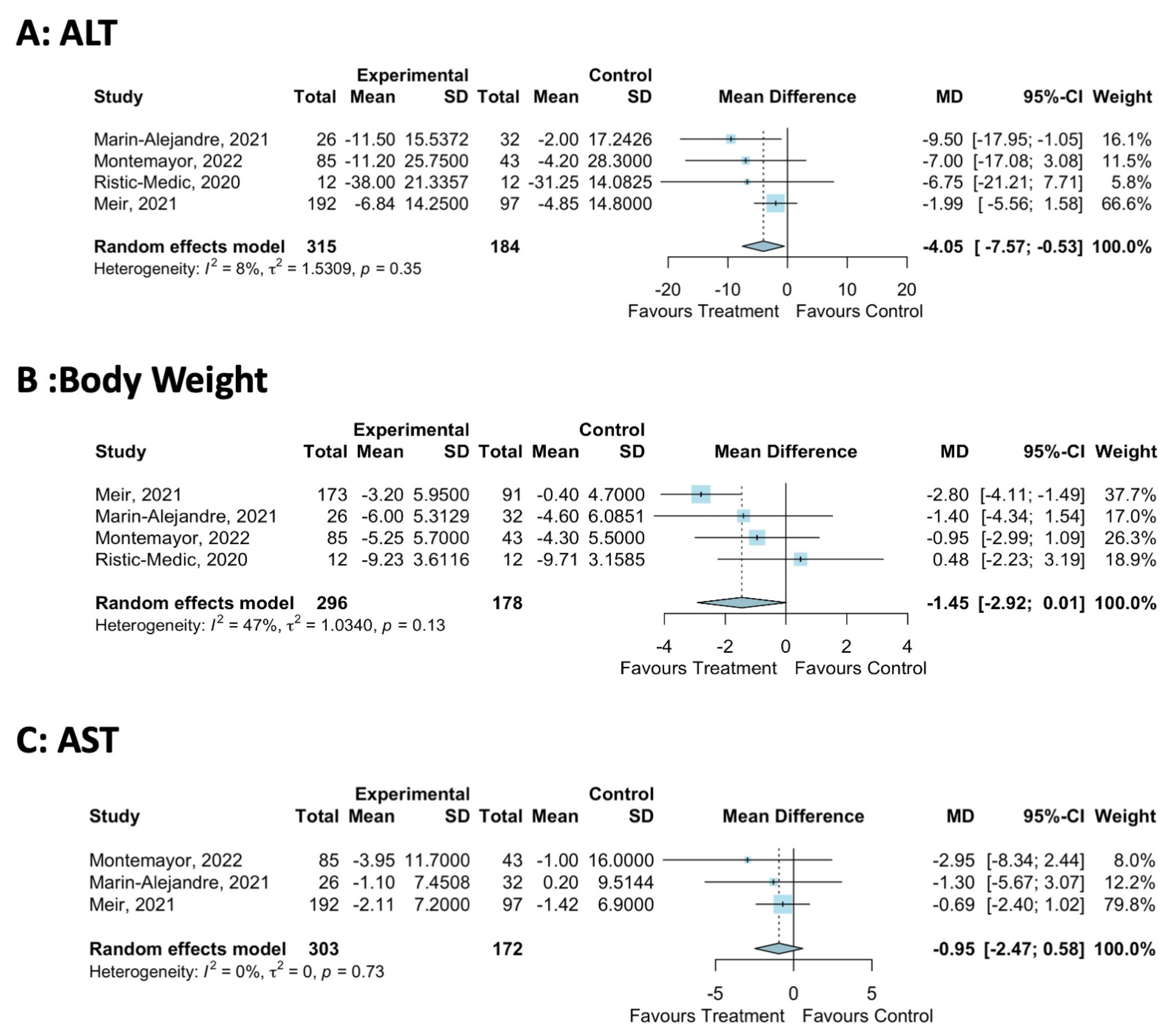
3.5.2. Primary Outcome—ALT
3.5.3. Secondary Liver Health Outcomes
3.5.4. Secondary Body Composition Outcomes
3.5.5. Sensitivity Analysis of the Effect of the Duration of the Mediterranean-LCD Intervention
3.6. Trials Assessing Green-Mediterranean LCD vs. Mediterranean-LCD and Healthy Dietary Intervention
3.6.1. Liver Health
3.6.2. Body Composition
4. Discussion
4.1. Total Dietary Replacement
4.2. Mediterranean-LCD
4.3. Green Mediterranean-LCD
4.4. Weight Loss for MASLD
4.5. Future Research
4.6. Strengths & Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Worm, N. Beyond body weight-loss: Dietary strategies targeting intrahepatic fat in NAFLD. Nutrients 2020, 12, 1316. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.V.; Newsome, P.N.; Francque, S.M.; Kanwal, F.; Terrault, N.A.; Rinella, M.E. A multi-society Delphi consensus statement on new fatty liver disease nomenclature. J. Hepatol. 2023, 79, E93–E94. [Google Scholar] [CrossRef] [PubMed]
- Armandi, A.; Schattenberg, J.M. Beyond the paradigm of weight loss in non-alcoholic fatty liver disease: From pathophysiology to novel dietary approaches. Nutrients 2021, 13, 1977. [Google Scholar] [CrossRef] [PubMed]
- Zelber-Sagi, S.; Salomone, F.; Mlynarsky, L. The Mediterranean dietary pattern as the diet of choice for non-alcoholic fatty liver disease: Evidence and plausible mechanisms. Liver Int. 2017, 37, 936–949. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL–EASD–EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef] [PubMed]
- Plauth, M.; Bernal, W.; Dasarathy, S.; Merli, M.; Plank, L.D.; Schütz, T.; Bischoff, S.C. ESPEN guideline on clinical nutrition in liver disease. Clin. Nutr. 2019, 38, 485–521. [Google Scholar] [CrossRef] [PubMed]
- Eslam, M.; Sarin, S.K.; Wong, V.W.-S.; Fan, J.-G.; Kawaguchi, T.; Ahn, S.H.; Zheng, M.-H.; Shiha, G.; Yilmaz, Y.; Gani, R.; et al. The Asian Pacific Association for the Study of the Liver clinical practice guidelines for the diagnosis and management of metabolic associated fatty liver disease. Hepatol. Int. 2020, 14, 889–919. [Google Scholar] [CrossRef] [PubMed]
- Stine, J.G.; Long, M.T.; Corey, K.E.; Sallis, R.E.; Allen, A.M.; Armstrong, M.J.; Conroy, D.E.; Cuthbertson, D.J.; Duarte-Rojo, A.; Hallsworth, K.; et al. American College of Sports Medicine (ACSM) International Multidisciplinary Roundtable report on physical activity and nonalcoholic fatty liver disease. Hepatol. Commun. 2023, 7, e0108. [Google Scholar] [CrossRef] [PubMed]
- Romeijn, M.M.; Kolen, A.M.; Holthuijsen, D.D.B.; Janssen, L.; Schep, G.; Leclercq, W.K.G.; van Dielen, F.M.H. Effectiveness of a Low-Calorie Diet for Liver Volume Reduction Prior to Bariatric Surgery: A Systematic Review. Obes. Surg. 2021, 31, 350–356. [Google Scholar] [CrossRef]
- Delbridge, E.; Proietto, J. State of the science: VLED (Very Low Energy Diet) for obesity. Asia Pac. J. Clin. Nutr. 2006, 15, 49–54. [Google Scholar]
- Opinion, S. Scientific Opinion on the essential composition of total diet replacements for weight control. EFSA J. 2015, 13, 3957. [Google Scholar] [CrossRef]
- Lean, M.E.; Leslie, W.S.; Barnes, A.C.; Brosnahan, N.; Thom, G.; McCombie, L.; Peters, C.; Zhyzhneuskaya, S.; Al-Mrabeh, A.; Hollingsworth, K.G.; et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): An open-label, cluster-randomised trial. Lancet 2018, 391, 541–551. [Google Scholar] [CrossRef]
- Taylor, R.; Al-Mrabeh, A.; Zhyzhneuskaya, S.; Peters, C.; Barnes, A.C.; Aribisala, B.S.; Hollingsworth, K.G.; Mathers, J.C.; Sattar, N.; Lean, M.E. Remission of Human Type 2 Diabetes Requires Decrease in Liver and Pancreas Fat Content but Is Dependent upon Capacity for β Cell Recovery. Cell Metab. 2018, 28, 547–556.e3. [Google Scholar] [CrossRef] [PubMed]
- Astbury, N.M.; Aveyard, P.; Nickless, A.; Hood, K.; Corfield, K.; Lowe, R.; Jebb, S.A. Doctor Referral of Overweight People to Low Energy total diet replacement Treatment (DROPLET): Pragmatic randomised controlled trial. BMJ 2018, 362, k3760. [Google Scholar] [CrossRef] [PubMed]
- Ryan, D.H.; Yockey, S.R. Weight Loss and Improvement in Comorbidity: Differences at 5%, 10%, 15%, and Over. Curr. Obes. Rep. 2017, 6, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Cho, E.E.L.; Ang, C.Z.; Quek, J.; Fu, C.E.; Lim, L.K.E.; Heng, Z.E.Q.; Tan, D.J.H.; Lim, W.H.; Yong, J.N.; Zeng, R.; et al. Global prevalence of non-alcoholic fatty liver disease in type 2 diabetes mellitus: An updated systematic review and meta-analysis. Gut 2023, 72, 2138–2148. [Google Scholar] [CrossRef]
- Dobbie, L.J.; Kassab, M.; Davison, A.S.; Grace, P.; Cuthbertson, D.J.; Hydes, T.J. Low screening rates despite a high prevalence of significant liver fibrosis in people with diabetes from primary and secondary care. J. Clin. Med. 2021, 10, 5755. [Google Scholar] [CrossRef] [PubMed]
- Semmler, G.; Datz, C.; Reiberger, T.; Trauner, M. Diet and exercise in NAFLD/NASH: Beyond the obvious. Liver Int. 2021, 41, 2249–2268. [Google Scholar] [CrossRef] [PubMed]
- Khalatbari-Soltani, S.; Imamura, F.; Brage, S.; De Lucia Rolfe, E.; Griffin, S.J.; Wareham, N.J.; Marques-Vidal, P.; Forouhi, N.G. The association between adherence to the Mediterranean diet and hepatic steatosis: Cross-sectional analysis of two independent studies, the UK Fenland Study and the Swiss CoLaus Study. BMC Med. 2019, 17, 1–14. [Google Scholar] [CrossRef]
- Kouvari, M.; Boutari, C.; Chrysohoou, C.; Fragkopoulou, E.; Antonopoulou, S.; Tousoulis, D.; Pitsavos, C.; Panagiotakos, D.; Mantzoros, C. Mediterranean diet is inversely associated with steatosis and fibrosis and decreases ten-year diabetes and cardiovascular risk in NAFLD subjects: Results from the ATTICA prospective cohort study. Clin. Nutr. 2021, 40, 3314–3324. [Google Scholar] [CrossRef]
- Rodriguez-Ramiro, I.; Vauzour, D.; Minihane, A.M. Polyphenols and non-alcoholic fatty liver disease: Impact and mechanisms. Proc. Nutr. Soc. 2016, 75, 47–60. [Google Scholar] [CrossRef] [PubMed]
- Meir, A.Y.; Rinott, E.; Tsaban, G.; Zelicha, H.; Kaplan, A.; Rosen, P.; Shelef, I.; Youngster, I.; Shalev, A.; Blüher, M.; et al. Effect of green-Mediterranean diet on intrahepatic fat: The DIRECT PLUS randomised controlled trial. Gut 2021, 70, 2085–2095. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration{\textquoteright}s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; Cochrane: London, UK, 2023; Volume 6, p. 4. [Google Scholar]
- Montemayor, S.; Bouzas, C.; Mascaró, C.M.; Casares, M.; Llompart, I.; Abete, I.; Angullo-Martinez, E.; Zulet, M.; Martínez, J.A.; Tur, J.A. Effect of Dietary and Lifestyle Interventions on the Amelioration of NAFLD in Patients with Metabolic Syndrome: The FLIPAN Study. Nutrients 2022, 14, 2223. [Google Scholar] [CrossRef] [PubMed]
- Tsaban, G.; Meir, A.Y.; Rinott, E.; Zelicha, H.; Kaplan, A.; Shalev, A.; Katz, A.; Rudich, A.; Tirosh, A.; Shelef, I.; et al. The effect of green Mediterranean diet on cardiometabolic risk; a randomised controlled trial. Heart 2021, 107, 1054–1061. [Google Scholar] [CrossRef] [PubMed]
- Gepner, Y.; Shelef, I.; Komy, O.; Cohen, N.; Schwarzfuchs, D.; Bril, N.; Rein, M.; Serfaty, D.; Kenigsbuch, S.; Zelicha, H.; et al. The beneficial effects of Mediterranean diet over low-fat diet may be mediated by decreasing hepatic fat content. J. Hepatol. 2019, 71, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Gepner, Y.; Shelef, I.; Schwarzfuchs, D.; Zelicha, H.; Tene, L.; Meir, A.Y.; Tsaban, G.; Cohen, N.; Bril, N.; Rein, M.; et al. Effect of distinct lifestyle interventions on mobilization of fat storage pools CENTRAL magnetic resonance imaging randomized controlled trial. Circulation 2018, 137, 1143–1157. [Google Scholar] [CrossRef] [PubMed]
- Marin-Alejandre, B.A.; Abete, I.; Cantero, I.; Monreal, J.I.; Elorz, M.; Herrero, J.I.; Benito-Boillos, A.; Quiroga, J.; Martinez-Echeverria, A.; Uriz-Otano, J.I.; et al. The metabolic and hepatic impact of two personalized dietary strategies in subjects with obesity and nonalcoholic fatty liver disease: The fatty liver in obesity (FLiO) randomized controlled trial. Nutrients 2019, 11, 2543. [Google Scholar] [CrossRef]
- Marin-Alejandre, B.A.; Cantero, I.; Perez-Diaz-Del-Campo, N.; Monreal, J.I.; Elorz, M.; Herrero, J.I.; Benito-Boillos, A.; Quiroga, J.; Martinez-Echeverria, A.; Uriz-Otano, J.I.; et al. Effects of two personalized dietary strategies during a 2-year intervention in subjects with nonalcoholic fatty liver disease: A randomized trial. Liver Int. 2021, 41, 1532–1544. [Google Scholar] [CrossRef]
- Browning, J.D.; Baker, J.A.; Rogers, T.; Davis, J.; Satapati, S.; Burgess, S.C. Short-term weight loss and hepatic triglyceride reduction: Evidence of a metabolic advantage with dietary carbohydrate restriction. Am. J. Clin. Nutr. 2011, 93, 1048–1052. [Google Scholar] [CrossRef]
- Cunha, G.M.; Guzman, G.; De Mello, L.L.C.; Trein, B.; Spina, L.; Bussade, I.; Prata, J.M.; Sajoux, I.; Countinho, W. Efficacy of a 2-Month Very Low-Calorie Ketogenic Diet (VLCKD) Compared to a Standard Low-Calorie Diet in Reducing Visceral and Liver Fat Accumulation in Patients With Obesity. Front. Endocrinol. 2020, 11, 607. [Google Scholar] [CrossRef]
- Ristic-Medic, D.; Kovacic, M.; Takic, M.; Arsic, A.; Petrovic, S.; Paunovic, M.; Jovicic, M.; Vucic, V. Calorie-Restricted Mediterranean and Low-Fat Diets Affect. Nutrients 2020, 13, 15. [Google Scholar] [CrossRef]
- Aller, R.; De Luis, D.A.; Izaola, O.; De La Fuente, B.; Bachiller, R. Effect of a high monounsaturated vs high polyunsaturated fat hypocaloric diets in nonalcoholic fatty liver disease. Eur. Rev. Med. Pharmacol. Sci. 2014, 18, 1041–1047. [Google Scholar]
- Chen, J.; Huang, Y.; Xie, H.; Bai, H.; Lin, G.; Dong, Y.; Shi, D.; Wang, J.; Zhang, Q.; Zhang, Y.; et al. Impact of a low-carbohydrate and high-fiber diet on nonalcoholic fatty liver disease. Asia Pac. J. Clin. Nutr. 2020, 29, 483–490. [Google Scholar] [CrossRef]
- Elias, M.C.; Parise, E.R.; de Carvalho, L.; Szejnfeld, D.; Netto, J.P. Effect of 6-month nutritional intervention on non-alcoholic fatty liver disease. Nutrition 2010, 26, 1094–1099. [Google Scholar] [CrossRef]
- Abd El-Kader, S.M.; Al-Shreef, F.M.; Al-Jiffri, O.H. Biochemical parameters response to weight loss in patients with non-alcoholic steatohepatitis. Afr. Health Sci. 2016, 16, 242–249. [Google Scholar] [CrossRef]
- Promrat, K.; Kleiner, D.E.; Niemeier, H.M.; Jackvony, E.; Kearns, M.; Wands, J.R.; Fava, J.L.; Wing, R.R. Randomized controlled trial testing the effects of weight loss on nonalcoholic steatohepatitis. Hepatology 2009, 51, 121–129. [Google Scholar] [CrossRef]
- Sattar, N.; Welsh, P.; Leslie, W.S.; Thom, G.; McCombie, L.; Brosnahan, N.; Richardson, J.; Gill, J.M.; Crawford, L.; Lean, M.E. Dietary Weight-Management for Type 2 Diabetes Remissions in South Asians: The South Asian Diabetes Remission FeasiBilitY And Randomised Trial (STANDby). Lancet Reg. Health-Southeast Asia 2022, 9, 100111. [Google Scholar] [CrossRef]
- Asghari, S.; Rezaei, M.; Rafraf, M.; Taghizadeh, M.; Asghari-Jafarabadi, M.; Ebadi, M. Effects of Calorie Restricted Diet on Oxidative/Antioxidative Status Biomarkers and Serum Fibroblast Growth Factor 21 Levels in Nonalcoholic Fatty Liver Disease Patients: A Randomized, Controlled Clinical Trial. Nutrients 2022, 14, 2509. [Google Scholar] [CrossRef]
- Al-Mrabeh, A.; Zhyzhneuskaya, S.V.; Peters, C.; Barnes, A.C.; Melhem, S.; Jesuthasan, A.; Aribisala, B.; Hollingsworth, K.G.; Lietz, G.; Mathers, J.C.; et al. Hepatic Lipoprotein Export and Remission of Human Type 2 Diabetes after Weight Loss. Cell Metab. 2020, 31, 233–249.e4. [Google Scholar] [CrossRef]
- Razavi Zade, M.; Telkabadi, M.H.; Bahmani, F.; Salehi, B.; Farshbaf, S.; Asemi, Z. The effects of DASH diet on weight loss and metabolic status in adults with non-alcoholic fatty liver disease: A randomized clinical trial. Liver Int. 2016, 36, 563–571. [Google Scholar] [CrossRef]
- Luukkonen, P.K.; Dufour, S.; Lyu, K.; Zhang, X.-M.; Hakkarainen, A.; Lehtimäki, T.E.; Cline, G.W.; Petersen, K.F.; Shulman, G.I.; Yki-Järvinen, H. Effect of a ketogenic diet on hepatic steatosis and hepatic mitochondrial metabolism in nonalcoholic fatty liver disease. Proc. Natl. Acad. Sci. USA 2020, 117, 7347–7354. [Google Scholar] [CrossRef]
- Ryan, M.C.; Abbasi, F.; Lamendola, C.; Carter, S.; McLaughlin, T.L. Serum Alanine Aminotransferase Levels Decrease Further With Carbohydrate Than Fat Restriction in Insulin-Resistant Adults. Diabetes Care 2007, 30, 1075–1080. [Google Scholar] [CrossRef]
- Scragg, J.; Avery, L.; Cassidy, S.; Taylor, G.; Haigh, L.; Boyle, M.; Trenell, M.I.; Anstee, Q.M.; McPherson, S.; Hallsworth, K. Feasibility of a Very Low Calorie Diet to Achieve a Sustainable 10% Weight Loss in Patients With Nonalcoholic Fatty Liver Disease. Clin. Transl. Gastroenterol. 2020, 11, e00231. [Google Scholar] [CrossRef]
- Larson-Meyer, D.E.; Newcomer, B.R.; Heilbronn, L.K.; Volaufova, J.; Smith, S.R.; Alfonso, A.J.; Lefevre, M.; Rood, J.C.; Williamson, D.A.; Ravussin, E.; et al. Effect of 6-month calorie restriction and exercise on serum and liver lipids and markers of liver function. Obesity 2008, 16, 1355–1362. [Google Scholar] [CrossRef]
- Guo, X.; Xu, Y.; He, H.; Cai, H.; Zhang, J.; Li, Y.; Yan, X.; Zhang, M.; Zhang, N.; Maddela, R.L.; et al. Effects of a Meal Replacement on Body Composition and Metabolic Parameters among Subjects with Overweight or Obesity. J. Obes. 2018, 2018, 2837367. [Google Scholar] [CrossRef]
- Shirai, K.; Saiki, A.; Oikawa, S.; Teramoto, T.; Yamada, N.; Ishibashi, S.; Tada, N.; Miyazaki, S.; Inoue, I.; Murano, S.; et al. The effects of partial use of formula diet on weight reduction and metabolic variables in obese type 2 diabetic patients—Multicenter trial. Obes. Res. Clin. Pract. 2013, 7, e43–e54. [Google Scholar] [CrossRef]
- Taheri, S.; Zaghloul, H.; Chagoury, O.; Elhadad, S.; Ahmed, S.H.; El Khatib, N.; Amona, R.A.; El Nahas, K.; Suleiman, N.; Alnaama, A.; et al. Effect of intensive lifestyle intervention on bodyweight and glycaemia in early type 2 diabetes (DIADEM-I): An open-label, parallel-group, randomised controlled trial. Lancet Diabetes Endocrinol. 2020, 8, 477–489. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef] [PubMed]
- Mazidi, M.; Kengne, A.P. Higher adherence to plant-based diets are associated with lower likelihood of fatty liver. Clin. Nutr. 2019, 38, 1672–1677. [Google Scholar] [CrossRef]
- Zhang, S.; Fu, J.; Zhang, Q.; Liu, L.; Meng, G.; Yao, Z.; Wu, H.; Bao, X.; Gu, Y.; Lu, M.; et al. Association between nut consumption and non-alcoholic fatty liver disease in adults. Liver Int. 2019, 39, 1732–1741. [Google Scholar] [CrossRef]
- Baratta, F.; Pastori, D.; Polimeni, L.; Bucci, T.; Ceci, F.; Calabrese, C.; Ernesti, I.; Pannitteri, G.; Violi, F.; Angelico, F.; et al. Adherence to Mediterranean Diet and Non-Alcoholic Fatty Liver Disease: Effect on Insulin Resistance. Am. J. Gastroenterol. 2017, 112, 1832–1839. [Google Scholar] [CrossRef] [PubMed]
- Trovato, F.M.; Catalano, D.; Martines, G.F.; Pace, P.; Trovato, G.M. Mediterranean diet and non-alcoholic fatty liver disease: The need of extended and comprehensive interventions. Clin. Nutr. 2015, 34, 86–88. [Google Scholar] [CrossRef]
- Yang, Y.; Zhang, D.; Feng, N.; Chen, G.; Liu, J.; Chen, G.; Zhu, Y. Increased intake of vegetables, but not fruit, reduces risk for hepatocellular carcinoma: A meta-analysis. Gastroenterology 2014, 147, 1031–1042. [Google Scholar] [CrossRef]
- Salomone, F.; Godos, J.; Zelber-Sagi, S. Natural antioxidants for non-alcoholic fatty liver disease: Molecular targets and clinical perspectives. Liver Int. 2016, 36, 5–20. [Google Scholar] [CrossRef] [PubMed]
- Rinott, E.; Meir, A.Y.; Tsaban, G.; Zelicha, H.; Kaplan, A.; Knights, D.; Tuohy, K.; Scholz, M.U.; Koren, O.; Stampfer, M.J.; et al. The effects of the Green-Mediterranean diet on cardiometabolic health are linked to gut microbiome modifications: A randomized controlled trial. Genome Med. 2022, 14, 29. [Google Scholar] [CrossRef] [PubMed]
- Mouries, J.; Brescia, P.; Silvestri, A.; Spadoni, I.; Sorribas, M.; Wiest, R.; Mileti, E.; Galbiati, M.; Invernizzi, P.; Adorini, L.; et al. Microbiota-driven gut vascular barrier disruption is a prerequisite for non-alcoholic steatohepatitis development. J. Hepatol. 2019, 71, 1216–1228. [Google Scholar] [CrossRef]
- Kolodziejczyk, A.A.; Zheng, D.; Shibolet, O.; Elinav, E. The role of the microbiome in NAFLD and NASH. EMBO Mol. Med. 2019, 11, e9302. [Google Scholar] [CrossRef]
- Wu, G.D.; Chen, J.; Hoffmann, C.; Bittinger, K.; Chen, Y.-Y.; Keilbaugh, S.A.; Bewtra, M.; Knights, D.; Walters, W.A.; Knight, R.; et al. Linking long-term dietary patterns with gut microbial enterotypes. Science 2011, 334, 105–108. [Google Scholar] [CrossRef]
- Verrastro, O.; Panunzi, S.; Castagneto-Gissey, L.; De Gaetano, A.; Lembo, E.; Capristo, E.; Guidone, C.; Angelini, G.; Pennestrì, F.; Sessa, L.; et al. Bariatric–metabolic surgery versus lifestyle intervention plus best medical care in non-alcoholic steatohepatitis (BRAVES): A multicentre, open-label, randomised trial. Lancet 2023, 401, 1786–1797. [Google Scholar] [CrossRef]
- Loomba, R.; Abdelmalek, M.F.; Armstrong, M.J.; Jara, M.; Kjær, M.S.; Krarup, N.; Lawitz, E.; Ratziu, V.; Sanyal, A.J.; Schattenberg, J.M.; et al. Semaglutide 2·4 mg once weekly in patients with non-alcoholic steatohepatitis-related cirrhosis: A randomised, placebo-controlled phase 2 trial. Lancet Gastroenterol. Hepatol. 2023, 8, 511–522. [Google Scholar] [CrossRef] [PubMed]
- Farhat, G.; Majeed, S.; Rutter, M.K.; Issa, B.; Harvie, M. Comparing the acceptability of total diet replacement and food-based low energy diets for type 2 diabetes remission amongst South Asians: A public and patient involvement activity. NIHR Open Res. 2022, 1, 24. [Google Scholar] [CrossRef] [PubMed]
- Pouwels, S.; Sakran, N.; Graham, Y.; Leal, A.; Pintar, T.; Yang, W.; Kassir, R.; Singhal, R.; Mahawar, K.; Ramnarain, D. Non-alcoholic fatty liver disease (NAFLD): A review of pathophysiology, clinical management and effects of weight loss. BMC Endocr. Disord. 2022, 22, 63. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intervention | Definition/Description |
|---|---|
| Low-Calorie Diet (LCD) | One of (A) 800–1500 kcal/day; (B) 500 kcal/day calorie reduction or (C) 25% reduction in calories from baseline |
| Very-Low-Calorie Diet (VLCD) | One of: (A) 450–800 kcal/day; (B) 1200 kcal/day calorie reduction; (C) 60% reduction in calories from baseline |
| Total-Dietary Replacement (TDR) | Very-Low-Calorie Diet utilising nutritionally complete meal replacements. This includes 3 months of total-meal replacement followed by structured food reintroduction for 2 to 8 weeks. |
| Mediterranean Low-Calorie Diet (MED-LCD) | Low-Calorie Diet, which follows the Mediterranean dietary pattern, i.e., a minimal consumption of processed/ultra-processed foods and a high consumption of whole grains, nuts, legumes, olive oil, vegetables and fruits. |
| Green Mediterranean Low-Calorie diet (GREEN-MED-LCD) | Low-Calorie Diet, which follows a green Mediterranean dietary pattern, i.e., a minimal consumption of processed/ultra-processed foods and a high consumption of whole grains, nuts, legumes, olive oil, vegetables and fruits. In addition, this is supplemented with foods high in dietary polyphenols, i.e., walnuts, green tea and Mankai. |
| Low-Carbohydrate Diet | Low-Calorie Diet which limits carbohydrate intake to <20 g/day. |
| Low-Calorie Diet—Polyunsaturated fatty acids | Low-Calorie Diet enriched in polyunsaturated fatty acids. |
| Low-Calorie Diet—Monounsaturated fatty acids | Low-Calorie diet enriched in monounsaturated fatty acids. |
| Very-Low-Calorie Ketogenic Diet | VLCD for 2 months, inducing ketogenesis. Consists of LCD (600–800 kcal/day) and is low in carbohydrates (<50 g/day) and lipids (10 g of olive oil/day) |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Randomised Controlled trial or cohort study | Not original research (excluding reviews, case reports and practice guidelines) |
| Participants Aged ≥ 18 years old | Not a Human Study |
| Presence of NAFLD or MASLD * | Does not report primary and/or secondary outcomes |
| Participants with overweight or obesity | No Comparator Group (i.e., control or alternative dietary intervention) |
| Reported in English | Non-English language publication |
| Treated with a Low-Calorie Diet or Very-Low-Calorie Diet Intervention |
| Comparison | Study | Design | N | Duration (Months) | Location | Sex (% Male) | Age (Years ± SD) | Ethnicity | |
|---|---|---|---|---|---|---|---|---|---|
| LCD vs. Control | Non-TDR | Asghari, 2022 [41] | RCT | 60 | 3 m | Iran | 65% M | 39.7 ± 6.3 y | Middle-Eastern ^ |
| Chen, 2020 [36] | RCT | 44 | 2 m | China | 63.6% M | 38.1 ± 9.4 y | East Asian ^ | ||
| Elias, 2010 [37] | Cohort | 31 | 6 m | Brazil | 48.3% M | 47.5 ± 11.6 y | Hispanic and Latino ^ | ||
| El-Kader, 2016 [38] | RCT | 100 | 3 m | Saudi Arabia | 70% M | 51.0 ± 5.6 y | Middle Eastern ^ | ||
| Promrat, 2009 [39] | RCT | 31 | 11 m | USA | 70.9% M | 48.5 ± 11.3 y | 84% Caucasian | ||
| TDR | Taylor, 2018 DIRECT [12,13] | RCT | 90/306 a | 12 m | UK | 57.8% M | 52.8 ± 7.9 y | 98.3% Caucasian | |
| Sattar, 2022 STAND-BY [40] | RCT | 25 | 3 m | UK | 52% M | 45.8 ± 11.1 y | South Asian | ||
| MED-LCD vs. Control or other LCD | Gepner, 2018/2019 CENTRAL [28,29] | RCT | 278 | 18 m | Israel | 89% M | 47.9 ± 9.3 y | Middle Eastern ^ | |
| Marin-Alejandre, 2019/2021FLiO [30,31] | RCT | 98 | 6–24 m | Spain | 52% M | 50.1 ± 9.3 y | Caucasian ^ | ||
| Montemayor, 2022 FLIPAN [26] | RCT | 128 b | 12 m | Spain | 63.3% M | 52.9 ± 7.27 y | Caucasian ^ | ||
| Ristic-Medic, 2020 [34] | RCT | 27 | 3 m | Serbia | 100% M | 33.6 ± 4.2 y | Caucasian ^ | ||
| Green-MED-LCD vs. MED-LCD or HDG | Meir, 2019/2021 DIRECT-PLUS [22,27] | RCT | 294 | 18 m | Israel | 88.1% M | 51.1 ± 10.5 y | Middle Eastern ^ | |
| Low-Carb LCD vs. LCD | Browning, 2011 [32] | Non-RCT * | 18 | 0.5 m | USA | 27.8% M | 44.5 ± 11.5 y | Not Stated | |
| VLCKD vs. LCD | Cunha, 2020 [33] | RCT | 46 | 2 m | Brazil | 17.4% M | 40.3 ± 11.3 y | Hispanic and Latino ^ | |
| LCD MUF vs. PUF | Aller, 2014 [35] | RCT | 44 | 3 m | Spain | 28.1% M | 49.3 ± 16.7 y | Caucasian ^ | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dobbie, L.J.; Burgess, J.; Hamid, A.; Nevitt, S.J.; Hydes, T.J.; Alam, U.; Cuthbertson, D.J. Effect of a Low-Calorie Dietary Intervention on Liver Health and Body Weight in Adults with Metabolic-Dysfunction Associated Steatotic Liver Disease (MASLD) and Overweight/Obesity: A Systematic Review and Meta-Analysis. Nutrients 2024, 16, 1030. https://doi.org/10.3390/nu16071030
Dobbie LJ, Burgess J, Hamid A, Nevitt SJ, Hydes TJ, Alam U, Cuthbertson DJ. Effect of a Low-Calorie Dietary Intervention on Liver Health and Body Weight in Adults with Metabolic-Dysfunction Associated Steatotic Liver Disease (MASLD) and Overweight/Obesity: A Systematic Review and Meta-Analysis. Nutrients. 2024; 16(7):1030. https://doi.org/10.3390/nu16071030
Chicago/Turabian StyleDobbie, Laurence J., Jamie Burgess, Azlinda Hamid, Sarah J. Nevitt, Theresa J. Hydes, Uazman Alam, and Daniel J. Cuthbertson. 2024. "Effect of a Low-Calorie Dietary Intervention on Liver Health and Body Weight in Adults with Metabolic-Dysfunction Associated Steatotic Liver Disease (MASLD) and Overweight/Obesity: A Systematic Review and Meta-Analysis" Nutrients 16, no. 7: 1030. https://doi.org/10.3390/nu16071030
APA StyleDobbie, L. J., Burgess, J., Hamid, A., Nevitt, S. J., Hydes, T. J., Alam, U., & Cuthbertson, D. J. (2024). Effect of a Low-Calorie Dietary Intervention on Liver Health and Body Weight in Adults with Metabolic-Dysfunction Associated Steatotic Liver Disease (MASLD) and Overweight/Obesity: A Systematic Review and Meta-Analysis. Nutrients, 16(7), 1030. https://doi.org/10.3390/nu16071030