
Inter-Individual Responses to a Blueberry Intervention across Multiple Endpoints


Abstract

1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Treatment
2.3. Clinical Endpoints
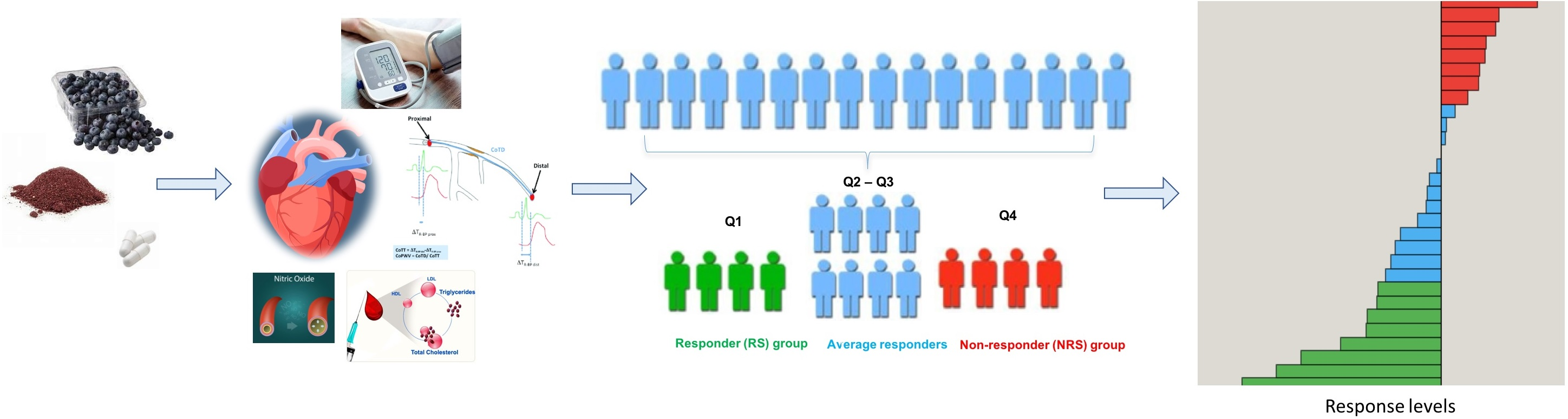
2.4. Characterising Responses to Interventions
2.5. Metabolite Profiling
2.6. Characterisation and Identification of Discriminating Features
3. Results
3.1. Baseline Characteristics
3.2. Interventional Effect on Clinical Endpoints
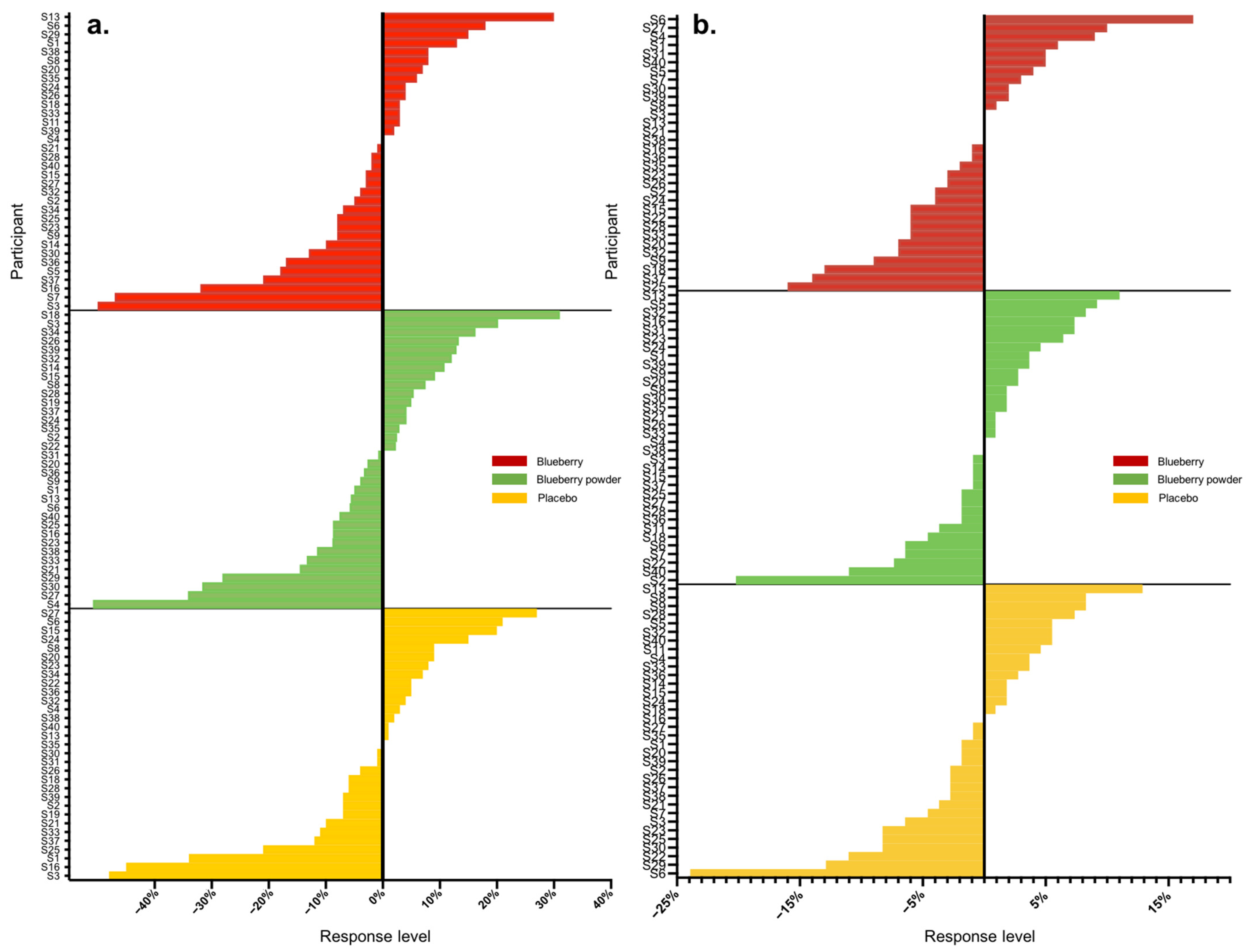
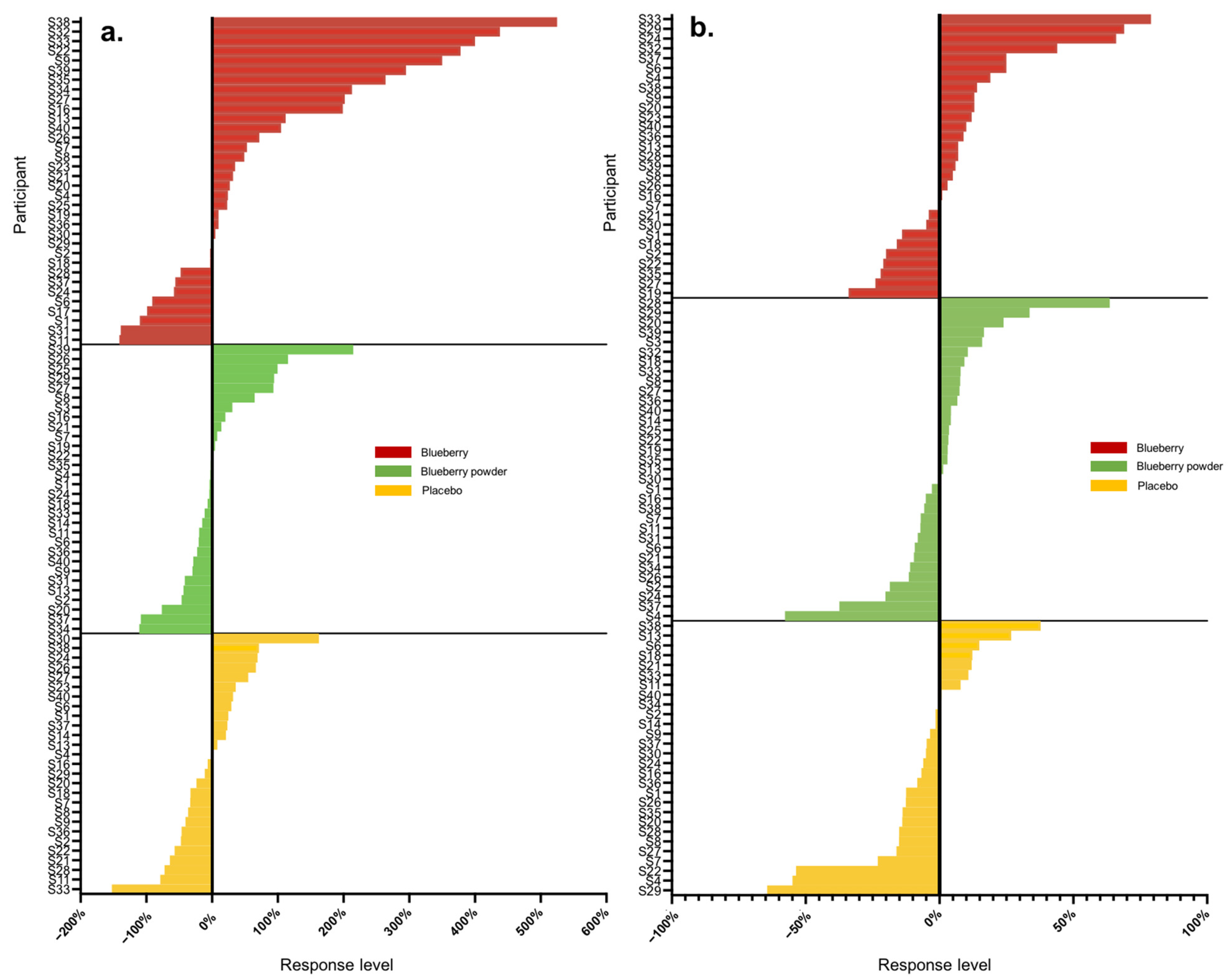
3.3. Inter-Individual Variation in Endpoints
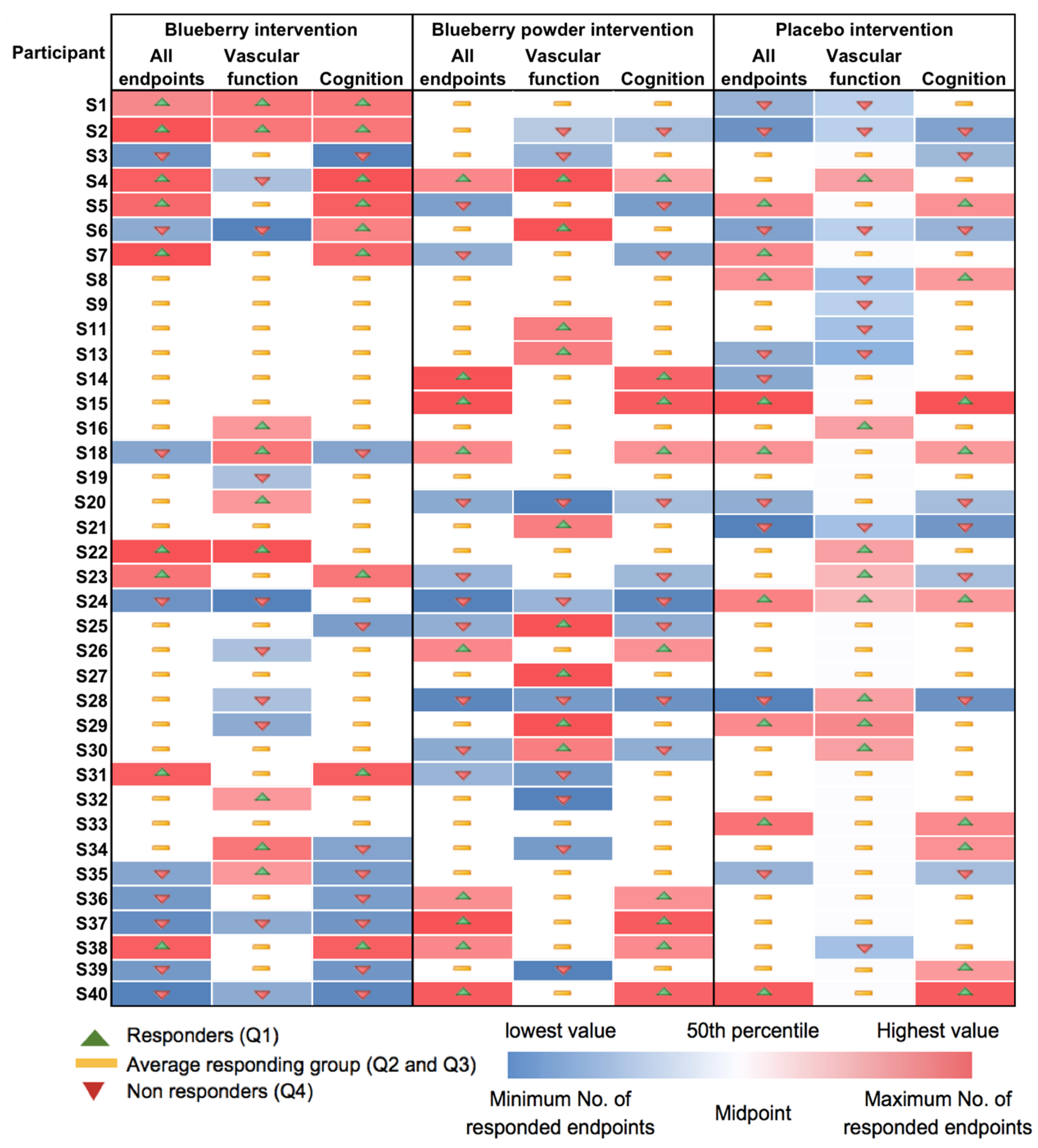
3.4. Characterisation of Responder and Non-Responder Groups
4. Discussion
4.1. Inter-Individual Variation in Responses of Clinical Endpoints
4.2. Consistency of Response
4.3. Predictors of Response
4.4. Methodological Factors Influencing Inter-Individual Variation
4.5. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Manach, C.; Milenkovic, D.; Van de Wiele, T.; Rodriguez-Mateos, A.; de Roos, B.; Garcia-Conesa, M.T.; Landberg, R.; Gibney, E.R.; Heinonen, M.; Tomas-Barberan, F.; et al. Addressing the inter-individual variation in response to consumption of plant food bioactives: Towards a better understanding of their role in healthy aging and cardiometabolic risk reduction. Mol. Nutr. Food Res. 2017, 61, 1600557. [Google Scholar] [CrossRef]
- Lampe, J.W.; Navarro, S.L.; Hullar, M.A.; Shojaie, A. Inter-individual differences in response to dietary intervention: Integrating omics platforms towards personalised dietary recommendations. Proc. Nutr. Soc. 2013, 72, 207–218. [Google Scholar] [CrossRef]
- Ostertag, L.M.; Kroon, P.A.; Wood, S.; Horgan, G.W.; Cienfuegos-Jovellanos, E.; Saha, S.; Duthie, G.G.; de Roos, B. Flavan-3-ol-enriched dark chocolate and white chocolate improve acute measures of platelet function in a gender-specific way--a randomized-controlled human intervention trial. Mol. Nutr. Food Res. 2013, 57, 191–202. [Google Scholar] [CrossRef]
- Zinck, J.W.; de Groh, M.; MacFarlane, A.J. Genetic modifiers of folate, vitamin B-12, and homocysteine status in a cross-sectional study of the Canadian population. Am. J. Clin. Nutr. 2015, 101, 1295–1304. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.J.; Jackson, K.G.; Dadd, T.; Mayes, A.E.; Brown, A.L.; Lovegrove, J.A.; Minihane, A.M. The impact of the catechol-O-methyltransferase genotype on vascular function and blood pressure after acute green tea ingestion. Mol. Nutr. Food Res. 2012, 56, 966–975. [Google Scholar] [CrossRef]
- Arumugam, M.; Raes, J.; Pelletier, E.; Le Paslier, D.; Yamada, T.; Mende, D.R.; Fernandes, G.R.; Tap, J.; Bruls, T.; Batto, J.M.; et al. Enterotypes of the human gut microbiome. Nature 2011, 473, 174–180. [Google Scholar] [CrossRef]
- Espin, J.C.; Gonzalez-Sarrias, A.; Tomas-Barberan, F.A. The gut microbiota: A key factor in the therapeutic effects of (poly)phenols. Biochem. Pharmacol. 2017, 139, 82–93. [Google Scholar] [CrossRef] [PubMed]
- Rowland, I.; Gibson, G.; Heinken, A.; Scott, K.; Swann, J.; Thiele, I.; Tuohy, K. Gut microbiota functions: Metabolism of nutrients and other food components. Eur. J. Nutr. 2018, 57, 1–24. [Google Scholar] [CrossRef]
- Wang, Y.; Lara, J.; Haskell-Ramsay, C.; Lodge, J.K. Effects of chronic consumption of specific fruit (berries, citrus and cherries) on CVD risk factors: A systematic review and meta-analysis of randomised controlled trials. Eur. J. Nutr. 2020, 60, 615–639. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Haskell-Ramsay, C.; Gallegos, J.L.; Lodge, J.K. Effects of chronic consumption of specific fruit (berries, cherries and citrus) on cognitive health: A systematic review and meta-analysis of randomised controlled trials. Eur. J. Clin. Nutr. 2023, 77, 7–22. [Google Scholar] [CrossRef]
- Garcia-Perez, I.; Posma, J.M.; Chambers, E.S.; Mathers, J.C.; Draper, J.; Beckmann, M.; Nicholson, J.K.; Holmes, E.; Frost, G. Dietary metabotype modelling predicts individual responses to dietary interventions. Nat. Food 2020, 1, 355–364. [Google Scholar] [CrossRef]
- Kalt, W.; Cassidy, A.; Howard, L.R.; Krikorian, R.; Stull, A.J.; Tremblay, F.; Zamora-Ros, R. Recent Research on the Health Benefits of Blueberries and Their Anthocyanins. Adv. Nutr. 2020, 11, 224–236. [Google Scholar] [CrossRef]
- Wang, Y.; Gallegos, J.L.; Haskell-Ramsay, C.; Lodge, J.K. Effects of Blueberry Consumption on Cardiovascular Health in Healthy Adults: A Cross-Over Randomised Controlled Trial. Nutrients 2022, 14, 2562. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, A.; O’Reilly, É.J.; Kay, C.; Sampson, L.; Franz, M.; Forman, J.P.; Curhan, G.; Rimm, E.B. Habitual intake of flavonoid subclasses and incident hypertension in adults. Am. J. Clin. Nutr. 2011, 93, 338–347. [Google Scholar] [CrossRef] [PubMed]
- Wedick, N.M.; Pan, A.; Cassidy, A.; Rimm, E.B.; Sampson, L.; Rosner, B.; Willett, W.; Hu, F.B.; Sun, Q.; van Dam, R.M. Dietary flavonoid intakes and risk of type 2 diabetes in US men and women. Am. J. Clin. Nutr. 2012, 95, 925–933. [Google Scholar] [CrossRef] [PubMed]
- Haskell-Ramsay, C.F.; Stuart, R.C.; Okello, E.J.; Watson, A.W. Cognitive and mood improvements following acute supplementation with purple grape juice in healthy young adults. Eur. J. Nutr. 2017, 56, 2621–2631. [Google Scholar] [CrossRef] [PubMed]
- Del Bo, C.; Porrini, M.; Fracassetti, D.; Campolo, J.; Klimis-Zacas, D.; Riso, P. A single serving of blueberry (V. corymbosum) modulates peripheral arterial dysfunction induced by acute cigarette smoking in young volunteers: A randomized-controlled trial. Food Funct. 2014, 5, 3107–3116. [Google Scholar] [CrossRef] [PubMed]
- Schrager, M.A.; Hilton, J.; Gould, R.; Kelly, V.E. Effects of blueberry supplementation on measures of functional mobility in older adults. Appl. Physiol. Nutr. Metab. 2015, 40, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Townsend, R.R.; Wilkinson, I.B.; Schiffrin, E.L.; Avolio, A.P.; Chirinos, J.A.; Cockcroft, J.R.; Heffernan, K.S.; Lakatta, E.G.; McEniery, C.M.; Mitchell, G.F.; et al. Recommendations for Improving and Standardizing Vascular Research on Arterial Stiffness: A Scientific Statement From the American Heart Association. Hypertension 2015, 66, 698–722. [Google Scholar] [CrossRef]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Watson, A.W.; Haskell-Ramsay, C.F.; Kennedy, D.O.; Cooney, J.M.; Trower, T.; Scheepens, A. Acute supplementation with blackcurrant extracts modulates cognitive functioning and inhibits monoamine oxidase-B in healthy young adults. J. Funct. Foods 2015, 17, 524–539. [Google Scholar] [CrossRef]
- Kimble, R.; Keane, K.M.; Lodge, J.K.; Howatson, G. The Influence of Tart Cherry (Prunus cerasus, cv Montmorency) Concentrate Supplementation for 3 Months on Cardiometabolic Risk Factors in Middle-Aged Adults: A Randomised, Placebo-Controlled Trial. Nutrients 2021, 13, 1417. [Google Scholar] [CrossRef]
- Xia, J.; Wishart, D.S. Using MetaboAnalyst 3.0 for comprehensive metabolomics data analysis. Curr. Protoc. Bioinform. 2016, 55, 14.10.1–14.10.91. [Google Scholar] [CrossRef]
- Hackstadt, A.J.; Hess, A.M. Filtering for increased power for microarray data analysis. BMC Bioinform. 2009, 10, 11. [Google Scholar] [CrossRef]
- van den Berg, R.A.; Hoefsloot, H.C.J.; Westerhuis, J.A.; Smilde, A.K.; van der Werf, M.J. Centering, scaling, and transformations: Improving the biological information content of metabolomics data. BMC Genom. 2006, 7, 142. [Google Scholar] [CrossRef]
- Al Hasani, S.; Al-Attabi, Z.; Waly, M.; Al-Habsi, N.; Al-Subhi, L.; Shafiur Rahman, M. Polyphenol and Flavonoid Stability of Wild Blueberry (Sideroxylon mascatense) during Air- and Freeze-Drying and Storage Stability as a Function of Temperature. Foods 2023, 12, 871. [Google Scholar] [CrossRef]
- Hatami, T.; Emami, S.A.; Miraghaee, S.S.; Mojarrab, M. Total Phenolic Contents and Antioxidant Activities of Different Extracts and Fractions from the Aerial Parts of Artemisia biennis Willd. Iran. J. Pharm. Res. 2014, 13, 551–559. [Google Scholar] [PubMed]
- Kelly, J.; Vanhatalo, A.; Bailey, S.J.; Wylie, L.J.; Tucker, C.; List, S.; Winyard, P.G.; Jones, A.M. Dietary nitrate supplementation: Effects on plasma nitrite and pulmonary O2 uptake dynamics during exercise in hypoxia and normoxia. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2014, 307, R920–R930. [Google Scholar] [CrossRef] [PubMed]
- Scholey, A.B.; French, S.J.; Morris, P.J.; Kennedy, D.O.; Milne, A.L.; Haskell, C.F. Consumption of cocoa flavanols results in acute improvements in mood and cognitive performance during sustained mental effort. J. Psychopharmacol. 2010, 24, 1505–1514. [Google Scholar] [CrossRef] [PubMed]
- Keane, K.; Haskell-Ramsay, C.; Veasey, R.; Howatson, G. Montmorency Tart cherries (Prunus cerasus L.) modulate vascular function acutely, in the absence of improvement in cognitive performance. Br. J. Nutr. 2016, 116, 1935–1944. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Pase, M.; Pipingas, A.; Raubenheimer, J.; Thurgood, M.; Villalon, L.; Macpherson, H.; Gibbs, A.; Scholey, A. Switching to a 10-day Mediterranean-style diet improves mood and cardiovascular function in a controlled crossover study. Nutrition 2015, 31, 647–652. [Google Scholar] [CrossRef]
- Miller, M.G.; Hamilton, D.A.; Joseph, J.A.; Shukitt-Hale, B. Dietary blueberry improves cognition among older adults in a randomized, double-blind, placebo-controlled trial. Eur. J. Nutr. 2018, 57, 1169–1180. [Google Scholar] [CrossRef] [PubMed]
- Bowtell, J.L.; Aboo-Bakkar, Z.; Conway, M.E.; Adlam, A.R.; Fulford, J. Enhanced task-related brain activation and resting perfusion in healthy older adults after chronic blueberry supplementation. Appl. Physiol. Nutr. Metab. 2017, 42, 773–779. [Google Scholar] [CrossRef] [PubMed]
- Boespflug, E.L.; Eliassen, J.C.; Dudley, J.A.; Shidler, M.D.; Kalt, W.; Summer, S.S.; Stein, A.L.; Stover, A.N.; Krikorian, R. Enhanced neural activation with blueberry supplementation in mild cognitive impairment. Nutr. Neurosci. 2018, 21, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Corriveau, R.A.; Bosetti, F.; Emr, M.; Gladman, J.T.; Koenig, J.I.; Moy, C.S.; Pahigiannis, K.; Waddy, S.P.; Koroshetz, W. The science of vascular contributions to cognitive impairment and dementia (VCID): A framework for advancing research priorities in the cerebrovascular biology of cognitive decline. Cell. Mol. Neurobiol. 2016, 36, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.M.; Kapil, V.; Fuentes-Calvo, I.; Bubb, K.J.; Pearl, V.; Milsom, A.B.; Khambata, R.; Maleki-Toyserkani, S.; Yousuf, M.; Benjamin, N.; et al. Enhanced Vasodilator Activity of Nitrite in Hypertension. Hypertension 2013, 61, 1091–1102. [Google Scholar] [CrossRef]
- Berry, S.E.; Valdes, A.M.; Drew, D.A.; Asnicar, F.; Mazidi, M.; Wolf, J.; Capdevila, J.; Hadjigeorgiou, G.; Davies, R.; Al Khatib, H.; et al. Human postprandial responses to food and potential for precision nutrition. Nat. Med. 2020, 26, 964–973. [Google Scholar] [CrossRef]
- Berry, S.; Valdes, A.; Davies, R.; Delahanty, L.; Drew, D.; Chan, A.T.; Segata, N.; Franks, P.; Spector, T. Predicting Personal Metabolic Responses to Food Using Multi-omics Machine Learning in over 1000 Twins and Singletons from the UK and US: The PREDICT I Study (OR31-01-19). Curr. Dev. Nutr. 2019, 3, nzz037.OR31-01-19. [Google Scholar] [CrossRef]
- Mendes-Soares, H.; Raveh-Sadka, T.; Azulay, S.; Edens, K.; Ben-Shlomo, Y.; Cohen, Y.; Ofek, T.; Bachrach, D.; Stevens, J.; Colibaseanu, D.; et al. Assessment of a Personalized Approach to Predicting Postprandial Glycemic Responses to Food Among Individuals without Diabetes. JAMA Netw. Open 2019, 2, e188102. [Google Scholar] [CrossRef]
- Kim, Y.J.; Huh, I.; Kim, J.Y.; Park, S.; Ryu, S.H.; Kim, K.-B.; Kim, S.; Park, T.; Kwon, O. Integration of Traditional and Metabolomics Biomarkers Identifies Prognostic Metabolites for Predicting Responsiveness to Nutritional Intervention against Oxidative Stress and Inflammation. Nutrients 2017, 9, 233. [Google Scholar] [CrossRef]
- Hughes, R.L.; Kable, M.E.; Marco, M.; Keim, N.L. The Role of the Gut Microbiome in Predicting Response to Diet and the Development of Precision Nutrition Models. Part II: Results. Adv. Nutr. 2019, 10, 979–998. [Google Scholar] [CrossRef]
- Tanev, K.S.; Federico, L.E.; Terry, D.P.; Clark, E.L.; Iverson, G.L. Cognitive Impairment and Predicting Response to Treatment in an Intensive Clinical Program for Post-9/11 Veterans with Posttraumatic Stress Disorder. J. Neuropsychiatry Clin. Neurosci. 2019, 31, 337–345. [Google Scholar] [CrossRef]
- Chen, J.; Gu, D.; Jaquish, C.E.; Chen, C.-S.; Rao, D.; Liu, D.; Hixson, J.E.; Hamm, L.L.; Gu, C.C.; Whelton, P.K. Association between blood pressure responses to the cold pressor test and dietary sodium intervention in a Chinese population. Arch. Intern. Med. 2008, 168, 1740–1746. [Google Scholar] [CrossRef] [PubMed]
- Barba, G.; Cappuccio, F.P.; Russo, L.; Stinga, F.; Iacone, R.; Strazzullo, P. Renal function and blood pressure response to dietary salt restriction in normotensive men. Hypertension 1996, 27, 1160–1164. [Google Scholar] [CrossRef] [PubMed]
- Livingstone, K.M.; Celis-Morales, C.; Navas-Carretero, S.; San-Cristobal, R.; Forster, H.; Woolhead, C.; O’Donovan, C.B.; Moschonis, G.; Manios, Y.; Traczyk, I. Characteristics of participants who benefit most from personalised nutrition: Findings from the pan-European Food4Me randomised controlled trial. Br. J. Nutr. 2020, 123, 1396–1405. [Google Scholar] [CrossRef] [PubMed]
- González-Sarrías, A.; García-Villalba, R.; Romo-Vaquero, M.; Alasalvar, C.; Örem, A.; Zafrilla, P.; Tomás-Barberán, F.A.; Selma, M.V.; Espín, J.C. Clustering according to urolithin metabotype explains the interindividual variability in the improvement of cardiovascular risk biomarkers in overweight-obese individuals consuming pomegranate: A randomized clinical trial. Mol. Nutr. Food Res. 2017, 61, 1600830. [Google Scholar] [CrossRef] [PubMed]
- Tomas-Barberan, F.A.; Gonzalez-Sarrias, A.; Garcia-Villalba, R.; Nunez-Sanchez, M.A.; Selma, M.V.; Garcia-Conesa, M.T.; Espin, J.C. Urolithins, the rescue of “old” metabolites to understand a “new” concept: Metabotypes as a nexus among phenolic metabolism, microbiota dysbiosis, and host health status. Mol. Nutr. Food Res. 2017, 61, 1500901. [Google Scholar] [CrossRef]
- de Roos, B.; Aura, A.-M.; Bronze, M.; Cassidy, A.; Conesa, M.-T.G.; Gibney, E.R.; Greyling, A.; Kaput, J.; Kerem, Z.; Knežević, N.; et al. Targeting the delivery of dietary plant bioactives to those who would benefit most: From science to practical applications. Eur. J. Nutr. 2019, 58, 65–73. [Google Scholar] [CrossRef]
- Gaitán, A.; Garolera, M.; Cerulla, N.; Chico, G.; Rodriguez-Querol, M.; Canela-Soler, J. Efficacy of an adjunctive computer-based cognitive training program in amnestic mild cognitive impairment and Alzheimer’s disease: A single-blind, randomized clinical trial. Int. J. Geriatr. Psychiatry 2013, 28, 91–99. [Google Scholar] [CrossRef]
- Zanchetti, A. Bottom blood pressure or bottom cardiovascular risk? How far can cardiovascular risk be reduced? J. Hypertens. 2009, 27, 1509–1520. [Google Scholar] [CrossRef]
- Lila, M.A.; Burton-Freeman, B.; Grace, M.; Kalt, W. Unraveling anthocyanin bioavailability for human health. Annu. Rev. Food Sci. Technol. 2016, 7, 375–393. [Google Scholar] [CrossRef]
- Bell, L.; Lamport, D.J.; Butler, L.T.; Williams, C.M. A Review of the Cognitive Effects Observed in Humans Following Acute Supplementation with Flavonoids, and Their Associated Mechanisms of Action. Nutrients 2015, 7, 10290–10306. [Google Scholar] [CrossRef]
- Rodriguez-Mateos, A.; Rendeiro, C.; Bergillos-Meca, T.; Tabatabaee, S.; George, T.W.; Heiss, C.; Spencer, J.P. Intake and time dependence of blueberry flavonoid-induced improvements in vascular function: A randomized, controlled, double-blind, crossover intervention study with mechanistic insights into biological activity. Am. J. Clin. Nutr. 2013, 98, 1179–1191. [Google Scholar] [CrossRef] [PubMed]
- Mathew, A.S.; Capel-Williams, G.M.; Berry, S.E.; Hall, W.L. Acute effects of pomegranate extract on postprandial lipaemia, vascular function and blood pressure. Plant Foods Hum. Nutr. 2012, 67, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Silva, S.; Costa, E.M.; Coelho, M.C.; Morais, R.M.; Pintado, M.E. Variation of anthocyanins and other major phenolic compounds throughout the ripening of four Portuguese blueberry (Vaccinium corymbosum L) cultivars. Nat. Prod. Res. 2017, 31, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Margraf, T.; Karnopp, A.R.; Rosso, N.D.; Granato, D. Comparison between Folin-Ciocalteu and Prussian Blue Assays to Estimate The Total Phenolic Content of Juices and Teas Using 96-Well Microplates. J. Food Sci. 2015, 80, C2397–C2403. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Rangel, J.C.; Benavides, J.; Heredia, J.B.; Cisneros-Zevallos, L.; Jacobo-Velázquez, D.A. The Folin–Ciocalteu assay revisited: Improvement of its specificity for total phenolic content determination. Anal. Methods 2013, 5, 5990–5999. [Google Scholar] [CrossRef]
- Cleophas, T.J. Carryover Effects in Clinical Research. In Human Experimentation: Methodologic Issues Fundamental to Clinical Trials; Springer: Dordrecht, The Netherlands, 1999; pp. 25–36. [Google Scholar] [CrossRef]
- Huang, C.C.; Leu, H.B.; Wu, T.C.; Lin, S.J.; Chen, J.W. Clinical predictors of the response to short-term thiazide treatment in nondiabetic essential hypertensives. J. Hum. Hypertens. 2008, 22, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Cuisset, T.; Frere, C.; Quilici, J.; Barbou, F.; Morange, P.E.; Hovasse, T.; Bonnet, J.L.; Alessi, M.C. High post-treatment platelet reactivity identified low-responders to dual antiplatelet therapy at increased risk of recurrent cardiovascular events after stenting for acute coronary syndrome. J. Thromb. Haemost. 2006, 4, 542–549. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Value 1 |
|---|---|
| Age (years) | 25.86 ± 6.81 |
| BMI (kg/m2) | 23.15 ± 3.12 |
| Gender | 13 male, 24 female |
| Ethnicity | 1 Black |
| 2 Indian Asian | |
| 3 Chinese Asian | |
| 31 Caucasian, European | |
| Fruit and vegetable intake (portions/day) | 2.13 ± 0.85 |
| Berry intake (portions/day) 2 | 0.06 ± 1.61 |
| Endpoint | Blueberry Intervention | Blueberry Powder Intervention | Placebo Intervention | ||||||
|---|---|---|---|---|---|---|---|---|---|
| ↑ | — | ↓ | ↑ | — | ↓ | ↑ | — | ↓ | |
| PWV | 49% | 6% | 46% | 53% | 0% | 47% | 56% | 3% | 41% |
| SBP | 52% | 9% | 39% | 43% | 14% | 40% | 53% | 3% | 44% |
| DBP | 56% | 6% | 38% | 49% | 14% | 37% | 41% | 6% | 53% |
| Nitrite (NO2−) | 71% | 0% | 29% | 37% | 0% | 63% | 48% | 0% | 52% |
| Glucose | 45% | 0% | 55% | 50% | 3% | 47% | 66% | 0% | 34% |
| TAG | 34% | 0% | 66% | 59% | 0% | 41% | 34% | 0% | 66% |
| Total cholesterol | 36% | 0% | 64% | 42% | 0% | 58% | 54% | 0% | 46% |
| HDL-C | 55% | 0% | 45% | 55% | 0% | 45% | 59% | 3% | 38% |
| LDL-C | 31% | 3% | 66% | 42% | 0% | 58% | 71% | 0% | 29% |
| Working memory 1 | 57% | 12% | 31% | 48% | 14% | 36% | 55% | 13% | 32% |
| Episodic memory 1 | 48% | 14% | 37% | 45% | 16% | 38% | 44% | 13% | 43% |
| Attention 1 | 47% | 11% | 42% | 50% | 8% | 42% | 45% | 3% | 52% |
| Alert 1 | 71% | 0% | 29% | 47% | 0% | 53% | 53% | 0% | 47% |
| Content 1 | 54% | 11% | 35% | 33% | 6% | 61% | 59% | 0% | 41% |
| Calm 1 | 62% | 3% | 35% | 58% | 3% | 39% | 39% | 6% | 55% |
| Mental fatigue 1 | 45% | 3% | 52% | 55% | 4% | 41% | 52% | 5% | 43% |
| Endpoint * | Response (%) | ||
|---|---|---|---|
| Blueberry Intervention | Blueberry Powder Intervention | Placebo Intervention | |
| PWV | −48–+27% | −51–+31% | −50–+30% |
| SBP | −16–+17% | −20–+11% | −24–+13% |
| DBP | −34–+16% | −28–+12% | −33–+25% |
| Nitrite (NO2−) | −141–+525% | −111–+215% | −152–+163% |
| Glucose | −33–+66% | −32–+25% | −33–+44% |
| TAG | −105–+95% | −94–+132% | −97–+132% |
| Total cholesterol | −30–+62% | −68–+43% | −45–+32% |
| HDL-C | −51–+85% | −90–+52% | −35–+26% |
| LDL-C | −34–+79% | −58–+64% | −64–+38% |
| Working memory | −39–+61% | −21–+51% | −35–+55% |
| Episodic memory | −30–+30% | −12–+21% | −20–+24% |
| Attention | −33–+18% | −34–+14% | −19–+19% |
| Alert | −57–+48% | −70–+59% | −40–+39% |
| Content | −41–+42% | −33–+28% | −27–+26% |
| Calm | −39–+60% | −29–+40% | −109–+24% |
| Mental fatigue | −65–+96% | −114–+80% | −112–+89% |
| Chi-Square Test Statistics 1 | |||||
|---|---|---|---|---|---|
| Factor | Response Following Blueberry Intervention | Response Following Blueberry Powder Intervention | |||
| All endpoints | Gender | X2 = 1.000 | p = 0.620 | X2 = 1.286 | p = 0.576 |
| BMI | X2 = 0.000 | p = 1.000 | X2 = 0.000 | p = 1.000 | |
| Visit | X2 = 0.000 | p = 1.000 | X2 = 1.067 | p = 0.587 | |
| Vascular Function | Gender | X2 = 0.234 | p = 1.000 | X2 = 1.000 | p = 0.620 |
| BMI | X2 = 0.234 | p = 1.000 | X2 = 0.000 | p = 1.000 | |
| Visit | X2 = 0.533 | p = 0.766 | X2 = 0.900 | p = 0.638 | |
| Cognition | Gender | X2 = 1.000 | p = 0.620 | X2 = 3.600 | p = 0.206 |
| BMI | X2 = 0.234 | p = 1.000 | X2 = 0.000 | p = 1.000 | |
| Visit | X2 = 1.111 | p = 0.574 | X2 = 1.067 | p = 0.587 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Haskell-Ramsay, C.; Gallegos, J.L.; Lodge, J.K. Inter-Individual Responses to a Blueberry Intervention across Multiple Endpoints. Nutrients 2024, 16, 895. https://doi.org/10.3390/nu16060895
Wang Y, Haskell-Ramsay C, Gallegos JL, Lodge JK. Inter-Individual Responses to a Blueberry Intervention across Multiple Endpoints. Nutrients. 2024; 16(6):895. https://doi.org/10.3390/nu16060895
Chicago/Turabian StyleWang, Yueyue, Crystal Haskell-Ramsay, Jose Lara Gallegos, and John K. Lodge. 2024. "Inter-Individual Responses to a Blueberry Intervention across Multiple Endpoints" Nutrients 16, no. 6: 895. https://doi.org/10.3390/nu16060895
APA StyleWang, Y., Haskell-Ramsay, C., Gallegos, J. L., & Lodge, J. K. (2024). Inter-Individual Responses to a Blueberry Intervention across Multiple Endpoints. Nutrients, 16(6), 895. https://doi.org/10.3390/nu16060895