
Association of Dietary Patterns with Cardiovascular Disease Risk Factors in Mexican Adults: Insights from a Cross-Sectional Descriptive Study

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Volunteers
2.2. Variables and Data Collection
2.2.1. Clinical History
2.2.2. Anthropometric Measurements
2.2.3. Physical Activity
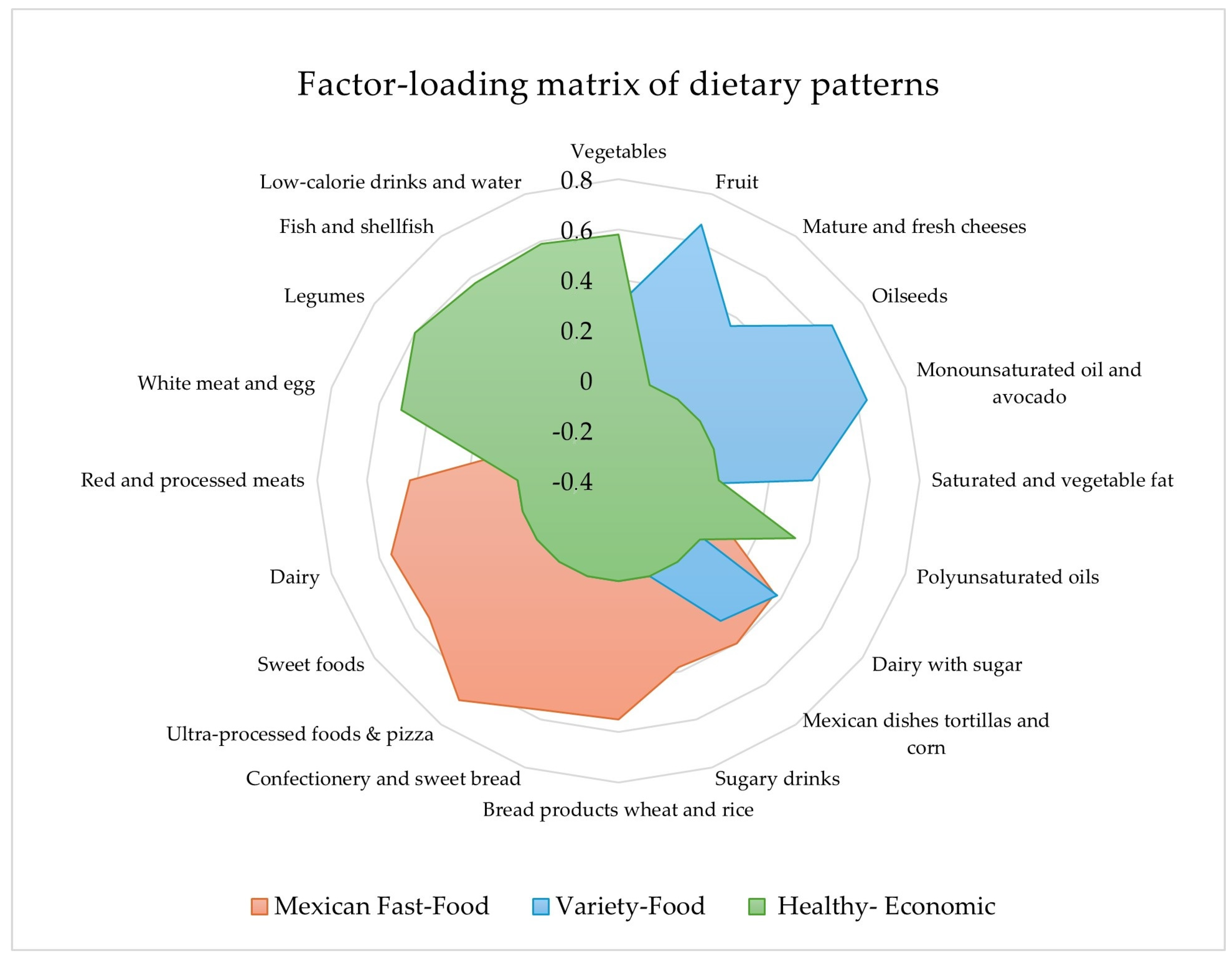
2.2.4. Diet and Pattern Analysis
2.3. Blood Extraction and Determination of Biomarkers
2.4. Statistic Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fung, T.T.; Willett, W.C.; Stampfer, M.J.; Manson, J.A.E.; Hu, F.B. Dietary patterns and the risk of coronary heart disease in women. Arch. Intern. Med. 2001, 161, 1857–1862. [Google Scholar] [CrossRef]
- Hu, F.B.; Rimm, E.B.; Stampfer, M.J.; Ascherio, A.; Spiegelman, D.; Willett, C.W. Prospective study of major dietary patterns and risk of coronary heart disease in men. Am. J. Clin. Nutr. 2000, 72, 912–921. [Google Scholar] [CrossRef]
- OMS. Obesidad y Sobrepeso. Available online: https://www.who.int/es/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 18 November 2020).
- Rivera, J.A.; Barquera, S.; Campirano, F.; Campos, I.; Safdie, M.; Tovar, V. Epidemiological and nutritional transition in Mexico: Rapid increase of non-communicable chronic diseases and obesity. Public Health Nutr. 2002, 5, 113–122. [Google Scholar] [CrossRef]
- Shamah-Levy, T.; Romero-Martínez, M.; Barrientos-Gutiérrez, T.; Cuevas-Nasu, L.; Bautista-Arredondo, S.; Colchero, M.; Gaona-Pineda, E.; Lazcano-Ponce, E.; Martínez-Barnetche, J.; Alpuche-Arana, C.; et al. Encuesta Nacional de Salud y Nutrición 2021 Sobre COVID-19. Resultados Nacionales; Instituto Nacional de Salud Pública: Cuernavaca, Mexico, 2022; ISBN 9786075112220. [Google Scholar]
- USDA Nutrition Evidence Systematic Review. Dietary Patterns and Risk of Cardiovascular Disease|Nutrition Evidence Systematic Review. Available online: https://pubmed.ncbi.nlm.nih.gov/35294140/ (accessed on 20 January 2024).
- Denova-Gutiérrez, E.; Tucker, K.L.; Flores, M.; Barquera, S.; Salmerón, J. Dietary patterns are associated with predicted cardiovascular disease risk in an urban mexican adult population. J. Nutr. 2016, 146, 90–97. [Google Scholar] [CrossRef]
- Denova-Gutiérrez, E.; Castañón, S.; Talavera, J.O.; Gallegos-Carrillo, K.; Flores, M.; Dosamantes-Carrasco, D.; Willett, W.C.; Salmerón, J. Dietary patterns are associated with metabolic syndrome in an urban Mexican population. J. Nutr. 2010, 140, 1855–1863. [Google Scholar] [CrossRef]
- Flores, M.; Macías, N.; Rivera, M.; Barquera, S.; Hernández, L.; García-Guerra, A.; Rivera-Dommarco, J. a Energy and nutrient intake among Mexican school-aged children, Mexican National Health and Nutrition Survey 2006. Salud Publica Mex. 2009, 51 (Suppl. S4), S540–S550. [Google Scholar] [CrossRef]
- Neri-Sánchez, M.; Martínez-Carrillo, B.E.; Valdés-Ramos, R.; Soto-Piña, A.E.; Vargas-Hernández, J.A.; Benítez-Arciniega, A.D. Dietary patterns, central obesity and serum lipids concentration in Mexican adults|Patrones de dieta, obesidad central y concentración de lípidos séricos en adultos Mexicanos. Nutr. Hosp. 2019, 36, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Karr, S. Epidemiology and management of hyperlipidemia. Am. J. Manag. Care 2017, 23, S139–S148. [Google Scholar] [PubMed]
- Wajchenberg, B.L.; Lé, B.; Wajchenberg, O. Subcutaneous and Visceral Adipose Tissue. Endocr. Rev. 2000, 21, 697–738. [Google Scholar] [CrossRef] [PubMed]
- Enomoto, M.; Adachi, H.; Hirai, Y.; Fukami, A.; Satoh, A.; Otsuka, M.; Kumagae, S.-I.; Nanjo, Y.; Yoshikawa, K.; Esaki, E.; et al. LDL-C/HDL-C Ratio Predicts Carotid Intima-Media Thickness Progression Better Than HDL-C or LDL-C Alone. J. Lipids 2011, 2011, 549137. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Malnutrition. Available online: https://www.who.int/health-topics/malnutrition#tab=tab_1 (accessed on 20 January 2024).
- Tong, P.C.Y.; Kong, A.P.; So, W.Y.; Yang, X.; Ho, C.S.; Ma, R.C.; Ozaki, R.; Chow, C.C.; Lam, C.W.; Chan, J.C.N.; et al. The usefulness of the International Diabetes Federation and the National Cholesterol Education Program’s Adult Treatment Panel III definitions of the metabolic syndrome in predicting coronary heart disease in subjects with type 2 diabetes. Diabetes Care 2007, 30, 1206–1211. [Google Scholar] [CrossRef]
- Elosua, R.; Garcia, M.; Aguilar, A.; Molina, L.; Covas, M.I.; Marrugat, J. Validation of the Minnesota leisure time physical activity questionnaire in Spanish women. Med. Sci. Sports Exerc. 2000, 32, 1431–1437. [Google Scholar] [CrossRef]
- World Health Organization. Physical Activity. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 24 February 2024).
- Macedo-Ojeda, G.; Vizmanos-Lamotte, B.; Márquez-Sandoval, Y.F.; Rodríguez-Rocha, N.P.; López-Uriarte, P.J.; Fernández-Ballart, J.D. Validation of a semi-quantitative food frequency questionnaire to assess food groups and nutrient intake. Nutr. Hosp. 2013, 28, 2212–2220. [Google Scholar] [PubMed]
- de Chàvez, M.M. Composiciòn de Alimentos, 2nd ed.; McGraw-Hill: Mexico City, Mexico, 2009; ISBN 9789701067413. [Google Scholar]
- Denova-Gutiérrez, E.; Clark, P.; Muñoz-Aguirre, P.; Flores, M.; Talavera, J.O.; Chico-Barba, L.G.; Rivas, R.; Ramírez, P.; Salmerón, J. Dietary patterns are associated with calcium and vitamin D intake in an adult Mexican population|Asociación entre los patrones dietarios y el consumo de calcio y vitamina D en población adulta mexicana. Nutr. Hosp. 2016, 33, 663–670. [Google Scholar] [CrossRef] [PubMed]
- Gaona-Pineda, E.B.; Martinez-Tapia, B.; Rodríguez-Ramírez, S.; Guerrero-Zúñiga, S.; Perez-Padilla, R.; Shamah-Levy, T. Dietary patterns and sleep disorders in Mexican adults from a National Health and Nutrition Survey. J. Nutr. Sci. 2021, 10, e34. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Ramírez, S.; Gaona-Pineda, E.B.; Martínez-Tapia, B.; Arango-Angarita, A.; Kim-Herrera, E.Y.; Valdez-Sánchez, A.; Concepción Medina-Zacarías, M.; Ramírez-Silva, I.; Shamah-Levy, T. Consumo de grupos de alimentos y su asociación con características sociodemográficas en población mexicana. Ensanut 2018–19. Salud Publica Mex. 2020, 62, 693–703. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Ramírez, S.; Martinez-Tapia, B.; González-Castell, D.; Cuevas-Nasu, L.; Shamah-Levy, T. Westernized and Diverse Dietary Patterns Are Associated With Overweight-Obesity and Abdominal Obesity in Mexican Adult Men. Front. Nutr. 2022, 9, 891609. [Google Scholar] [CrossRef] [PubMed]
- Moe, Å.M.; Ytterstad, E.; Hopstock, L.A.; Løvsletten, O.; Carlsen, M.H.; Sørbye, S.H. Associations and predictive power of dietary patterns on metabolic syndrome and its components. Nutr. Metab. Cardiovasc. Dis. 2023, 34, 681–690. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C.; Ahluwalia, N.; Brouns, F.; Buetler, T.; Clement, K.; Cunningham, K.; Esposito, K.; Jönsson, L.S.; Kolb, H.; Lansink, M.; et al. Dietary factors and low-grade inflammation in relation to overweight and obesity. Br. J. Nutr. 2011, 106 (Suppl. S3), S1–S78. [Google Scholar] [CrossRef]
- Guibrunet, L.; Ortega-Avila, A.G.; Arnés, E.; Ardila, F.M. Socioeconomic, demographic and geographic determinants of food consumption in Mexico. PLoS ONE 2023, 18, e0288235. [Google Scholar] [CrossRef]
- Marrón-Ponce, J.A.; Sánchez-Pimienta, T.G.; Rodríguez-Ramírez, S.; Batis, C.; Cediel, G. Ultra-processed foods consumption reduces dietary diversity and micronutrient intake in the Mexican population. J. Hum. Nutr. Diet. 2023, 36, 241–251. [Google Scholar] [CrossRef]
- Marrón-Ponce, J.A.; Flores, M.; Cediel, G.; Monteiro, C.A.; Batis, C. Associations between Consumption of Ultra-Processed Foods and Intake of Nutrients Related to Chronic Non-Communicable Diseases in Mexico. J. Acad. Nutr. Diet. 2019, 119, 1852–1865. [Google Scholar] [CrossRef]
- Ciobanu, D.; Porojan, M.; Bala, C.; Zah, A.M.; Oroian, I.; Roman, G.; Rusu, A. Lifestyle factors, dietary patterns, and social determinants of social and eating jetlag: A cross-sectional survey. Chronobiol. Int. 2024, 41, 248–258. [Google Scholar] [CrossRef]
- Białkowska, A.; Górnicka, M.; Zielinska-Pukos, M.A.; Hamulka, J. Associations between Dietary Patterns, Anthropometric and Cardiometabolic Indices and the Number of MetS Components in Polish Adults with Metabolic Disorders. Nutrients 2023, 15, 2237. [Google Scholar] [CrossRef]
- Chen, M.; Xu, Y.; Wang, X.; Shan, S.; Cheng, G. Association between the prudent dietary pattern and blood pressure in Chinese adults is partially mediated by body composition. Front. Nutr. 2023, 10, 1131126. [Google Scholar] [CrossRef]
- Ginsberg, H.N.; Zhang, Y.L.; Hernandez-Ono, A. Regulation of plasma triglicerides in insulin resistance and diabetes. Arch. Med. Res. 2005, 36, 232–240. [Google Scholar] [CrossRef]
- Morales-Gurrola, G.; Simental-Mendia, L.E.; Castellanos Juarez, F.X.; Salas-Pachecho, J.M.; Guerrero-Romero, F. The triglycerides and glucose index is associated with cardiovascular risk factor in metabolically obese normal-weight subjects. J. Endocrinol. Investig. 2020, 43, 995–1000. [Google Scholar] [CrossRef]
- World Health Organization. Physical Inactivity a Leading Cause of Disease and Disability, Warns WHO. Available online: https://www.who.int/news/item/04-04-2002-physical-inactivity-a-leading-cause-of-disease-and-disability-warns-who (accessed on 20 January 2024).
- World Health Organization. Alimentación Sana. Available online: https://www.who.int/es/news-room/fact-sheets/detail/healthy-diet (accessed on 29 November 2023).
- Milagro, F.I.; Mansego, M.L.; De Miguel, C.; Martínez, J.A. Dietary factors, epigenetic modifications and obesity outcomes: Progresses and perspectives. Mol. Asp. Med. 2013, 34, 782–812. [Google Scholar] [CrossRef]
- Must, A.; Tybor, D.J. Physical activity and sedentary behavior: A review of longitudinal studies of weight and adiposity in youth. Int. J. Obes. 2005, 29 (Suppl. S2), S84–S96. [Google Scholar] [CrossRef]
- Thorp, A.A.; Owen, N.; Neuhaus, M.; Dunstan, D.W. Sedentary behaviors and subsequent health outcomes in adults a systematic review of longitudinal studies, 1996–2011. Am. J. Prev. Med. 2011, 41, 207–215. [Google Scholar] [CrossRef]
- Heini, A.F.; Weinsier, R.L. Divergent trends in obesity and fat intake patterns: The American paradox. Am. J. Med. 1997, 102, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Weinsier, R.L.; Hunter, G.R.; Heini, A.F.; Goran, M.I.; Sell, S.M. The etiology of obesity: Relative contribution of metabolic factors, diet, and physical activity. Am. J. Med. 1998, 105, 145–150. [Google Scholar] [CrossRef]
- Chen, Q.J.; Lai, H.M.; Chen, B.D.; Li, X.M.; Zhai, H.; He, C.H.; Pan, S.; Luo, J.Y.; Gao, J.; Liu, F.; et al. Appropriate LDL-C-to-HDL-C Ratio Cutoffs for Categorization of Cardiovascular Disease Risk Factors among Uygur Adults in Xinjiang, China. Int. J. Environ. Res. Public Health 2016, 13, 235. [Google Scholar] [CrossRef]
- Snetselaar, L.G.; de Jesus, J.M.; DeSilva, D.M.; Stoody, E.E. Dietary Guidelines for Americans, 2020–2025: Understanding the Scientific Process, Guidelines, and Key Recommendations. Nutr. Today 2021, 56, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Lavie, C.J.; Ozemek, C.; Carbone, S.; Katzmarzyk, P.T.; Blair, S.N. Sedentary Behavior, Exercise, and Cardiovascular Health. Circ. Res. 2019, 124, 799–815. [Google Scholar] [CrossRef]
- Benditt, E. Origins of human atherosclerotic plaques. The role of altered gene expression. Arch. Pathol. Lab. Med. 1988, 112, 997–1001. [Google Scholar]
- Villablanca, A.C.; McDonald, J.M.; Rutledge, J.C. Smoking and cardiovascular disease. Clin. Chest Med. 2000, 21, 159–172. [Google Scholar] [CrossRef]
- Togo, P.; Osler, M.; Sørensen, T.I.A.; Heitmann, B.L. Food intake patterns and body mass index in observational studies. Int. J. Obes. Relat. Metab. Disord. 2001, 25, 1741–1751. [Google Scholar] [CrossRef]
- Nutricloud. Available online: https://www.nutricloud.mx/ (accessed on 20 January 2024).

{kind=link}
{kind=link}
| Variables | Men (n = 42) | Women (n = 124) | Total (n = 165) | p |
|---|---|---|---|---|
| Age (years), M ± SD | 36.24 ± 9.15 | 40.13 ± 9.69 | 39.9 ± 9.6 | 0.02 * |
| Age group, n (%) | ||||
| ≤49 | 38 (22.9) | 98 (59.6) | 136 (82.4) | 0.11 |
| ≥50 | 4 (2.4) | 25 (15.1) | 29 (17.5) | |
| Civil status, n (%) | ||||
| Single | 17 (10.2) | 33 (20.5) | 50 (30.3) | 0.14 |
| Married | 25 (15.1) | 75 (45.2) | 100 (60.2) | |
| Divorced | 0 (0) | 6 (3.6) | 6 (3.6) | |
| Living together | 0 (0) | 7 (4.2) | 7 (4.2) | |
| Widower | 0 (0) | 2 (1.2) | 2 (1.2) | |
| School level, n (%) | ||||
| Primary | 0 (0) | 6 (3.6) | 6 (3.6) | <0.001 * |
| Secondary | 4 (2.4) | 56 (33.7) | 60 (36.1) | |
| High school | 12 (7.2) | 42 (25.9) | 54 (32.7) | |
| Degree | 20 (12.0) | 9 (5.4) | 29 (17.5) | |
| Technical career | 4 (2.4) | 10 (6.0) | 14 (8.4) | |
| Master’s degree | 2 (1.2) | 0 (0) | 2 (1.2) | |
| Smoking, n (%) | ||||
| Smoker | 6 (3.6) | 19 (11.4) | 25 (15.1) | 0.04 * |
| Non-smoker | 31 (18.7) | 101 (61.4) | 132 (80.0) | |
| Former smoker | 5 (3.0) | 3 (1.8) | 8 (4.8) | |
| Family history of illness in close relatives (parents, brothers, and sisters), n (%) | ||||
| Obesity | 15 (9.0) | 35 (21.1) | 50 (30.1) | 0.36 |
| Diabetes mellitus 2 | 16 (9.6) | 59 (35.5) | 75 (45.2) | 0.28 |
| Dyslipidemias | 5 (3.0) | 23 (13.9) | 28 (16.9) | 0.32 |
| Arterial hypertension | 11 (6.6) | 57 (34.3) | 68 (41.0) | 0.02 * |
| Heart disease | 1 (0.6) | 20 (12.0) | 21 (12.7) | 0.02 * |
| Physical activity, n (%) | ||||
| Active (150–300 min/week) | 21 (50) | 25 (20.16) | 46 (27.8) | <0.001 * |
| Sedentary (<150 min/week) | 21 (50) | 98 (79.03) | 114 (72.12) | |
| Variables | Normal Weight (n = 34) | Overweight (n = 69) | Obesity (n = 58) | Total (n = 161) | p |
|---|---|---|---|---|---|
| Anthropometric | |||||
| BMI (kg/m2) | 23.0 ± 1.6 a | 27.4 ± 1.4 b | 32.0 ± 1.2 c | 28.0 ± 3.6 | 0.001 * |
| Waist circumference (cm) | 76.5 ± 6.2 a | 85.5 ± 7.4 b | 95.5 ± 10.4 c | 87.0 ± 10.9 | 0.001 * |
| Biochemical | |||||
| Glucose (mg/dL) | 79.1 ± 7.9 | 76.0 ± 7.0 c | 85.1 ± 24.9 c | 79.5 ± 16.5 | 0.005 * |
| Cholesterol total (mg/dL) | 172.5 ± 38.4 | 188.0 ± 41.8 | 182.2 ± 34.0 | 182.8 ± 38.6 | 0.161 |
| HDL-c (mg/dL) | 54.9 ± 8.7 ab | 47.2 ± 11.0 a | 45.9 ± 15.0 b | 48.2 ± 12.5 | 0.005 * |
| LDL-c (mg/dL) | 99.4 ± 36.7 | 116.0 ± 37.8 | 111.7 ± 31.5 | 110.9 ± 35.7 | 0.08 |
| Triglycerides (mg/dL) | 93.8 ± 43.2 b | 119.6 ± 49.5 c | 161.5 ± 97.2 bc | 129.2 ± 74.0 | 0.001 * |
| LDL/HDL-c ratio | 1.89 ± 0.80 ab | 2.60 ± 1.06 a | 2.60 ± 0.96 b | 2.44 ± 1.01 | 0.003 * |
| Clinical (mm /Hg) | |||||
| Systolic blood pressure | 111.5 ± 9.9 | 115.4 ± 14.7 | 117.8 ± 13.7 | 115.4 ± 13.5 | 0.080 |
| Diastolic blood pressure | 66.1 ± 6.7 b | 67.7 ± 9.0 c | 71.7 ± 10.4 bc | 68.7 ± 9.3 | 0.009 * |
| Variable | Mexican Fast-Food | Variety-Food | Healthy-Economic | p |
|---|---|---|---|---|
| Energy (kcal/d) | 3166 ± 1185 a | 2762 ± 852 b | 2624 ± 827 b | 0.01 * |
| Carbohydrates (%) | 48.53 ± 4.28 b | 49.46 ± 4.35 a | 47.15 ± 5.84 b | 0.05 * |
| Sugar (%) | 5.87 ± 4.07 | 5.75 ± 3.69 | 4.93 ± 4.14 | 0.41 |
| Protein (%) | 13.48 ± 2.80 | 13.55 ± 1.61 | 14.27 ± 2.76 | 0.17 |
| Lipids (%) | 38.00 ± 4.17 | 36.99 ± 3.75 | 38.57 ± 5.05 | 0.16 |
| Saturated fatty acids (%) | 31.26 ± 5.99 a | 27.97 ± 4.47 b | 27.21 ± 4.83 b | 0.001 * |
| Monounsaturated fatty acids (%) | 26.26 ± 3.60 | 27.31 ± 3.85 | 26.35 ± 4.92 | 0.31 |
| Polyunsaturated fatty acids (%) | 18.42 ± 4.40 a | 19.93 ± 4.31 b | 22.65 ± 5.00 c | 0.001 * |
| Dietary cholesterol (mg) | 366.54 ± 157.63 a | 285.01 ± 95.77 b | 383.52 ± 251.53 c | 0.01 * |
| Dietary fiber (g) | 23.24 ± 12.98 a | 27.94 ± 15.77 b | 22.56 ± 6.00 a | 0.05 * |
| (95% CI for OR) | |||||
|---|---|---|---|---|---|
| Cardiovascular Disease Risk Factors Scale | B (ES) | p | Odds Ratio | Lower | Higher |
| Physical activity | 1.5 (0.37) | <0.001 * | 4.85 | 2.32 | 10.15 |
| Smoking habits | 1.8 (0.48) | <0.001 * | 6.21 | 2.40 | 16.09 |
| Adherence to the Mexican Fast-Food DP | 0.59 (0.25) | 0.032 * | 1.71 | 1.04 | 2.80 |
| Adherence to the Variety-Food DP | 0.16 (0.29) | 0.570 | 1.18 | 0.65 | 2.12 |
| Adherence to the Healthy-Economic DP | −0.34 (0.34) | 0.310 | 0.70 | 0.36 | 1.39 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vázquez-Aguilar, A.; Rueda-Robles, A.; Rivas-García, L.; Vázquez-Lorente, H.; Duque-Soto, C.M.; Jiménez-López, K.L.; Marín-Arriola, I.C.; Sánchez-Jiménez, M.A.; López-Uriarte, P.J. Association of Dietary Patterns with Cardiovascular Disease Risk Factors in Mexican Adults: Insights from a Cross-Sectional Descriptive Study. Nutrients 2024, 16, 804. https://doi.org/10.3390/nu16060804
Vázquez-Aguilar A, Rueda-Robles A, Rivas-García L, Vázquez-Lorente H, Duque-Soto CM, Jiménez-López KL, Marín-Arriola IC, Sánchez-Jiménez MA, López-Uriarte PJ. Association of Dietary Patterns with Cardiovascular Disease Risk Factors in Mexican Adults: Insights from a Cross-Sectional Descriptive Study. Nutrients. 2024; 16(6):804. https://doi.org/10.3390/nu16060804
Chicago/Turabian StyleVázquez-Aguilar, Alejandra, Ascensión Rueda-Robles, Lorenzo Rivas-García, Héctor Vázquez-Lorente, Carmen María Duque-Soto, Karla Lizbet Jiménez-López, Isabel Cristina Marín-Arriola, Martha Alicia Sánchez-Jiménez, and Patricia Josefina López-Uriarte. 2024. "Association of Dietary Patterns with Cardiovascular Disease Risk Factors in Mexican Adults: Insights from a Cross-Sectional Descriptive Study" Nutrients 16, no. 6: 804. https://doi.org/10.3390/nu16060804
APA StyleVázquez-Aguilar, A., Rueda-Robles, A., Rivas-García, L., Vázquez-Lorente, H., Duque-Soto, C. M., Jiménez-López, K. L., Marín-Arriola, I. C., Sánchez-Jiménez, M. A., & López-Uriarte, P. J. (2024). Association of Dietary Patterns with Cardiovascular Disease Risk Factors in Mexican Adults: Insights from a Cross-Sectional Descriptive Study. Nutrients, 16(6), 804. https://doi.org/10.3390/nu16060804