


Trends in Calcium Intake among the US Population: Results from the NHANES (1999–2018)
 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
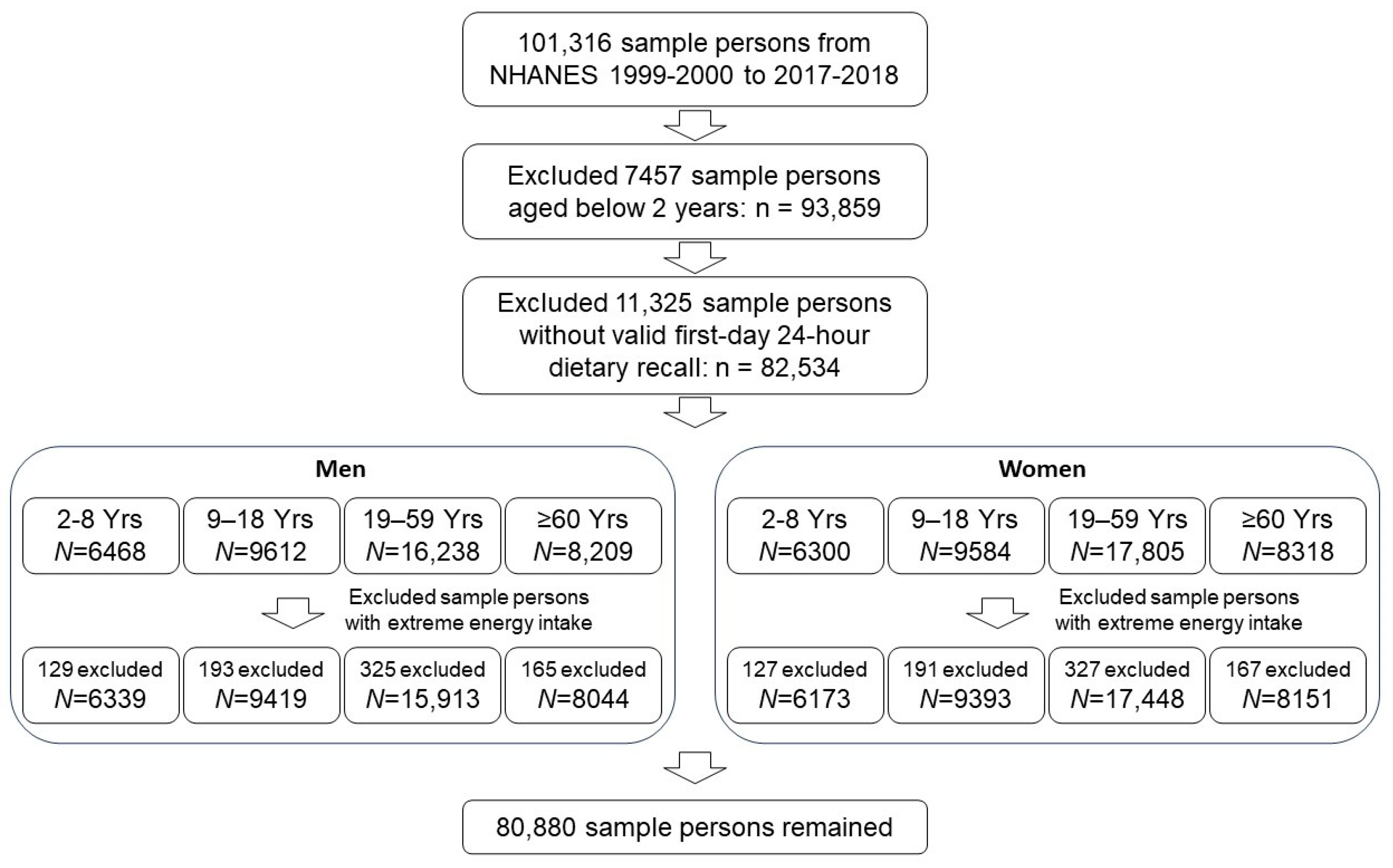
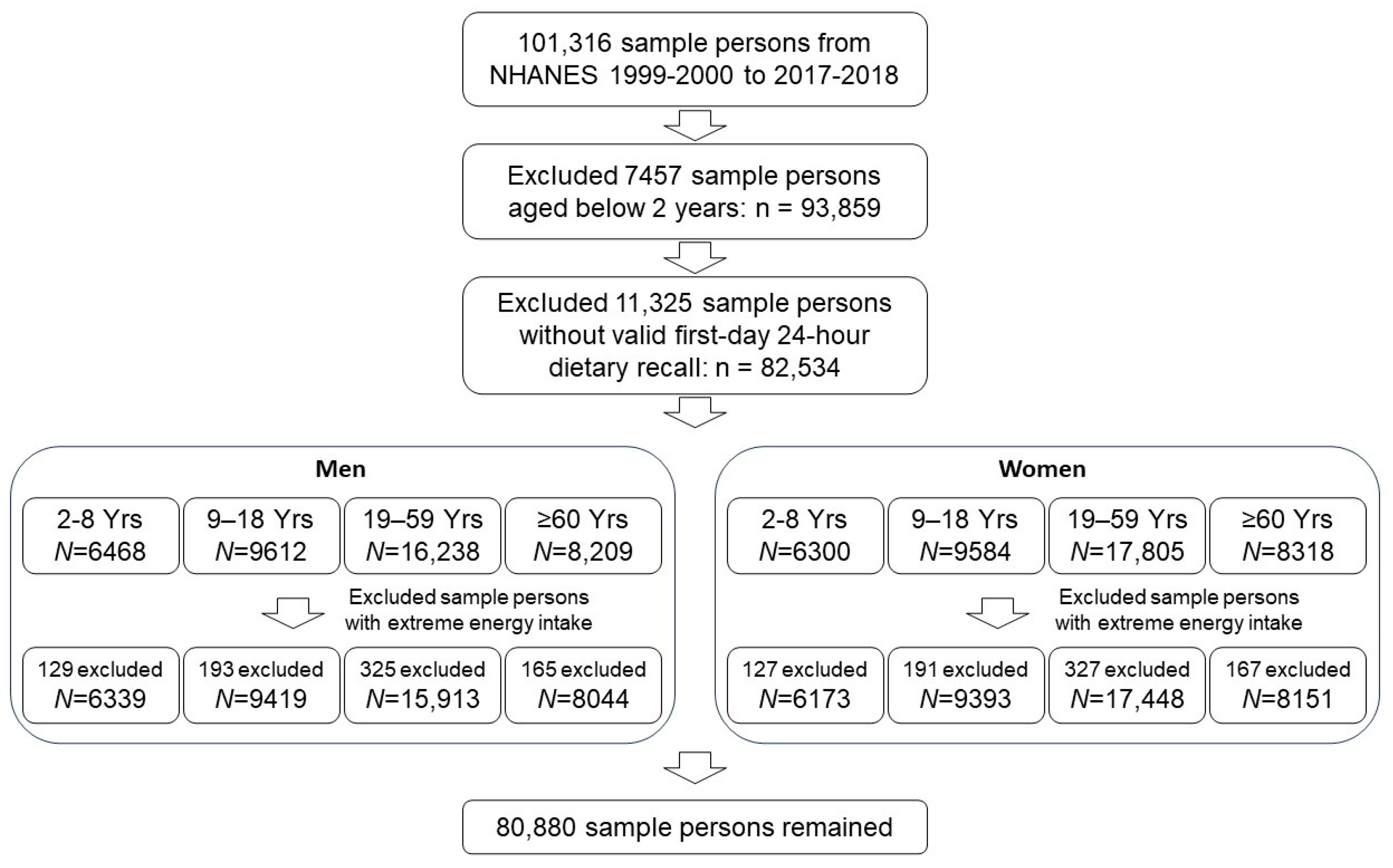
2.1. Data Source and Study Population
2.2. Dietary Calcium Intake Assessment
2.3. Dietary Supplementation of Calcium
2.4. Statistical Analysis
3. Results
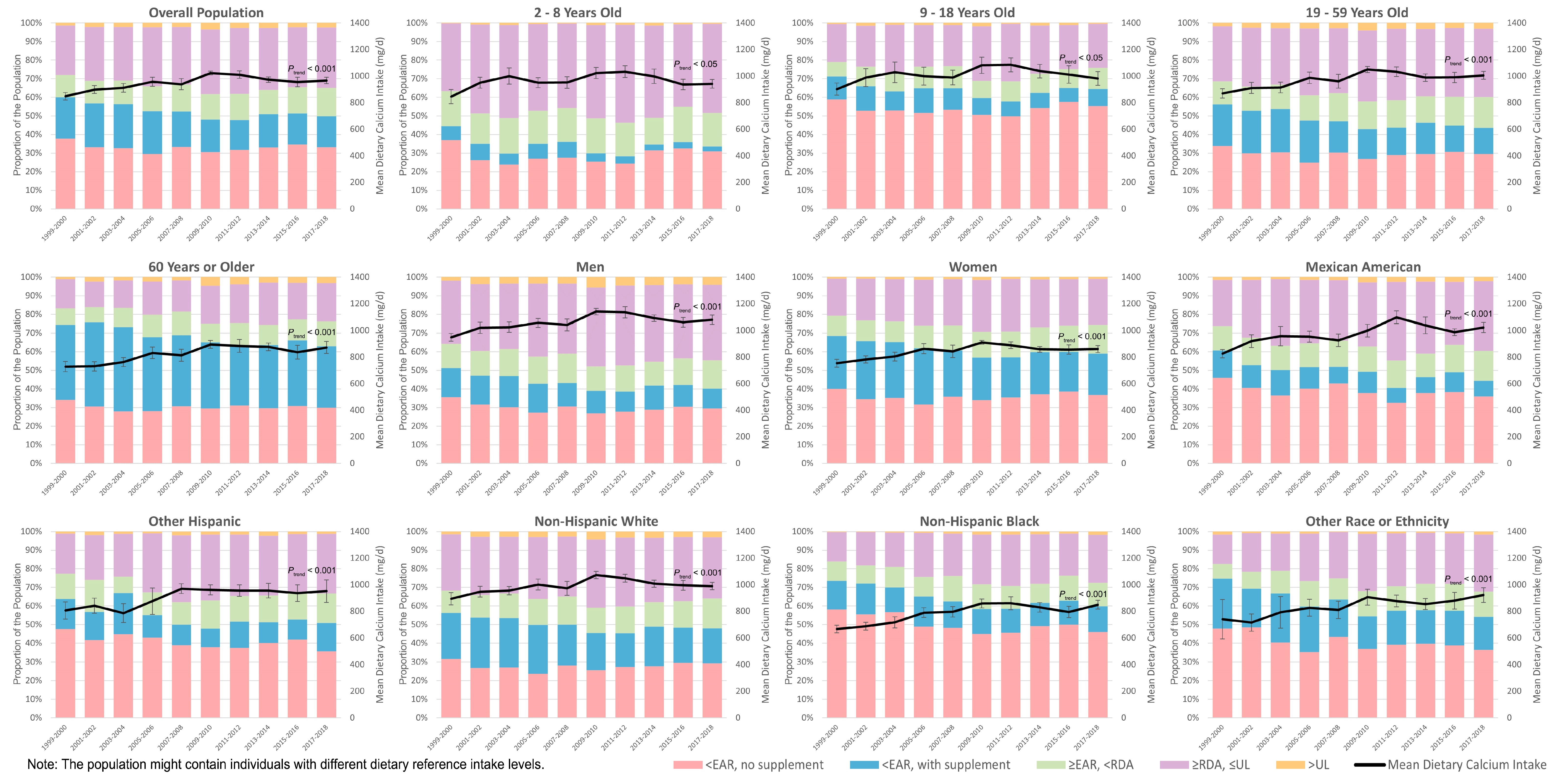
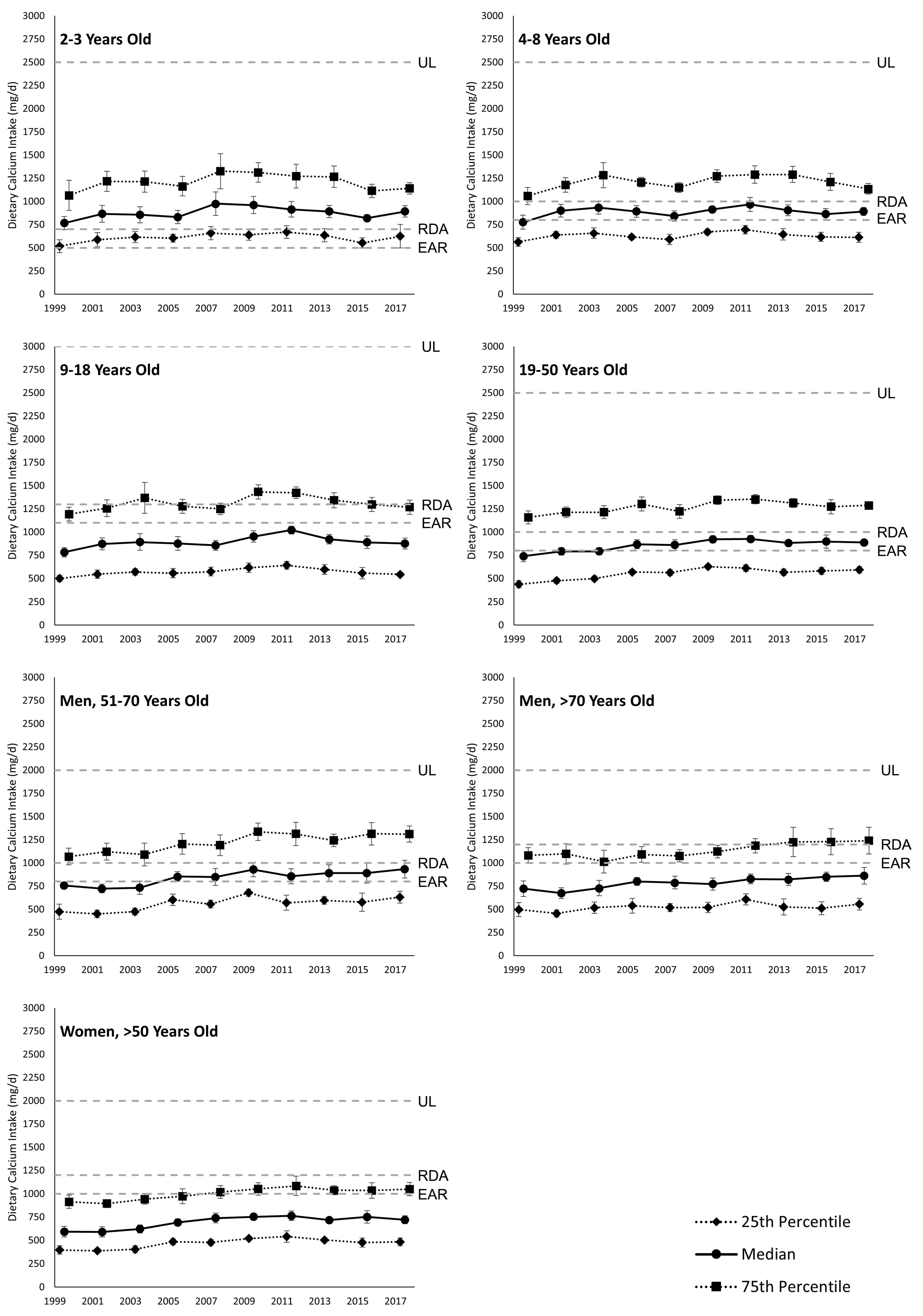
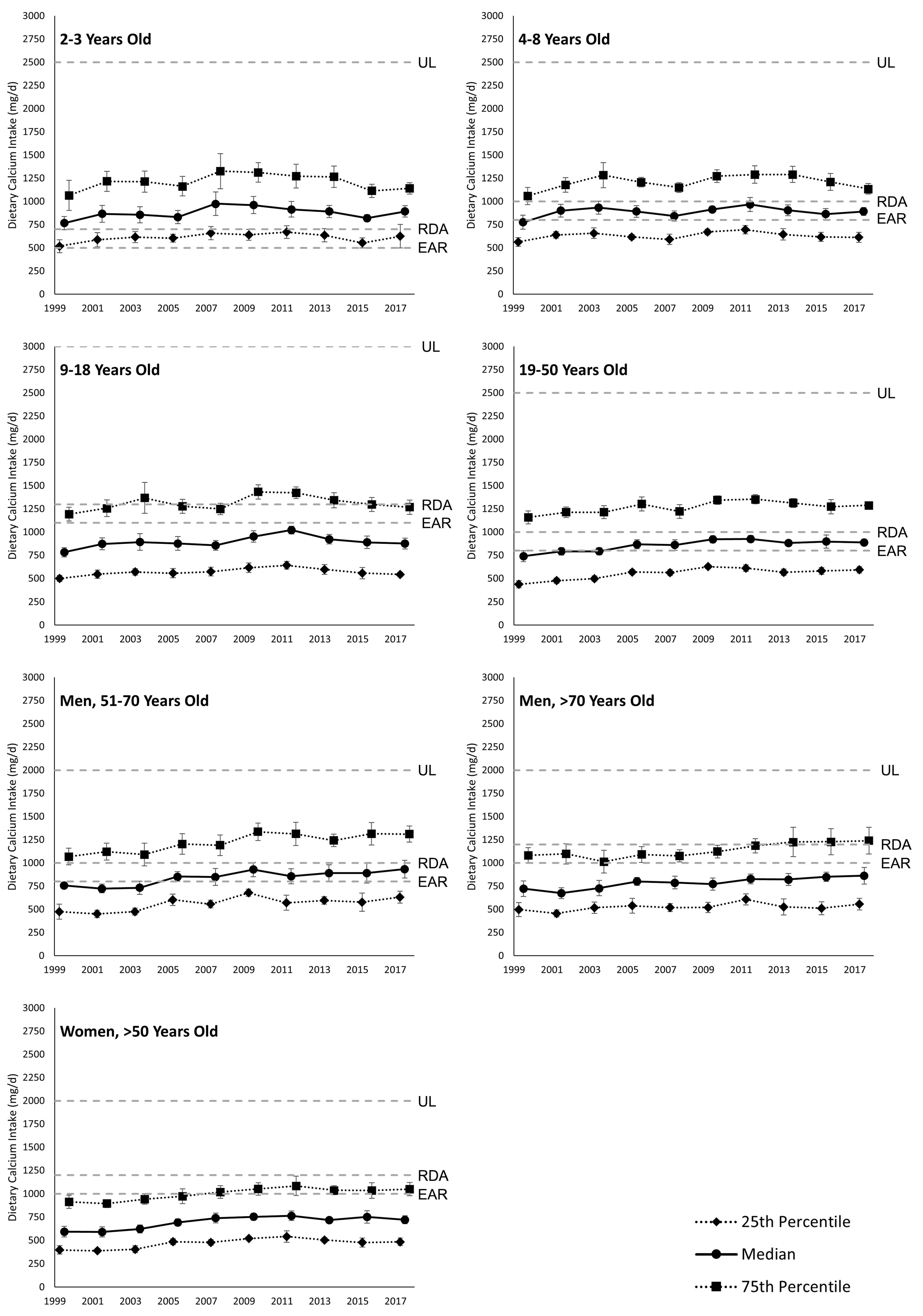
3.1. Dietary Calcium Intake
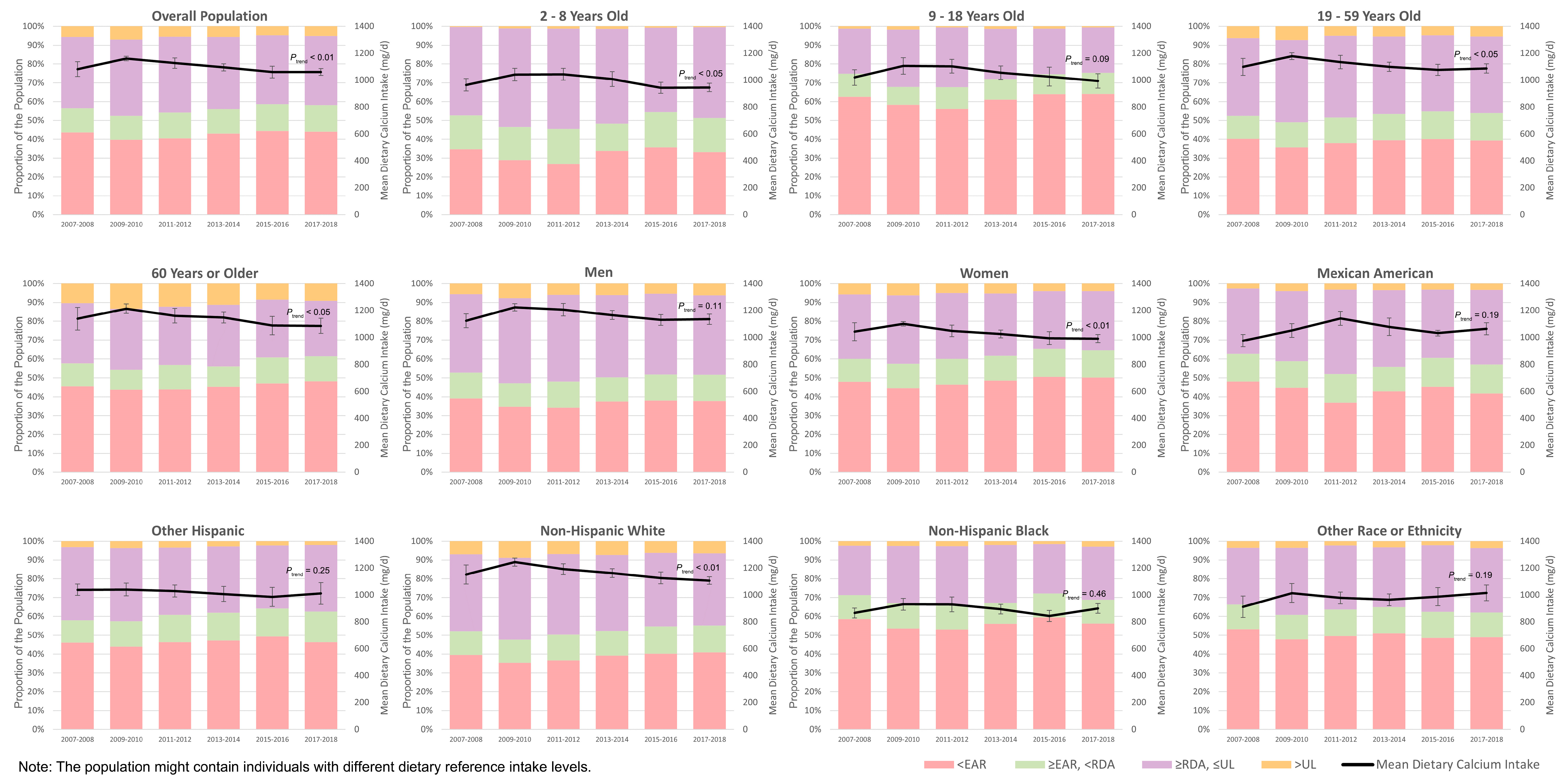
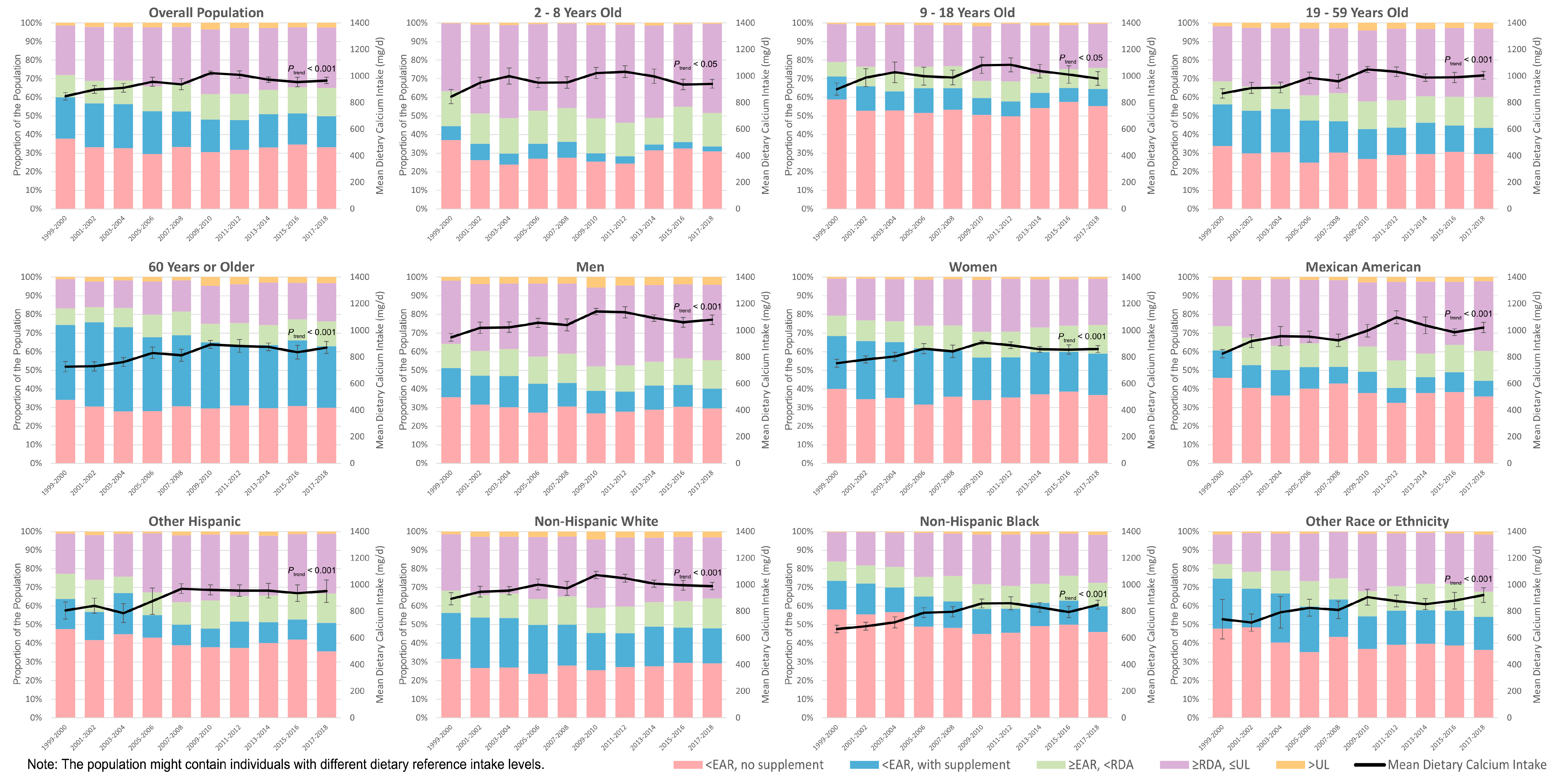
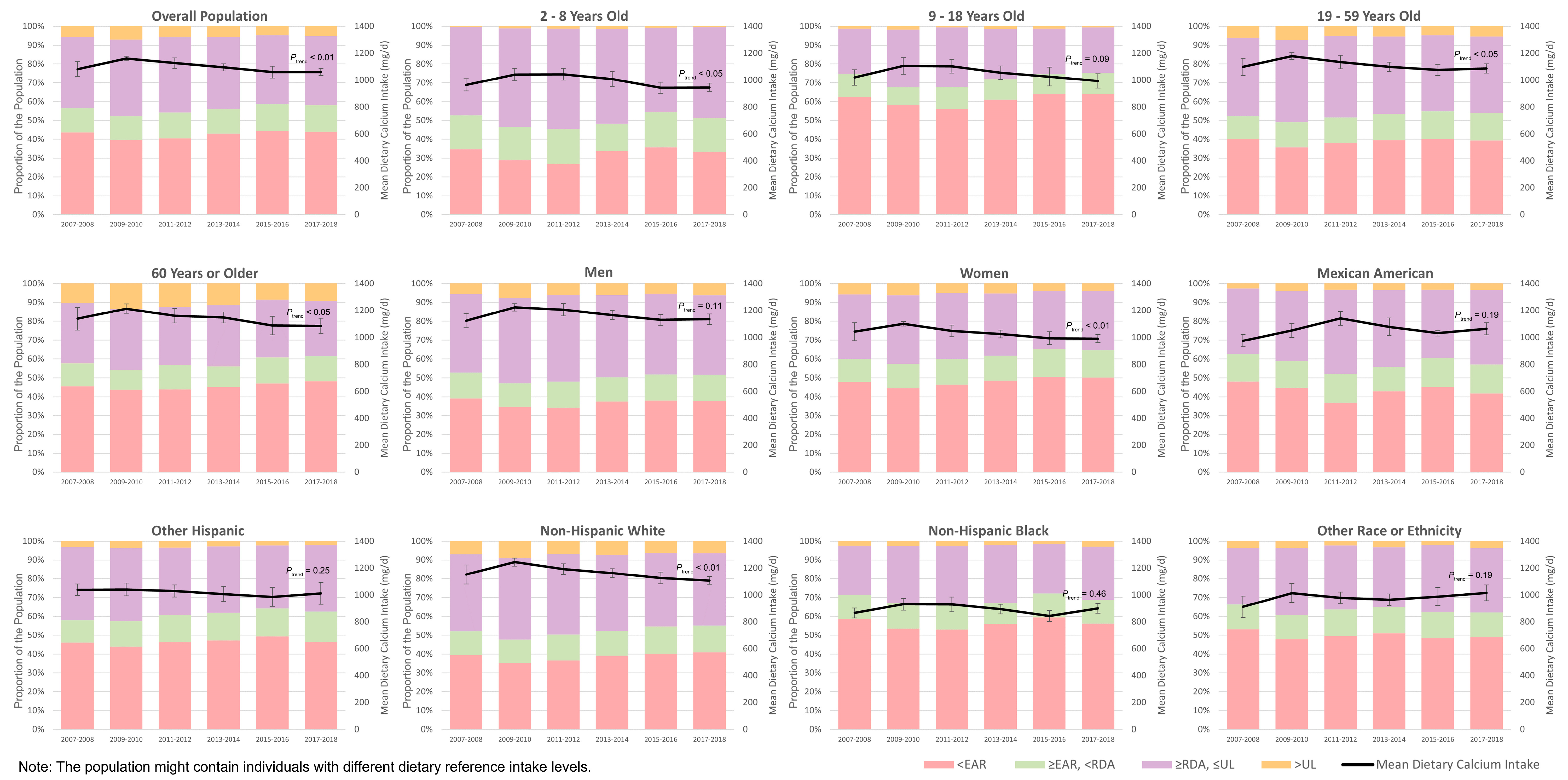
3.2. Proportion with Insufficient or Excessive Dietary Calcium Intake
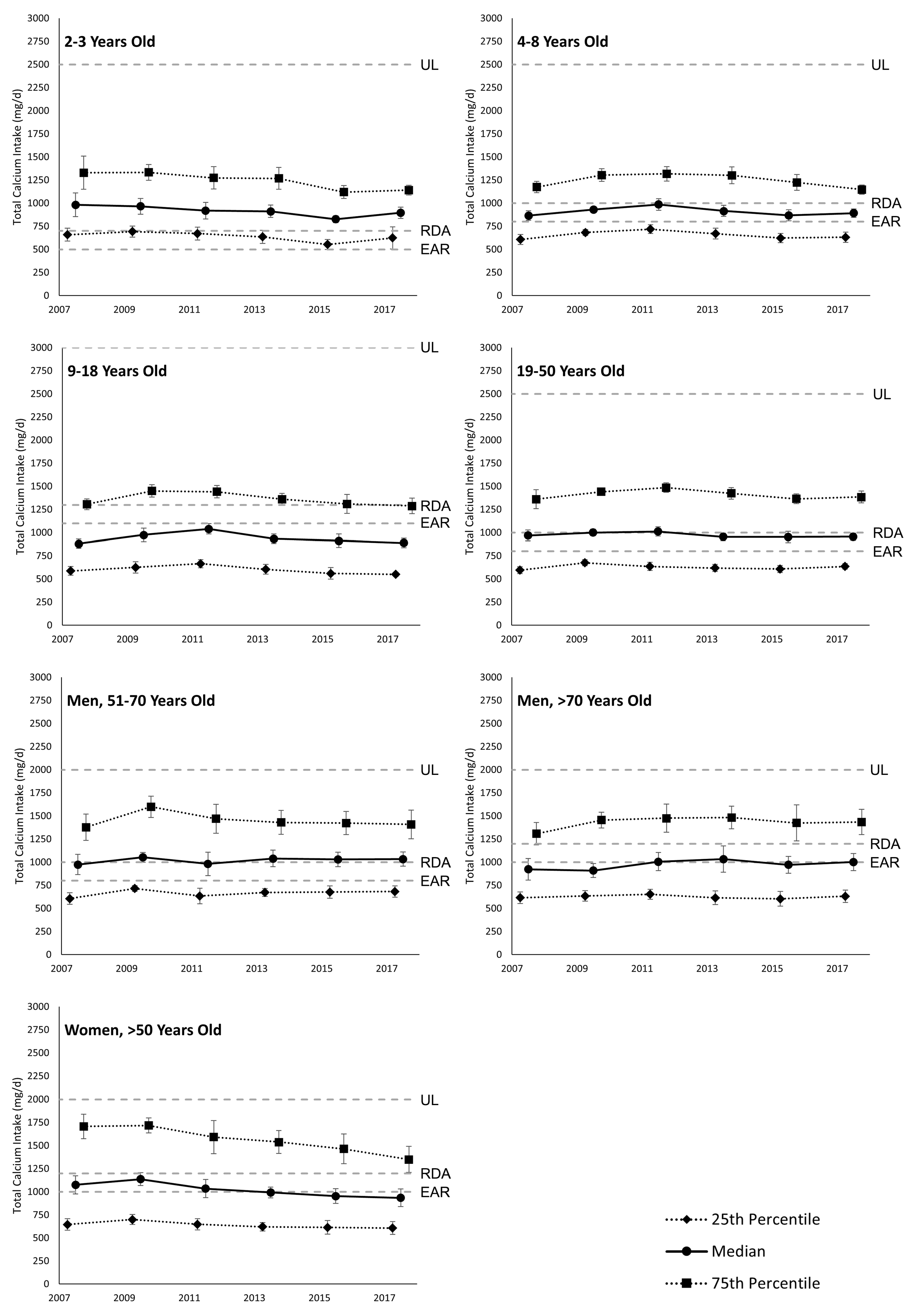
3.3. Total Daily Calcium Intake
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Life Stage Group | EAR | RDA | UL |
|---|---|---|---|
| 2–3 years old | 500 mg | 700 mg | 2500 mg |
| 4–8 years old | 800 mg | 1000 mg | 2500 mg |
| 9–18 years old * | 1100 mg | 1300 mg | 3000 mg |
| 19–50 years old * | 800 mg | 1000 mg | 2500 mg |
| Men | |||
| 51–70 years old | 800 mg | 1000 mg | 2000 mg |
| >70 years old | 1000 mg | 1200 mg | 2000 mg |
| Women | |||
| >50 years old | 1000 mg | 1200 mg | 2000 mg |
| Pregnancy or Lactation * | |||
| 14–18 years old | 1100 mg | 1300 mg | 3000 mg |
| 19–50 years old | 800 mg | 1000 mg | 2500 mg |
Appendix C

References
- Cormick, G.; Belizán, J.M. Calcium intake and health. Nutrients 2019, 11, 1606. [Google Scholar] [CrossRef]
- Yao, P.; Bennett, D.; Mafham, M.; Lin, X.; Chen, Z.; Armitage, J.; Clarke, R. Vitamin D and calcium for the prevention of fracture: A systematic review and meta-analysis. JAMA Netw. Open 2019, 2, e1917789. [Google Scholar] [CrossRef] [PubMed]
- Rizzoli, R.; Biver, E.; Brennan-Speranza, T.C. Nutritional intake and bone health. Lancet Diabetes Endocrinol. 2021, 9, 606–621. [Google Scholar] [CrossRef] [PubMed]
- Shen, X.; Gu, X.; Liu, Y.-Y.; Yang, L.; Zheng, M.; Jiang, L. Association between dietary calcium and depression among American adults: National health and nutrition examination survey. Front. Nutr. 2023, 10, 1042522. [Google Scholar] [CrossRef] [PubMed]
- Sllamniku Dalipi, Z.; Dragidella, F. Calcium and Vitamin D Supplementation as Non-Surgical Treatment for Periodontal Disease with a Focus on Female Patients: Literature Review. Dent. J. 2022, 10, 120. [Google Scholar] [CrossRef] [PubMed]
- Subramaniam, T.; Fauzi, M.B.; Lokanathan, Y.; Law, J.X. The role of calcium in wound healing. Int. J. Mol. Sci. 2021, 22, 6486. [Google Scholar] [CrossRef] [PubMed]
- Shlisky, J.; Mandlik, R.; Askari, S.; Abrams, S.; Belizan, J.M.; Bourassa, M.W.; Cormick, G.; Driller-Colangelo, A.; Gomes, F.; Khadilkar, A.; et al. Calcium deficiency worldwide: Prevalence of inadequate intakes and associated health outcomes. Ann. N. Y. Acad. Sci. 2022, 1512, 10–28. [Google Scholar] [CrossRef] [PubMed]
- Fleming, K.H.; Heimbach, J.T. Consumption of calcium in the US: Food sources and intake levels. J. Nutr. 1994, 124, 1426S–1430S. [Google Scholar] [CrossRef] [PubMed]
- Ajong, A.B.; Kenfack, B.; Ali, I.M.; Yakum, M.N.; Ukaogo, P.O.; Mangala, F.N.; Aljerf, L.; Telefo, P.B. Calcium supplementation in pregnancy: An analysis of potential determinants in an under-resourced setting. PLoS ONE 2023, 18, e0292303. [Google Scholar] [CrossRef]
- Sutter, D.O.; Bender, N. Nutrient status and growth in vegan children. Nutr. Res. 2021, 91, 13–25. [Google Scholar] [CrossRef]
- Beal, T.; White, J.M.; Arsenault, J.E.; Okronipa, H.; Hinnouho, G.-M.; Murira, Z.; Torlesse, H.; Garg, A. Micronutrient gaps during the complementary feeding period in South Asia: A Comprehensive Nutrient Gap Assessment. Nutr. Rev. 2021, 79, 26–34. [Google Scholar] [CrossRef]
- Hoy, M.K.; Goldman, J.D. Calcium intake of the US population: What we eat in America, NHANES 2009–2010. In FSRG Dietary Data Briefs; United States Department of Agriculture (USDA): Beltsville, MD, USA, 2014. [Google Scholar]
- U.S. Department of Agriculture; U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2020–2025; U.S. Department of Agriculture: Washington, DC, USA, 2020.
- Cifelli, C.J.; Fulgoni, K.; Fulgoni, V.L., III; Hess, J.M. Disparity in Dairy Servings Intake by Ethnicity and Age in NHANES 2015–2018. Curr. Dev. Nutr. 2023, 7, 100010. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Johns, R.A.; Stafford, R.S. Americans are not meeting current calcium recommendations. Am. J. Clin. Nutr. 2007, 85, 1361–1366. [Google Scholar] [CrossRef]
- Morgan, K.J.; Stampley, G.; Zabik, M.; Fischer, D.R. Magnesium and calcium dietary intakes of the US population. J. Am. Coll. Nutr. 1985, 4, 195–206. [Google Scholar] [CrossRef]
- Mangano, K.M.; Walsh, S.J.; Insogna, K.L.; Kenny, A.M.; Kerstetter, J.E. Calcium intake in the United States from dietary and supplemental sources across adult age groups: New estimates from the National Health and Nutrition Examination Survey 2003–2006. J. Am. Diet. Assoc. 2011, 111, 687–695. [Google Scholar] [CrossRef]
- Juul, F.; Parekh, N.; Martinez-Steele, E.; Monteiro, C.A.; Chang, V.W. Ultra-processed food consumption among US adults from 2001 to 2018. Am. J. Clin. Nutr. 2022, 115, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Steele, E.M.; Du, M.; Pomeranz, J.L.; O’Connor, L.E.; Herrick, K.A.; Luo, H.; Zhang, X.; Mozaffarian, D.; Zhang, F.F. Trends in consumption of ultraprocessed foods among US youths aged 2–19 years, 1999–2018. JAMA 2021, 326, 519–530. [Google Scholar] [CrossRef]
- Vieux, F.; Maillot, M.; Rehm, C.D.; Barrios, P.; Drewnowski, A. Trends in tap and bottled water consumption among children and adults in the United States: Analyses of NHANES 2011–16 data. Nutr. J. 2020, 19, 10. [Google Scholar] [CrossRef] [PubMed]
- Marriott, B.P.; Hunt, K.J.; Malek, A.M.; Newman, J.C. Trends in intake of energy and total sugar from sugar-sweetened beverages in the United States among children and adults, NHANES 2003–2016. Nutrients 2019, 11, 2004. [Google Scholar] [CrossRef]
- Drewnowski, A.; Rehm, C.D.; Constant, F. Water and beverage consumption among adults in the United States: Cross-sectional study using data from NHANES 2005–2010. BMC Public Health 2013, 13, 1068. [Google Scholar] [CrossRef]
- Drewnowski, A.; Rehm, C.D.; Constant, F. Water and beverage consumption among children age 4–13y in the United States: Analyses of 2005–2010 NHANES data. Nutr. J. 2013, 12, 85. [Google Scholar] [CrossRef] [PubMed]
- Della Corte, K.; Fife, J.; Gardner, A.; Murphy, B.L.; Kleis, L.; Della Corte, D.; Schwingshackl, L.; LeCheminant, J.D.; Buyken, A.E. World trends in sugar-sweetened beverage and dietary sugar intakes in children and adolescents: A systematic review. Nutr. Rev. 2021, 79, 274–288. [Google Scholar] [CrossRef] [PubMed]
- Dai, J.; Soto, M.J.; Dunn, C.G.; Bleich, S.N. Trends and patterns in sugar-sweetened beverage consumption among children and adults by race and/or ethnicity, 2003–2018. Public Health Nutr. 2021, 24, 2405–2410. [Google Scholar] [CrossRef] [PubMed]
- Ricciuto, L.; Fulgoni, V.L., III; Gaine, P.C.; Scott, M.O.; DiFrancesco, L. Trends in added sugars intake and sources among US children, adolescents, and teens using NHANES 2001–2018. J. Nutr. 2022, 152, 568–578. [Google Scholar] [CrossRef] [PubMed]
- DiFrancesco, L.; Fulgoni, V.L., III; Gaine, P.C.; Scott, M.O.; Ricciuto, L. Trends in added sugars intake and sources among US adults using the National Health and Nutrition Examination Survey (NHANES) 2001–2018. Front. Nutr. 2022, 9, 897952. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Giovannucci, E.; Rosner, B.; Willett, W.C.; Cho, E. Longitudinal and secular trends in dietary supplement use: Nurses’ health study and health professionals follow-up study, 1986–2006. J. Acad. Nutr. Diet. 2014, 114, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Kantor, E.D.; Rehm, C.D.; Du, M.; White, E.; Giovannucci, E.L. Trends in dietary supplement use among US adults from 1999–2012. JAMA 2016, 316, 1464–1474. [Google Scholar] [CrossRef]
- Cowan, A.E.; Tooze, J.A.; Gahche, J.J.; Eicher-Miller, H.A.; Guenther, P.M.; Dwyer, J.T.; Potischman, N.; Bhadra, A.; Carroll, R.J.; Bailey, R.L. Trends in overall and micronutrient-containing dietary supplement use in US adults and children, NHANES 2007–2018. J. Nutr. 2022, 152, 2789–2801. [Google Scholar] [CrossRef]
- Rooney, M.R.; Michos, E.D.; Hootman, K.C.; Harnack, L.; Lutsey, P.L. Trends in calcium supplementation, National Health and Nutrition Examination Survey (NHANES) 1999–2014. Bone 2018, 111, 23–27. [Google Scholar] [CrossRef]
- National Center for Health Statistics. About the National Health and Nutrition Examination Survey. Available online: https://www.cdc.gov/nchs/nhanes/about_nhanes.htm (accessed on 2 May 2023).
- Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey—Survey Participants. Available online: https://www.cdc.gov/nchs/nhanes/participant/participant-confidentiality.htm (accessed on 2 May 2023).
- Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey—NCHS Ethics Review Board (ERB) Approval. Available online: https://www.cdc.gov/nchs/nhanes/irba98.htm (accessed on 2 May 2023).
- Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey—Examination Consent. Available online: https://www.cdc.gov/nchs/data/nhanes/nhanes_01_02/nh.cnstbrch.pdf (accessed on 2 May 2023).
- Millen, B.E.; Quatromoni, P.A.; Gagnon, D.R.; Cupples, L.A.; Franz, M.M.; D’Agostino, R.B. Dietary patterns of men and women suggest targets for health promotion: The Framingham Nutrition Studies. Am. J. Health Promot. 1996, 11, 42–52. [Google Scholar] [CrossRef] [PubMed]
- Rosinger, A.Y.; Patel, A.I.; Weaks, F. Examining recent trends in the racial disparity gap in tap water consumption: NHANES 2011–2018. Public Health Nutr. 2022, 25, 207–213. [Google Scholar] [CrossRef]
- Agarwal, S.; Fulgoni, V.L., III. Association of Pork (All Pork, Fresh Pork and Processed Pork) Consumption with Nutrient Intakes and Adequacy in US Children (Age 2–18 Years) and Adults (Age 19+ Years): NHANES 2011–2018 Analysis. Nutrients 2023, 15, 2293. [Google Scholar] [CrossRef]
- Overcash, F.; Reicks, M. Diet quality and eating practices among Hispanic/Latino men and women: NHANES 2011–2016. Int. J. Environ. Res. Public Health 2021, 18, 1302. [Google Scholar] [CrossRef] [PubMed]
- Qin, Y.; Cifelli, C.J.; Agarwal, S.; Fugoni, V.L. Dairy food consumption is beneficially linked with iodine status in US children and adults: NHANES 2001–2018. Public Health Nutr. 2023, 26, 1828–1839. [Google Scholar] [CrossRef]
- Murakami, K.; Livingstone, M.B.E. Prevalence and characteristics of misreporting of energy intake in US children and adolescents: National Health and Nutrition Examination Survey (NHANES) 2003–2012. Br. J. Nutr. 2016, 115, 294–304. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.; Rooney, M.R.; Wallace, A.S.; Kim, H.; Echouffo-Tcheugui, J.B.; McEvoy, J.W.; Ndumele, C.; Christenson, R.H.; Selvin, E.; Rebholz, C.M. Associations between diet quality and NT-proBNP in US adults, NHANES 1999–2004. Am. J. Prev. Cardiol. 2023, 16, 100528. [Google Scholar] [CrossRef] [PubMed]
- Del Valle, H.B.; Yaktine, A.L.; Taylor, C.L.; Ross, A.C. Dietary Reference Intakes for Calcium and Vitamin D; National Academies Press (US): Washington, DC, USA, 2011. [Google Scholar]
- Centers for Disease Control and Prevention. SAS Survey Procedure Tips. Available online: https://wwwn.cdc.gov/nchs/nhanes/tutorials/softwaretips.aspx (accessed on 2 May 2023).
- Centers for Disease Control and Prevention. Weighting. Available online: https://wwwn.cdc.gov/nchs/nhanes/tutorials/Weighting.aspx (accessed on 2 May 2023).
- Kaptein, M.; De Ruyter, B.; Markopoulos, P.; Aarts, E. Adaptive persuasive systems: A study of tailored persuasive text messages to reduce snacking. ACM Trans. Interact. Intell. Syst. (TiiS) 2012, 2, 10. [Google Scholar] [CrossRef]
- Korda, H.; Itani, Z. Harnessing social media for health promotion and behavior change. Health Promot. Pract. 2013, 14, 15–23. [Google Scholar] [CrossRef]
- Gough, A.; Hunter, R.F.; Ajao, O.; Jurek, A.; McKeown, G.; Hong, J.; Barrett, E.; Ferguson, M.; McElwee, G.; McCarthy, M. Tweet for behavior change: Using social media for the dissemination of public health messages. JMIR Public Health Surveill. 2017, 3, e6313. [Google Scholar] [CrossRef]
- Liu, G.; Sun, S.; Guo, B.; Miao, B.; Luo, Z.; Xia, Z.; Ying, D.; Liu, F.; Guo, B.; Tang, J. Bioactive peptide isolated from casein phosphopeptides promotes calcium uptake in vitro and in vivo. Food Funct. 2018, 9, 2251–2260. [Google Scholar] [CrossRef]
- Rosanoff, A.; Weaver, C.M.; Rude, R.K. Suboptimal magnesium status in the United States: Are the health consequences underestimated? Nutr. Rev. 2012, 70, 153–164. [Google Scholar] [CrossRef]
- Bonjour, J.-P. Calcium and phosphate: A duet of ions playing for bone health. J. Am. Coll. Nutr. 2011, 30, 438S–448S. [Google Scholar] [CrossRef] [PubMed]
- Veldurthy, V.; Wei, R.; Oz, L.; Dhawan, P.; Jeon, Y.H.; Christakos, S. Vitamin D, calcium homeostasis and aging. Bone Res. 2016, 4, 16041. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Liu, F.; Liu, G.; Miao, J.; Xiao, H.; Xiao, J.; Qiu, Z.; Luo, Z.; Tang, J.; Cao, Y. Effects of casein phosphopeptides on calcium absorption and metabolism bioactivity in vitro and in vivo. Food Funct. 2018, 9, 5220–5229. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Guo, B.; Sun, S.; Luo, M.; Liu, F.; Miao, J.; Tang, J.; Huang, Y.; Cao, Y.; Song, M. Promoting the Calcium-Uptake Bioactivity of Casein Phosphopeptides in vitro and in vivo. Front. Nutr. 2021, 8, 743791. [Google Scholar] [CrossRef] [PubMed]
- Trailokya, A.; Srivastava, A.; Bhole, M.; Zalte, N. Calcium and calcium salts. J. Assoc. Physicians India 2017, 65, 100–103. [Google Scholar] [PubMed]
- Zhang, Y.Y.; Stockmann, R.; Ng, K.; Ajlouni, S. Opportunities for plant-derived enhancers for iron, zinc, and calcium bioavailability: A review. Compr. Rev. Food Sci. Food Saf. 2021, 20, 652–685. [Google Scholar] [CrossRef]
- Shkembi, B.; Huppertz, T. Calcium absorption from food products: Food matrix effects. Nutrients 2021, 14, 180. [Google Scholar] [CrossRef]
| Characteristics | No. of Participants (Weighted %) by NHANES Cycle a | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1999–2000 (n = 7878) | 2001–2002 (n = 8855) | 2003–2004 (n = 8099) | 2005–2006 (n = 8380) | 2007–2008 (n = 8381) | 2009–2010 (n = 8922) | 2011–2012 (n = 7808) | 2013–2014 (n = 7879) | 2015–2016 (n = 7738) | 2017–2018 (n = 6940) | |
| Sex | ||||||||||
| Men | 3828 (48.6%) | 4288 (48.7%) | 3955 (49.1%) | 4065 (48.8%) | 4207 (47.9%) | 4436 (48.7%) | 3920 (49.4%) | 3843 (49.3%) | 3790 (48.7%) | 3383 (48.7%) |
| Women | 4050 (51.4%) | 4567 (51.3%) | 4144 (50.9%) | 4315 (51.2%) | 4174 (52.1%) | 4486 (51.3%) | 3888 (50.6%) | 4036 (50.7%) | 3948 (51.3%) | 3557 (51.3%) |
| Age Group | ||||||||||
| 2–8 years | 1113 (11.1%) | 1399 (10.1%) | 1175 (9.66%) | 1372 (9.82%) | 1379 (9.91%) | 1419 (9.76%) | 1415 (10.0%) | 1189 (9.10%) | 1157 (9.13%) | 894 (8.90%) |
| 9–18 years | 2387 (14.7%) | 2562 (15.3%) | 2303 (15.0%) | 2326 (14.6%) | 1533 (14.1%) | 1670 (14.2%) | 1524 (13.3%) | 1644 (13.8%) | 1544 (13.6%) | 1319 (13.6%) |
| 19–59 years | 2873 (57.6%) | 3400 (58.8%) | 2987 (57.5%) | 3306 (57.4%) | 3553 (58.4%) | 3958 (57.6%) | 3390 (57.4%) | 3530 (57.0%) | 3395 (56.0%) | 2969 (55.4%) |
| ≥60 years | 1505 (16.6%) | 1494 (15.8%) | 1634 (17.9%) | 1376 (18.2%) | 1916 (17.6%) | 1875 (18.5%) | 1479 (19.4%) | 1516 (20.1%) | 1642 (21.2%) | 1758 (22.1%) |
| Race and Ethnicity | ||||||||||
| Mexican American | 2665 (7.60%) | 2218 (8.47%) | 1985 (8.95%) | 2204 (9.35%) | 1686 (9.59%) | 1941 (9.90%) | 1052 (9.70%) | 1334 (10.8%) | 1468 (10.7%) | 1011 (11.0%) |
| Other Hispanic | 467 (7.58%) | 398 (5.72%) | 257 (3.30%) | 269 (2.91%) | 970 (5.37%) | 945 (5.59%) | 809 (6.66%) | 745 (5.95%) | 1007 (6.71%) | 587 (6.88%) |
| Non-Hispanic White | 2686 (67.9%) | 3770 (69.5%) | 3402 (70.5%) | 3294 (69.6%) | 3490 (67.7%) | 3847 (65.9%) | 2495 (63.3%) | 2985 (62.8%) | 2495 (61.3%) | 2423 (59.3%) |
| Non-Hispanic Black | 1784 (11.6%) | 2133 (11.6%) | 2119 (12.0%) | 2207 (12.2%) | 1878 (12.0%) | 1657 (12.0%) | 2167 (12.4%) | 1697 (11.8%) | 1653 (11.6%) | 1600 (11.6%) |
| Other race or ethnicity b | 276 (5.39%) | 336 (4.68%) | 336 (5.17%) | 406 (5.89%) | 357 (5.34%) | 532 (6.63%) | 1285 (7.94%) | 1118 (8.69%) | 1115 (9.74%) | 1319 (11.2%) |
| Pregnancy c | ||||||||||
| Pregnant | 244 (5.58%) | 261 (4.65%) | 223 (4.76%) | 315 (5.47%) | 46 (2.25%) | 48 (2.94%) | 36 (2.15%) | 43 (2.59%) | 48 (3.06%) | 38 (2.64%) |
| Not pregnant | 492 (36.2%) | 625 (39.7%) | 675 (47.1%) | 781 (50.3%) | 702 (37.6%) | 741 (35.2%) | 542 (32.8%) | 631 (35.6%) | 621 (36.9%) | 577 (39.2%) |
| Refused, do not know, or missing | 1241 (58.2%) | 1343 (55.7%) | 1057 (48.1%) | 1072 (44.2%) | 1035 (60.1%) | 1252 (61.9%) | 1092 (65.1%) | 1216 (61.8%) | 1106 (60.1%) | 898 (58.2%) |
| Lactation c | ||||||||||
| Currently breastfeeding | 42 (1.60%) | 61 (2.74%) | 50 (2.45%) | 49 (2.23%) | 30 (1.65%) | 32 (1.11%) | 21 (1.58%) | 40 (2.73%) | 41 (2.36%) | 38 (2.65%) |
| Not breastfeeding | 155 (7.28%) | 175 (6.54%) | 115 (4.79%) | 162 (6.12%) | 99 (4.95%) | 113 (5.01%) | 69 (3.27%) | 101 (6.87%) | 118 (7.36%) | 102 (8.80%) |
| Refused, do not know, or missing | 1780 (91.1%) | 1993 (90.7%) | 1790 (92.8%) | 1957 (91.6%) | 1654 (93.4%) | 1896 (93.9%) | 1580 (95.2%) | 1749 (90.4%) | 1616 (90.3%) | 1373 (88.6%) |
| Mean Daily Dietary Calcium Intake (mg/d), (95% CI) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1999–2000 | 2001–2002 | 2003–2004 | 2005–2006 | 2007–2008 | 2009–2010 | 2011–2012 | 2013–2014 | 2015–2016 | 2017–2018 | |
| Total Diet | ||||||||||
| Men | 948 (919, 977) | 1019 (977, 1061) | 1024 (986, 1062) | 1056 (1022, 1089) | 1041 (996, 1085) | 1141 (1116, 1165) | 1135 (1093, 1177) | 1091 (1066, 1116) | 1060 (1024, 1096) | 1079 (1044, 1114) |
| Women | 753 (723, 782) | 782 (755, 810) | 804 (771, 837) | 862 (824, 900) | 843 (796, 890) | 910 (896, 925) | 888 (863, 913) | 858 (837, 879) | 856 (820, 891) | 860 (834, 886) |
| 2–8 years old | 845 (791, 898) | 950 (909, 991) | 999 (938, 1061) | 951 (913, 988) | 951 (906, 995) | 1022 (981, 1064) | 1033 (989, 1076) | 998 (943, 1052) | 936 (896, 976) | 941 (909, 973) |
| 9–18 years old | 902 (857, 947) | 988 (920, 1057) | 1028 (951, 1106) | 999 (932, 1066) | 989 (934, 1044) | 1081 (1020, 1141) | 1084 (1031, 1137) | 1037 (987, 1088) | 1012 (946, 1077) | 981 (929, 1033) |
| 19–59 years old | 869 (834, 903) | 910 (868, 952) | 914 (874, 954) | 987 (943, 1030) | 961 (909, 1012) | 1049 (1027, 1072) | 1032 (996, 1068) | 988 (959, 1016) | 990 (951, 1029) | 1005 (975, 1034) |
| ≥60 years old | 728 (689, 767) | 730 (695, 765) | 762 (728, 795) | 831 (787, 876) | 813 (768, 858) | 894 (864, 925) | 883 (835, 931) | 876 (847, 905) | 835 (784, 887) | 872 (826, 918) |
| Mexican American | 825 (793, 857) | 920 (872, 967) | 957 (885, 1029) | 954 (913, 995) | 925 (879, 971) | 998 (951, 1046) | 1098 (1050, 1145) | 1038 (976, 1099) | 986 (961, 1012) | 1022 (985, 1059) |
| Other Hispanic | 805 (740, 870) | 842 (785, 899) | 785 (714, 855) | 875 (776, 975) | 969 (933, 1006) | 960 (922, 999) | 955 (912, 998) | 955 (900, 1011) | 936 (873, 998) | 951 (866, 1036) |
| Non-Hispanic White | 894 (848, 941) | 947 (906, 988) | 955 (923, 986) | 1001 (959, 1042) | 972 (920, 1025) | 1073 (1046, 1100) | 1048 (1018, 1079) | 1007 (980, 1034) | 995 (957, 1032) | 989 (961, 1017) |
| Non-Hispanic Black | 666 (637, 695) | 687 (658, 716) | 716 (674, 759) | 789 (752, 826) | 796 (757, 836) | 858 (825, 892) | 860 (811, 908) | 829 (793, 865) | 794 (751, 837) | 849 (816, 882) |
| Other race or ethnicity | 740 (592, 888) | 714 (649, 779) | 791 (672, 910) | 826 (763, 889) | 809 (743, 875) | 905 (846, 965) | 877 (833, 921) | 854 (812, 895) | 879 (816, 942) | 922 (867, 976) |
| Overall | 848 (819, 876) | 898 (868, 928) | 912 (879, 945) | 957 (923, 990) | 938 (896, 980) | 1022 (1009, 1036) | 1010 (982, 1038) | 973 (953, 993) | 955 (920, 991) | 966 (942, 991) |
| Diet and Dietary Supplements | ||||||||||
| Men | NA * | NA * | NA * | NA * | 1123 (1071, 1175) | 1223 (1196, 1250) | 1206 (1160, 1252) | 1166 (1133, 1199) | 1130 (1090, 1169) | 1135 (1097, 1173) |
| Women | NA * | NA * | NA * | NA * | 1042 (976, 1109) | 1101 (1085, 1118) | 1048 (1005, 1091) | 1025 (996, 1055) | 994 (945, 1042) | 991 (960, 1021) |
| 2–8 years old | NA * | NA * | NA * | NA * | 965 (919, 1010) | 1041 (995, 1087) | 1044 (1000, 1087) | 1008 (952, 1064) | 943 (902, 984) | 945 (914, 977) |
| 9–18 years old | NA * | NA * | NA * | NA * | 1019 (961, 1077) | 1105 (1044, 1166) | 1103 (1052, 1153) | 1056 (1005, 1106) | 1026 (956, 1096) | 994 (940, 1047) |
| 19–59 years old | NA * | NA * | NA * | NA * | 1098 (1035, 1161) | 1177 (1152, 1203) | 1134 (1085, 1183) | 1099 (1065, 1133) | 1077 (1036, 1118) | 1086 (1052, 1120) |
| ≥60 years old | NA * | NA * | NA * | NA * | 1139 (1055, 1223) | 1214 (1179, 1249) | 1161 (1107, 1215) | 1148 (1107, 1189) | 1088 (1019, 1156) | 1086 (1030, 1141) |
| Mexican American | NA * | NA * | NA * | NA * | 975 (930, 1021) | 1051 (1001, 1101) | 1141 (1090, 1192) | 1078 (1013, 1144) | 1032 (1010, 1053) | 1064 (1020, 1108) |
| Other Hispanic | NA * | NA * | NA * | NA * | 1038 (996, 1080) | 1040 (993, 1087) | 1028 (983, 1073) | 1007 (950, 1063) | 985 (915, 1056) | 1011 (930, 1092) |
| Non-Hispanic White | NA * | NA * | NA * | NA * | 1151 (1080, 1223) | 1244 (1214, 1273) | 1191 (1151, 1232) | 1162 (1129, 1195) | 1126 (1082, 1169) | 1106 (1079, 1134) |
| Non-Hispanic Black | NA * | NA * | NA * | NA * | 865 (828, 902) | 930 (886, 974) | 928 (873, 983) | 893 (857, 930) | 843 (802, 884) | 899 (864, 935) |
| Other race or ethnicity | NA * | NA * | NA * | NA * | 911 (831, 991) | 1014 (944, 1084) | 977 (934, 1021) | 963 (920, 1007) | 987 (919, 1055) | 1014 (955, 1073) |
| Overall | NA * | NA * | NA* | NA * | 1081 (1026, 1136) | 1160 (1144, 1177) | 1126 (1087, 1165) | 1095 (1068, 1121) | 1060 (1016, 1103) | 1061 (1035, 1086) |
| From 1999–2000 to 2017–2018 | From 1999–2000 to 2007–2008 | From 2009–2010 to 2017–2018 | ||||
|---|---|---|---|---|---|---|
| Coefficient Estimate (mg/d·10 years−1) | p for Trend | Coefficient Estimate (mg/d·10 years−1) | p for Trend | Coefficient Estimate (mg/d·10 years−1) | p for Trend | |
| Total Diet | ||||||
| Men | 62.5 (43.5, 81.5) | <0.001 | 110 (49.7, 170) | <0.001 | −99.0 (−152, −46.5) | <0.001 |
| Women | 55.2 (38.8, 71.7) | <0.001 | 129 (67.5, 190) | <0.001 | −66.6 (−104, −29.6) | <0.001 |
| 2–8 years old | 34.7 (8.23, 61.2) | <0.05 | 108 (28.6, 188) | <0.01 | −130 (−191, −69.3) | <0.001 |
| 9–18 years old | 36.7 (4.46, 68.8) | <0.05 | 90.5 (3.97, 177) | <0.05 | −135 (−226, −44.1) | <0.01 |
| 19–59 years old | 70.5 (50.8, 90.3) | <0.001 | 129 (59.3, 199) | <0.001 | −65.5 (−112, −19.5) | <0.01 |
| ≥60 years old | 80.1 (56.5, 104) | <0.001 | 136 (69.3, 202) | <0.001 | −44.9 (−113, 22.7) | 0.19 |
| Mexican American | 88.1 (61.3, 115) | <0.001 | 105 (30.9, 179) | <0.01 | −33.5 (−113, 45.6) | 0.40 |
| Other Hispanic | 84.9 (42.9, 127) | <0.001 | 183 (97.6, 269) | <0.001 | −18.9 (−123.0, 85) | 0.72 |
| Non-Hispanic White | 51.0 (30.3, 71.7) | <0.001 | 104 (26.4, 181) | <0.01 | −111 (−157, −64.8) | <0.001 |
| Non-Hispanic Black | 95.8 (75.4, 116) | <0.001 | 182 (124, 240) | <0.001 | −42.6 (−100, 15.3) | 0.15 |
| Other race or ethnicity | 95.3 (47.5, 143) | <0.001 | 123 (−51.9, 299) | 0.16 | 31.3 (−57.4, 120) | 0.48 |
| Overall | 59.0 (43.1, 75.0) | <0.001 | 118 (61.9, 175) | <0.001 | −83.2 (−119, −46.9) | <0.001 |
| Diet and Dietary Supplements | ||||||
| Men | NA * | NA * | NA * | NA * | −126 (−182, −69.9) | <0.001 |
| Women | NA * | NA * | NA * | NA * | −137 (−184, −89.8) | <0.001 |
| 2–8 years old | NA * | NA * | NA * | NA * | −147 (−210, −83.2) | <0.001 |
| 9–18 years old | NA * | NA * | NA * | NA * | −150 (−242, −57.4) | <0.01 |
| 19–59 years old | NA * | NA * | NA * | NA * | −120 (−173, −66.2) | <0.001 |
| ≥60 years old | NA * | NA * | NA * | NA * | −163 (−244, −82.4) | <0.001 |
| Mexican American | NA * | NA * | NA * | NA * | −42.1 (−126, 42.0) | 0.32 |
| Other Hispanic | NA * | NA * | NA * | NA * | −48.6 (−152, 54.9) | 0.35 |
| Non-Hispanic White | NA * | NA * | NA * | NA * | −170 (−220, −121) | <0.001 |
| Non-Hispanic Black | NA * | NA * | NA * | NA * | −73.8 (−142, −5.81) | <0.05 |
| Other race or ethnicity | NA * | NA * | NA * | NA * | 17.7 (−80.7, 116) | 0.72 |
| Overall | NA * | NA * | NA * | NA * | −132 (−175, −90.0) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, Z.; Li, Y.; Ba, D.M.; Veldheer, S.J.; Sun, L.; Geng, T.; Gao, X. Trends in Calcium Intake among the US Population: Results from the NHANES (1999–2018). Nutrients 2024, 16, 726. https://doi.org/10.3390/nu16050726
Yu Z, Li Y, Ba DM, Veldheer SJ, Sun L, Geng T, Gao X. Trends in Calcium Intake among the US Population: Results from the NHANES (1999–2018). Nutrients. 2024; 16(5):726. https://doi.org/10.3390/nu16050726
Chicago/Turabian StyleYu, Zhongyi, Yaqi Li, Djibril M. Ba, Susan J. Veldheer, Liang Sun, Tingting Geng, and Xiang Gao. 2024. "Trends in Calcium Intake among the US Population: Results from the NHANES (1999–2018)" Nutrients 16, no. 5: 726. https://doi.org/10.3390/nu16050726
APA StyleYu, Z., Li, Y., Ba, D. M., Veldheer, S. J., Sun, L., Geng, T., & Gao, X. (2024). Trends in Calcium Intake among the US Population: Results from the NHANES (1999–2018). Nutrients, 16(5), 726. https://doi.org/10.3390/nu16050726