
Preventive Vitamin D Supplementation and Risk for COVID-19 Infection: A Systematic Review and Meta-Analysis

 ,
, 
Abstract
1. Introduction
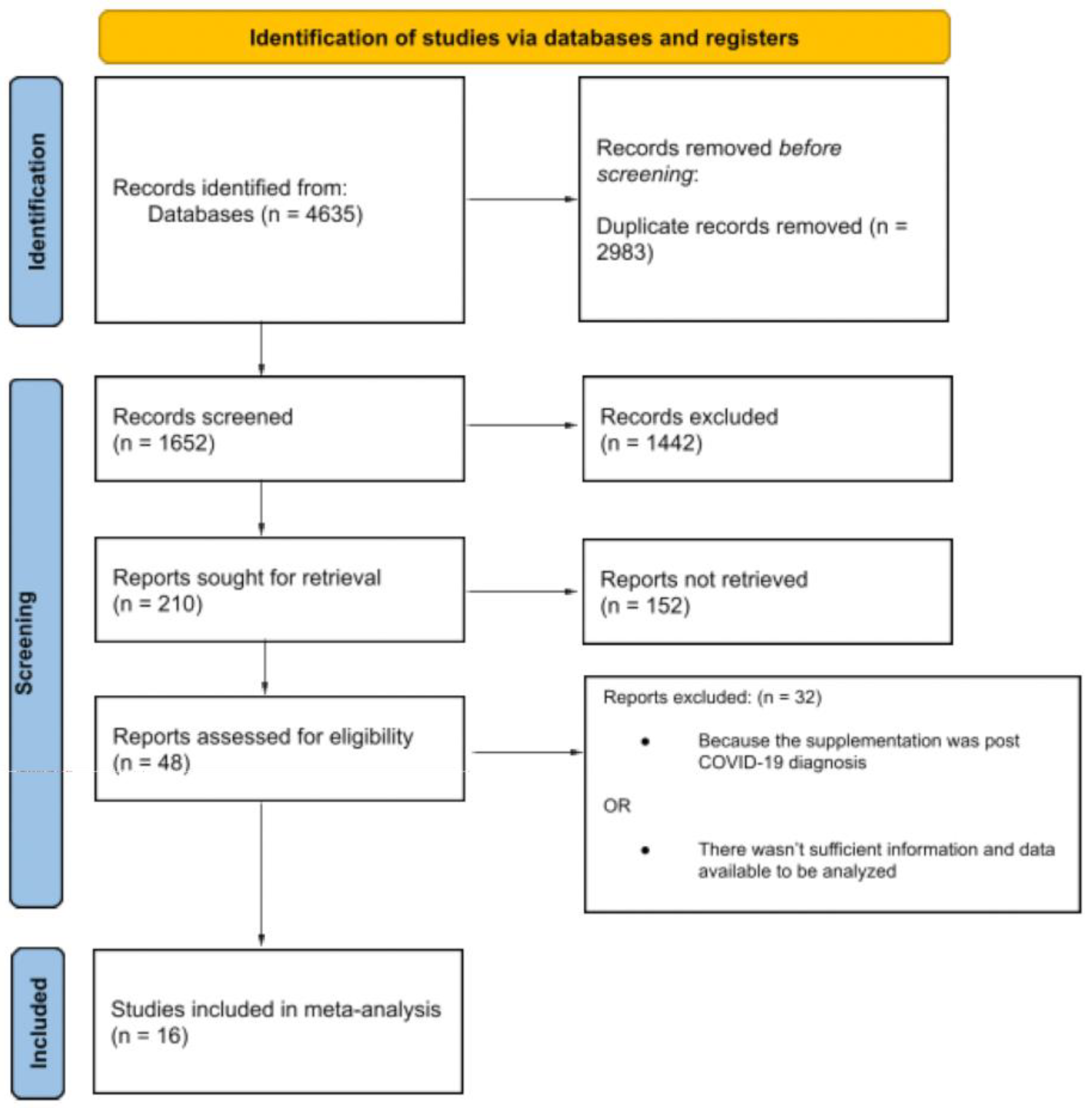
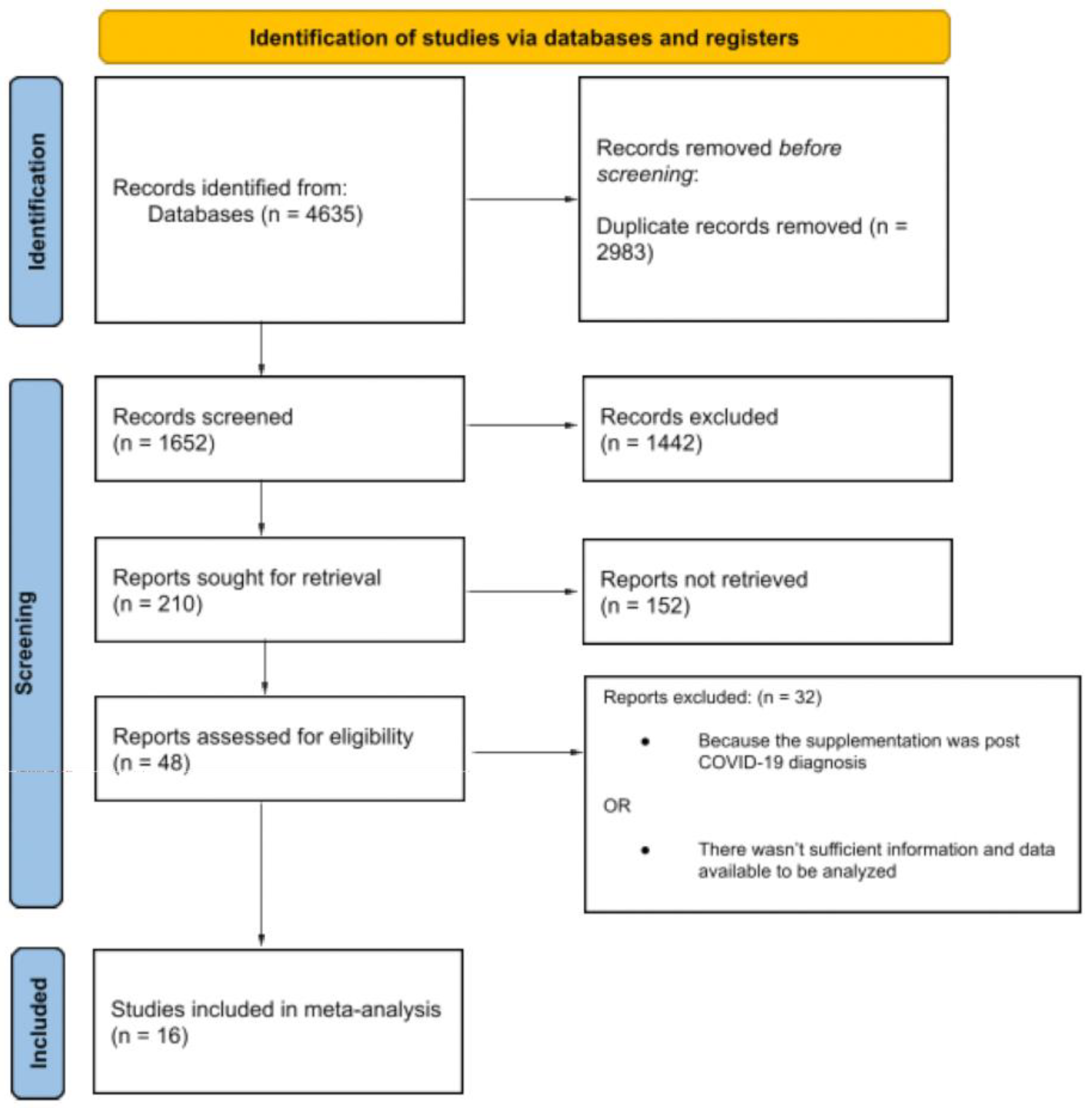
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Selection of Studies
2.3. Data Extraction and Risk of Bias Assessment
2.4. Statistical Analysis
3. Results
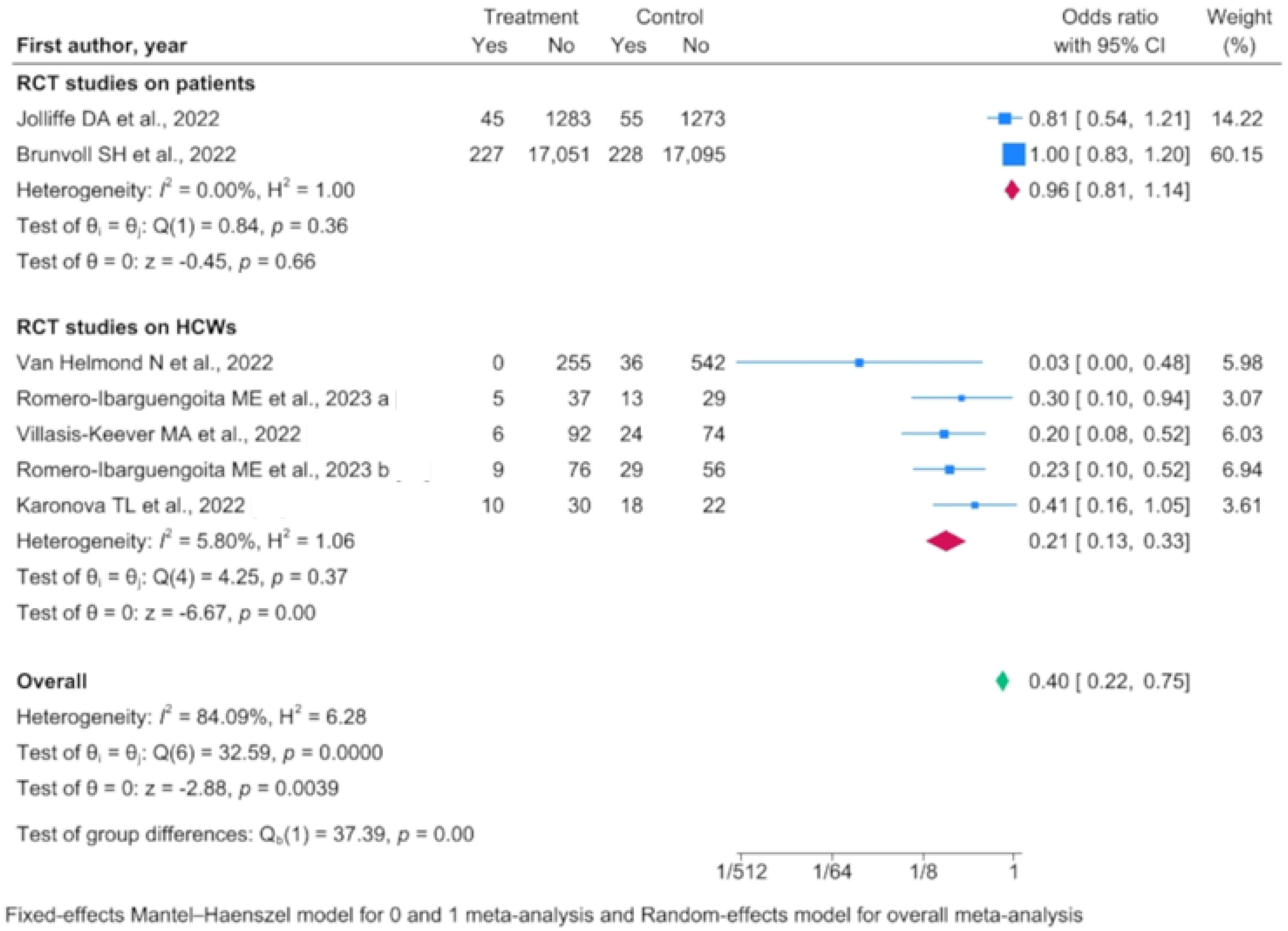
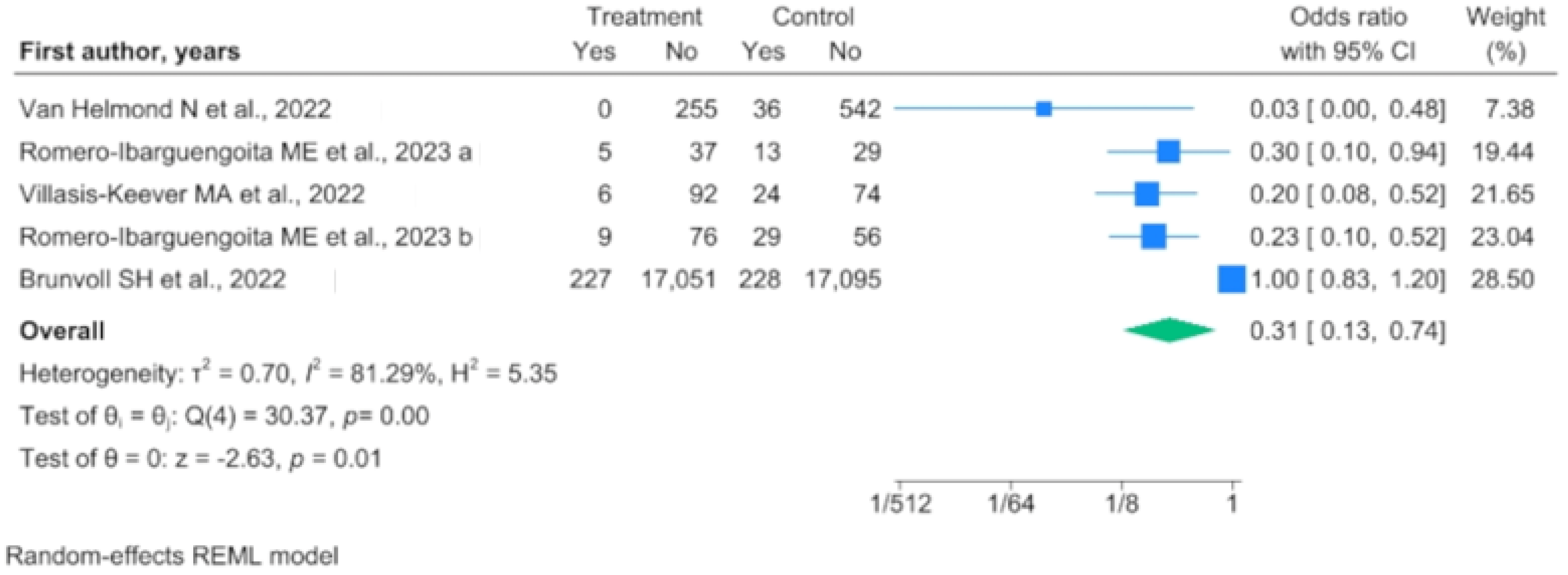
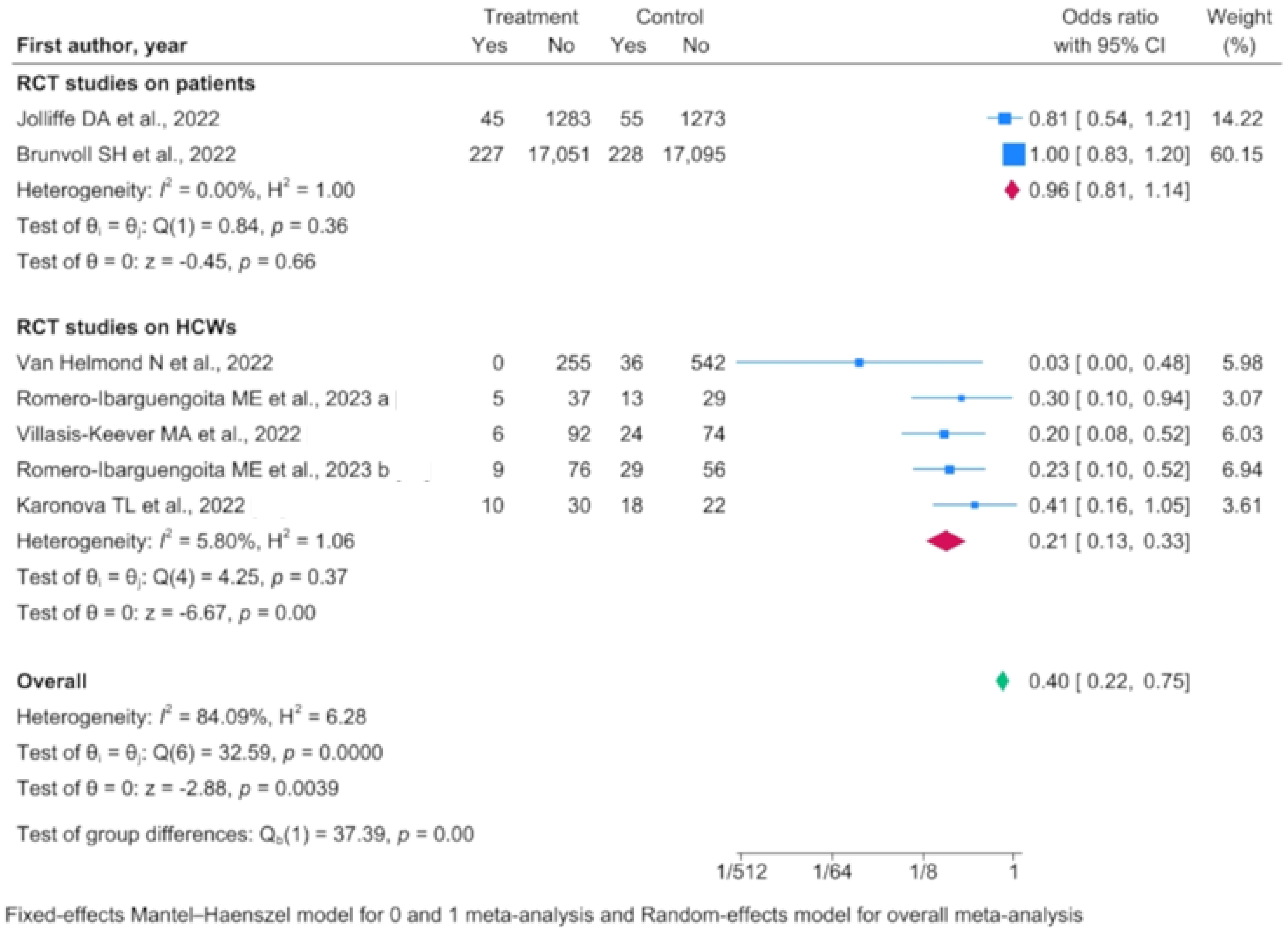
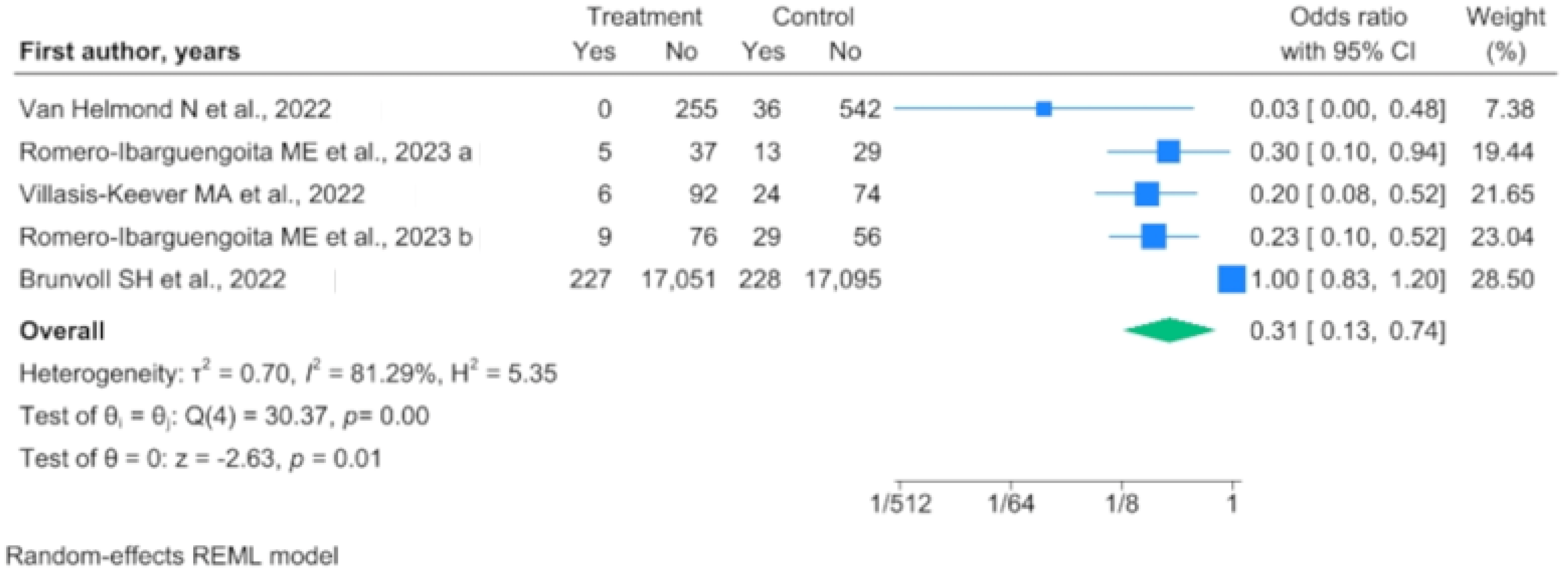
3.1. Evidence from RCTs on COVID-19 Infection Risk
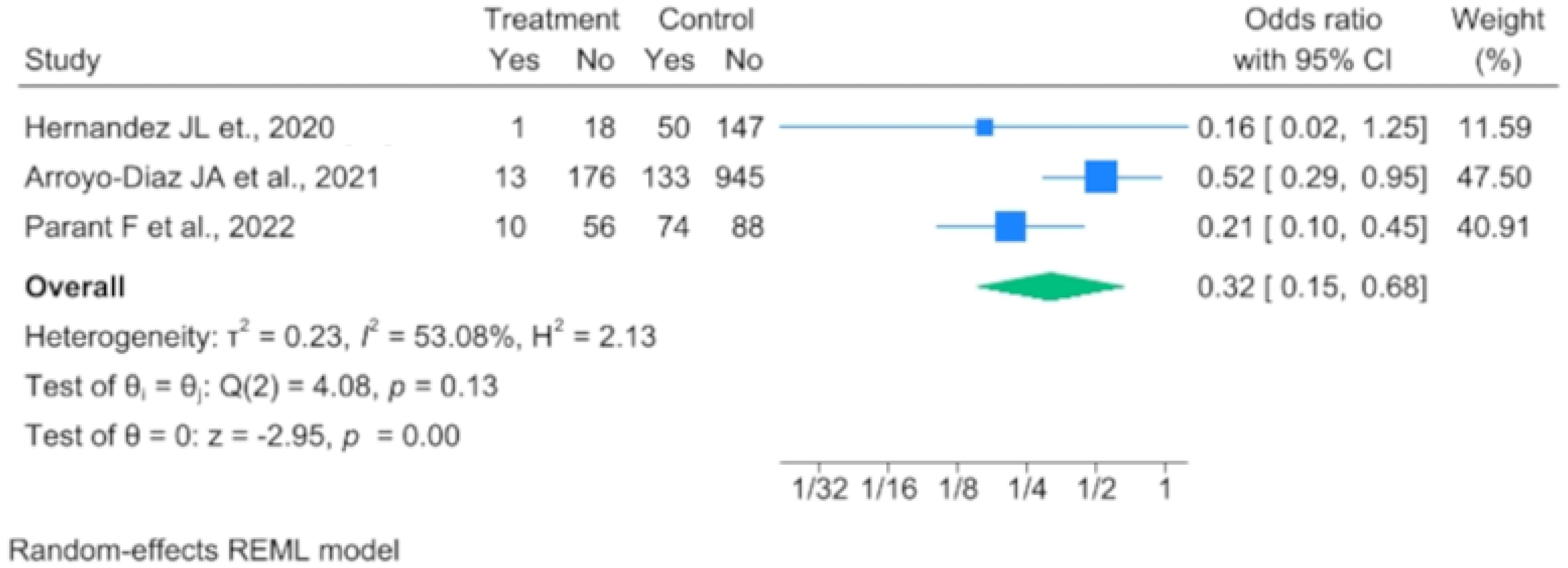
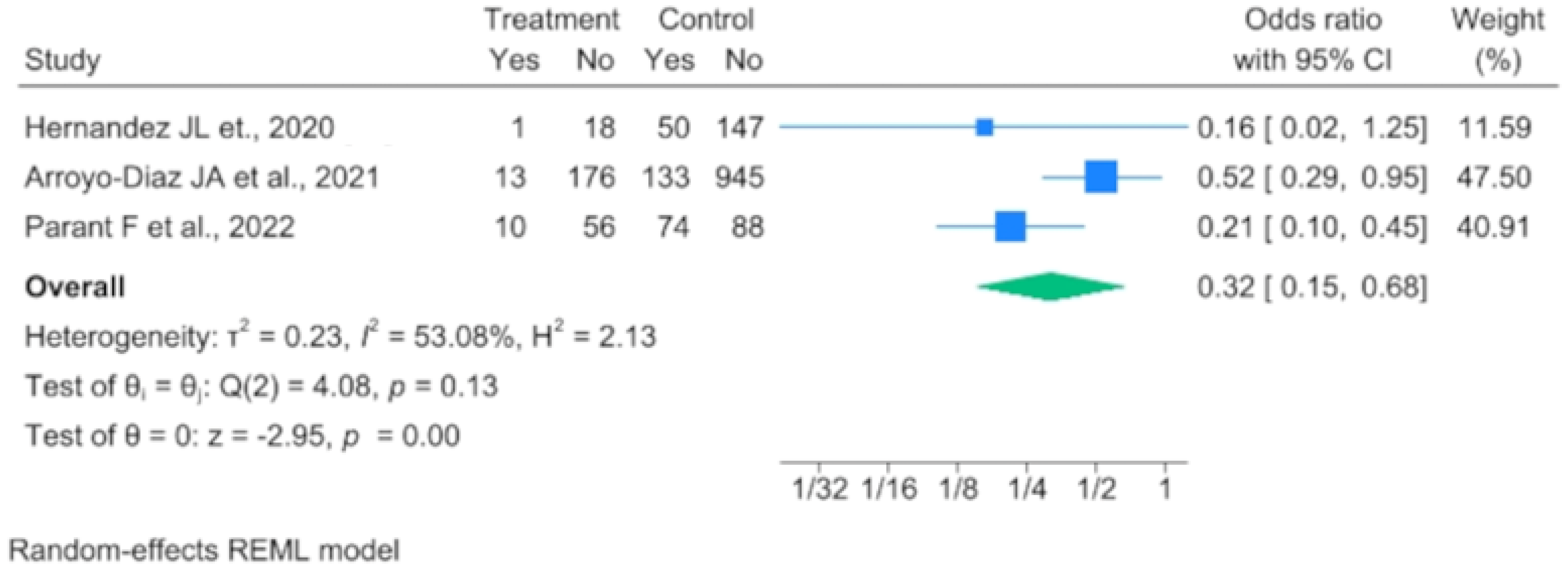
3.2. Evidence from Analytic Studies on COVID-19 Infection Risk
3.3. Evidence from RCTs and Analytical Studies on SARS-CoV-2-Related Mortality
3.4. Evidence from Analytical Studies on ICU Admissions
4. Discussion
Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ICU | intensive care unit |
| IC | confidence interval |
| OR | Odds Ratio |
| PTH | parathyroid hormone |
| COPD | Chronic Obstructive Pulmonary Disease |
| HCW | healthcare worker |
| RCT | randomized control trial |
References
- Bikle, D.D. Vitamin D: Newer Concepts of Its Metabolism and Function at the Basic and Clinical Level. J. Endocr. Soc. 2020, 4, bvz038. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D Deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (IOM). Dietary Reference Intakes for Calcium and Vitamin D; The National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Jones, G. Vitamin D. In Modern Nutrition in Health and Disease, 11th ed.; Ross, A.C., Caballero, B., Cousins, R.J., Tucker, K.L., Ziegler, T.R., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2014. [Google Scholar]
- Brown, L.L.; Cohen, B.; Tabor, D.; Zappalà, G.; Maruvada, P.; Coates, P.M. The vitamin D paradox in Black Americans: A systems-based approach to investigating clinical practice, research, and public health—Expert panel meeting report. BMC Proc. 2018, 12 (Suppl. S6), 6. [Google Scholar] [CrossRef] [PubMed]
- Vitamin D Fact Sheet for Health Professionals. Available online: https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/#:~:text=Serum%20concentrations%20of%2025(OH)D%20and%20health&text=Some%20people%20are%20potentially%20at,are%20sufficient%20for%20most%20people (accessed on 20 December 2023).
- Dawson-Hughes, B.; Heaney, R.P.; Holick, M.F.; Lips, P.; Meunier, P.J.; Vieth, R. Estimates of optimal vitamin D status. Osteoporos. Int. 2005, 16, 713–716. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, R.; Marcocci, C.; Carmeliet, G.; Bikle, D.; White, J.H.; Dawson-Hughes, B.; Lips, P.; Munns, C.F.; Lazaretti-Castro, M.; Giustina, A.; et al. Skeletal and Extraskeletal Actions of Vitamin D: Current Evidence and Outstanding Questions. Endocr. Rev. 2018, 40, 1109–1151. [Google Scholar] [CrossRef]
- Bouillon, R.; Quesada-Gomez, J.M. Vitamin D Endocrine System and COVID-19. JBMR Plus 2021, 5, e10576. [Google Scholar] [CrossRef]
- Gunville, C.F.; Mourani, P.M.; Ginde, A.A. The Role of Vitamin D in Prevention and Treatment of Infection. Inflamm. Allergy-Drug Targets 2013, 12, 239–245. [Google Scholar] [CrossRef]
- Nnoaham, K.E.; Clarke, A. Low serum vitamin D levels and tuberculosis: A systematic review and meta-analysis. Leuk. Res. 2008, 37, 113–119. [Google Scholar] [CrossRef]
- Jolliffe, D.A.; Greenberg, L.; Hooper, R.L.; Mathyssen, C.; Rafiq, R.; De Jongh, R.T.; Camargo, C.A.; Griffiths, C.J.; Janssens, W.; Martineau, A.R. Vitamin D to prevent exacerbations of COPD: Systematic review and meta-analysis of individual participant data from randomised controlled trials. Thorax 2019, 74, 337–345. [Google Scholar] [CrossRef]
- Lamers, M.M.; Haagmans, B.L. SARS-CoV-2 pathogenesis. Nat. Rev. Microbiol. 2022, 20, 270–284. [Google Scholar] [CrossRef]
- Gu, J.; Korteweg, C. Pathology and Pathogenesis of Severe Acute Respiratory Syndrome. Am. J. Pathol. 2007, 170, 1136–1147. [Google Scholar] [CrossRef] [PubMed]
- Sartini, M.; Del Puente, F.; Oliva, M.; Carbone, A.; Blasi Vacca, E.; Parisini, A.; Boni, S.; Bobbio, N.; Feasi, M.; Battistella, A.; et al. Riding the COVID Waves: Clinical Trends, Outcomes, and Remaining Pitfalls of the SARS-CoV-2 Pandemic: An Analysis of Two High-Incidence Periods at a Hospital in Northern Italy. J. Clin. Med. 2021, 10, 5239. [Google Scholar] [CrossRef] [PubMed]
- Ali, N. Role of vitamin D in preventing of COVID-19 infection, progression and severity. J. Infect. Public Health 2020, 13, 1373–1380. [Google Scholar] [CrossRef] [PubMed]
- Hastie, C.E.; Mackay, D.F.; Ho, F.; Celis-Morales, C.A.; Katikireddi, S.V.; Niedzwiedz, C.L.; Jani, B.D.; Welsh, P.; Mair, F.S.; Gray, S.R.; et al. Vitamin D concentrations and COVID-19 infection in UK Biobank. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 561–565. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- CRD42023469817. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=469817 (accessed on 11 October 2023).
- Ma, L.-L.; Wang, Y.-Y.; Yang, Z.-H.; Huang, D.; Weng, H.; Zeng, X.-T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med. Res. 2020, 7, 7. [Google Scholar] [CrossRef]
- Annweiler, G.; Corvaisier, M.; Gautier, J.; Dubée, V.; Legrand, E.; Sacco, G.; Annweiler, C. Vitamin D Supplementation Associated to Better Survival in Hospitalized Frail Elderly COVID-19 Patients: The GERIA-COVID Quasi-Experimental Study. Nutrients 2020, 12, 3377. [Google Scholar] [CrossRef]
- Hernández, J.L.; Nan, D.; Fernandez-Ayala, M.; García-Unzueta, M.; Hernández-Hernández, M.A.; López-Hoyos, M.; Muñoz-Cacho, P.; Olmos, J.M.; Gutiérrez-Cuadra, M.; Ruiz-Cubillán, J.J.; et al. Vitamin D Status in Hospitalized Patients with SARS-CoV-2 Infection. J. Clin. Endocrinol. Metab. 2021, 106, e1343–e1353. [Google Scholar] [CrossRef]
- Brunvoll, S.H.; Nygaard, A.B.; Ellingjord-Dale, M.; Holland, P.; Istre, M.S.; Kalleberg, K.T.; Søraas, C.L.; Holven, K.B.; Ulven, S.M.; Hjartåker, A.; et al. Prevention of COVID-19 and other acute respiratory infections with cod liver oil supplementation, a low dose vitamin D supplement: Quadruple blinded, randomised placebo controlled trial. BMJ 2022, 378, e071245. [Google Scholar] [CrossRef]
- Gibbons, J.B.; Norton, E.C.; McCullough, J.S.; Meltzer, D.O.; Lavigne, J.; Fiedler, V.C.; Gibbons, R.D. Association between vitamin D supplementation and COVID-19 infection and mortality. Sci. Rep. 2022, 12, 19397. [Google Scholar] [CrossRef]
- Jolliffe, D.A.; Holt, H.; Greenig, M.; Talaei, M.; Perdek, N.; Pfeffer, P.; Vivaldi, G.; Maltby, S.; Symons, J.; Barlow, N.L.; et al. Effect of a test-and-treat approach to vitamin D supplementation on risk of all cause acute respiratory tract infection and COVID-19: Phase 3 randomised controlled trial (CORONAVIT). BMJ 2022, 378, e071230. [Google Scholar] [CrossRef] [PubMed]
- Oristrell, J.; Oliva, J.C.; Casado, E.; Subirana, I.; Domínguez, D.; Toloba, A.; Balado, A.; Grau, M. Vitamin D supplementation and COVID-19 risk: A population-based, cohort study. J. Endocrinol. Investig. 2022, 45, 167–179. [Google Scholar] [CrossRef] [PubMed]
- Parant, F.; Bouloy, J.; Haesebaert, J.; Bendim’red, L.; Goldet, K.; Vanhems, P.; Henaff, L.; Gilbert, T.; Cuerq, C.; Blond, E.; et al. Vitamin D and COVID-19 Severity in Hospitalized Older Patients: Potential Benefit of Prehospital Vitamin D Supplementation. Nutrients 2022, 14, 1641. [Google Scholar] [CrossRef] [PubMed]
- Villasis-Keever, M.A.; López-Alarcón, M.G.; Miranda-Novales, G.; Zurita-Cruz, J.N.; Barrada-Vázquez, A.S.; González-Ibarra, J.; Martínez-Reyes, M.; Grajales-Muñiz, C.; Santacruz-Tinoco, C.E.; Martínez-Miguel, B.; et al. Efficacy and Safety of Vitamin D Supplementation to Prevent COVID-19 in Frontline Healthcare Workers. A Randomized Clinical Trial. Arch. Med. Res. 2022, 53, 423–430. [Google Scholar] [CrossRef]
- Romero-Ibarguengoitia, M.E.; Gutiérrez-González, D.; Cantú-López, C.; Sanz-Sánchez, M.; González-Cantú, A. Effect of Vitamin D3 Supplementation vs. Dietary–Hygienic Measures on SARS-CoV-2 Infection Rates in Hospital Workers with 25-Hydroxyvitamin D3 [25(OH)D3] Levels ≥20 ng/mL. Microorganisms 2023, 11, 282. [Google Scholar] [CrossRef] [PubMed]
- Cangiano, B.; Fatti, L.M.; Danesi, L.; Gazzano, G.; Croci, M.; Vitale, G.; Gilardini, L.; Bonadonna, S.; Chiodini, I.; Caparello, C.F.; et al. Mortality in an Italian nursing home during COVID-19 pandemic: Correlation with gender, age, ADL, vitamin D supplementation, and limitations of the diagnostic tests. Aging 2020, 12, 24522–24534. [Google Scholar] [CrossRef] [PubMed]
- Arroyo-Díaz, J.A.; Julve, J.; Vlacho, B.; Corcoy, R.; Ponte, P.; Román, E.; Navas-Méndez, E.; Llauradó, G.; Franch-Nadal, J.; Domingo, P.; et al. Previous Vitamin D Supplementation and Morbidity and Mortality Outcomes in People Hospitalised for COVID-19: A Cross-Sectional Study. Front. Public Health 2021, 9, 758347. [Google Scholar] [CrossRef] [PubMed]
- Cereda, E.; Bogliolo, L.; Lobascio, F.; Barichella, M.; Zecchinelli, A.L.; Pezzoli, G.; Caccialanza, R. Vitamin D supplementation and outcomes in coronavirus disease 2019 (COVID-19) patients from the outbreak area of Lombardy, Italy. Nutrition 2021, 82, 111055. [Google Scholar] [CrossRef]
- Ma, H.; Zhou, T.; Heianza, Y.; Qi, L. Habitual use of vitamin D supplements and risk of coronavirus disease 2019 (COVID-19) infection: A prospective study in UK Biobank. Am. J. Clin. Nutr. 2021, 113, 1275–1281. [Google Scholar] [CrossRef]
- Oristrell, J.; Oliva, J.C.; Subirana, I.; Casado, E.; Domínguez, D.; Toloba, A.; Aguilera, P.; Esplugues, J.; Fafián, P.; Grau, M. Association of Calcitriol Supplementation with Reduced COVID-19 Mortality in Patients with Chronic Kidney Disease: A Population-Based Study. Biomedicines 2021, 9, 509. [Google Scholar] [CrossRef] [PubMed]
- Karonova, T.L.; Golovatyuk, K.A.; Kudryavtsev, I.V.; Chernikova, A.T.; Mikhaylova, A.A.; Aquino, A.D.; Lagutina, D.I.; Zaikova, E.K.; Kalinina, O.V.; Golovkin, A.S.; et al. Effect of Cholecalciferol Supplementation on the Clinical Features and Inflammatory Markers in Hospitalized COVID-19 Patients: A Randomized, Open-Label, Single-Center Study. Nutrients 2022, 14, 2602. [Google Scholar] [CrossRef]
- van Helmond, N.; Brobyn, T.L.; LaRiccia, P.J.; Cafaro, T.; Hunter, K.; Roy, S.; Bandomer, B.; Ng, K.Q.; Goldstein, H.; Mitrev, L.V.; et al. Vitamin D3 Supplementation at 5000 IU Daily for the Prevention of Influenza-like Illness in Healthcare Workers: A Pragmatic Randomized Clinical Trial. Nutrients 2022, 15, 180. [Google Scholar] [CrossRef]
- Kaufman, H.W.; Niles, J.K.; Kroll, M.H.; Bi, C.; Holick, M.F. SARS-CoV-2 positivity rates associated with circulating 25-hydroxyvitamin D levels. PLoS ONE 2020, 15, e0239252. [Google Scholar] [CrossRef] [PubMed]
- Grant, W.B.; Lahore, H.; McDonnell, S.L.; Baggerly, C.A.; French, C.B.; Aliano, J.L.; Bhattoa, H.P. Evidence that Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths. Nutrients 2020, 12, 988. [Google Scholar] [CrossRef] [PubMed]
- Sabetta, J.R.; DePetrillo, P.; Cipriani, R.J.; Smardin, J.; Burns, L.A.; Landry, M.L. Serum 25-Hydroxyvitamin D and the Incidence of Acute Viral Respiratory Tract Infections in Healthy Adults. PLoS ONE 2010, 5, e11088. [Google Scholar] [CrossRef]
- Charoenngam, N.; Shirvani, A.; Reddy, N.; Vodopivec, D.M.; Apovian, C.M.; Holick, M.F. Association of Vitamin D Status with Hospital Morbidity and Mortality in Adult Hospitalized Patients with COVID-19. Endocr. Pract. 2021, 27, 271–278. [Google Scholar] [CrossRef]
- Liu, Y.; Clare, S.; D’erasmo, G.; Heilbronner, A.; Dash, A.; Krez, A.; Zaworski, C.; Haseltine, K.; Serota, A.; Miller, A.; et al. Vitamin D and SARS-CoV-2 Infection: SERVE Study (SARS-CoV-2 Exposure and the Role of Vitamin D among Hospital Employees). J. Nutr. 2023, 153, 1420–1426. [Google Scholar] [CrossRef]
- Martineau, A.R. Vitamin D in the prevention or treatment of COVID-19. Proc. Nutr. Soc. 2023, 82, 200–207. [Google Scholar] [CrossRef]
- Shah, K.; Varna, V.P.; Sharma, U.; Mavalankar, D. Does vitamin D supplementation reduce COVID-19 severity? A systematic review. QJM Int. J. Med. 2022, 115, 665–672. [Google Scholar] [CrossRef]
- Hariyanto, T.I.; Intan, D.; Hananto, J.E.; Harapan, H.; Kurniawan, A. Vitamin D supplementation and COVID-19 outcomes: A systematic review, meta-analysis and meta-regression. Rev. Med. Virol. 2022, 32, e2269. [Google Scholar] [CrossRef]
- Ødum, S.F.; Kongsbak-Wismann, M. Vitamin D and SARS-CoV-2. Basic Clin. Pharmacol. Toxicol. 2023, 133, 6–15. [Google Scholar] [CrossRef] [PubMed]
- Hu, X. The Effect of Active Vitamin D on Coronavirus. Highlights Sci. Eng. Technol. 2023, 30, 238–245. [Google Scholar] [CrossRef]
- Pal, R.; Banerjee, M.; Bhadada, S.K.; Shetty, A.J.; Singh, B.; Vyas, A. Vitamin D supplementation and clinical outcomes in COVID-19: A systematic review and meta-analysis. J. Endocrinol. Investig. 2022, 45, 53–68. [Google Scholar] [CrossRef]
- Beran, A.; Mhanna, M.; Srour, O.; Ayesh, H.; Stewart, J.M.; Hjouj, M.; Khokher, W.; Mhanna, A.S.; Ghazaleh, D.; Khader, Y.; et al. Clinical significance of micronutrient supplements in patients with coronavirus disease 2019: A comprehensive systematic review and meta-analysis. Clin. Nutr. ESPEN 2022, 48, 167–177. [Google Scholar] [CrossRef]
- Wang, J.; Feng, M.; Ying, S.; Zhou, J.; Li, X. Efficacy and Safety of Vitamin D Supplementation for Pulmonary Tu-berculosis: A Systematic Review and Meta-analysis. Iran. J. Public Health 2018, 47, 466–472. [Google Scholar]
- Charan, J.; Goyal, J.P.; Saxena, D.; Yadav, P. Vitamin D for prevention of respiratory tract infections: A systematic review and meta-analysis. J. Pharmacol. Pharmacother. 2012, 3, 300–303. [Google Scholar] [CrossRef] [PubMed]
- Autier, P.; Gandini, S. Vitamin D Supplementation and Total Mortality: A Meta-Analysis of Randomized Controlled Trials. Arch. Intern. Med. 2007, 167, 1730–1737. [Google Scholar] [CrossRef]
- Parisini, A.; Boni, S.; Vacca, E.B.; Bobbio, N.; Del Puente, F.; Feasi, M.; Prinapori, R.; Lattuada, M.; Sartini, M.; Cristina, M.L.; et al. Impact of the COVID-19 Pandemic on Epidemiology of Antibiotic Resistance in an Intensive Care Unit (ICU): The Experience of a North-West Italian Center. Antibiotics 2023, 12, 1278. [Google Scholar] [CrossRef]
- Petrakis, V.; Panopoulou, M.; Rafailidis, P.; Lemonakis, N.; Lazaridis, G.; Terzi, I.; Papazoglou, D.; Panagopoulos, P. The Impact of the COVID-19 Pandemic on Antimicrobial Resistance and Management of Bloodstream Infections. Pathogens 2023, 12, 780. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Search Strategy | Details | |
|---|---|---|
| Search string | (“COVID-19” OR “SARS-CoV-2” OR “coronavirus” OR “2019-nCoV”) AND (“vitamin D” OR “cholecalciferol” OR “calcitriol”) | |
| Inclusion criteria | P (patients/population): | Patients and healthcare workers |
| I (intervention/exposure): | Patients or healthcare workers supplemented with Vit D before COVID-19 infection | |
| C (comparisons/comparators): | Patients or healthcare workers who received the standard dose, a lower dose, no therapy or a placebo | |
| O (outcome): | COVID-19 incidence, ICU admissions and mortality | |
| S (study design): | RCT, cohort, cross-sectional, case–control and quasi-experimental studies were considered | |
| Databases | PubMed/MEDLINE, Scopus, Cochrane and Google Scholar | |
| Exclusion criteria | Experimental studies investigating in vitro or animal models Study design: editorial, commentaries, expert opinions, letters to the editor, review articles, original non-prospective studies and articles with insufficient details | |
| Time filter | None (from inception) | |
| Language filter | None (any language) | |
| References | Study Design, Setting | Participants | Vitamin D Supplementation Group | Control Group | Outcomes (Relevant for This Meta-Analysis) | ||||
|---|---|---|---|---|---|---|---|---|---|
| No. | Age | Sex, Male | No. | Age | Sex, Male | ||||
| Annweiler, G. et al., 2020 [21] | Quasi-experimental with retrospective collection of data, France | Patients | 29 | 88 (87–93) | 9 (31.0) | 32 | 88 (84–92) | 19 (59.4) | Mortality |
| Hernandez, J.L. et. al., 2020 [22] | Case–Control, Spain | Patients | 19 | 60.0 (59.0–75.0) | 7 (36.8) | 197 | 61.0 (56.0–66.0) | 123 (62.4) | Mortality, ICU admission |
| Arroyo-Diaz, J.A. et al., 2021 [31] | Cross-Sectional, Spain | Patients | 189 | 73.3 ± 13.7 | 62 (32.8) | 1078 | 63.2 ± 16.3 | 634 (58.8) | Mortality, ICU admission |
| Cangiano, B. et al., 2021 [30] | Prospective Cohort, Italy | Patients | 20 | NA | NA | 78 | NA | NA | Mortality |
| Cereda, E. et al., 2021 [32] | Retrospective Cohort, Italy | Patients | 18 | 68.8 ± 10.6 | 16 (42.1) | 152 | 70.5 ± 13.1 | 141 (49.3) | Mortality |
| Ma, H. et al., 2021 [33] | Prospective Cohort, USA | Patients | 363 | 59.1 ± 8.1 | 141 (38.8) | 7934 | 57.4 ± 8.6 | 3964 (50.0) | SARS-CoV-2 Incidence |
| Oristrell, J. et al., 2021 [34] | Case–Control, Spain | Patients | 6252 | 70.2 ± 15.6 | 2656 (42.5) | 12,504 | 70.7 ± 14.7 | 5319 (42.5) | Mortality, COVID-19 incidence |
| Brunvoll, S.H. et al., 2022 [23] | RCT, Norway | Patients | 17,278 | 45.0 ± 13.5 | 6117 (35.4) | 17,323 | 44.9 ± 13.4 | 6137 (35.4) | SARS-CoV-2 Incidence |
| Gibbons, J.B. et al., 2022 [24] | Retrospective Cohort, USA | Patients | 33,216 | 58 | 29,130 (87.7) | 33,216 | 58 | 29,097 (87.6) | Mortality, COVID-19 Incidence |
| Retrospective Cohort, USA | Patients | 199,498 | 63 | 179,349 (89.9) | 199,498 | 64 | 179,748 (90.1) | Mortality, COVID-19 Incidence | |
| Jolliffe, D.A. et al., 2022 [25] | RCT, UK | Patients | 1346 | 60.7 (50.2–68.5) | 506 (37.6) | 1328 | 59.8 (50.3–67.4) | 498 (37.5) | Mortality, COVID-19 Incidence |
| Karonova, T.L. et al., 2022 [35] | RCT, Russia | Healthcare Workers | 38 | 34 ± 2 | 6 (15.8) | 40 | 36 ± 2 | 6 (15.0) | COVID-19 Incidence |
| Oristrell, J. et al., 2022 [26] | Retrospective Cohort, Spain | Patients | 108,343 | 70.0 ± 14.0 | 17,926 (16.5) | 216,686 | 70.0 ± 14.6 | 35,272 (16.3) | Mortality, COVID-19 Incidence |
| Retrospective Cohort, Spain | Patients | 134,703 | 68.8 ± 14.9 | 29,474 (21.9) | 269,406 | 68.8 ± 15.1 | 59,582 (22.1) | Mortality, COVID-19 Incidence | |
| Parant, F. et al., 2022 [27] | Retrospective Cohort, France | Patients | 66 | NA | 27 (40.9) | 162 | NA | 102 (63.0) | Mortality, ICU admission |
| Van Helmond, N. et al., 2022 [36] | RCT, USA | Healthcare Workers | 255 | 47 ± 12 | 55 (21.6) | 578 | 50 ± 13 | 131 (22.7) | COVID-19 Incidence |
| Villasis-Keever, M.A. et al., 2022 [28] | Double-Blind RCT, Mexico | Healthcare Workers | 94 | 36.0 (30–43) | NA | 98 | 39.0 (31–48) | NA | COVID-19 Incidence |
| Romero-Ibarguengoita, M.E. et al., 2023 [29] | Prospective Quasi-Experimental, Mexico | Healthcare Workers | 43 | NA | 17 (39.5) | 42 | NA | 23 (54.8) | COVID-19 Incidence |
| Prospective Quasi-Experimental, Mexico | Healthcare Workers | 28 | NA | 8 (28.6) | 85 | NA | 20 (23.5) | COVID-19 Incidence | |
| References | Treatment Arms | COVID-19 Incidence (n/N, %) | All-Cause Mortality (n/N, %) | ICU Admission (n/N, %) | |||
|---|---|---|---|---|---|---|---|
| Intervention | Control | Intervention | Control | Intervention | Control | ||
| Annweiler, G. et al., 2020 [21] | Intervention: 50,000 IU/month, 80,000 IU or 10,000 IU every 2–3 months (cholecalciferol); control: no vitamin D supplementation | NA | NA | 2/29 10.53 | 10/32 31.25 | NA | NA |
| Hernandez, J.L. et al., 2020 [22] | Intervention: (11 patients were taking cholecalciferol, 25,000 IU/monthly in 10 cases and 5600 IU/weekly in 1, and 8 patients were on calcifediol, 0.266 mg/monthly) | NA | NA | 2/19 10.53 | 20/197 5.08 | 1/19 5.26 | 50/197 25.38 |
| Arroyo-Diaz, J.A. et al., 2021 [31] | Intervention: regularly supplemented with vitamin D (not specified); control: no vitamin D supplementation | NA | NA | 50/189 26.46 | 167/1078 15.49 | 13/189 6.88 | 133/1078 12.34 |
| Cangiano, B. et al., 2021 [30] | Intervention: 25,000 IU of cholecalciferol 2 times a month; control: no vitamin D supplementation | NA | NA | 3/20 15 | 39/78 50 | NA | NA |
| Cereda, E. et al., 2021 [32] | Intervention: 54,000 IU/month of calciferol; control: no vitamin D supplementation | NA | NA | 7/18 38.89 | 40/152 26.32 | NA | NA |
| Ma, H. et al., 2021 [33] | Intervention: regularly supplemented with vitamin D (not specified); control: no vitamin D supplementation | 49/363 13.50 | 1329/7934 16.75 | NA | NA | NA | NA |
| Oristrell, J. et al., 2021 [34] | Intervention: regularly supplemented with vitamin D (mean daily calcitriol dose: ≤0.1 μg/d; >0.1–0.2 μg/d; >0.2–<0.4 μg/d; ≥0.4 μg/d); control: no vitamin D supplementation | 328/6252 5.25 | 703/12,504 5.62 | 76/6252 1.22 | 208/12,504 1.66 | NA | NA |
| Brunvoll, S.H. et al., 2022 [23] | Intervention: 5 mL/day of cod liver oil (equal to 10 μg/d or 400 IU/d of vitamin D3); control: placebo | 227/17,278 1.31 | 228/17,323 1.32 | NA | NA | NA | NA |
| Gibbons, J.B. et al., 2022 [24] | Intervention: regularly supplemented with vitamin D (vitamin D2 or ergocalciferol); control: no vitamin D supplementation | 716/33,216 2.16 | 987/33,216 2.98 | 65/33,216 0.19 | 86/33,216 0.26 | NA | NA |
| Intervention: regularly supplemented with vitamin D (vitamin D3 or cholecalciferol); control: no vitamin D supplementation | 5315/199,498 2.66 | 6591/199,498 3.30 | 462/199,498 0.23 | 689/199,498 0.35 | NA | NA | |
| Jolliffe, D.A. et al., 2022 [25] | Intervention: 3200 IU/day of vitamin D3; control: 800 IU/day | 45/1346 3.34 | 55/1328 4.14 | NA | NA | NA | NA |
| Karonova, T.L. et al., 2022 [35] | Intervention: 50,000 IU/week of cholecalciferol for 2 consecutive weeks, followed by 5000 IU/day for the rest of the study; control: 2000 IU/day | 10/38 26.31 | 18/40 45.00 | NA | NA | NA | NA |
| Oristrell, J. et al., 2022 [26] | Intervention: >250 μg of cholecalciferol per dose (equal to 10,000 IU); control: no vitamin D supplementation | 4352/108,343 4.02 | 9142/216,686 4.22 | 716/108,343 0.66 | 1492/216,686 0.69 | NA | NA |
| Intervention: >250 μg of calcifediol per dose (equal to 10,000 IU); control: no vitamin D supplementation | 5662/134,703 4.20 | 11,401/269,406 4.23 | 934/134,703 0.69 | 1859/269,406 0.69 | NA | NA | |
| Parant, F. et al., 2022 [27] | Intervention: <1000 IU/d or 80,000 IU or 100,000 IU every 2–3 months of cholecalciferol; control: no vitamin D supplementation | NA | NA | 7/66 10.61 | 28/162 17.28 | 10/66 15.15 | 74/162 45.68 |
| Van Helmond, N. et al., 2022 [36] | Intervention: 5000 IU/d of vitamin D3; control: placebo | 0/255 0.00 | 36/578 6.23 | NA | NA | NA | NA |
| Villasis-Keever, M.A. et al., 2022 [28] | Intervention: 4000 IU/d of cholecalciferol; control: placebo | 6/94 6.38 | 24/98 24.49 | NA | NA | NA | NA |
| Romero-Ibarguengoita, M.E. et al., 2023 [29] | Intervention: 52,000 IU/month of vitamin D3; control: no vitamin D supplementation | 5/43 11.63 | 13/42 30.95 | NA | NA | NA | NA |
| Intervention: 90,000 IU/month of vitamin D3; control: no vitamin D supplementation | 9/28 32.14 | 29/85 34.12 | NA | NA | NA | NA | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sartini, M.; Del Puente, F.; Oliva, M.; Carbone, A.; Bobbio, N.; Schinca, E.; Giribone, L.; Cristina, M.L. Preventive Vitamin D Supplementation and Risk for COVID-19 Infection: A Systematic Review and Meta-Analysis. Nutrients 2024, 16, 679. https://doi.org/10.3390/nu16050679
Sartini M, Del Puente F, Oliva M, Carbone A, Bobbio N, Schinca E, Giribone L, Cristina ML. Preventive Vitamin D Supplementation and Risk for COVID-19 Infection: A Systematic Review and Meta-Analysis. Nutrients. 2024; 16(5):679. https://doi.org/10.3390/nu16050679
Chicago/Turabian StyleSartini, Marina, Filippo Del Puente, Martino Oliva, Alessio Carbone, Nicoletta Bobbio, Elisa Schinca, Luana Giribone, and Maria Luisa Cristina. 2024. "Preventive Vitamin D Supplementation and Risk for COVID-19 Infection: A Systematic Review and Meta-Analysis" Nutrients 16, no. 5: 679. https://doi.org/10.3390/nu16050679
APA StyleSartini, M., Del Puente, F., Oliva, M., Carbone, A., Bobbio, N., Schinca, E., Giribone, L., & Cristina, M. L. (2024). Preventive Vitamin D Supplementation and Risk for COVID-19 Infection: A Systematic Review and Meta-Analysis. Nutrients, 16(5), 679. https://doi.org/10.3390/nu16050679