
Dietary Patterns, Dietary Adequacy and Nutrient Intake in Adults Commencing Peritoneal Dialysis: Outcomes from a Longitudinal Cohort Study
 ,
,
Abstract
1. Introduction
2. Materials and Methods
3. Results
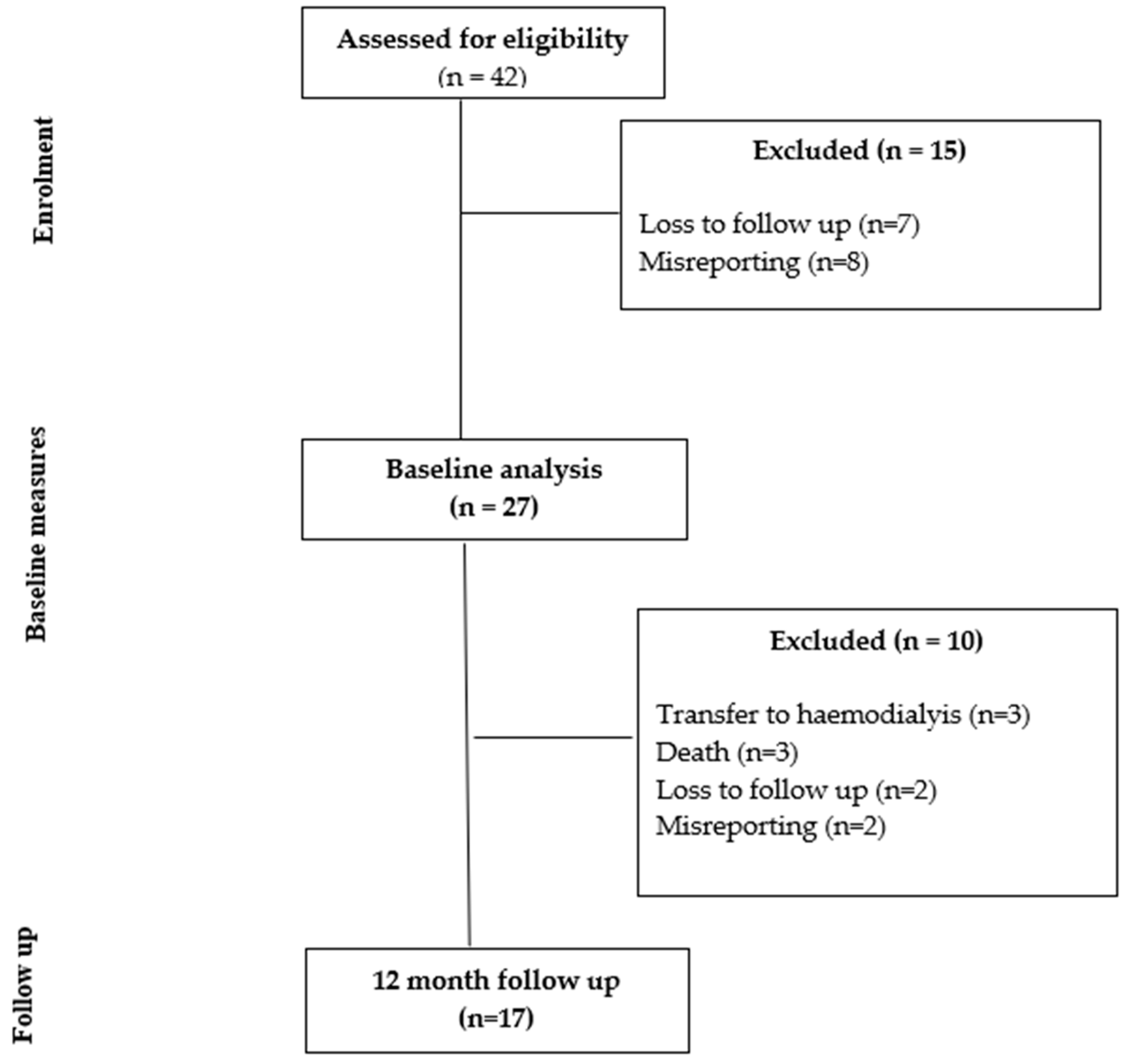
3.1. Characteristics of Participants
3.2. Nutrient Intake
3.3. Diet Quality
3.4. Dietary Patterns
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Australia & New Zealand Dialysis & Transplant Registry. ANZDATA 43rd Annual Report 2020 (Data to 2019); ANZDATA: Adelaide, Australia, 2020. [Google Scholar]
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J. KDOQI Clinical Practice guideline for nutrition in CKD: 2020 update. Am. J. Kidney Dis. 2020, 76, S1–S107. [Google Scholar] [CrossRef]
- Kiebalo, T.; Holotka, J.; Habura, I.; Pawlaczyk, K. Nutritional Status in Peritoneal Dialysis: Nutritional Guidelines, Adequacy and the Management of Malnutrition. Nutrients 2020, 12, 1715. [Google Scholar] [CrossRef]
- Wright, M.; Woodrow, G.; O’Brien, S.; King, N.; Dye, L.; Blundell, J.; Brownjohn, A.; Turney, J. Disturbed Appetite Patterns and Nutrient Intake in Peritoneal Dialysis Patients. Perit. Dial. Int. 2003, 23, 550–556. [Google Scholar] [CrossRef]
- Lambert, K.; Mullan, J.; Mansfield, K. An integrative review of the methodology and findings regarding dietary adherence in end stage kidney disease. BMC Nephrol. 2017, 18, 318. [Google Scholar] [CrossRef] [PubMed]
- Akbulut, G.; Sanlıer, N.; Inal, S.; Tek, N.A.; Oneç, K.; Erten, Y. Daily dietary energy and macronutrient intake and anthropometric measurements of the peritoneal dialysis patients. Ren. Fail. 2013, 35, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Fernström, A.; Hylander, B.; Rössner, S. Energy intake in patients on continuous ambulatory peritoneal dialysis and haemodialysis. J. Intern. Med. 1996, 240, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-M.; Kang, B.C.; Kim, H.-J.; Kyung, M.-S.; Oh, H.J.; Kim, J.-H.; Kwon, O.; Ryu, D.-R. Comparison of hemodialysis and peritoneal dialysis patients’ dietary behaviors. BMC Nephrol. 2020, 21, 91. [Google Scholar] [CrossRef] [PubMed]
- Therrien, M.; Byham-Gray, L.; Denmark, R.; Beto, J. Comparison of Dietary Intake Among Women on Maintenance Dialysis to a Women’s Health Initiative Cohort: Results from the NKF-CRN Second National Research Question Collaborative Study. J. Ren. Nutr. 2014, 24, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Chan, G.C.-K.; Ng, J.K.-C.; Cheng, P.M.-S.; Chow, K.-M.; Szeto, C.-C.; Li, P.K.-T. Dietary Micronutrient Intake and Its Relationship with the Malnutrition & Inflammation & Frailty Complex in Patients Undergoing Peritoneal Dialysis. Nutrients 2023, 15, 4934. [Google Scholar]
- Uribarri, J.; Leibowitz, J.; Dimaano, F. Caloric intake in a group of peritoneal dialysis patients. Am. J. Kidney Dis. 1998, 32, 1019–1022. [Google Scholar] [CrossRef]
- Dong, J.; Li, Y.; Xu, Y.; Xu, R. Daily protein intake and survival in patients on peritoneal dialysis. Nephrol. Dial. Transplant. 2011, 26, 3715–3721. [Google Scholar] [CrossRef] [PubMed]
- Azarnoush, H.; Mortazavi, M.; Rouhani, M.H.; Seirafian, S.; Atapour, A.; Hosseini, M.; Toghyani, A. Dietary nutrients’ intake and sleep quality in peritoneal dialysis patients. Sleep Sci. 2021, 14, 174–178. [Google Scholar] [CrossRef]
- Kim, H.; Lim, H.; Choue, R. A Better Diet Quality Is Attributable to Adequate Energy Intake in Hemodialysis Patients. Clin. Nutr. Res. 2015, 4, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.T.; Palmer, S.C.; Wai, S.N.; Ruospo, M.; Carrero, J.J.; Campbell, K.L.; Strippoli, G.F. Healthy Dietary Patterns and Risk of Mortality and ESRD in CKD: A Meta-Analysis of Cohort Studies. Clin. J. Am. Soc. Nephrol. 2017, 12, 272–279. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef] [PubMed]
- Australia & New Zealand Dialysis & Transplant Registry. Dialysis Hospital Report 2016–2021; NZDATA: Adelaide, Australia, 2022. [Google Scholar]
- Western Sydney Local Health District. A Better West: Western Sydney Local Health District Priorities 2017–2021; Western Sydney Local Health District: North Parramatta, Australia, 2023. [Google Scholar]
- Ash, S.; Campbell, K.; Maclaughlin, H.; McCoy, E.; Chan, M.; Anderson, K.; Corke, K.; Dumont, R.; Lloyd, L.; Meade, A.; et al. Evidence based practice guidelines for the nutritional management of chronic kidney disease. Nutr. Diet. 2006, 63, S33–S45. [Google Scholar] [CrossRef]
- National Health and Medical Research Council. Australian National Dietary Guidelines; The Council: Canberra, Australia, 2013. [Google Scholar]
- Cicely Saunders Institute. IPOS-Renal. Available online: https://pos-pal.org/maix/ipos-renal-in-english.php (accessed on 26 August 2021).
- Detsky, A.S.; McLaughlin, J.R.; Baker, J.P.; Johnston, N.; Whittaker, S.; Mendelson, R.A.; Jeejeebhoy, K.N. What is subjective global assessment of nutritional status? JPEN J. Parenter. Enter. Nutr. 1987, 11, 8–13. [Google Scholar] [CrossRef]
- Food Standards Australia New Zealand. AUSNUT 2011-13 Australian Food Composition Database; Food Standards Australia New Zealand: Canberra, Australia, 2014.
- National Health and Medical Research Council. Nutrient Reference Values for Australia and New Zealand; National Health and Medical Research Council: Canberra, Australia, 2020.
- Kim, H.J.; Oh, K. Methodological issues in estimating sodium intake in the Korea National Health and Nutrition Examination Survey. Epidemiol. Health 2014, 36, e2014033. [Google Scholar] [CrossRef]
- American Heart Association. AHA Sugar Recommendation. Available online: https://www.heart.org/en/healthy-living/healthy-eating/eat-smart/sugar/how-much-sugar-is-too-much#:~:text=AHA%20Sugar%20Recommendation&textMen%20should%20consume%20no%20more,or%20100%20calories)%20per%20day (accessed on 11 December 2023).
- Stanford, J.; Charlton, K.; Stefoska-Needham, A.; Zheng, H.; Bird, L.; Borst, A.; Fuller, A.; Lambert, K. Associations Among Plant-Based Diet Quality, Uremic Toxins, and Gut Microbiota Profile in Adults Undergoing Hemodialysis Therapy. J. Ren. Nutr. 2021, 31, 177–188. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. Australian Health Survey—Discretionary Food List; Australian Bureau of Statistics: Canberra, Australia, 2014.
- Rhee, J.J.; Sampson, L.; Cho, E.; Hughes, M.D.; Hu, F.B.; Willett, W.C. Comparison of methods to account for implausible reporting of energy intake in epidemiologic studies. Am. J. Epidemiol. 2015, 181, 225–233. [Google Scholar] [CrossRef]
- Hair, J.H.; Black, W.C.; Babin, B.J. Multivariate Data Analysis: Global Edition, 7th ed.; Pearson Education Limited: Harlow, UK, 2014. [Google Scholar]
- Kaiser, H.F. An index of factorial simplicity. Psychometrika 1974, 39, 31–36. [Google Scholar] [CrossRef]
- KDOQI. Clinical Practice Recommendations for Peritoneal Dialysis Adequacy. Am. J. Kidney Dis. 2006, 48, S130–S158. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, A.E.; Goodlad, C.; Clemenger, M.; Haddoub, S.S.; McGrory, J.; Pryde, K.; Tonkins, E.; Hisole, N.; Brown, E.A. Evaluation of physical symptoms in patients on peritoneal dialysis. Int. J. Nephrol. 2012, 2012, 305424. [Google Scholar] [CrossRef] [PubMed]
- Salamon, K.; Woods, J.; Paul, E.; Huggins, C. Peritoneal dialysis patients have higher prevalence of gastrointestinal symptoms than hemodialysis patients. J. Ren. Nutr. 2013, 23, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.; Zhou, Z.; Xu, H.; Wang, H.; Liu, B.; Cui, Y.; Yang, W.; Li, X.; Chen, L. Diminished Appetite Predicts Mortality of Chinese Peritoneal Dialysis Patients. Biol. Res. Nurs. 2013, 16, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Mehrotra, R.; Davison, S.N.; Farrington, K.; Flythe, J.E.; Foo, M.; Madero, M.; Morton, R.L.; Tsukamoto, Y.; Unruh, M.L.; Cheung, M.; et al. Managing the symptom burden associated with maintenance dialysis: Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2023, 104, 441–454. [Google Scholar] [CrossRef] [PubMed]
- Martín-del-Campo, F.; Batis-Ruvalcaba, C.; González-Espinoza, L.; Rojas-Campos, E.; Angel, J.R.; Ruiz, N.; González, J.; Pazarín, L.; Cueto-Manzano, A.M. Dietary micronutrient intake in peritoneal dialysis patients: Relationship with nutrition and inflammation status. Perit. Dial. Int. 2012, 32, 183–191. [Google Scholar] [CrossRef]
- Crabtree, J.H.; Shrestha, B.M.; Chow, K.M.; Figueiredo, A.E.; Povlsen, J.V.; Wilkie, M.; Abdel-Aal, A.; Cullis, B.; Goh, B.L.; Briggs, V.R.; et al. Creating and Maintaining Optimal Peritoneal Dialysis Access in the Adult Patient: 2019 Update. Perit. Dial. Int. 2019, 39, 414–436. [Google Scholar] [CrossRef]
- Kosmadakis, G.; Albaret, J.; Da Costa Correia, E.; Somda, F.; Aguilera, D. Constipation in Peritoneal Dialysis Patients. Perit. Dial. Int. 2019, 39, 399–404. [Google Scholar] [CrossRef]
- Pereira, N.B.F.; Ramos, C.I.; de Andrade, L.S.; Teixeira, R.R.; Nakao, L.S.; Rodrigues, S.D.; de Lima, J.D.; Dalboni, M.A.; Cuppari, L. Influence of bowel habits on gut-derived toxins in peritoneal dialysis patients. J. Nephrol. 2020, 33, 1049–1057. [Google Scholar] [CrossRef]
- Wang, H.; Wang, X.; Dou, H.; Li, C.; Cui, M.; Gu, C.; Yang, L. Risk factors for peritoneal dialysis–associated peritonitis. Eur. J. Inflamm. 2018, 16, 2058739218772243. [Google Scholar] [CrossRef]
- Tharapanich, H.; Halue, G.; Kanjanabuch, T.; Phannajit, J.; Lorvinitnun, P.; Chieochanthanakij, R.; Treamtrakanpon, W.; Parinyasiri, U.; Lowmseng, N.; Songviriyavithaya, P.; et al. WCN23-1055 constipation and clinical outcomes in peritoneal dialysis thailand results from pdopps. Kidney Int. Rep. 2023, 8, S360–S361. [Google Scholar] [CrossRef]
- Moore, I.; Byrne, P.; Ilic, N.; Chen, J.H.-C.; Lambert, K. The Prevalence and Lived Experience of Pain in People Undertaking Dialysis. Kidney Dial. 2023, 3, 24–35. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. National Health Survey; Australian Bureau of Statistics: Canberra, Australia, 2023.
- Chen, X.; Wei, G.; Jalili, T.; Metos, J.; Giri, A.; Cho, M.E.; Boucher, R.; Greene, T.; Beddhu, S. The Associations of Plant Protein Intake with All-Cause Mortality in CKD. Am. J. Kidney Dis. 2016, 67, 423–430. [Google Scholar] [CrossRef]
- Stanford, J.; Zuck, M.; Stefoska-Needham, A.; Charlton, K.; Lambert, K. Acceptability of Plant-Based Diets for People with Chronic Kidney Disease: Perspectives of Renal Dietitians. Nutrients 2022, 14, 216. [Google Scholar] [CrossRef]
- Yasuda, G.; Shibata, K.; Takizawa, T.; Ikeda, Y.; Tokita, Y.; Umemura, S.; Tochikubo, O. Prevalence of constipation in continuous ambulatory peritoneal dialysis patients and comparison with hemodialysis patients. Am. J. Kidney Dis. 2002, 39, 1292–1299. [Google Scholar] [CrossRef]
- Kosmadakis, G.; Albaret, J.; da Costa Correia, E.; Somda, F.; Aguilera, D. Gastrointestinal Disorders in Peritoneal Dialysis Patients. Am. J. Nephrol. 2018, 48, 319–325. [Google Scholar] [CrossRef]
- National Health and Medical Research Council. Australian Guide to Healthy Eating. Available online: https://www.nhmrc.gov.au/adg (accessed on 10 January 2024).

{kind=link}
| Participants Characteristics | Baseline (n = 27) | Follow Up (n = 17) | p-Value |
|---|---|---|---|
| Demographics | |||
| Age, mean (SD) | 63.04 (13.37) | 66.24 (12.59) | 0.43 |
| Female, n (%) | 8 (30%) | 2 (12%) | 0.17 |
| Ethnicity, n (%) | 0.90 | ||
| Asian | 10 (37%) | 7 (41%) | |
| Indigenous Australian | 0 | 0 | |
| Caucasian | 8 (30%) | 2 (11%) | |
| Pacific Islander | 4 (15%) | 4 (24%) | |
| Middle Eastern | 5 (18%) | 4 (24%) | |
| Anthropometry | |||
| Weight (kg), mean (SD) | 77.91 (16.53) | 78.91 (15.71) | 0.84 |
| BMI (kg/m2), mean (SD) | 27.14 (3.74) | 27.76 (4.7) | 0.26 |
| BMI Class (kg/m2), n (%) | 0.05 | ||
| Underweight (<18.5) | 0 | 0 | |
| Normal (18.5–24.9) | 8 (30%) | 5 (30%) | |
| Overweight (25–29.9) | 11 (40%) | 6 (35%) | |
| Obese (>30) | 8 (30%) | 6 (35%) | |
| Diabetes, n (%) | 11 (41%) | 8 (47%) | 0.68 |
| PD type, n (%) | 0.89 | ||
| CAPD/APD | 18 (66%) | 11 (65%) | |
| IPD | 9 (33%) | 6 (35%) | |
| Food intake confirmed with photos | 23 (85%) | 15 (88) | 0.77 |
| Nutritional Status | 0.16 | ||
| Well nourished (SGA = A) | 13 (77) | 15 (88) | |
| Mild or moderately malnourished (SGA = B) | 4 (24) | 1 (6) | |
| Malnourished (SGA = C) | 0 (0) | 1 (6) | |
| nPCR | - | 0.79 (IQR: 0.67–1.04) | - |
| Membrane transporter status | |||
| High | - | 5 (29) | - |
| High average | - | 4 (24) | |
| Low average | - | 7 (41) | |
| Low | - | 1 (6) | |
| Dialysis Adequacy Kt/V | - | 1.79 (IQR:1.54–2.02) | - |
| Biochemistry at follow up | - | - | - |
| Sodium (mmol/L) | - | 134 (3.5) | - |
| Potassium (mmol/L) | - | 4.3 (0.8) | - |
| Bicarbonate (mmol/L) | - | 26 (3.3) | - |
| Urea (mmol/L) | - | 22 (6.2) | - |
| Creatinine (umol/L) | - | 744 (197) | - |
| Calcium (corrected) (mmol/L) | - | 2.5 (0.2) | - |
| Phosphate (mmol/L) | - | 1.67 (0.47) | - |
| Magnesium (mmol/L) | - | 0.88 (0.15) | - |
| Albumin (g/L) | - | 29.4 (3.0) | - |
| Hemoglobin (g/L) | - | 107 (14) | - |
| IPOS score, median (IQR) | |||
| Pain | 1.00 (0.00–2.00) | - | |
| Shortness of breath | 0.50 (0.00–1.00) | - | |
| Weakness or lack of energy | 1.50 (0.00–2.25) | - | |
| Nausea | 0.00 (0.00–1.00) | - | |
| Vomiting | 0.00 (0.00–0.00) | - | |
| Poor appetite | 0.50 (0.00–2.00) | - | |
| Constipation | 1.00 (0.75–2.00) | - | |
| Sore or dry mouth | 1.00 (0.00–2.00) | - | |
| Drowsiness | 1.00 (0.00–2.00) | - | |
| Poor mobility | 1.00 (0.00–2.00) | - | |
| Itching | 1.00 (0.00–2.00) | - | |
| Difficulty sleeping | 1.00 (0.00–2.00) | - | |
| Restless legs | 0.00 (0.00–1.00) | - | |
| Changes in skin | 0.50 (0.00–2.00) | - | |
| Diarrhea | 0.00 (0.00–0.00) | - | |
| Total Score | 12 (6–19) | - |
| Baseline (n = 17) Mean (SD) | Follow Up (n = 17) Mean (SD) | p Value a | Mean Difference (SD) | p Value b | |
|---|---|---|---|---|---|
| Demographic characteristics | |||||
| Weight (kg) | 77.00 (13.29) | 78.91 (15.71) | 0.23 | 1.91 (6.27) | - |
| BMI (kg/m2) | 27.14 (3.74) | 27.76 (4.70) | 0.26 | 0.62 (0.53) | - |
| Macronutrients | |||||
| Energy (kJ) median (IQR) | 8459 (6763–9366) | 6665 (6253–10,012) | 0.57 | –767 (5160) | - |
| Energy (kcal/kg/day) (median (IQR) | 26.9 (20.6–30.1) | 22.7 (17.3–30.6) | 0.73 | –1.8 (12.1) | 0.80 |
| Protein (g) | 97 (32) | 77 (24) | 0.07 | –20 (43) | - |
| Protein (g/kg) | 1.29 (0.46) | 1.00 (0.37) | 0.05 | –0.29 (0.57) | 0.25 |
| Fat (g) | 77 (28) | 64 (26) | 0.20 | −12 (38) | - |
| Sat fat (g) | 28 (11) | 20 (8) | 0.02 | −7 (11) | -- |
| CHO (g) | 204 (79) | 186 (72) | 0.44 | −18 (84) | - |
| Micronutrients | |||||
| Phosphorus (mg) | 1329 (345) | 1006 (344) | 0.01 | −323 (448) | 0.03 |
| Potassium (mg) | 2955 (933) | 2589 (1013) | 0.33 | −366 (1509) | 0.81 |
| Calcium (mg) | 671 (320) | 495 (247) | 0.03 | −176 (304) | 0.01 |
| Zinc (mg) | 9.87 (4.07) | 8.94 (3.69) | 0.41 | −1 (5) | 0.02 |
| Vitamin B6 (mg) | 1.65 (0.87) | 2.07 (1.45) | 0.34 | 0 (2) | 0.11 |
| Vitamin C (mg) | 97 (77) | 130 (118) | 0.41 | 33 (156) | 0.002 |
| Fiber (g) | 23.8 (10.8) | 24.1 (10.1) | 0.93 | 0.29 (13.5) | 0.01 |
| % kJ from fiber | 2.35 (0.76) | 2.68 (0.83) | 0.17 | 0.33 (0.94) | - |
| % kJ from CHO | 41.30 (9.21) | 42.44 (8.62) | 0.66 | 1.14 (10.60) | - |
| Core food groups | |||||
| Grain serves | 7.3 (4.0) | 5.6 (3.1) | 0.07 | −1.7 (3.7) | 0.08 |
| Fruit serves | 1.4 (1.3) | 2.1 (1.6) | 0.15 | 0.7 (1.9) | 0.17 |
| Vegetable serves | 3.8 (2.3) | 4.0 (2.8) | 0.83 | 0.2 (3.4) | 0.32 |
| Dairy serves | 1.1 (1.0) | 0.6 (0.7) | 0.08 | −0.4 (1.0) | 0.03 |
| Meat/ alternative serves | 3.0 (1.3) | 2.3 (1.1) | 0.11 | −0.7 (1.6) | 0.28 |
| Alcohol standard serves | 0.3 (0.6) | 0.41 (1.0) | 0.21 | 0.2 (0.5) | 1.00 |
| Added sugar (g) | 24 (23) | 14 (14) | 0.11 | −10 (25) | <0.001 |
| Diet Quality Indices (Range of possible scores: PDI: 46–230; Healthy PDI; 53–265; Unhealthy PDI:51–255) | |||||
| Plant-Based Diet Index (PDI) | 137.9 (9.7) | 137.9 (8.5) | 1.00 | 0.2 (12.4) | - |
| Healthy PDI | 160.4 (14.3) | 158.9 (13.0) | 0.60 | −1.4 (11) | - |
| Unhealthy PDI | 154.8 (16.2) | 153.7 (19.2) | 0.67 | −1.1 (10.2) | - |
| Nutrient/Food Target | Proportion Meeting Targets at Baseline n (%) | Proportion Meeting Targets at 12 Months n (%) | p Value |
|---|---|---|---|
| Adequate Energy (25–35 kcal/kg/day) | 10 (59) | 8 (47) | 0.49 |
| Protein (1–1.2 g/kg) | 7 (41%) | 5 (30%) | 0.25 |
| Phosphorus (≤1000 mg/day) | 2 (12%) | 8 (47%) | 0.03 |
| Calcium (800–1000 mg/day) | 5 (29%) | 0 (0%) | 0.01 |
| Adequate zinc (≥12 mg/day) | 4 (24%) | 3 (18%) | 0.02 |
| Adequate Vitamin B6 (≥1.4 mg/day) | 13 (76%) | 11 (65%) | 0.11 |
| Adequate Vitamin C (≥30 mg/day) | 16 (94%) | 14 (82%) | 0.002 |
| Adequate fiber (≥30 g/day) | 3 (18%) | 7 (41%) | 0.005 |
| Adequate grains (4 servings/day) | 15 (88%) | 10 (59%) | 0.08 |
| Adequate fruit (2 servings/day) | 4 (24%) | 8 (47%) | 0.17 |
| Adequate vegetables (5 servings/day) | 6 (35%) | 7 (41%) | 0.32 |
| Adequate dairy (≤1 servings/day) | 11 (41%) | 9 (53%) | 0.63 |
| Meat and alternative (2–3 servings/day) | 8 (47%) | 4 (24%) | 0.28 |
| Alcohol (≤4 standard drinks/day) | 17 (100%) | 17 (100%) | 1.00 |
| Added sugar (<10% total energy or <36 g/day) | 13 (76%) | 16 (94%) | 0.001 |
| Food Component | Pattern 1 Breads and Cereals | Pattern 2 Milk and Potatoes | Pattern 3 Semi Vegetarian |
|---|---|---|---|
| Refined grains | 0.977 | ||
| Wholegrains | 0.976 | ||
| Milk | 0.705 | ||
| Potato products | 0.676 | ||
| Red/orange vegetables | 0.761 | ||
| Fruit | −0.495 | ||
| Legumes | 0.372 | ||
| Seafood | |||
| Nuts and seeds | |||
| Yoghurt | |||
| Dark green vegetables | |||
| Cheese | |||
| Poultry | |||
| Eggs | |||
| Alcoholic drinks | |||
| Amount (%) of variance explained | 13.433 | 7.135 | 6.925 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lambert, K.; Ryan, M.; Flanagan, J.; Broinowski, G.; Nicdao, M.; Stanford, J.; Chau, K. Dietary Patterns, Dietary Adequacy and Nutrient Intake in Adults Commencing Peritoneal Dialysis: Outcomes from a Longitudinal Cohort Study. Nutrients 2024, 16, 663. https://doi.org/10.3390/nu16050663
Lambert K, Ryan M, Flanagan J, Broinowski G, Nicdao M, Stanford J, Chau K. Dietary Patterns, Dietary Adequacy and Nutrient Intake in Adults Commencing Peritoneal Dialysis: Outcomes from a Longitudinal Cohort Study. Nutrients. 2024; 16(5):663. https://doi.org/10.3390/nu16050663
Chicago/Turabian StyleLambert, Kelly, Michele Ryan, Jade Flanagan, Georgie Broinowski, Maryann Nicdao, Jordan Stanford, and Katrina Chau. 2024. "Dietary Patterns, Dietary Adequacy and Nutrient Intake in Adults Commencing Peritoneal Dialysis: Outcomes from a Longitudinal Cohort Study" Nutrients 16, no. 5: 663. https://doi.org/10.3390/nu16050663
APA StyleLambert, K., Ryan, M., Flanagan, J., Broinowski, G., Nicdao, M., Stanford, J., & Chau, K. (2024). Dietary Patterns, Dietary Adequacy and Nutrient Intake in Adults Commencing Peritoneal Dialysis: Outcomes from a Longitudinal Cohort Study. Nutrients, 16(5), 663. https://doi.org/10.3390/nu16050663