

Obesity and Nutrigenetics Testing: New Insights

 and
and
Abstract
1. Introduction
2. Obesity: Epidemiology, Diagnosis, and Treatment
3. Precision Nutrition and Exposome
4. Nutritional Genomics
5. Genetic Aspects of Obesity
6. Genetic Testing (GT)
6.1. Direct-to-Consumer Genetic Testings (DTC-GT)
6.2. Nutrigenetic Tests
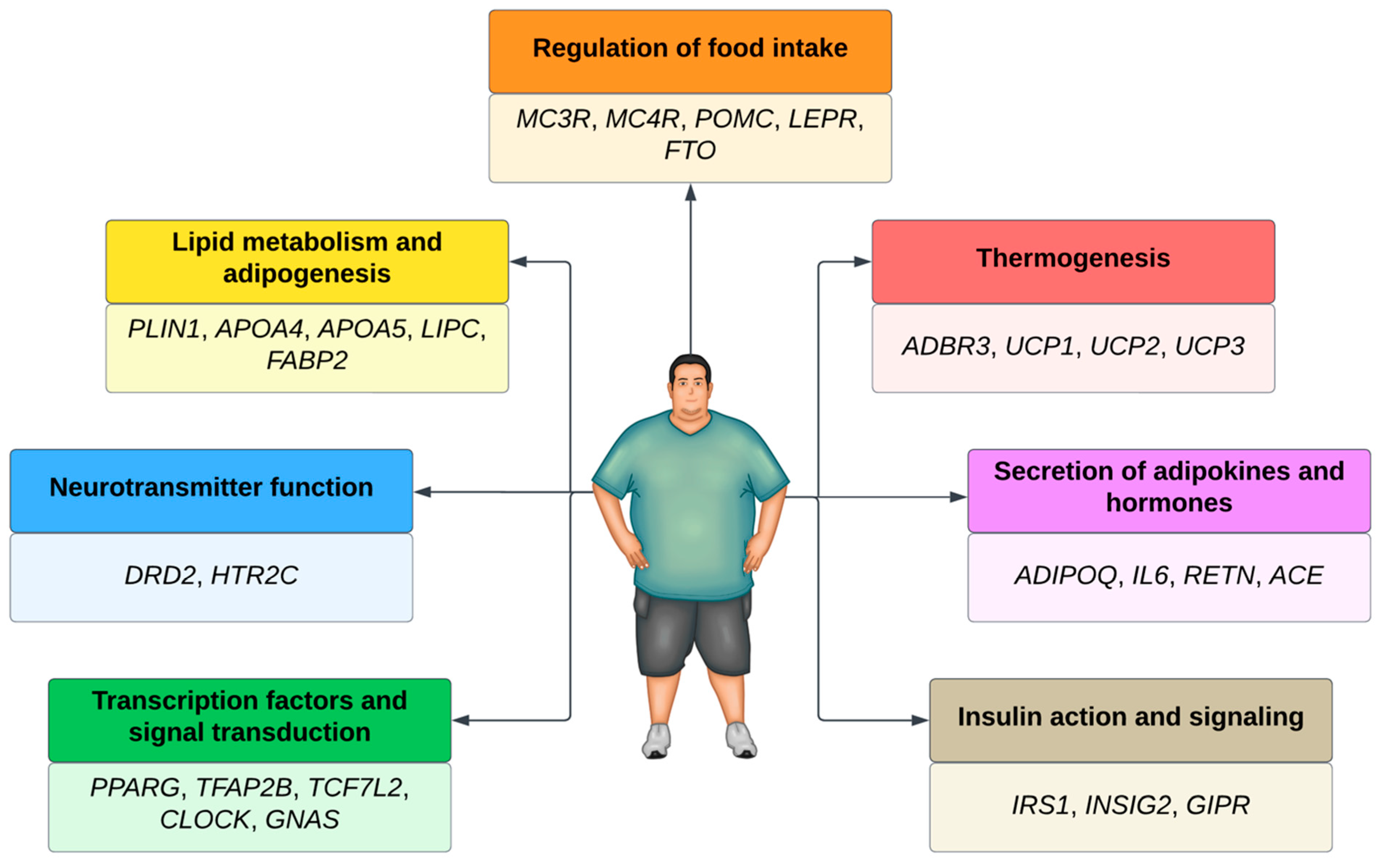
6.3. Targets of Nutrigenetic Tests
6.4. Evidence from Nutrigenetics Testing in Obesity
6.5. Overview of Ethical Issues and Positions on Nutrigenetics Tests
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- International Classification of Diseases for Mortality and Morbidity Statistics (11th Revision); World Health Organization: Geneva, Switzerland, 2024. Available online: https://icd.who.int/browse11/l-m/en (accessed on 24 January 2024).
- World Obesity Federation. World Obesity Atlas 2022; World Obesity Federation: London, UK, 2022; Available online: https://s3-eu-west-1.amazonaws.com/wof-files/World_Obesity_Atlas_2022.pdf (accessed on 23 October 2023).
- Chong, B.; Jayabaskaran, J.; Kong, G.; Chan, Y.H.; Chin, Y.H.; Goh, R.; Kannan, S.; Ng, C.H.; Loong, S.; Kueh, M.T.W.; et al. Trends and Predictions of Malnutrition and Obesity in 204 Countries and Territories: An Analysis of the Global Burden of Disease Study 2019. EClinicalMedicine 2023, 57, 101850. [Google Scholar] [CrossRef]
- Loos, R.; Yeo, G. The Genetics of Obesity: From Discovery to Biology. Nat. Rev. Genet. 2022, 23, 120–133. [Google Scholar] [CrossRef]
- World Health Organization. WHO Acceleration Plan to Stop Obesity. Available online: https://iris.who.int/bitstream/handle/10665/370281/9789240075634-eng.pdf?sequence=1 (accessed on 23 October 2023).
- Vazquez-Vidal, I.; Desmarchelier, C.; Jones, P. Nutrigenetics of Blood Cholesterol Concentrations: Towards Personalized Nutrition. Curr. Cardiol. Rep. 2019, 21, 38. [Google Scholar] [CrossRef] [PubMed]
- Joffe, Y.; Houghton, C. A Novel Approach to the Nutrigenetics and Nutrigenomics of Obesity and Weight Management. Cur Oncol. Rep. 2016, 18, 43. [Google Scholar] [CrossRef]
- Corrêa, T.; Quintanilha, B.; Norde, M.; Pinhel, M.; Nonino, C.; Rogero, M. Nutritional Genomics, Inflammation and Obesity. Arch. Endocrinol. Metab. 2020, 64, 205–222. [Google Scholar] [CrossRef] [PubMed]
- De Toro-Martín, J.; Arsenault, B.; Després, J.; Vohl, M. Precision Nutrition: A Review of Personalized Nutritional Approaches for the Prevention and Management of Metabolic Syndrome. Nutrients 2017, 9, 913. [Google Scholar] [CrossRef]
- Marcotte, B.; Cormier, H.; Garneau, V.; Robitaille, J.; Desroches, S.; Vohl, M. Nutrigenetic Testing for Personalized Nutrition: An Evaluation of Public Perceptions, Attitudes, and Concerns in a Population of French Canadians. Lifestyle Genom. 2019, 11, 155–162. [Google Scholar]
- Xiang, L.; Wu, H.; Pan, A.; Patel, B.; Xiang, G.; Qi, L.; Kaplan, R.; Hu, F.; Wylie-Rosett, J.; Qi, Q. FTO Genotype and Weight Loss in Diet and Lifestyle Interventions: A Systematic Review and Meta-Analysis. Am. J. Clin. Nutr. 2016, 103, 1162–1170. [Google Scholar] [CrossRef]
- Keathley, J.; Garneau, V.; Marcil, V.; Mutch, D.; Robitaille, J.; Rudkowska, I.; Sofian, G.; Desroches, S.; Vohl, M. Nutrigenetics, Omega-3 and Plasma Lipids/Lipoproteins/Apolipoproteins with Evidence Evaluation Using the GRADE Approach: A Systematic Review. BMJ Open 2022, 12, e054417. [Google Scholar] [CrossRef]
- Pérez-Beltrán, Y.; Rivera-Iñiguez, I.; Gonzalez-Becerra, K.; Pérez-Naitoh, N.; Tovar, J.; Sáyago-Ayerdi, S.; Mendivil, E. Personalized Dietary Recommendations Based on Lipid-Related Genetic Variants: A Systematic Review. Front. Nutr. 2022, 9, 830283. [Google Scholar] [CrossRef]
- Horne, J.; Gilliland, J.; Madill, J.; Shelley, J. A Critical Examination of Legal and Ethical Considerations for Nutrigenetic Testing with Recommendations for Improving Regulation in Canada: From Science to Consumer. J. Law. Biosci. 2020, 7, lsaa003. [Google Scholar] [CrossRef]
- World Health Organization. WHO European Regional Obesity Report 2022; World Health Organization, Regional Office for Europe: Copenhagen, Denmark, 2022.
- Wharton, S.; Lau, D.; Vallis, M.; Sharma, A.; Biertho, L.; Campbell-Scherer, D.; Adamo, K.; Alberga, A.; Bell, R.; Boulé, N.; et al. Obesity in Adults: A Clinical Practice Guideline. Can. Med. Assoc. J. 2020, 192, E875–E891. [Google Scholar] [CrossRef]
- Whitlock, G.; Lewington, S.; Sherliker, P.; Clarke, R.; Emberson, J.; Halsey, J.; Qizilbash, N.; Collins, R.; Peto, R.; Prospective Studies Collaboration. Body-Mass Index and Cause-Specific Mortality in 900 000 Adults: Collaborative Analyses of 57 Prospective Studies. Lancet 2009, 373, 1083–1096. [Google Scholar]
- Wolin, K.; Carson, K.; Colditz, G. Obesity and Cancer. Oncologist 2010, 15, 556–565. [Google Scholar] [CrossRef]
- GBD 2015 Obesity Collaborators; Afshin, A.; Forouzanfar, M.; Reitsma, M.; Sur, P.; Estep, K.; Lee, A.; Marczak, L.; Mokdad, A.H.; Moradi-Lakeh, M.; et al. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar]
- Lauby-Secretan, B.; Scoccianti, C.; Loomis, D.; Grosse, Y.; Bianchini, F.; Straif, K. Body Fatness and Cancer: Viewpoint of the IARC Working Group. N. Engl. J. Med. 2016, 375, 794–798. [Google Scholar] [CrossRef]
- Brock, J.; Billeter, A.; Müller-Stich, B.; Herth, F. Obesity and the Lung: What We Know Today. Respiration 2020, 99, 856–866. [Google Scholar] [CrossRef] [PubMed]
- Commodore-Mensah, Y.; Selvin, E.; Aboagye, J.; Turkson-Ocran, R.A.; Li, X.; Himmelfarb, C.D.; Ahima, R.S.; Cooper, L.A. Hypertension, Overweight/Obesity, and Diabetes among Immigrants in the United States: An Analysis of the 2010–2016 National Health Interview Survey. BMC Public Health 2018, 18, 773. [Google Scholar] [CrossRef] [PubMed]
- Brownell, K.; Kersh, R.; Ludwig, D.; Post, R.C.; Puhl, R.M.; Schwartz, M.B.; Willett, W.C. Personal Responsibility and Obesity: A Constructive Approach to a Controversial Issue. Health Aff. 2010, 29, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Tekes, B.; Üzümcüoglu, Y.; Hoe, C.; Özkan, T. The Relationship Between Hofstede’s Cultural Dimensions, Schwartz’s Cultural Values, and Obesity. Psychol. Rep. 2018, 122, 968–987. [Google Scholar] [CrossRef] [PubMed]
- Pagliai, G.; Dinu, M.; Madarena, M.; Bonaccio, M.; Iacoviello, L.; Sofi, F. Consumption of Ultra-Processed Foods and Health Status: A Systematic Review and Meta-Analysis. Br. J. Nutr. 2021, 125, 308–318. [Google Scholar] [CrossRef]
- Harb, A.; Shechter, A.; Koch, P.; St-Onge, M.-P. Ultra-Processed Foods and the Development of Obesity in Adults. Eur. J. Clin. Nutr. 2023, 77, 619–627. [Google Scholar] [CrossRef]
- Ministério Da Saúde; Secretaria de Vigilância em Saúde e Ambiente; Departamento de Análise Epidemiológica e Vigilância de Doenças Não Transmissíveis. Vigitel Brasil 2023: Vigilância de Fatores de Risco e Proteção Para Doenças Crônicas Por Inquérito Telefônico; Ministério da Saúde: Brasilia, Brazil, 2023; p. 131.
- Malik, V.; Popkin, B.; Bray, G.; Després, J.; Hu, F. Sugar-Sweetened Beverages, Obesity, Type 2 Diabetes Mellitus, and Cardiovascular Disease Risk. Circulation 2010, 121, 1356–1364. [Google Scholar] [CrossRef]
- Schulze, M.; Manson, J.E.; Ludwig, D.S.; Colditz, G.A.; Stampfer, M.J.; Willett, W.C.; Hu, F.B. Sugar-Sweetened Beverages, Weight Gain, and Incidence of Type 2 Diabetes in Young and Middle-Aged Women. JAMA 2004, 292, 927–934. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Hao, T.; Rimm, E.; Willett, W.; Hu, F. Changes in Diet and Lifestyle and Long-Term Weight Gain in Women and Men. N. Engl. J. Med. 2011, 364, 2392–2404. [Google Scholar] [CrossRef]
- Malik, V.; Hu, F. Sugar-Sweetened Beverages and Health: Where Does the Evidence Stand? Am. J. Clin. Nutr. 2011, 94, 1161–1162. [Google Scholar] [CrossRef]
- Pepe, R.; Lottenberg, A.; Fujiwara, C.; Beyruti, M.; Cintra, D.E.C.; Machado, R.M.; Rodrigues, A.; Jensen, N.S.O.; Caldas, A.; Fernandes, A.E.; et al. Posicionamento Sobre o Tratamento Nutricional do Sobrepeso e da Obesidade. ABESO 2022, 1, 260. [Google Scholar]
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. 2013 AHA/ACC/ TOS Guideline for the Management of Overweight and Obesity in Adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. J. Am. Coll. Cardiol. 2014, 63, 2985–3023. [Google Scholar] [CrossRef] [PubMed]
- Blüher, M. Obesity: Global Epidemiology and Pathogenesis. Nat. Rev. Endocrinol. 2019, 15, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Horne, J.; Gilliland, J.; O’Connor, C.; Seabrook, J.; Janet, M. Change in Weight, BMI, and Body Composition in a Population-Based Intervention Versus Genetic-Based Intervention: The NOW Trial. Obesity 2020, 28, 1419–1427. [Google Scholar] [CrossRef] [PubMed]
- Müller, T.; Clemmensen, C.; Finan, B.; DiMarchi, R.; Tschöp, M. Anti-Obesity Therapy: From Rainbow Pills to Polyagonists. Pharmacol. Rev. 2018, 70, 712–746. [Google Scholar] [CrossRef] [PubMed]
- Angelidi, A.; Belanger, M.; Kokkinos, A.; Koliaki, C.; Mantzoros, C. Novel Noninvasive Approaches to the Treatment of Obesity: From Pharmacotherapy to Gene Therapy. Endocr. Rev. 2022, 43, 507–557. [Google Scholar] [CrossRef] [PubMed]
- Sharretts, J.; Galescu, O.; Gomatam, S.; Andraca-Carrera, E.; Hampp, C.; Yanoff, L. Cancer Risk Associated with Lorcaserin: The FDA’s Review of the CAMELLIA-TIMI 61 Trial. N. Engl. J. Med. 2020, 383, 1000–1002. [Google Scholar] [CrossRef] [PubMed]
- Associação Brasileira para o Estudo da Obesidade e da Síndrome Metabólica. Diretrizes Brasileiras de Obesidade 2016, 4th ed.; ABESO: São Paulo, SP, Brazil, 2016; 188p. [Google Scholar]
- Cornier, M. A Review of Current Guidelines for the Treatment of Obesity. Am. J. Manag. Care. 2022, 28 (Suppl. S15), S288–S296. [Google Scholar] [PubMed]
- Telese, A.; Sehgal, V.; Magee, C.; Naik, S.; Alqahtani, S.; Lovat, L.; Haidry, R.J. Bariatric and Metabolic Endoscopy: A New Paradigm. Clin. Transl. Gastroenterol. 2021, 12, e00364. [Google Scholar] [CrossRef]
- Rubino, F.; Nathan, D.; Eckel, R.; Schauer, P.R.; Alberti, K.G.M.M.; Zimmet, P.Z.; Del Prato, S.; Ji, L.; Sadikot, S.M.; Herman, W.H.; et al. Delegates of the 2nd Diabetes Surgery Summit. Metabolic Surgery in the Treatment Algorithm for Type 2 Diabetes: A Joint Statement by International Diabetes Organizations. Obes. Surg. 2017, 27, 2–21. [Google Scholar] [CrossRef]
- Hinney, A.; Körner, A.; Fischer-Posovszky, P. The Promise of New Anti-Obesity Therapies Arising from Knowledge of Genetic Obesity Traits. Nat. Rev. Endocrinol. 2022, 18, 623–637. [Google Scholar] [CrossRef]
- Antwi, J. Precision Nutrition to Improve Risk Factors of Obesity and Type 2 Diabetes. Curr. Nutr. Rep. 2023, 12, 679–694. [Google Scholar] [CrossRef]
- Ramaswami, R.; Bayer, R.; Galea, S. Precision Medicine from a Public Health Perspective. Annu. Rev. Public Health 2018, 39, 153–168. [Google Scholar] [CrossRef]
- Collins, F.; Varmus, H. A New Initiative on Precision Medicine. N. Engl. J. Med. 2015, 372, 793–795. [Google Scholar] [CrossRef]
- Corella, D.; Coltell, O.; Portolés, O.; Sotos-Prieto, M.; Fernández-Carrión, R.; Ramirez-Sabio, J.; Zanón-Moreno, V.; Mattei, J.; Sorlí, J.; Ordovas, J. A Guide to Applying the Sex-Gender Perspective to Nutritional Genomics. Nutrients 2018, 11, 4. [Google Scholar] [CrossRef]
- Wild, C. Complementing the Genome with an “Exposome”: The Outstanding Challenge of Environmental Exposure Measurement in Molecular Epidemiology. Cancer Epidemiol. Biomark. Prev. 2005, 14, 1847–1850. [Google Scholar] [CrossRef]
- Miller, G.; Jones, D. The Nature of Nurture: Refining the Definition of the Exposome. Toxicol. Sci. 2014, 137, 1–2. [Google Scholar] [CrossRef]
- Ramos-Lopez, O.; Martinez, J.; Milagro, F. Holistic Integration of Omics Tools for Precision Nutrition in Health and Disease. Nutrients 2022, 14, 4074. [Google Scholar] [CrossRef]
- Fournier, T.; Poulain, J.; Jacob, M. Genômica Nutricional: (Re)Considerando as Relações Alimentação-Saúde via Religação das Ciências Sociais, Biomédicas e da Vida. Rev. Inter-Legere 2019, 2, c18336. [Google Scholar]
- Camp, K.; Trujillo, E. Position of the Academy of Nutrition and Dietetics: Nutritional Genomics. J. Acad. Nutr. Diet. 2014, 114, 299–312. [Google Scholar] [CrossRef] [PubMed]
- Dhanapal, A.; Wuni, R.; Ventura, E.; Chiet, T.; Cheah, E.; Loganathan, A.; Quen, P.; Appukutty, M.; Noh, M.; Givens, I.; et al. Implementation of Nutrigenetics and Nutrigenomics Research and Training Activities for Developing Precision Nutrition Strategies in Malaysia. Nutrients 2022, 14, 5108. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, P.; Newsome, J.; Santos, H.; Schiller, M. Prioritization of Variants for Investigation of Genotype-Directed Nutrition in Human Superpopulations. Int. J. Mol. Sci. 2019, 20, 3516. [Google Scholar] [CrossRef]
- Steck, S.; Keku, T.; Butler, L.; Galanko, J.; Massa, B.; Millikan, R.; Sandler, R. Polymorphisms in Methionine Synthase, Methionine Synthase Reductase and Serine Hydroxymethyltransferase, Folate and Alcohol Intake, and Colon Cancer Risk. Lifestyle Genom. 2008, 1, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Sohn, Y. The Genetics of Obesity: A Narrative Review. Precis. Futur. Med. 2022, 6, 226–232. [Google Scholar] [CrossRef]
- Rankinen, T.; Zuberi, A.; Chagnon, Y.; Weisnagel, S.; Argyropoulos, G.; Walts, B.; Al, E. The Human Obesity Gene Map: The 2005 Update. Obesity 2006, 14, 529–644. [Google Scholar] [CrossRef]
- Ndiaye, F.; Huyvaert, M.; Ortalli, A.; Canouil, M.; Lecoeur, C.; Verbanck, M.; Lobbens, S.; Khamis, A.; Marselli, L.; Marchetti, P.; et al. The Expression of Genes in Top Obesity-Associated Loci Is Enriched in Insula and Substantia Nigra Brain Regions Involved in Addiction and Reward. Int. J. Obes. 2020, 44, 539–543. [Google Scholar] [CrossRef]
- Morais, C.; Cominetti, C. Bioetica e Testes Nutrigenéticos Preditivos. In Genômica Nutricional dos Fundamentos à Nutrição Molecular; Cominetti, C., Rogero, M., Horst, M., Eds.; Manole: Barueri, Brazil, 2017; pp. 516–521. [Google Scholar]
- Justice, A.; Winkler, T.; Al, F.M.; Feitosa, M.F.; Graff, M.; Fisher, V.A.; Young, K.; Barata, L.; Deng, X.; Czajkowski, J.; et al. Genome-Wide Meta-Analysis of 241,258 Adults Accounting for Smoking Behaviour Identifies Novel Loci for Obesity Traits. Nat. Commun. 2017, 8, 14977. [Google Scholar] [CrossRef]
- National Center for Biotechnology Information. Database of Single Nucleotide Polymorphisms. dbSNP. Available online: https://www.ncbi.nlm.nih.gov/snp/ (accessed on 16 October 2023).
- Cominetti, C.; Rogero, M.; Horst, M. Brazilian Society for Food and Nutrition Position Statement: Nutrigenetic Tests. Nutrire 2017, 42, 931. [Google Scholar] [CrossRef]
- García-Solís, P.; Reyes-Bastidas, M.; Flores, K.; García, O.; Rosado, J.; Méndez-Villa, L.; Garcia, G.C.; García-Gutiérrez, D.; Kuri-García, A.; Hernández-Montiel, H.; et al. Fat Mass Obesity-Associated (FTO) (Rs9939609) and Melanocortin 4 Receptor (MC4R) (Rs17782313) SNP Are Positively Associated with Obesity and Blood Pressure in Mexican School-Aged Children. Br. J. Nutr. 2016, 116, 1834–1840. [Google Scholar] [CrossRef]
- Walley, A.; Asher, J.; Froguel, P. The Genetic Contribuiton to Non-Syndromic Human Obesity. Nat. Rev. Genet. 2009, 10, 431–442. [Google Scholar] [CrossRef]
- Floris, M.; Cano, A.; Porru, L.; Addis, R.; Cambedda, A.; Idda, M.L.; Steri, M.; Ventura, C.; Maioli, M. Direct-to-Consumer Nutrigenetics Testing: An Overview. Nutrients 2020, 12, 566. [Google Scholar] [CrossRef] [PubMed]
- Pagon, R.; Hanson, N.; Neufeld-Kaiser, W.; Covington, M. Genetic Testing. West. J. Med. 2001, 174, 344–347. [Google Scholar] [CrossRef]
- Genetic Alliance; The New York-Mid-Atlantic Consortium for Genetic and Newborn Screening Services. Understanding Genetics: A New York, Mid-Atlantic Guide for Patients and Health Professionals; Genetic Alliance: Damascus, MD, USA, 2009. [Google Scholar]
- Oliveri, S.; Ferrari, F.; Manfrinati, A.; Pravettoni, G. A Systematic Review of the Psychological Implications of Genetic Testing: A Comparative Analysis Among Cardiovascular, Neurodegenerative and Cancer Diseases. Front. Genet. 2018, 9, 624. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) Committee on Assessing Genetic Risks; Andrews, L.B.; Fullarton, J.E.; Holtzman, N.A.; Motulsky, A.G. Assessing Genetic Risks: Implications for Health and Social Policy; National Academies Press: Washington, DC, USA, 1994. [Google Scholar]
- Rafi, I.; Qureshi, N.; Lucassen, A.; Modell, M.; Elmslie, F.; Kai, J.; Kirk, M.; Starey, N.; Goff, S.; Brennan, P.; et al. “Over-the-Counter” Genetic Testing: What Does It Really Mean for Primary Care? Br. J. Gen. Pract. 2009, 59, 283–287. [Google Scholar] [CrossRef]
- Inglese, S.; Lavazza, A.; Abbate, C. Crystal Ball Health Policies: A Case Against Preventive Testing For Alzheimer’s Disease. Front. Aging Neurosci. 2022, 14, 842629. [Google Scholar] [CrossRef]
- World Health Organization. Accelerating Access to Genomics for Global Health: Promotion, Implementation, Collaboration, and Ethical, Legal, and Social Issues: A Report of the WHO Science Council; WHO: Geneva, Switzerland, 2022.
- Ordovas, J.; Ferguson, L.; Tai, E.; Mathers, J. Personalised Nutrition and Health. BMJ 2018, 361, bmj.k2173. [Google Scholar] [CrossRef] [PubMed]
- Ginoza, M.; Isasi, R. Regulating Preimplantation Genetic Testing across the World: A Comparison of International Policy and Ethical Perspectives. Cold Spring Harb. Perspect. Med. 2020, 10, a036681. [Google Scholar] [CrossRef] [PubMed]
- Burke, W. Genetic Tests: Clinical Validity and Clinical Utility. Curr. Protoc. Hum. Genet. 2014, 81, 9.15.1–9.15.8. [Google Scholar] [CrossRef]
- National Human Genome Research Institute. Regulation of Genetic Tests. Available online: https://www.genome.gov/about-genomics/policy-issues/Regulation-of-Genetic-Tests (accessed on 16 October 2023).
- Abul-Husn, N.; Owusu Obeng, A.; Sanderson, S.; Gottesman, O.; Scott, S. Implementation and Utilization of Genetic Testing in Personalized Medicine. Pharmgenom. Pers. Med. 2014, 7, 227–240. [Google Scholar]
- Jiang, S.; Liberti, L.; Lebo, D. Direct-to-Consumer Genetic Testing: A Comprehensive Review. Ther. Innov. Regul. Sci. 2023, 57, 1190–1198. [Google Scholar] [CrossRef]
- Evans, J.; Skrzynia, C.; Burke, W. The Complexities of Predictive Genetic Testing. BMJ 2001, 322, 1052–1056. [Google Scholar] [CrossRef]
- Xi, Q.; Jin, S.; Morris, S. Economic Evaluations of Predictive Genetic Testing: A Scoping Review. PLoS ONE 2023, 18, e0276572. [Google Scholar] [CrossRef] [PubMed]
- Rose, A.; Peters, N.; Shea, J.; Armstrong, K. Attitudes and Misconceptions about Predictive Genetic Testing for Cancer Risk. Commun. Genet. 2005, 8, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Garrett, J.; Lantos, J.; Biesecker, L.; Childerhose, J.; Chung, W.; Holm, I.; Koenig, B.; McEwen, J.; Wilfond, B.; Brothers, K. Clinical Sequencing Exploratory Research (CSER) Consortium Pediatrics Working Group. Rethinking the “Open Future” Argument against Predictive Genetic Testing of Children. Genet. Med. 2019, 21, 2190–2198. [Google Scholar] [CrossRef]
- Saya, S.; McIntosh, J.; Winship, I.; Clendenning, M.; Milton, S.; Oberoi, J.; Dowty, J.; Buchanan, D.; Jenkins, M.; Emery, J. A Genomic Test for Colorectal Cancer Risk: Is This Acceptable and Feasible in Primary Care? Public Health Genom. 2020, 23, 110–121. [Google Scholar] [CrossRef] [PubMed]
- Kvaratskhelia, E.; Chokoshvili, D.; Kvintradze, M.; Surmava, S.; Dzagoevi, K.; Borry, P.; Abzianidze, E. Public Attitudes towards the Genetic Testing in Georgia. J. Commun. Genet. 2021, 12, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Wells, I.; Simons, G.; Davenport, C.; Mallen, C.; Raza, K.; Falahee, M. Acceptability of Predictive Testing for Ischemic Heart Disease in Those with a Family History and the Impact of Results on Behavioural Intention and Behaviour Change: A Systematic Review. BMC Public Health 2022, 22, 1751. [Google Scholar] [CrossRef] [PubMed]
- Naidoo, L.; Reddy, P. Stakeholder Knowledge and Attitudes toward the Use of Predictive Genetic Testing in South Africa. J. Community Genet. 2022, 13, 567–577. [Google Scholar] [CrossRef] [PubMed]
- De, S.; Pietilä, A.; Iso-Touru, T.; Hopia, A.; Tahvonen, R.; Vähäkangas, K. Information Provided to Consumers about Direct-to-Consumer Nutrigenetic Testing. Public Health Genom. 2019, 22, 162–173. [Google Scholar] [CrossRef] [PubMed]
- Martins, M.; Murry, L.; Telford, L.; Moriarty, F. Direct-to-Consumer Genetic Testing: An Updated Systematic Review of Healthcare Professionals’ Knowledge and Views, and Ethical and Legal Concerns. Eur. J. Hum. Genet. 2022, 30, 1331–1343. [Google Scholar] [CrossRef] [PubMed]
- Petersen, L.; Lefferts, J. Lessons Learned from Direct-to-Consumer Genetic Testing. Clin. Lab. Med. 2020, 40, 83–92. [Google Scholar] [CrossRef]
- Basch, C.; Hillyer, G.; Samuel, L.; Datuowei, E.; Cohn, B. Direct-to-Consumer Genetic Testing in the News: A Descriptive Analysis. J. Commun. Genet. 2023, 14, 63–69. [Google Scholar] [CrossRef]
- Guasch-Ferré, M.; Dashti, H.; Merino, J. Nutritional Genomics and Direct-to-Consumer Genetic Testing: An Overview. Adv. Nutr. 2018, 9, 128–135. [Google Scholar] [CrossRef]
- Phillips, A. Only a Click Away—DTC Genetics for Ancestry, Health, Love…and More: A View of the Business and Regulatory Landscape. Appl. Transl. Genom. 2016, 8, 16–22. [Google Scholar] [CrossRef]
- Malgorzata, M.; Maria, S.; Michał, W. Genetic Testing-Whether to Allow Complete Freedom? Direct to Consumer Tests versus Genetic Tests for Medical Purposes. J. Appl. Genet. 2022, 63, 119–126. [Google Scholar] [CrossRef]
- Naureen, Z.; Miggiano, G.; Aquilanti, B.; Velluti, V.; Matera, G.; Gagliardi, L.; Zulian, A.; Romanelli, R.; Bertelli, M. Genetic Test for the Prescription of Diets in Support of Physical Activity. Acta Biomed. 2020, 91, e2020011. [Google Scholar]
- Roosan, D.; Wu, Y.; Tran, M.; Huang, Y.; Baskys, A.; Roosan, M.R. Opportunities to Integrate Nutrigenomics into Clinical Practice and Patient Counseling. Eur. J. Clin. Nutr. 2023, 77, 36–44. [Google Scholar] [CrossRef]
- Stewart-Knox, B.; Bunting, B.; Gilpin, S.; Parr, H.J.; Pinhão, S.; Strain, J.J.; de Almeida, M.D.V.; Gibney, M. Attitudes toward Genetic Testing and Personalised Nutrition in a Representative Sample of European Consumers. Br. J. Nutr. 2008, 101, 982–989. [Google Scholar] [CrossRef]
- Oliveri, S.; Marton, G.; Vergani, L.; Cutica, I.; Gorini, A.; Spinella, F.; Pravettoni, G. Genetic Testing Consumers in Italy: A Preliminary Investigation of the Socio-Demographic Profile, Health-Related Habits, and Decision Purposes. Front. Public Health 2020, 8, 511. [Google Scholar] [CrossRef] [PubMed]
- Kaufman-Shriqui, V.; Salem, H.; Boaz, M.; Birk, R. Knowledge and Attitudes Towards Nutrigenetics: Findings from the 2018 Unified Forces Preventive Nutrition Conference (UFPN). Nutrients 2020, 12, 335. [Google Scholar] [CrossRef] [PubMed]
- Braakhuis, A.; Monnard, C.; Ellis, A.; Rozga, M. Consensus Report of the Academy of Nutrition and Dietetics: Incorporating Genetic Testing into Nutrition Care. J. Acad. Nutr. Diet. 2021, 121, 545–552. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Beltrán, Y.; González-Becerra, K.; Rivera-Iñiguez, I.; Martínez-López, E.; Ramos-Lopez, O.; Alcaraz-Mejía, M.; Rodríguez-Echevarría, R.; Sáyago-Ayerdi, S.; Mendivil, E. A Nutrigenetic Strategy for Reducing Blood Lipids and Low-Grade Inflammation in Adults with Obesity and Overweight. Nutrients 2023, 15, 4324. [Google Scholar] [CrossRef] [PubMed]
- Dudbridge, F. Power and Predictive Accuracy of Polygenic Risk Scores. PLoS Genet. 2013, 9, e003348. [Google Scholar] [CrossRef]
- Torkamani, A.; Topol, E. Polygenic Risk Scores Expand to Obesity. Cell 2019, 177, 518–520. [Google Scholar] [CrossRef]
- Joo, Y.; Actkins, K.; Pacheco, J.; Basile, A.; Carroll, R.; Crosslin, D.; Day, F.; Denny, J.C.; Edwards, D.R.V.; Hakonarson, H.; et al. A Polygenic and Phenotypic Risk Prediction for Polycystic Ovary Syndrome Evaluated by Phenome-Wide Association Studies. J. Clin. Endocrinol. Metab. 2020, 105, 1918–1936. [Google Scholar] [CrossRef]
- Park, J.; Lu, C. Polygenic Scores in the Direct-to-Consumer Setting: Challenges and Opportunities for a New Era in Consumer Genetic Testing. J. Pers. Med. 2023, 13, 573. [Google Scholar] [CrossRef]
- Arkadianos, I.; Valdes, A.; Marinos, E.; Florou, A.; Gill, R.; Grimaldi, K. Improved Weight Management Using Genetic Information to Personalize a Calorie Controlled Diet. Nutr. J. 2007, 6, 29. [Google Scholar] [CrossRef] [PubMed]
- Langley-Evans, S. Nutrigenetics and the Early Life Origins of Health and Disease: Effects of Protein Restriction. In Principles of Nutrigenetics and Nutrigenomics: Fundamentals for Individualized Nutrition; Caterina, R., Alfredo Martinez, J., Kohlmeier, M., Eds.; Elsevier: London, UK, 2019; pp. 113–119. [Google Scholar]
- Tamilvanan, J.; Kalpana, C. A Comparitive Analysis: Improved Weight Management Using Nutrigenetically Tailored Diet among Indians. J. Surv. Fish. Sci. 2023, 10, 4856–4862. [Google Scholar]
- Vranceanu, M.; Pickering, C.; Filip, L.; Pralea, I.; Sundaram, S.; Al-Saleh, A.; Popa, D.; Grimaldi, K. A Comparison of a Ketogenic Diet with a LowGI/Nutrigenetic Diet over 6 Months for Weight Loss and 18-Month Follow-Up. BMC Nutr. 2020, 6, 53. [Google Scholar] [CrossRef]
- Frankwich, K.; Egnatios, J.; Kenyon, M.; Rutledge, T.; Liao, P.; Gupta, S.; Herbst, K.; Zarrinpar, A. Differences in Weight Loss Between Persons on Standard Balanced vs Nutrigenetic Diets in a Randomized Controlled Trial. Clin. Gastroenterol. Hepatol. 2015, 13, 1625–1632.e1. [Google Scholar] [CrossRef]
- Robinson, K.; Rozga, M.; Braakhuis, A.; Ellis, A.; Monnard, C.; Sinley, R.; Wanner, A.; Vargas, A. Effect of Incorporating Genetic Testing Results into Nutrition Counseling and Care on Dietary Intake: An Evidence Analysis Center Systematic Review—Part I. J. Acad. Nutr. Diet. 2020, 121, 553–581.e3. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Ye, Z.; Whelan, K.; Truby, H. The Effect of Communicating the Genetic Risk of Cardiometabolic Disorders on Motivation and Actual Engagement in Preventative Lifestyle Modification and Clinical Outcome: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Br. J. Nutr. 2016, 116, 924–934. [Google Scholar] [CrossRef] [PubMed]
- Hollands, G.; French, D.; Griffin, S.J.; Prevost, A.T.; Sutton, S.; King, S.; Marteau, T.M. The Impact of Communicating Genetic Risks of Disease on Risk-Reducing Health Behaviour: Systematic Review with Metaanalysis. Br. Med. J. 2016, 352, i1102. [Google Scholar] [CrossRef]
- Bates, B.; Lynch, J.; Bevan, J.; Condit, C. Warranted Concerns, Warranted Outlooks: A Focus Group Study of Public Understandings of Genetic Research. Soc. Sci. Med. 2005, 60, 331–344. [Google Scholar] [CrossRef]
- Petersen, A. Securing Our Genetic Health: Engendering Trust in UK Biobank. Sociol. Health Illn. 2005, 27, 271–292. [Google Scholar] [CrossRef] [PubMed]
- Skirton, H.; Frazier, L.; Calvin, A.; Cohen, M. A Legacy for the Children—Attitudes of Older Adults in the United Kingdom to Genetic Testing. J. Clin. Nurs. 2006, 15, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Alain, D.; Lut, M.; Christel, F. Organisation and Financing of Genetic Testing in Belgium; The Belgian Health Care Knowledge Centre: Brussels, Belgium, 2007. [Google Scholar]
- Kalokairinou, L.; Howard, H.; Slokenberga, S.; Fisher, E.; Flatscher-Thöni, M.; Hartlev, M.; van Hellemondt, R.; Juškevičius, J.; Kapelenska-Pregowska, J.; Kováč, P.; et al. Legislation of Direct-to-consumer Genetic Testing in Europe: A Fragmented Regulatory Landscape. J. Commun. Genet. 2018, 9, 117–132. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Liang, B.; Zhu, L.; Shen, Y.; He, L. The Rise of the Genetic Counseling Profession in China. Am. J. Med. Genet. Part C Semin. Med. Genet. 2019, 181C, 170–176. [Google Scholar] [CrossRef]
- Bill, S. An Act to Prohibit and Prevent Genetic Discrimination; Parliament of Canada: Ottawa, ON, Canada, 2017.
- Pepe, R.; Lottenberg, A.; Fujiwara, C.; Beyruti, M.; Cintra, D.; Machado, R.; Rodrigues, A.; Jensen, N.; Caldas, A.; Fernandes, A.; et al. Position Statement on Nutrition Therapy for Overweight and Obesity: Nutrition Department of the Brazilian Association for the Study of Obesity and Metabolic Syndrome (ABESO-2022). Diabetol. Metab. Syndr. 2023, 15, 124. [Google Scholar] [CrossRef]


{kind=link}
| Author (Year) | Country | Nutrigenetic Company and the Number of SNPs Tested | Study Type | Aim of the Study | Participants | Main Results |
|---|---|---|---|---|---|---|
| Tamilvanan, Kalpana (2023) [107] | India | Nutrigenetic test (not specified); 15 SNPs tested in 10 genes involved in body weight and metabolism | Observational | To examine the usefulness of nutrigenetic testing in designing personalized diets and its potential to enhance weight loss | Healthy adults (n = 106) with BMI 25–40 kg/m2 and previous failures of weight loss maintenance. Nutrigenetic group (n = 54) and non-nutrigenetic group (n = 52) | The nutrigenetic group significantly reduced waist circumference and BMI at 60 and 90 days follow-up than the non-nutrigenetic group. |
| Vranceanu et al. (2020) [108] | Romania | NutriGENE by Eurogenetica Ltd./DNAfit, London, UK. Tested 28 SNPs in 22 genes with evidence of gene-diet/lifestyle interactions | Observational | To observe weight loss and biochemical parameters of participants following two different diet plans: ketogenic diet or low-glycemic index nutrigenetic (low-GI/NG) diet | Overweight and obese subjects (n = 114). Keto group (n = 53) and low-GI/NG group (n = 61) | After 24 weeks, the keto group lost more weight. However, at the 18-month follow-up, the low-GI/NG group lost significantly more weight and had more significant improvement in total cholesterol, HDL-c, and fasting glucose. |
| Frankwich et al. (2015) [109] | United States | Pathway Genomics, Inc., San Diego, CA, USA. Tested seven SNPs in seven genes involved in body weight and metabolism | RCT | To evaluate whether participants who followed a nutrigenetic-guided diet lost ≥ 5% of their body weight than participants on a standard balanced diet for 8 and 24 weeks | Obese or overweight US veterans (n = 51) were randomly assigned to groups placed on a nutrigenetic-guided diet (n = 30) or a standard balanced diet (n = 21) | No significant differences regarding weight loss, BMI, and waist circumference, among other outcomes, were observed between the groups. |
| Arkadianos et al. (2007) [105] | Greece | Sciona MyCellf kit (Sciona Inc., Boulder, CO, USA). Tested 24 SNPs in 19 genes involved in metabolism. | Clinical trial | Evaluate whether the use of nutrigenetic testing could promote long-term weight management. | Patients with a history of unsuccessful attempts at weight loss. Nutrigenetic group (n = 50) and control group (n = 43) | After 300 days, the nutrigenetic group had better long-term BMI reduction and improved blood fasting glucose. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duarte, M.K.R.N.; Leite-Lais, L.; Agnez-Lima, L.F.; Maciel, B.L.L.; Morais, A.H.d.A. Obesity and Nutrigenetics Testing: New Insights. Nutrients 2024, 16, 607. https://doi.org/10.3390/nu16050607
Duarte MKRN, Leite-Lais L, Agnez-Lima LF, Maciel BLL, Morais AHdA. Obesity and Nutrigenetics Testing: New Insights. Nutrients. 2024; 16(5):607. https://doi.org/10.3390/nu16050607
Chicago/Turabian StyleDuarte, Mychelle Kytchia Rodrigues Nunes, Lúcia Leite-Lais, Lucymara Fassarella Agnez-Lima, Bruna Leal Lima Maciel, and Ana Heloneida de Araújo Morais. 2024. "Obesity and Nutrigenetics Testing: New Insights" Nutrients 16, no. 5: 607. https://doi.org/10.3390/nu16050607
APA StyleDuarte, M. K. R. N., Leite-Lais, L., Agnez-Lima, L. F., Maciel, B. L. L., & Morais, A. H. d. A. (2024). Obesity and Nutrigenetics Testing: New Insights. Nutrients, 16(5), 607. https://doi.org/10.3390/nu16050607